
Robot-Assisted Total Thyroidectomy with or without Robot-Assisted Neck Dissection in Pediatric Patients with Differentiated Thyroid Cancer

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
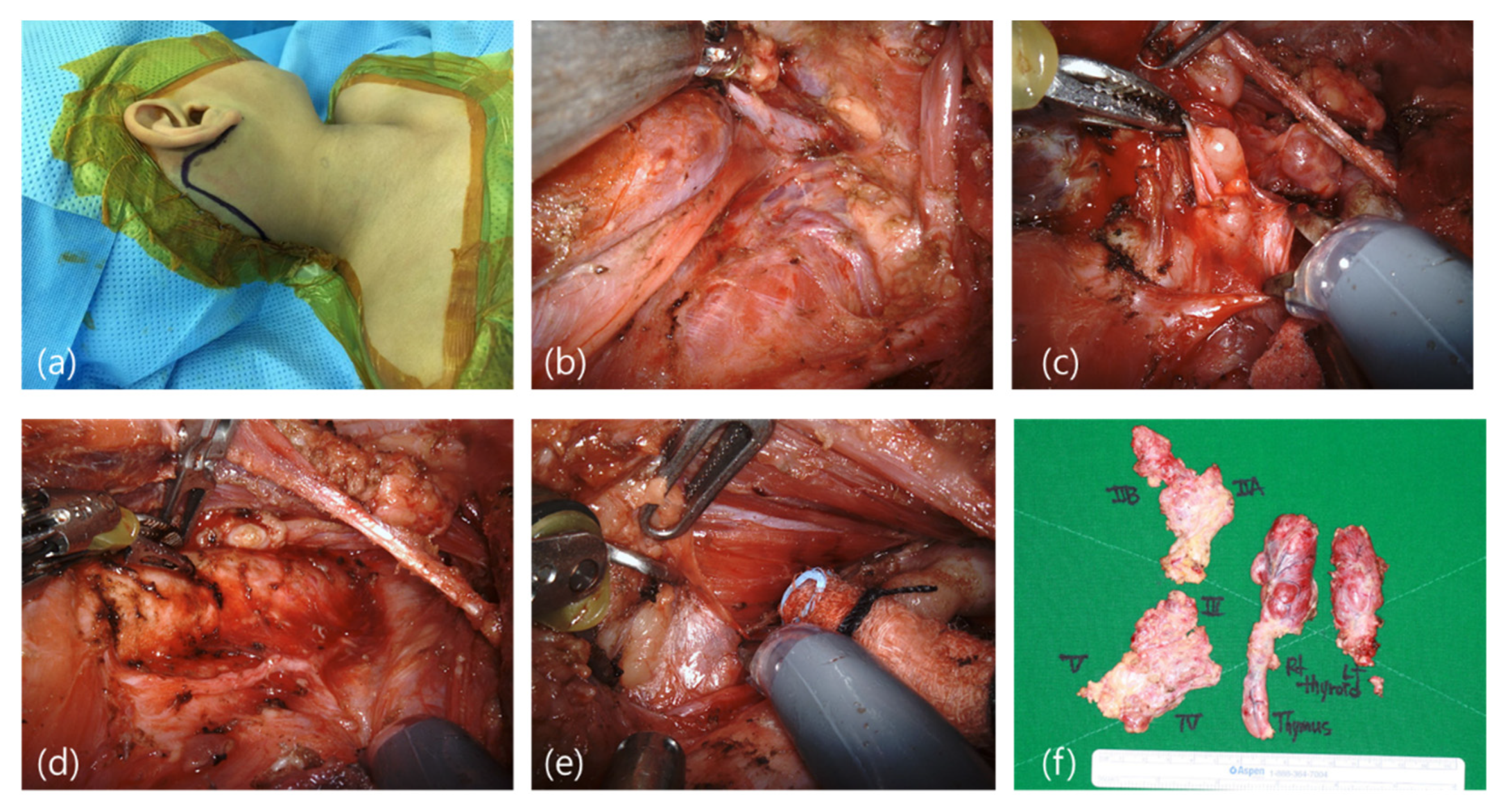
2.2. Surgical Technique
2.2.1. Robot-Assisted Modified Radical Neck Dissection (Levels II, III, IV, and V)
2.2.2. Robot-Assisted Total Thyroidectomy with Central Compartment Node Dissection
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Markovina, S.; Grigsby, P.W.; Schwarz, J.K.; DeWees, T.; Moley, J.F.; Siegel, B.A.; Perkins, S.M. Treatment approach, surveillance, and outcome of well-differentiated thyroid cancer in childhood and adolescence. Thyroid. Off. J. Am. Thyroid. Assoc. 2014, 24, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Steliarova-Foucher, E.; Stiller, C.A.; Pukkala, E.; Lacour, B.; Plesko, I.; Parkin, D.M. Thyroid cancer incidence and survival among European children and adolescents (1978–1997): Report from the Automated Childhood Cancer Information System project. Eur. J. Cancer 2006, 42, 2150–2169. [Google Scholar] [CrossRef] [PubMed]
- Avram, A.M.; Shulkin, B.L. Thyroid cancer in children. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2014, 55, 705–707. [Google Scholar] [CrossRef][Green Version]
- Dzepina, D. Surgical and pathological characteristics of papillary thyroid cancer in children and adolescents. Int. J. Pediatrics 2012, 2012, 125389. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vander Poorten, V.; Hens, G.; Delaere, P. Thyroid cancer in children and adolescents. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 135–142. [Google Scholar] [CrossRef]
- Ledbetter, D.J. Thyroid surgery in children. Semin. Pediatric Surg. 2014, 23, 60–65. [Google Scholar] [CrossRef]
- La Quaglia, M.P.; Corbally, M.T.; Heller, G.; Exelby, P.R.; Brennan, M.F. Recurrence and morbidity in differentiated thyroid carcinoma in children. Surgery 1988, 104, 1149–1156. [Google Scholar]
- Steinmuller, T.; Klupp, J.; Wenking, S.; Neuhaus, P. Complications associated with different surgical approaches to differentiated thyroid carcinoma. Langenbeck’s Arch. Surg./Dtsch. Ges. Fur Chir. 1999, 384, 50–53. [Google Scholar] [CrossRef]
- Gagner, M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br. J. Surg. 1996, 83, 875. [Google Scholar] [CrossRef]
- Kang, S.-W.; Jeong, J.; Yun, J.-S.; Sung, T.Y.; Lee, S.C.; Lee, Y.S.; Nam, K.-H.; Chang, H.S.; Chung, W.Y.; Park, C.S. Robot-assisted endoscopic surgery for thyroid cancer: Experience with the first 100 patients. Surg. Endosc. 2009, 23, 2399–2406. [Google Scholar] [CrossRef]
