
Skeletal, Dental and Soft Tissue Cephalometric Changes after Orthodontic Treatment of Dental Class II Malocclusion with Maxillary First Molar or First Premolar Extractions

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Selection
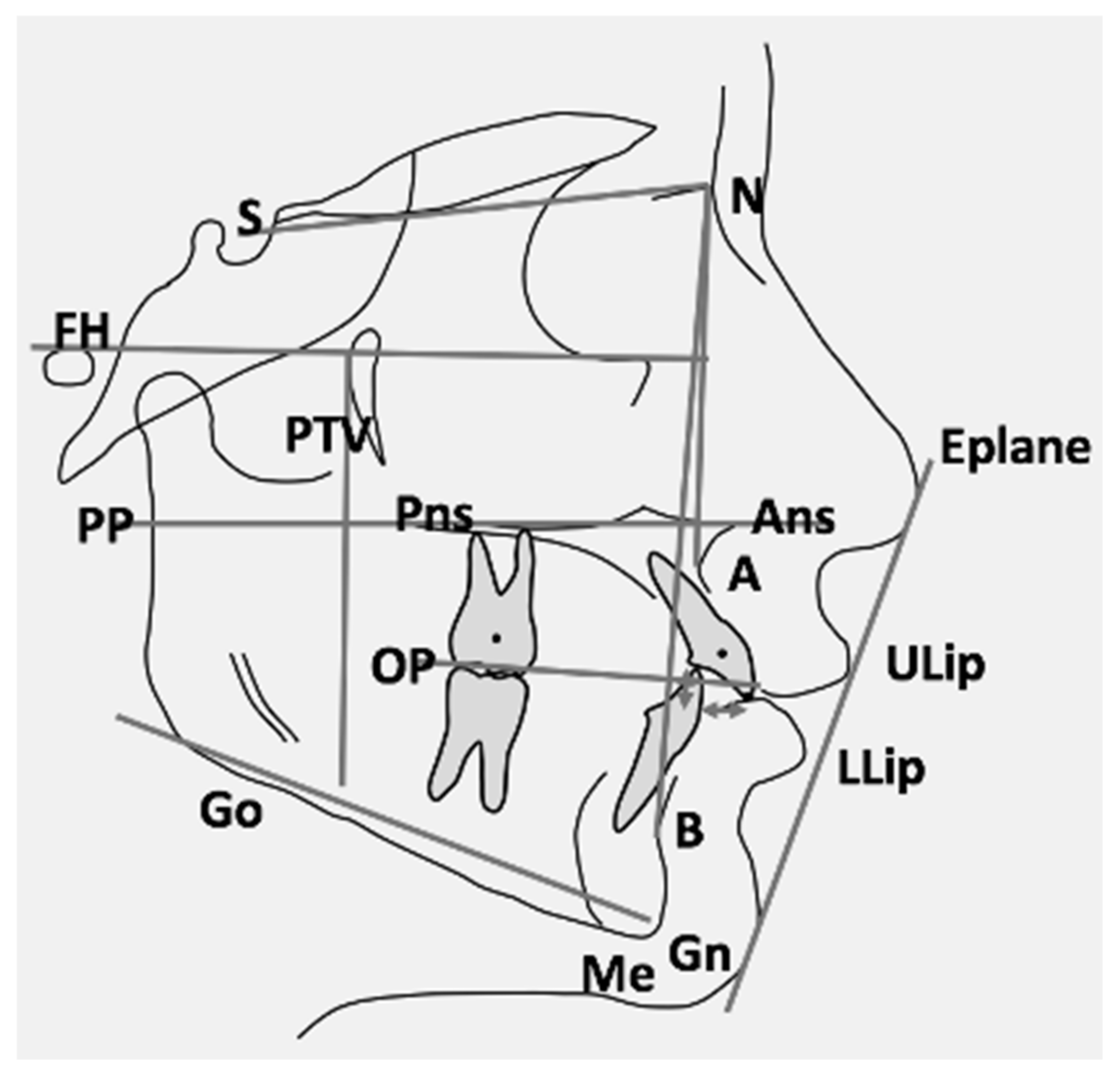
2.2. Cephalometric Analysis
2.3. Method Error and Statistical Analysis
3. Results
3.1. Skeletal Changes
3.2. Dental Changes
3.3. Soft Tissues and Profile Changes
4. Discussion
5. Conclusions
- Orthodontic treatment with maxillary first premolar or first molar extraction produces comparable vertical skeletal results. Therefore, an increased SN^GoGn angle should not be considered the discriminating factor for choosing a first molar extraction treatment over a first premolar extraction treatment.
