
How Long Does It Take to Regain Normocalcaemia in the Event of Postsurgical Hypoparathyroidism? A Detailed Time Course Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Postsurgical Follow-up Data
2.3. Definition of Postsurgical Hypoparathyroidism
2.4. Handling of Data and Statistical Analysis
2.5. Ethics Approval and Consent to Participate
3. Results
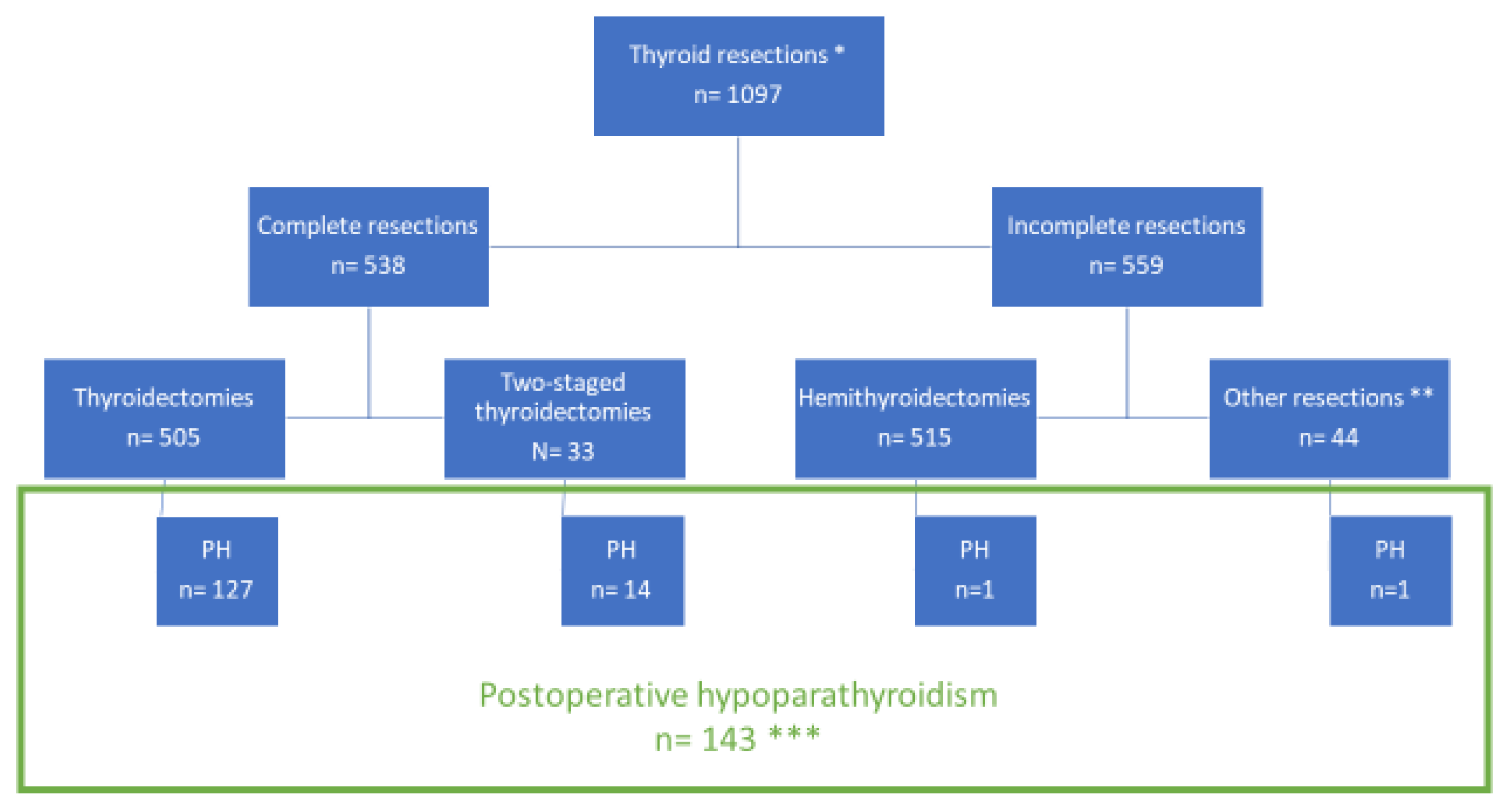
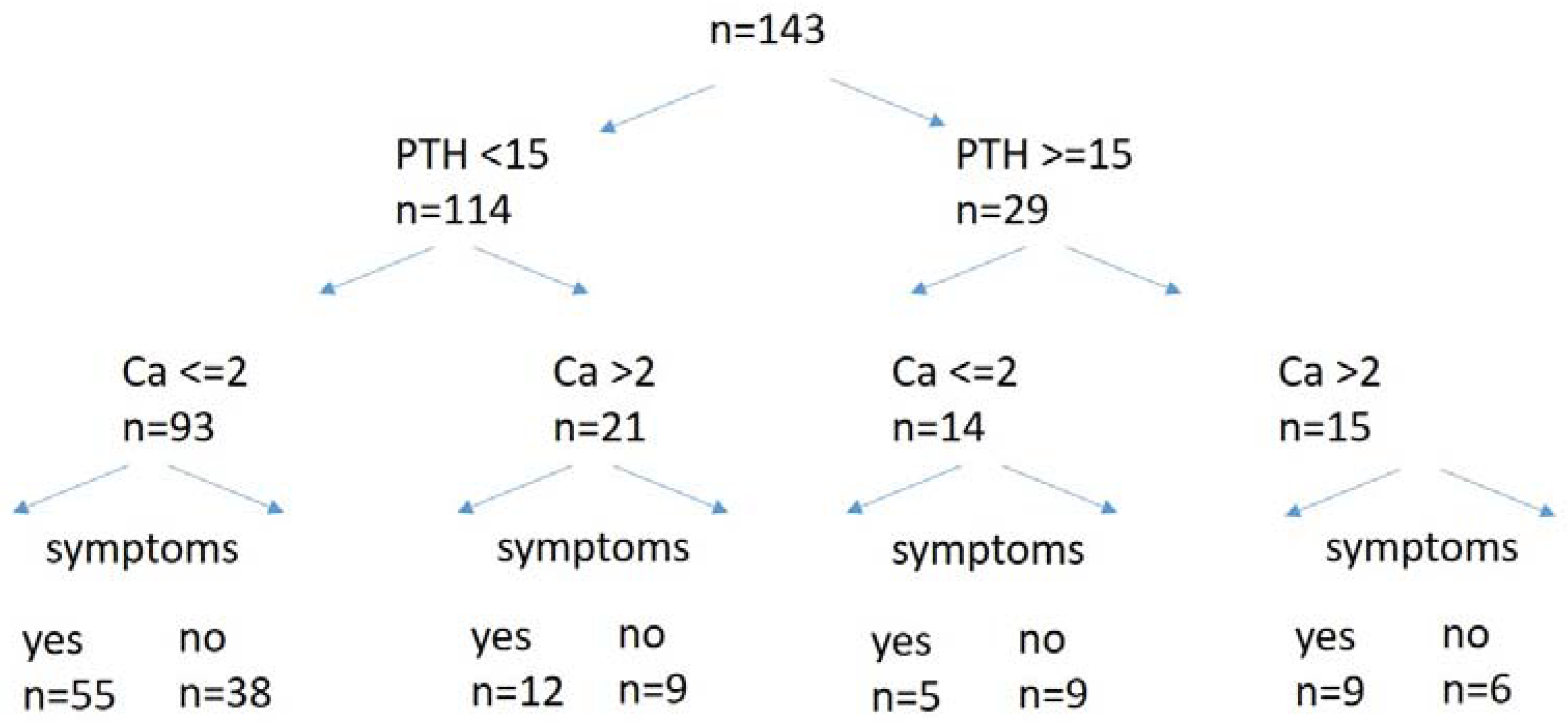
3.1. Postsurgical Hypocalcaemia—Patient Characteristics
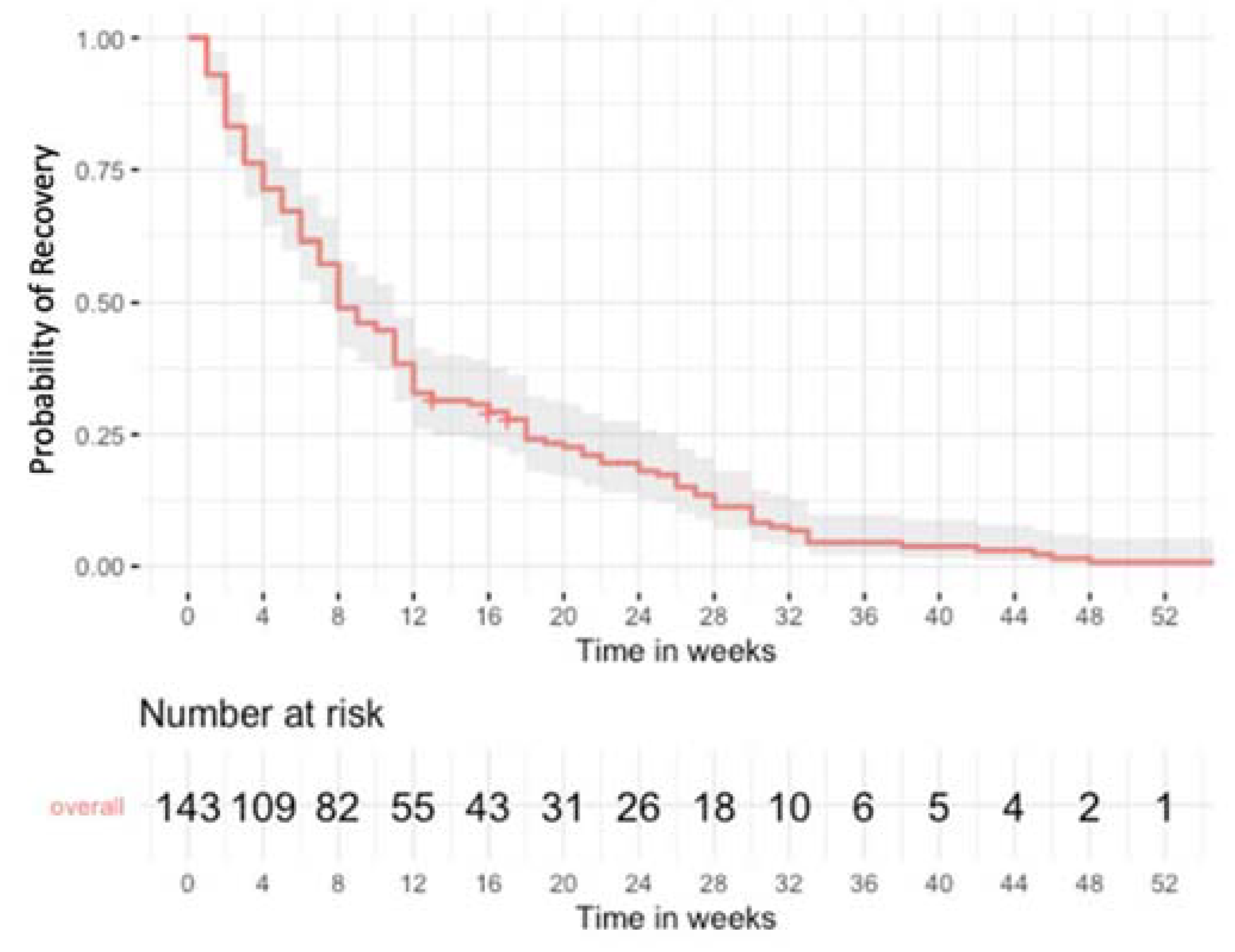
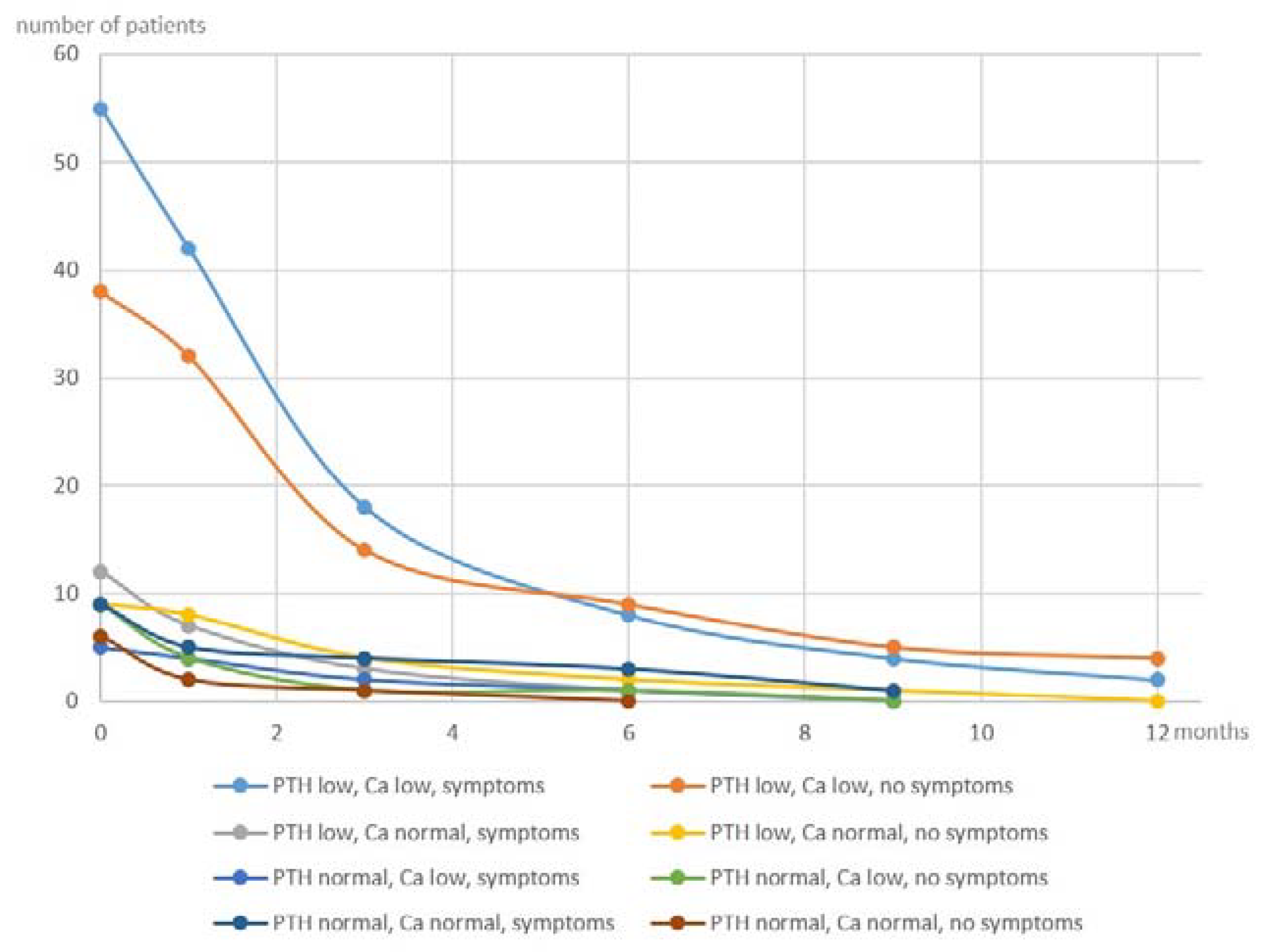
3.2. Postsurgical Hypoparathyroidism—Time Course of Recovery
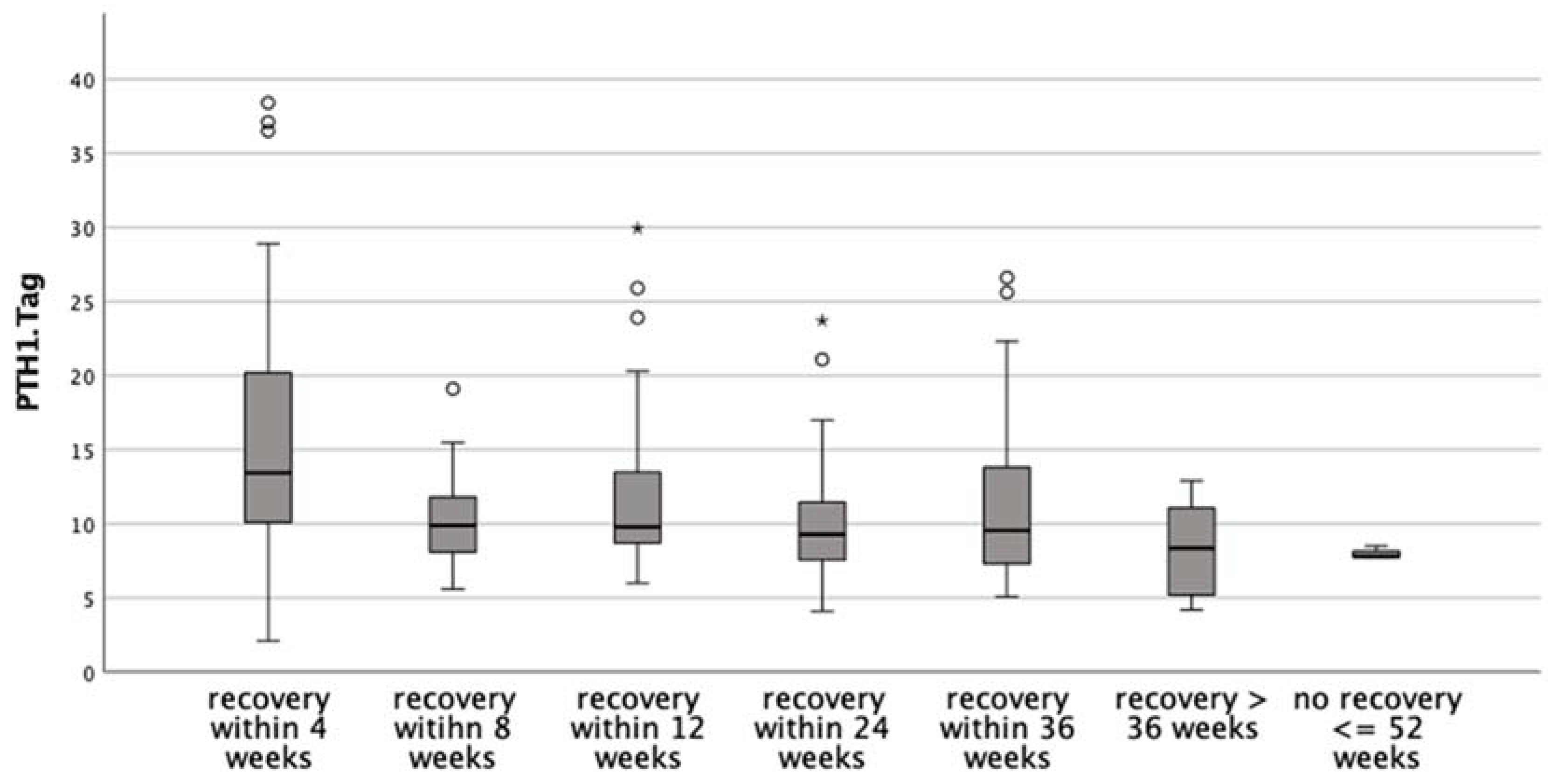
3.3. Postsurgical Hypoparathyroidism—Predictors for Time to Recovery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Dhahri, S.F.; Mubasher, M.; Mufarji, K.; Allam, O.S.; Terkawi, A.S. Factors predicting post-thyroidectomy hypoparathyroidism recovery. World J. Surg. 2014, 38, 2304–2310. [Google Scholar] [CrossRef] [PubMed]