- Lee, J.; Chung, W.Y. Robotic thyroidectomy and neck dissection: Past, present, and future. Cancer J. 2013, 19, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.M.; Chung, W.Y.; Holsinger, F.C. Feasibility and surgical approach of transaxillary robotic thyroidectomy without CO2 insufflation. Head Neck 2010, 32, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.R.; Kang, S.-W.; Lee, S.H.; Rhee, K.Y.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Park, C.S. Feasibility and safety of a new robotic thyroidectomy through a gasless, transaxillary single-incision approach. J. Am. Coll. Surg. 2010, 211, e13–e19. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H.K.; Holsinger, F.C.; Tufano, R.P.; Chung, H.J.; Kim, W.S.; Koh, Y.W.; Choi, E.C. Robotic Total Thyroidectomy with Modified Radical Neck Dissection via Unilateral Retroauricular Approach. Ann. Surg. Oncol. 2014, 21, 3872–3875. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.S.; Koh, Y.W.; Byeon, H.K.; Park, Y.M.; Chung, H.J.; Kim, E.S.; Lee, E.J.; Park, S.C.; Choi, E.C. Robot-assisted neck dissection via a transaxillary and retroauricular approach versus a conventional transcervical approach in papillary thyroid cancer with cervical lymph node metastases. J. Laparoendosc. Adv. Surg. Tech. Part A 2014, 24, 367–372. [Google Scholar] [CrossRef]
- Terris, D.J.; Singer, M.C.; Seybt, M.W. Robotic facelift thyroidectomy: Patient selection and technical considerations. Surg. Laparosc. Endosc. Percutaneous Tech. 2011, 21, 237–242. [Google Scholar] [CrossRef]
- Lee, H.S.; Kim, W.S.; Hong, H.J.; Ban, M.J.; Lee, D.; Koh, Y.W.; Choi, E.C. Robot-assisted Supraomohyoid neck dissection via a modified face-lift or retroauricular approach in early-stage cN0 squamous cell carcinoma of the oral cavity: A comparative study with conventional technique. Ann. Surg. Oncol. 2012, 19, 3871–3878. [Google Scholar] [CrossRef]
- Kim, W.S.; Byeon, H.K.; Park, Y.M.; Ha, J.G.; Kim, E.S.; Koh, Y.W.; Choi, E.C. Therapeutic robot-assisted neck dissection via a retroauricular or modified facelift approach in head and neck cancer: A comparative study with conventional transcervical neck dissection. Head Neck 2015, 37, 249–254. [Google Scholar] [CrossRef]
- Vaisman, F.; Bulzico, D.A.; Pessoa, C.H.; Bordallo, M.A.N.; de Mendona, U.B.T.; Dias, F.L.; Coeli, C.M.; Corbo, R.; Vaisman, M. Prognostic factors of a good response to initial therapy in children and adolescents with differentiated thyroid cancer. Clinics 2011, 66, 281–286. [Google Scholar] [CrossRef]