- The significantly larger reduction of upper lip protrusion and overjet after maxillary first molar extraction compared to first premolar extraction suggests preferring molar extraction treatment in the case of a Class II malocclusion with a protrusive soft tissue profile and increased overjet.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Männchen, R.; Serafin, M.; Fastuca, R.; Caprioglio, A. Does Early Treatment Improve Clinical Outcome of Class II Patients? A Retrospective Study. Children 2022, 9, 232. [Google Scholar] [CrossRef] [PubMed]
- Evrard, A.; Tepedino, M.; Cattaneo, P.M.; Cornelis, M.A. Which factors influence orthodontists in their decision to extract? A questionnaire survey. J. Clin. Exp. Dent. 2019, 11, e432–e438. [Google Scholar] [CrossRef] [PubMed]
- Serafin, M.; Fastuca, R.; Castellani, E.; Caprioglio, A. Occlusal Plane Changes After Molar Distalization with a Pendulum Appliance in Growing Patients with Class II Malocclusion: A Retrospective Cephalometric Study. Turk. J. Orthod. 2021, 34, 10–17. [Google Scholar] [CrossRef]
- Moser, L.; Di Lorenzo, E.; Serafin, M.; Maino, G.; Schneider-Moser, U.; Cozzani, M.; Caprioglio, A. Maxillary premolars extraction or molar distalization with or without TAD’s: Cephalometric evaluation of soft tissue changes in Class II treatment. South Eur. J. Orthod. Dentofac. Res. 2020, 7, 4–11. [Google Scholar] [CrossRef]
- Raposo, R.; Peleteiro, B.; Paço, M.; Pinho, T. Orthodontic camouflage versus orthodontic-orthognathic surgical treatment in class II malocclusion: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Janson, M.; Nakamura, A.; de Freitas, M.R.; Henriques, J.F.; Pinzan, A. Influence of cephalometric characteristics on the occlusal success rate of Class II malocclusions treated with 2- and 4-premolar extraction protocols. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Brambilla Ada, C.; Henriques, J.F.; de Freitas, M.R.; Neves, L.S. Class II treatment success rate in 2- and 4-premolar extraction protocols. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Atik, E.; Akarsu-Guven, B.; Kocadereli, I. Soft tissue effects of three different Class II/1-camouflage treatment strategies. J. Orofac. Orthop. 2017, 78, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Chew, M.T.; Sandham, A. Effectiveness and duration of two-arch fixed appliance treatment. Aust. Orthod. J. 2000, 16, 98–103. [Google Scholar]
- Seben, M.P.; Valarelli, F.P.; de Freitas, K.M.; Cançado, R.H.; Bittencourt Neto, A.C. Cephalometric changes in Class II division 1 patients treated with two maxillary premolars extraction. Dent. Press J. Orthod. 2013, 18, 61–69. [Google Scholar] [CrossRef][Green Version]
- Stalpers, M.J.; Booij, J.W.; Bronkhorst, E.M.; Kuijpers-Jagtman, A.M.; Katsaros, C. Extraction of maxillary first permanent molars in patients with Class II Division 1 malocclusion. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 316–323. [Google Scholar] [CrossRef]