- Glinoer, D.; Andry, G.; Chantrain, G.; Samil, N. Clinical aspects of early and late hypocalcaemia afterthyroid surgery. Eur. J. Surg. Oncol. 2000, 26, 571–577. [Google Scholar] [CrossRef]
- Cayo, A.K.; Yen, T.W.; Misustin, S.M.; Wall, K.; Wilson, S.D.; Evans, D.B.; Wang, T.S. Predicting the need for calcium and calcitriol supplementation after total thyroidectomy: Results of a prospective, randomized study. Surgery 2012, 152, 1059–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paduraru, D.N.; Ion, D.; Carsote, M.; Andronic, O.; Bolocan, A. Post-thyroidectomy Hypocalcemia—Risk Factors and Management. Chirurgia 2019, 114, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Thomusch, O.; Machens, A.; Sekulla, C.; Ukkat, J.; Brauckhoff, M.; Dralle, H. The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: A multivariate analysis of 5846 consecutive patients. Surgery 2003, 133, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Bilezikian, J.P.; Khan, A.; Potts, J.T., Jr.; Brandi, M.L.; Clarke, B.L.; Shoback, D.; Juppner, H.; D’Amour, P.; Fox, J.; Rejnmark, L.; et al. Hypoparathyroidism in the adult: Epidemiology, diagnosis, pathophysiology, target-organ involvement, treatment, and challenges for future research. J. Bone Miner. Res. 2011, 26, 2317–2337. [Google Scholar] [CrossRef]
- Chow, T.L.; Choi, C.Y.; Chiu, A.N. Postoperative PTH monitoring of hypocalcemia expedites discharge after thyroidectomy. Am. J. Otolaryngol. 2014, 35, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Kakava, K.; Tournis, S.; Papadakis, G.; Karelas, I.; Stampouloglou, P.; Kassi, E.; Triantafillopoulos, I.; Villiotou, V.; Karatzas, T. Postsurgical Hypoparathyroidism: A Systematic Review. In Vivo 2016, 30, 171–179. [Google Scholar]