- O’Connell, D.A.; Diamond, C.; Seikaly, H.; Harris, J.R. Objective and subjective scar aesthetics in minimal access vs conventional access parathyroidectomy and thyroidectomy surgical procedures: A paired cohort study. Arch. Otolaryngol.–Head Neck Surg. 2008, 134, 85–93. [Google Scholar] [CrossRef]
- Cuesta, R.; Beauregard, C. Psychosocial, Behavioral, and Emotional Effects Following Otoplasty. In Advanced Cosmetic Otoplasty; Shiffman, M.A., Ed.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 575–580. [Google Scholar]
- Skinner, M.A.; Wells, S.A., Jr. Medullary carcinoma of the thyroid gland and the MEN 2 syndromes. Semin. Pediatric Surg. 1997, 6, 134–140. [Google Scholar]
- Holsinger, F.C.; Chung, W.Y. Robotic thyroidectomy. Otolaryngol. Clin. N. Am. 2014, 47, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.C.; Terris, D.J. Robotic facelift thyroidectomy. Otolaryngol. Clin. N. Am. 2014, 47, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.W.; Lee, S.H.; Ryu, H.R.; Lee, K.Y.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Park, C.S. Initial experience with robot-assisted modified radical neck dissection for the management of thyroid carcinoma with lateral neck node metastasis. Surgery 2010, 148, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Lee, H.; Kang, S.; Hong, H.J.; Koh, Y.W.; Lee, H.Y.; Choi, H.; Choi, E.C. Feasibility of Robot-Assisted Neck Dissections via a Transaxillary and Retroauricular (“TARA”) Approach in Head and Neck Cancer: Preliminary Results. Ann. Surg. Oncol. 2012, 19, 1009–1017. [Google Scholar] [CrossRef]
- Terris, D.J.; Singer, M.C.; Seybt, M.W. Robotic facelift thyroidectomy: II. Clinical feasibility and safety. Laryngoscope 2011, 121, 1636–1641. [Google Scholar] [CrossRef]
- Terris, D.J.; Singer, M.C. Qualitative and quantitative differences between 2 robotic thyroidectomy techniques. Otolaryngol.–Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg. 2012, 147, 20–25. [Google Scholar] [CrossRef]
- Chen, Y.; Masiakos, P.T.; Gaz, R.D.; Hodin, R.A.; Parangi, S.; Randolph, G.W.; Sadow, P.M.; Stephen, A.E. Pediatric thyroidectomy in a high volume thyroid surgery center: Risk factors for postoperative hypocalcemia. J. Pediatric Surgery. 2015, 50, 1316–1319. [Google Scholar] [CrossRef]
- Sasson, A.R.; Pingpank, J.F., Jr.; Wetherington, R.W.; Hanlon, A.L.; Ridge, J.A. Incidental parathyroidectomy during thyroid surgery does not cause transient symptomatic hypocalcemia. Arch. Otolaryngol.–Head Neck Surg. 2001, 127, 304–308. [Google Scholar] [CrossRef]
- Harness, J.K.; Thompson, N.W.; McLeod, M.K.; Pasieka, J.L.; Fukuuchi, A. Differentiated thyroid carcinoma in children and adolescents. World J. Surg. 1992, 16, 547–553; discussion 53–54. [Google Scholar] [CrossRef]