- Sabri, R. Multidisciplinary management of permanent first molar extractions. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 682–692. [Google Scholar] [CrossRef]
- Booij, J.W.; Kuijpers-Jagtman, A.M.; Katsaros, C. A treatment method for Class II Division 1 patients with extraction of permanent maxillary first molars. World J. Orthod. 2009, 10, 41–48. [Google Scholar]
- Williams, R. Single arch extraction—Upper first molars or what to do when nonextraction treatment fails. Am. J. Orthod. 1979, 76, 376–393. [Google Scholar] [CrossRef]
- Booij, J.W.; Goeke, J.; Bronkhorst, E.M.; Pancherz, H.; Ruf, S.; Katsaros, C. Overjet correction and space closure mechanisms for Class II treatment by extracting the maxillary first molars. J. Orofac. Orthop. 2011, 72, 196–203. [Google Scholar] [CrossRef]
- Booij, J.W.; Goeke, J.; Bronkhorst, E.M.; Katsaros, C.; Ruf, S. Class II treatment by extraction of maxillary first molars or Herbst appliance: Dentoskeletal and soft tissue effects in comparison. J. Orofac. Orthop. 2013, 74, 52–63. [Google Scholar] [CrossRef]
- McNamara, J.A., Jr.; Franchi, L. The cervical vertebral maturation method: A user’s guide. Angle Orthod. 2018, 88, 133–143. [Google Scholar] [CrossRef]
- Ozaki, T.; Ozaki, S.; Kuroda, K. Premolar and additional first molar extraction effects on soft tissue. Effects on high Angle Class II division 1 patients. Angle Orthod. 2007, 77, 244–253. [Google Scholar] [CrossRef]
- Kouvelis, G.; Dritsas, K.; Doulis, I.; Kloukos, D.; Gkantidis, N. Effect of orthodontic treatment with 4 premolar extractions compared with nonextraction treatment on the vertical dimension of the face: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 175–187. [Google Scholar] [CrossRef]
- Sivakumar, A.; Valiathan, A. Cephalometric assessment of dentofacial vertical changes in Class I subjects treated with and without extraction. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 869–875. [Google Scholar] [CrossRef]
- Paquette, D.E.; Beattie, J.R.; Johnston, L.E., Jr. A long-term comparison of nonextraction and premolar extraction edgewise therapy in “borderline” Class II patients. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 1–14. [Google Scholar] [CrossRef]
- Sambataro, S.; Fastuca, R.; Oppermann, N.J.; Lorusso, P.; Baccetti, T.; Franchi, L.; Caprioglio, A. Cephalometric changes in growing patients with increased vertical dimension treated with cervical headgear. J. Orofac. Orthop. 2017, 78, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Caprioglio, A.; Fontana, M.; Longoni, E.; Cozzani, M. Long-term evaluation of the molar movements following Pendulum and fixed appliances. Angle Orthod. 2013, 83, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Caprioglio, A.; Cozzani, M.; Fontana, M. Comparative evaluation of molar distalization therapy with erupted second molar: Segmented versus Quad Pendulum appliance. Prog. Orthod. 2014, 15, 49. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Cozzani, M.; Caprioglio, A. Non-compliance maxillary molar distalizing appliances: An overview of the last decade. Prog. Orthod. 2012, 13, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Aliaga-Del Castillo, A.; Niederberger, A. Changes in apical base sagittal relationship in Class II malocclusion treatment with and without premolar extractions: A systematic review and meta-analysis. Angle Orthod. 2017, 87, 338–355. [Google Scholar] [CrossRef] [PubMed]