- Cusano, N.E.; Anderson, L.; Rubin, M.R.; Silva, B.C.; Costa, A.G.; Irani, D.; Sliney, J., Jr.; Bilezikian, J.P. Recovery of parathyroid hormone secretion and function in postoperative hypoparathyroidism: A case series. J. Clin. Endocrinol. Metab. 2013, 98, 4285–4290. [Google Scholar] [CrossRef] [Green Version]
- Selberherr, A.; Scheuba, C.; Riss, P.; Niederle, B. Postoperative hypoparathyroidism after thyroidectomy: Efficient and cost-effective diagnosis and treatment. Surgery 2015, 157, 349–353. [Google Scholar] [CrossRef]
- Pfleiderer, A.G.; Ahmad, N.; Draper, M.R.; Vrotsou, K.; Smith, W.K. The timing of calcium measurements in helping to predict temporary and permanent hypocalcaemia in patients having completion and total thyroidectomies. Ann. R. Coll. Surg. Engl. 2009, 91, 140–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asari, R.; Passler, C.; Kaczirek, K.; Scheuba, C.; Niederle, B. Hypoparathyroidism after total thyroidectomy: A prospective study. Arch. Surg. 2008, 143, 132–137, discussion 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pattou, F.; Combemale, F.; Fabre, S.; Carnaille, B.; Decoulx, M.; Wemeau, J.L.; Racadot, A.; Proye, C. Hypocalcemia following thyroid surgery: Incidence and prediction of outcome. World J. Surg. 1998, 22, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Erbil, Y.; Barbaros, U.; Temel, B.; Turkoglu, U.; Issever, H.; Bozbora, A.; Ozarmagan, S.; Tezelman, S. The impact of age, vitamin D(3) level, and incidental parathyroidectomy on postoperative hypocalcemia after total or near total thyroidectomy. Am. J. Surg. 2009, 197, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Edafe, O.; Antakia, R.; Laskar, N.; Uttley, L.; Balasubramanian, S.P. Systematic review and meta-analysis of predictors of post-thyroidectomy hypocalcaemia. Br. J. Surg. 2014, 101, 307–320. [Google Scholar] [CrossRef]
- DGAV. Thyroid surgery quality assurance registry of the German Association of Surgeons (DGAV); StuDoQ|Thyroid. 2021. Available online: http://www.dgav.de/studoq.html (accessed on 23 November 2021).