- Koh, Y.W.; Choi, E.C. Robotic approaches to the neck. Otolaryngol. Clin. N. Am. 2014, 47, 433–454. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.S.; Ban, M.J.; Chang, J.W.; Byeon, H.K.; Kim, H.; Han, J.H.; Koh, Y.W.; Choi, E.C. Learning Curve for Robot-Assisted Neck Dissection in Head and Neck Cancer: A 3-Year Prospective Case Study and Analysis. JAMA Otolaryngol.–Head Neck Surg. 2014, 140, 1191–1197. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients | Gender/ Age (Years) | BMI (kg/m2) | Side a | Operation | CCND | Pathology | Tumor Size | ETE | CND | MRND | ECS | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TA1 | F/19 | 23.57 | L | HT | + | AH | 3.5 | − | 0/1 | 115 | ||
| TA2 | M/17 | 18.7 | R | HT | − | PC | 2 | − | − | 104 | ||
| TA3 | F/16 | 20.66 | B | TT | − | PC | 1.8 | − | − | 112 | ||
| TA4 | M/17 | 19.67 | B | TT | + | PC | 0.9 | − | 0/2 | 107 | ||
| TA5 | F/15 | 15.56 | B | TT c MND | + | PC | 2.7 | + | 3/6 | 9/32 | 104 | |
| TA6 | M/14 | 20.27 | R | TT c MND | + | PC | 1.7 | + | 0/5 | 11/42 | + | 98 |
| TA7 | F/19 | 18.2 | B | TT c MND | + | PC | 3.5 | + | 0/1 | 22/64 | 97 | |
| RA1 | F/13 | 18.29 | L | HT | + | PC | 2 | + | 0/7 | 79 | ||
| RA2 | F/16 | 27.85 | R | HT | − | PC | 1.2 | − | − | 57 | ||
| RA3 | M/15 | 24.44 | R | HT | − | PC | 3.5 | − | − | 93 | ||
| RA4 | F/17 | 23 | L | HT | + | PC | 3.5 | − | 0/5 | 76 | ||
| RA5 | F/18 | 20.74 | L | HT | − | PC | 0.9 | − | − | 50 | ||
| RA6 | F/18 | 14.68 | R | HT | + | PC | 3.3 | + | 2/5 | + | 27 | |
| RA7 | M/18 | 18.69 | R | HT | + | PC | 0.5 | + | 1/9 | 26 | ||
| RA8 | F/18 | 24.22 | R | HT | _ | FC | 1.2 | − | − | 107 | ||
| RA9 | F/17 | 22.99 | R | TT | + | PC | 1 | − | 3/9 | 92 | ||
| RA10 | F/18 | 18.34 | L | TT c MND | + | PC | 0.8 | − | 1/6 | 9/43 | 94 | |
| RA11 | F/15 | 22.76 | R | TT c MND | + | PC | 1.9 | + | 0/14 | 3/65 | 75 | |
| RA12 | F/17 | 28.93 | R | TT c MND | + | PC | 4 | + | 2/8 | 13/67 | 45 | |
| RA13 | F/9 | 17.09 | R | TT c MND | + | PC | 1.5 | + | 1/5 | 8/92 | + | 41 |
| RA14 | M/13 | 19.01 | R | TT c MND | + | PC | 5 | + | 3/5 | 6/49 | 17 | |
| RA15 | F/18 | 26.25 | R | TT c MND | + | PC | 1.1 | − | 5/10 | 8/65 | 17 | |
| Con1 | F/16 | 25.9 | R | HT | + | PC | 2.5 | + | 7/7 | 72 | ||
| Con2 | F/20 | 20.7 | R | TT | − | PC | − | − | 143 | |||
| Con3 | F/16 | 18.03 | L | TT | + | PC | 0.8 | + | 0/2 | 104 | ||
| Con4 | F/16 | 21.65 | B | TT | + | PC | 1.3 | + | 2/4 | 101 | ||
| Con5 | F/10 | 16.94 | L | TT | + | PC | 0.6 | − | 0/4 | − | ||
| Con6 | F/17 | 25.9 | B | Completion thyroidectomy c MND | − | PC | 3.9 | − | 0/1 | 10/52 | 72 | |