- LaHaye, M.B.; Buschang, P.H.; Alexander, R.G.; Boley, J.C. Orthodontic treatment changes of chin position in Class II Division 1 patients. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 732–741. [Google Scholar] [CrossRef]
- Sangcharearn, Y.; Ho, C. Effect of Incisor Angulation on Overjet and Overbite in Class II Camouflage Treatment. A typodont study. Angle Orthod. 2007, 77, 1011–1018. [Google Scholar] [CrossRef]
- Zecca, P.A.; Fastuca, R.; Beretta, M.; Caprioglio, A.; Macchi, A. Correlation Assessment between Three-Dimensional Facial Soft Tissue Scan and Lateral Cephalometric Radiography in Orthodontic Diagnosis. Int. J. Dent. 2016, 2016, 1473918. [Google Scholar] [CrossRef]
- Janson, G.; Mendes, L.M.; Junqueira, C.H.; Garib, D.G. Soft-tissue changes in Class II malocclusion patients treated with extractions: A systematic review. Eur. J. Orthod. 2016, 38, 631–637. [Google Scholar] [CrossRef]
- Konstantonis, D.; Vasileiou, D.; Papageorgiou, S.N.; Eliades, T. Soft tissue changes following extraction vs. nonextraction orthodontic fixed appliance treatment: A systematic review and meta-analysis. Eur. J. Oral Sci. 2018, 126, 167–179. [Google Scholar] [CrossRef]
- Kim, K.; Choi, S.H.; Choi, E.H.; Choi, Y.J.; Hwang, C.J.; Cha, J.Y. Unpredictability of soft tissue changes after camouflage treatment of Class II division 1 malocclusion with maximum anterior retraction using miniscrews. Angle Orthod. 2017, 87, 230–238. [Google Scholar] [CrossRef]


{kind=link}
| Measurements T0 | U6 | U4 | p | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Soft tissue | |||||
| ULip-E Plane (mm) | −0.83 | 2.23 | −1.59 | 2.59 | 0.239 |
| LLip-E Plane (mm) | −0.11 | 2.33 | −0.99 | 2.78 | 0.2 |
| Skeletal | |||||
| SNA (°) | 83.04 | 3.16 | 81.53 | 3.83 | 0.108 |
| SNB (°) | 75.58 | 2.83 | 76.97 | 2.88 | 0.078 |
| ANB (°) | 7.47 | 1.84 | 4.53 | 2.40 | <0.001 * |
| SN^PP (°) | 5.49 | 2.73 | 5.95 | 2.90 | 0.549 |
| SN^GoGn (°) | 33.27 | 1.84 | 29.98 | 3.52 | <0.001 * |
| PTV-A point (mm) | 50.37 | 2.80 | 48.13 | 3.44 | 0.009 * |
| PTV-B point (mm) | 39.74 | 4.55 | 41.49 | 3.87 | 0.143 |
| ANS Menton (mm) | 66.54 | 3.41 | 63.74 | 4.28 | 0.008 * |
| Occlusal plane | |||||
| SN^OP (°) | 19.72 | 3.53 | 18.27 | 3.91 | 0.152 |
| OP^GoGn (°) | 13.56 | 3.23 | 11.69 | 2.70 | 0.029 * |
| Dental-angular | |||||
| SN^maxillary incisor (°) | 105.72 | 6.25 | 105.51 | 8.36 | 0.913 |
| SN^maxillary second molar (°) | 60.92 | 5.73 | 61.40 | 6.77 | 0.776 |
| Dental-linear | |||||
| PTV-maxillary incisor centroid (mm) | 52.69 | 3.76 | 51.44 | 3.84 | 0.229 |
| PTV-maxillary second molar centroid (mm) | 10.44 | 3.01 | 10.40 | 2.75 | 0.953 |