- Allemeyer, E.H.; Kossow, M.S.; Riemann, B.; Hoffmann, M.W. Risk Factors for Permanent Postoperative Hypoparathyreoidism. Zentralbl. Chir. 2019, 145, 168–175. [Google Scholar] [CrossRef]
- Almquist, M.; Hallgrimsson, P.; Nordenstrom, E.; Bergenfelz, A. Prediction of permanent hypoparathyroidism after total thyroidectomy. World J. Surg. 2014, 38, 2613–2620. [Google Scholar] [CrossRef]
- Evans, J.D. Straightforward Statistics for the Behavioral Sciences; Brooks/Cole Pub. Co.: Pacific Grove, CA, USA, 1996. [Google Scholar]
- Lorente-Poch, L.; Sancho, J.J.; Muñoz-Nova, J.L.; Sánchez-Velázquez, P.; Sitges-Serra, A. Defining the syndromes of parathyroid failure after total thyroidectomy. Gland Surg. 2015, 4, 82–90. [Google Scholar] [CrossRef]
- Sitges-Serra, A. Etiology and Diagnosis of Permanent Hypoparathyroidism after Total Thyroidectomy. J. Clin. Med. 2021, 10, 543. [Google Scholar] [CrossRef]
- Harsløf, T.; Rolighed, L.; Rejnmark, L. Huge variations in definition and reported incidence of postsurgical hypoparathyroidism: A systematic review. Endocrine 2019, 64, 176–183. [Google Scholar] [CrossRef]
- Koimtzis, G.D.; Stefanopoulos, L.; Giannoulis, K.; Papavramidis, T.S. What are the real rates of temporary hypoparathyroidism following thyroidectomy? It is a matter of definition: A systematic review. Endocrine 2021, 73, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Nagarajan, N.; Kahan, S.; Schneider, E.B.; Zeiger, M.A. Association of Parathyroid Hormone Level with Postthyroidectomy Hypocalcemia: A Systematic Review. JAMA Surg. 2018, 153, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Strajina, V.; Dy, B.M.; McKenzie, T.J.; Thompson, G.B.; Lyden, M.L. Predicting Postthyroidectomy Hypocalcemia: Improving Predictive Ability of Parathyroid Hormone Level. Am. Surg. 2020, 86, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Suwannasarn, M.; Jongjaroenprasert, W.; Chayangsu, P.; Suvikapakornkul, R.; Sriphrapradang, C. Single measurement of intact parathyroid hormone after thyroidectomy can predict transient and permanent hypoparathyroidism: A prospective study. Asian J. Surg. 2017, 40, 350–356. [Google Scholar] [CrossRef] [Green Version]
- Sitges-Serra, A.; Gomez, J.; Barczynski, M.; Lorente-Poch, L.; Iacobone, M.; Sancho, J. A nomogram to predict the likelihood of permanent hypoparathyroidism after total thyroidectomy based on delayed serum calcium and iPTH measurements. Gland Surg. 2017, 6 (Suppl. S1), S11–S19. [Google Scholar] [CrossRef] [Green Version]
- Vaitsi, K.D.; Anagnostis, P.; Veneti, S.; Papavramidis, T.S.; Goulis, D.G. Preoperative Vitamin D Deficiency is a Risk Factor for Postthyroidectomy Hypoparathyroidism: A Systematic Review and Meta-Analysis of Observational Studies. J. Clin. Endocrinol. Metab. 2021, 106, 1209–1224. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) Unless Otherwise Stated | All Procedures | Procedures w Postsurgical Hypoparathyroidism (PH) n = 143 |
|---|---|---|
| n = 1097 | ||