| Con7 | F/14 | 28.44 | L | TT c MND | + | PC | 1.8 | + | 15/18 | 35/58 | + | 151 |
| Con8 | M/11 | 20.98 | B | TT c MND | + | PC | 4.1 | + | 7/11 | 19/89 | + | 30 |
| Approach | RA | TA/TARA | Robot-Assisted | Conventional | p-Value |
|---|---|---|---|---|---|
| Hemithyroidectomy | 173.0 ± 32.0 | 119.5 ± 0.5 | 167.3 ± 33.2 | 92.0 ± 0.0 | <0.001 * |
| Total Thyroidectomy | 120.0 ± 0.0 | 256.0 ± 35.4 | 204.5 ± 52.9 | 168.3 ± 10.2 | 0.13 |
| Total Thyroidectomy c Modified Neck Dissection | 335.0 ± 57.5 | 534 ± 5.6 | 377.5 ± 98.8 | 350.0 ± 14.1 | 0.26 |
| Patients | Total Operation Time (min) | Flap Elevation and Dissection under Direct Vision (min) | Robot Docking for RAND (min) | Console Time for RAND (min) | Flap Elevation for TT (min) | Robot Docking for iT (min) | Console Time for iT (min) | Robot Docking for cT (min) | Console Time for cT (min) |
|---|---|---|---|---|---|---|---|---|---|
| TA5 | 530 | - | 5 | 157 | 3 | 105 | 62 | ||
| TA6 | 520 | 266 | - | - | 11 | 130 | 5 | 50 | |
| TA7 | 538 | 90 | 5 | 265 | |||||
| RA10 | 310 | 135 | 5 | 110 | 10 | 5 | 50 | ||
| RA11 | 430 | 185 | 5 | 40 | 5 | 63 | |||
| RA12 | 310 | 25 | 10 | 250 | |||||
| RA13 | 300 | 30 | 11 | 205 | |||||
| RA14 | 358 | 15 | 12 | 314 | |||||
| RA15 | 280 | 12 | 12 | 247 | - | - | |||
| Con6 | 340 | ||||||||
| Con7 | 360 | ||||||||
| Con8 | 410 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Sim, N.S.; Kim, D.; Choi, E.C.; Chang, J.W.; Koh, Y.W. Robot-Assisted Total Thyroidectomy with or without Robot-Assisted Neck Dissection in Pediatric Patients with Differentiated Thyroid Cancer. J. Clin. Med. 2022, 11, 3320. https://doi.org/10.3390/jcm11123320
Kim D, Sim NS, Kim D, Choi EC, Chang JW, Koh YW. Robot-Assisted Total Thyroidectomy with or without Robot-Assisted Neck Dissection in Pediatric Patients with Differentiated Thyroid Cancer. Journal of Clinical Medicine. 2022; 11(12):3320. https://doi.org/10.3390/jcm11123320
Chicago/Turabian StyleKim, Dahee, Nam Suk Sim, Dachan Kim, Eun Chang Choi, Jae Won Chang, and Yoon Woo Koh. 2022. "Robot-Assisted Total Thyroidectomy with or without Robot-Assisted Neck Dissection in Pediatric Patients with Differentiated Thyroid Cancer" Journal of Clinical Medicine 11, no. 12: 3320. https://doi.org/10.3390/jcm11123320
APA StyleKim, D., Sim, N. S., Kim, D., Choi, E. C., Chang, J. W., & Koh, Y. W. (2022). Robot-Assisted Total Thyroidectomy with or without Robot-Assisted Neck Dissection in Pediatric Patients with Differentiated Thyroid Cancer. Journal of Clinical Medicine, 11(12), 3320. https://doi.org/10.3390/jcm11123320