| PP-maxillary incisor tip (mm) | 28.04 | 1.74 | 27.43 | 3.00 | 0.331 |
| PP-maxillary second molar centroid (mm) | 12.69 | 2.65 | 12.00 | 6.61 | 0.575 |
| Overjet (mm) | 7.75 | 1.63 | 5.82 | 1.73 | <0.001 * |
| Overbite (mm) | 1.97 | 2.61 | 2.20 | 1.76 | 0.727 |
| Cephalometric Variables U4 | T0 | T1 | p | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Soft tissue | |||||
| ULip-E Plane (mm) | −1.59 | 2.59 | −3.52 | 1.96 | <0.001 * |
| LLip-E Plane (mm) | −0.99 | 2.78 | −2.60 | 1.61 | <0.001 * |
| Skeletal | |||||
| SNA (°) | 81.53 | 3.83 | 80.06 | 3.67 | <0.001 * |
| SNB (°) | 76.97 | 2.88 | 76.61 | 2.76 | 0.13 |
| ANB (°) | 4.53 | 2.40 | 3.45 | 2.52 | 0.02 * |
| SN^PP (°) | 5.95 | 2.90 | 6.18 | 3.05 | 0.40 |
| SN^GoGn (°) | 29.98 | 3.52 | 30.30 | 2.91 | 0.53 |
| PTV-A point (mm) | 48.13 | 3.44 | 47.96 | 3.94 | 0.65 |
| PTV-B point (mm) | 41.49 | 3.87 | 41.77 | 4.60 | 0.60 |
| ANS Menton (mm) | 63.74 | 4.28 | 67.00 | 4.94 | <0.001 * |
| Occlusal plane | |||||
| SN^OP (°) | 18.27 | 3.91 | 18.89 | 3.91 | 0.25 |
| OP^GoGn (°) | 11.69 | 2.70 | 11.42 | 2.73 | 0.54 |
| Dental-angular | |||||
| SN^maxillary incisor (°) | 105.51 | 8.36 | 102.35 | 5.68 | 0.12 |
| SN^maxillary second molar (°) | 61.40 | 6.77 | 70.12 | 4.64 | <0.001 * |
| Dental-linear | |||||
| PTV-maxillary incisor centroid (mm) | 51.44 | 3.84 | 49.04 | 3.91 | <0.001 * |
| PTV-maxillary second molar centroid (mm) | 10.40 | 2.75 | 14.05 | 3.48 | <0.001 * |
| PP-maxillary incisor tip (mm) | 27.43 | 3.00 | 27.64 | 2.75 | 0.64 |
| PP-maxillary second molar centroid (mm) | 12.00 | 6.61 | 16.00 | 2.82 | 0.01 * |
| Overjet (mm) | 5.82 | 1.73 | 2.55 | 0.93 | <0.001 * |
| Overbite (mm) | 2.20 | 1.76 | 0.24 | 0.84 | <0.001 * |
| Cephalometric Variables U6 | T0 | T1 | p | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Soft tissue | |||||
| ULip-E Plane (mm) | −0.83 | 2.23 | −3.81 | 2.21 | <0.001 * |
| LLip-E Plane (mm) | −0.11 | 2.33 | −2.06 | 2.32 | <0.001 * |
| Skeletal | |||||
| SNA (°) | 83.04 | 3.16 | 80.70 | 3.50 | <0.001 * |
| SNB (°) | 75.58 | 2.83 | 75.18 | 2.90 | 0.08 |
| ANB (°) | 7.47 | 1.84 | 5.52 | 2.01 | <0.001 * |
| SN^PP (°) | 5.49 | 2.73 | 5.58 | 3.14 | 0.77 |
| SN^GoGn (°) | 33.27 | 1.84 | 34.03 | 2.66 | 0.02 * |
| PTV-A point (mm) | 50.37 | 2.80 | 49.59 | 2.93 | 0.04 * |
| PTV-B point (mm) | 39.74 | 4.55 | 39.71 | 4.48 | 0.94 |
| ANS Menton (mm) | 66.54 | 3.41 | 70.74 | 4.19 | <0.001 * |
| Occlusal plane | |||||
| SN^OP (°) | 19.72 | 3.53 | 21.24 | 3.82 | <0.001 * |
| OP^GoGn (°) | 13.56 | 3.23 | 12.79 | 3.69 | 0.12 |
| Dental-angular | |||||
| SN^maxillary incisor (°) | 105.72 | 6.25 | 102.95 | 4.50 | 0.01 * |
| SN^maxillary second molar (°) | 60.92 | 5.73 | 70.49 | 5.51 | <0.001 * |
| Dental-linear | |||||
| PTV-maxillary incisor centroid (mm) | 52.69 | 3.76 | 50.00 | 3.24 | <0.001 * |
| PTV-maxillary second molar centroid (mm) | 10.44 | 3.01 | 17.10 | 5.74 | <0.001 * |
| PP-maxillary incisor tip (mm) | 28.04 | 1.74 | 29.13 | 1.95 | <0.001 * |