| Malignant thyroid condition | 155 (14.1) | 20 (14) |
| Central LAD | 67 (6.1) | 22 (16.8) |
| Graves’ disease | 86 (7.8) | 16 (11.2) |
| Reoperative Surgery | 126 (11.5) | 12 (8.4) |
| Thyroidectomy | 505 (46) | 127 (88.8) |
| Hemithyroidectomy (HTx) | 515 (46.9) | 2 (1.4) |
| Two-staged bilateral HTx | 33 (3.0) | 14 (9.8) |
| PTG visualised | ||
| 0 | 71 (6.5) | 7 (4.9) |
| 1 | 205 (18.7) | 3 (3.1) |
| 2 | 390 (35.6) | 22 (15.4) |
| 3 | 152 (13.9) | 43 (30.1) |
| 4 | 279 (25.4) | 68 (47.5) |
| PTG autograft | ||
| 0 | 938 (85.5) | 110 (76.9) |
| 1 | 146 (13.3) | 31 (21.7) |
| 2 | 12 (1.1) | 2 (1.4) |
| 4 | 1 (0.1) | 0 |
| PTH POD 1, median (IQR) | - | 10.4 (8.1–14.4) |
| PTH POD 2, median (IQR) | - | 9.8 (7.6–11.9) |
| Calcium POD 1, median (IQR) | - | 2.1 (2.0–2.2) |
| Calcium POD 2, median (IQR) | - | 2.0 (1.9–2.1) |
| n (%) Unless Otherwise Stated | Recovered ≤ 12 Weeks | Recovered > 12 Weeks | p-Value |
|---|---|---|---|
| n = 96 | n = 47 | ||
| Female gender | 85 (88.5) | 37 (78.7) | 0.136 |
| Thyroidectomy | 85 (88.5) | 42 (89.4) | 1 |
| Graves’ disease | 14 (14.6) | 2 (4.3) | 0.09 |
| Malignant thyroid condition | 13 (13.5) | 7 (14.9) | 0.803 |
| Central LND | 15 (15.6) | 9 (19.1) | 0.637 |
| Reoperative surgery | 5 (10.6) | 7 (7.3) | 0.53 |
| PTG visualised | 0.066 | ||
| 0 | 5 (5.2) | 2 (4.3) | |
| 1 | 3 (3.1) | 0 | |
| 2 | 11 (11.5) | 11 (23.4) | |
| 3 | 25 (26) | 18 (38.3) | |
| 4 | 52 (54.2) | 16 (34) | |
| PTG autograft | 0.223 | ||
| 0 | 77 (80.2) | 33 (70.2) | |
| 1 | 17 (17.7) | 14 (29.8) | |
| 2 | 2 (2.1) | 0 | |
| Immediate calcium substitution | 13 (13.5) | 2 (4.3) | 0.144 |
| Symptoms of PH | 55 (57.3) | 26 (55.3) | 0.859 |
| PTH POD 1, median (IQR) | 11.0 (7.3–11.6) | 9.1 (9–15.4) | 0.006 |
| PTH POD 2, median (IQR) | 10.2 (7.8–13.6) | 8.6 (7.8–12.2) | 0.008 |
| Calcium POD 1, median (IQR) | 2.1 (2–1.1) | 2.1 (2–2.2) | 0.544 |
| Calcium POD 2, median (IQR) | 2 (1.9–2.1) | 2 (1.9–2.1) | 0.31 |
| n (%) Unless Otherwise Stated | Recovered ≤ 24 Weeks | Recovered > 24 Weeks | p-Value |
|---|---|---|---|
| n = 116 | n = 27 | ||
| Female gender | 98 (84.5) | 24 (88.9) | 0.765 |
| Thyroidectomy | 104 (89.7) | 23 (85.2) | 0.592 |
| Malignant thyroid condition | 16 (13.8) | 4 (14.8) | 1 |
| Central LAD | 17 (14.7) | 7 (25.9) | 0.163 |
| Graves’ disease | 15 (12.9) | 1 (3.7) | 0.307 |
| Reoperative surgery | 8 (6.9) | 4 (14.8) | 0.24 |
| PTG visualised | 0.089 | ||
| 0 | 5 (4.3) | 2 (7.4) | 0.62 |
| 1 | 3 (2.6) | 0 | 1 |
| 2 | 15 (12.9) | 7 (25.9) | 0.135 |
| 3 | 33 (28.4) | 10 (37.0) | 0.485 |
| 4 | 60 (51.7) | 8 (29.6) | 0.053 |
| PTG autograft | 1 | ||
| 0 | 90 (77.6) | 20 (74.1) | |
| 1 | 24 (20.7) | 7 (25.9) | |
| 2 | 2 (1.7) | 0 | |
| Immediate calcium substitution | 14 (12.1) | 1 (3.7) | 0.304 |
| Symptoms of PH | 68 (58.6) | 13 (48.1) | 0.39 |
| PTH POD 1, median (IQR) | 10.8 (8.45–15.1) | 8.8 (7.3–12.7) | 0.033 |
| PTH POD 2, median (IQR) | 9.9 (7.78–12.53) | 8.4 (7–10.45) | 0.057 |
| PTH > 15 and <65 POD 1 | 48 (42.1) | 7 (25.9) | 0.132 |