| PP-maxillary second molar centroid (mm) | 12.69 | 2.65 | 15.89 | 2.37 | <0.001 * |
| Overjet (mm) | 7.75 | 1.63 | 2.89 | 0.78 | <0.001 * |
| Overbite (mm) | 1.97 | 2.61 | 0.42 | 0.87 | <0.001 * |
| Measurements T1 | U6 | U4 | p | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Soft tissue | |||||
| ULip-E Plane (mm) | −2.98 | 1.65 | −1.93 | 1.57 | 0.021 * |
| LLip-E Plane (mm) | −1.95 | 1.91 | −1.61 | 2.31 | 0.551 |
| Skeletal | |||||
| SNA (°) | −2.34 | 1.95 | −1.47 | 1.91 | 0.102 |
| SNB (°) | −0.39 | 1.34 | −0.36 | 1.03 | 0.912 |
| ANB (°) | −1.95 | 1.65 | −1.08 | 1.98 | 0.076 |
| SN^PP (°) | 0.09 | 1.79 | 0.22 | 1.20 | 0.756 |
| SN^GoGn (°) | 0.76 | 1.99 | 0.33 | 2.33 | 0.458 |
| PTV-A point (mm) | −0.77 | 2.30 | −0.17 | 1.66 | 0.291 |
| PTV-B point (mm) | −0.04 | 3.25 | 0.28 | 2.38 | 0.698 |
| ANS Menton (mm) | 4.20 | 2.30 | 3.26 | 2.75 | 0.165 |
| Occlusal plane | |||||
| SN^OP (°) | 1.52 | 2.82 | 0.61 | 2.38 | 0.216 |
| OP^GoGn (°) | −0.76 | 2.98 | −0.27 | 1.96 | 0.496 |
| Dental-angular | |||||
| SN^maxillary incisor (°) | −2.77 | 6.36 | −3.16 | 8.89 | 0.849 |
| SN^maxillary second molar (°) | 9.57 | 6.95 | 8.72 | 6.69 | 0.653 |
| Dental-linear | |||||
| PTV-maxillary incisor centroid (mm) | −2.70 | 2.58 | −2.40 | 2.04 | 0.651 |
| PTV-maxillary second molar centroid (mm) | 6.66 | 5.00 | 3.66 | 2.20 | 0.012 * |
| PP-maxillary incisor tip (mm) | 1.09 | 1.52 | 0.20 | 2.00 | 0.061 * |
| PP-maxillary second molar centroid (mm) | 3.20 | 2.86 | 4.00 | 6.07 | 0.493 |
| Overjet (mm) | −4.86 | 1.62 | −3.27 | 1.90 | 0.001 * |
| Overbite (mm) | −1.55 | 2.41 | −1.96 | 1.59 | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Booij, J.W.; Serafin, M.; Fastuca, R.; Kuijpers-Jagtman, A.M.; Caprioglio, A. Skeletal, Dental and Soft Tissue Cephalometric Changes after Orthodontic Treatment of Dental Class II Malocclusion with Maxillary First Molar or First Premolar Extractions. J. Clin. Med. 2022, 11, 3170. https://doi.org/10.3390/jcm11113170
Booij JW, Serafin M, Fastuca R, Kuijpers-Jagtman AM, Caprioglio A. Skeletal, Dental and Soft Tissue Cephalometric Changes after Orthodontic Treatment of Dental Class II Malocclusion with Maxillary First Molar or First Premolar Extractions. Journal of Clinical Medicine. 2022; 11(11):3170. https://doi.org/10.3390/jcm11113170
Chicago/Turabian StyleBooij, Johan Willem, Marco Serafin, Rosamaria Fastuca, Anne Marie Kuijpers-Jagtman, and Alberto Caprioglio. 2022. "Skeletal, Dental and Soft Tissue Cephalometric Changes after Orthodontic Treatment of Dental Class II Malocclusion with Maxillary First Molar or First Premolar Extractions" Journal of Clinical Medicine 11, no. 11: 3170. https://doi.org/10.3390/jcm11113170
APA StyleBooij, J. W., Serafin, M., Fastuca, R., Kuijpers-Jagtman, A. M., & Caprioglio, A. (2022). Skeletal, Dental and Soft Tissue Cephalometric Changes after Orthodontic Treatment of Dental Class II Malocclusion with Maxillary First Molar or First Premolar Extractions. Journal of Clinical Medicine, 11(11), 3170. https://doi.org/10.3390/jcm11113170