| PTH ≥ 10 POD 1 | 54 (46.6) | 18 (66.7) | 0.086 |
| Calcium POD 1, median (IQR) | 2.1 (2–2.2) | 2.0 (2–2.1) | 0.096 |
| Calcium POD 2, median (IQR) | 2 (1.9–2.1) | 1.95 (1.8–2.1) | 0.387 |
| Univariable Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | Lower CI | Upper CI | p-Value | OR | Lower CI | Upper CI | p-Value | |
| (a) recovery within 4 weeks (within 4 weeks n = 41 vs. later than 4 weeks n = 102) | ||||||||
| Graves’ disease | 3.82 | 1.32 | 11.08 | 0.014 | 2.40 | 0.72 | 8.07 | 0.156 |
| Central LAD | 0.61 | 0.21 | 1.75 | 0.355 | ||||
| All PTG visualized | 1.86 | 0.89 | 3.88 | 0.097 | 2.02 | 0.88 | 4.63 | 0.098 |
| PTG autograft | 1.35 | 0.64 | 2.89 | 0.433 | ||||
| PTH POD 1 | 1.12 | 1.05 | 1.19 | <0.001 | 1.13 | 1.06 | 1.20 | <0.001 |
| Calcium POD 1 | 0.40 | 0.03 | 4.70 | 0.464 | ||||
| Symptoms | 1.12 | 0.54 | 2.32 | 0.772 | ||||
| Female gender | 2.71 | 0.75 | 9.77 | 0.127 | 2.69 | 0.64 | 11.34 | 0.178 |
| HL ChiSq 13.966, p 0.083, AUC 0.771 | ||||||||
| (b) recovery within 24 weeks (within 12 weeks n = 116 vs. later than 24 weeks n = 27) | ||||||||
| Graves’ disease | 3.86 | 0.49 | 30.3 | 0.201 | ||||
| Malignity | 0.92 | 0.28 | 3.01 | 0.890 | ||||
| All PTG visualized | 2.55 | 1.03 | 6.29 | 0.043 | 2.69 | 1.08 | 6.69 | 0.033 |
| PTG autograft | 0.92 | 0.38 | 2.25 | 0.856 | ||||
| PTH POD 1 | 1.07 | 0.98 | 1.16 | 0.136 | 1.07 | 0.98 | 1.16 | 0.125 |
| Ca POD 1 | 7.04 | 0.40 | 125.0 | 0.184 | ||||
| Symptoms | 0.65 | 0.28 | 1.52 | 0.325 | ||||
| Female gender | 0.68 | 0.19 | 2.50 | 0.562 | ||||
| HL ChiSq 7.267, p 0.508, AUC 0.664 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guglielmetti, L.; Schmidt, S.; Busch, M.; Wagner, J.; Naddaf, A.; Leitner, B.; Harsch, S.; Zielke, A.; Smaxwil, C. How Long Does It Take to Regain Normocalcaemia in the Event of Postsurgical Hypoparathyroidism? A Detailed Time Course Analysis. J. Clin. Med. 2022, 11, 3202. https://doi.org/10.3390/jcm11113202
Guglielmetti L, Schmidt S, Busch M, Wagner J, Naddaf A, Leitner B, Harsch S, Zielke A, Smaxwil C. How Long Does It Take to Regain Normocalcaemia in the Event of Postsurgical Hypoparathyroidism? A Detailed Time Course Analysis. Journal of Clinical Medicine. 2022; 11(11):3202. https://doi.org/10.3390/jcm11113202
Chicago/Turabian StyleGuglielmetti, Laura, Sina Schmidt, Mirjam Busch, Joachim Wagner, Ali Naddaf, Barbara Leitner, Simone Harsch, Andreas Zielke, and Constantin Smaxwil. 2022. "How Long Does It Take to Regain Normocalcaemia in the Event of Postsurgical Hypoparathyroidism? A Detailed Time Course Analysis" Journal of Clinical Medicine 11, no. 11: 3202. https://doi.org/10.3390/jcm11113202
APA StyleGuglielmetti, L., Schmidt, S., Busch, M., Wagner, J., Naddaf, A., Leitner, B., Harsch, S., Zielke, A., & Smaxwil, C. (2022). How Long Does It Take to Regain Normocalcaemia in the Event of Postsurgical Hypoparathyroidism? A Detailed Time Course Analysis. Journal of Clinical Medicine, 11(11), 3202. https://doi.org/10.3390/jcm11113202