
Regional Citrate Anticoagulation and Systemic Anticoagulation during Pediatric Continuous Renal Replacement Therapy: A Systematic Literature Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
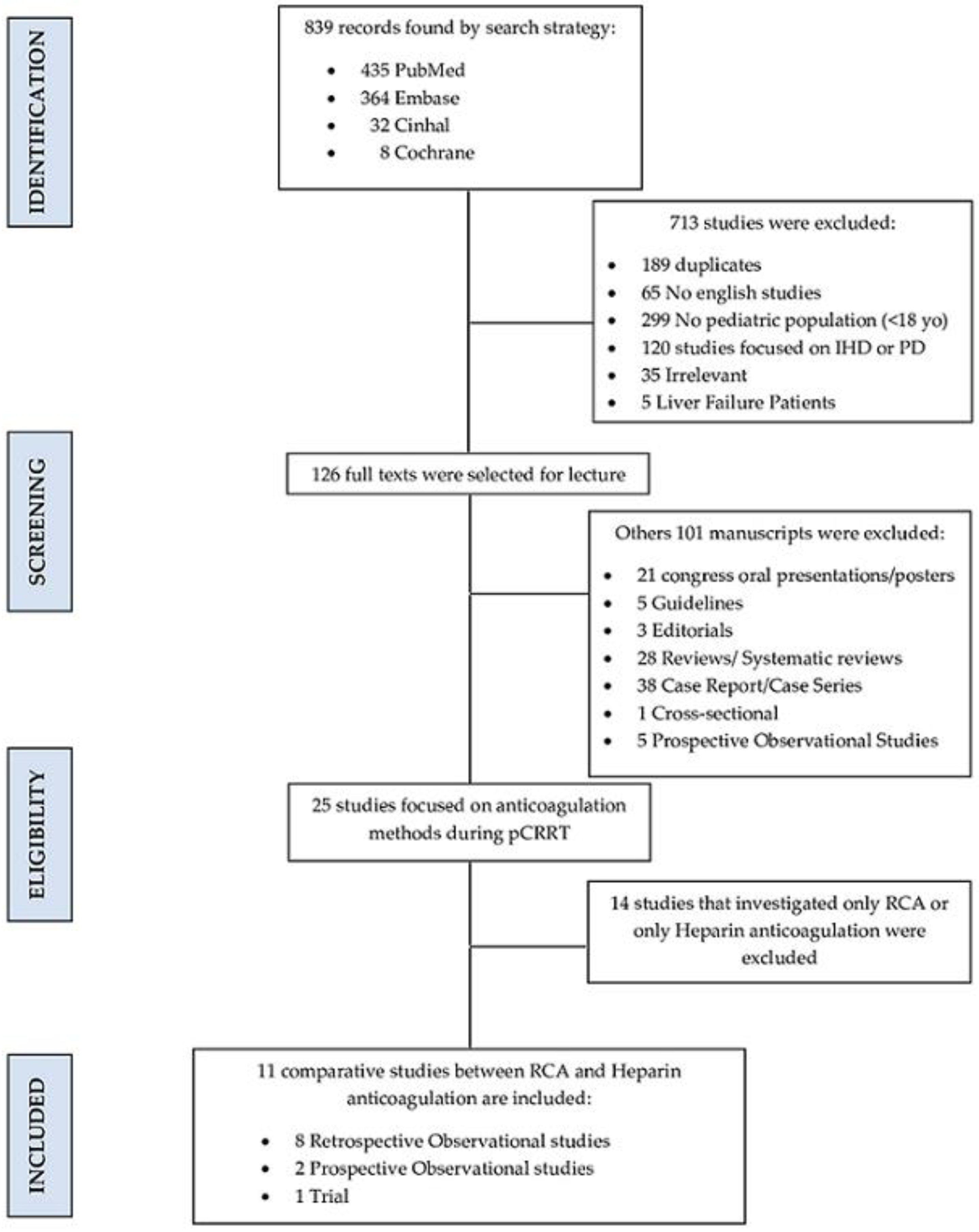
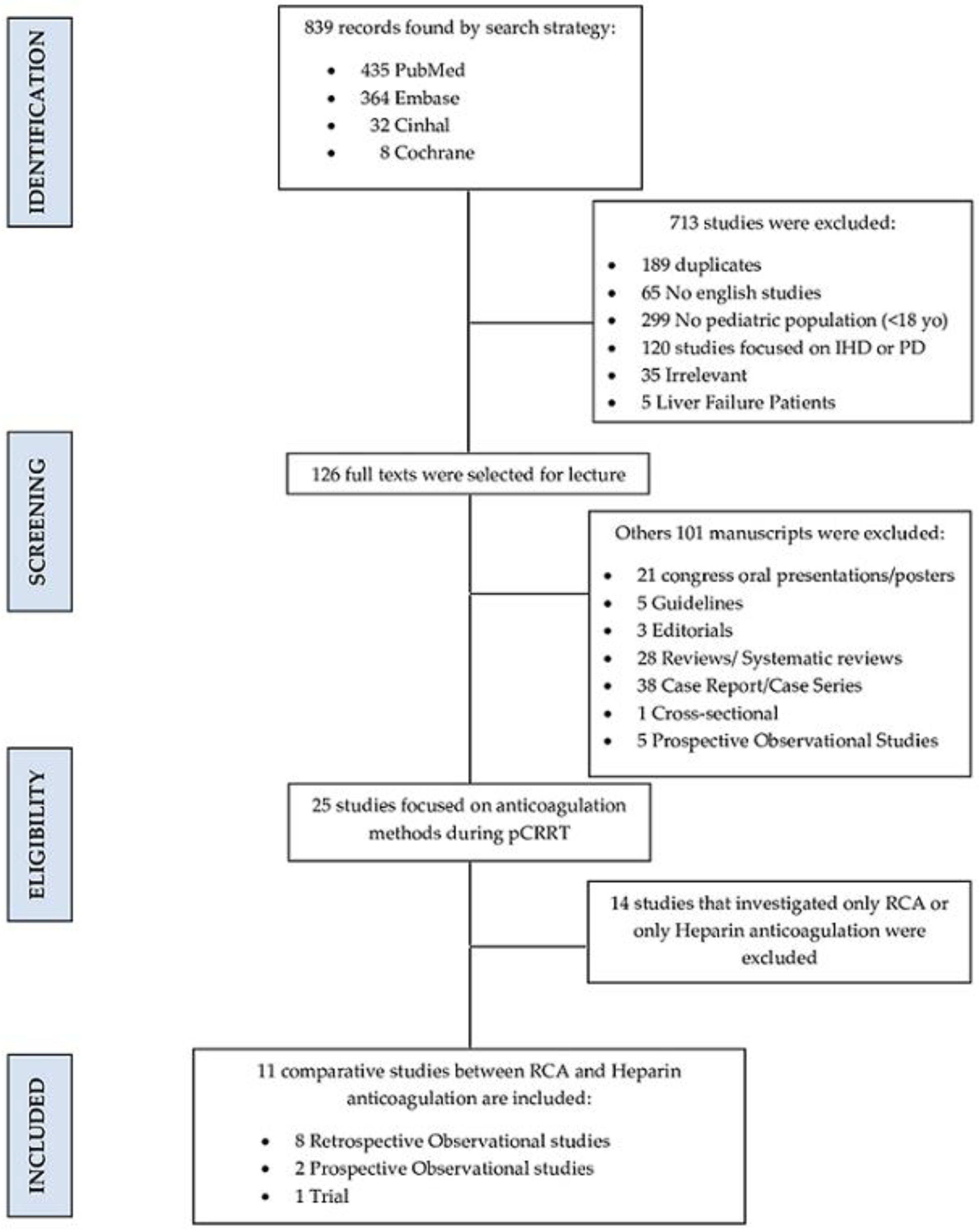
2. Materials and Methods
3. Results
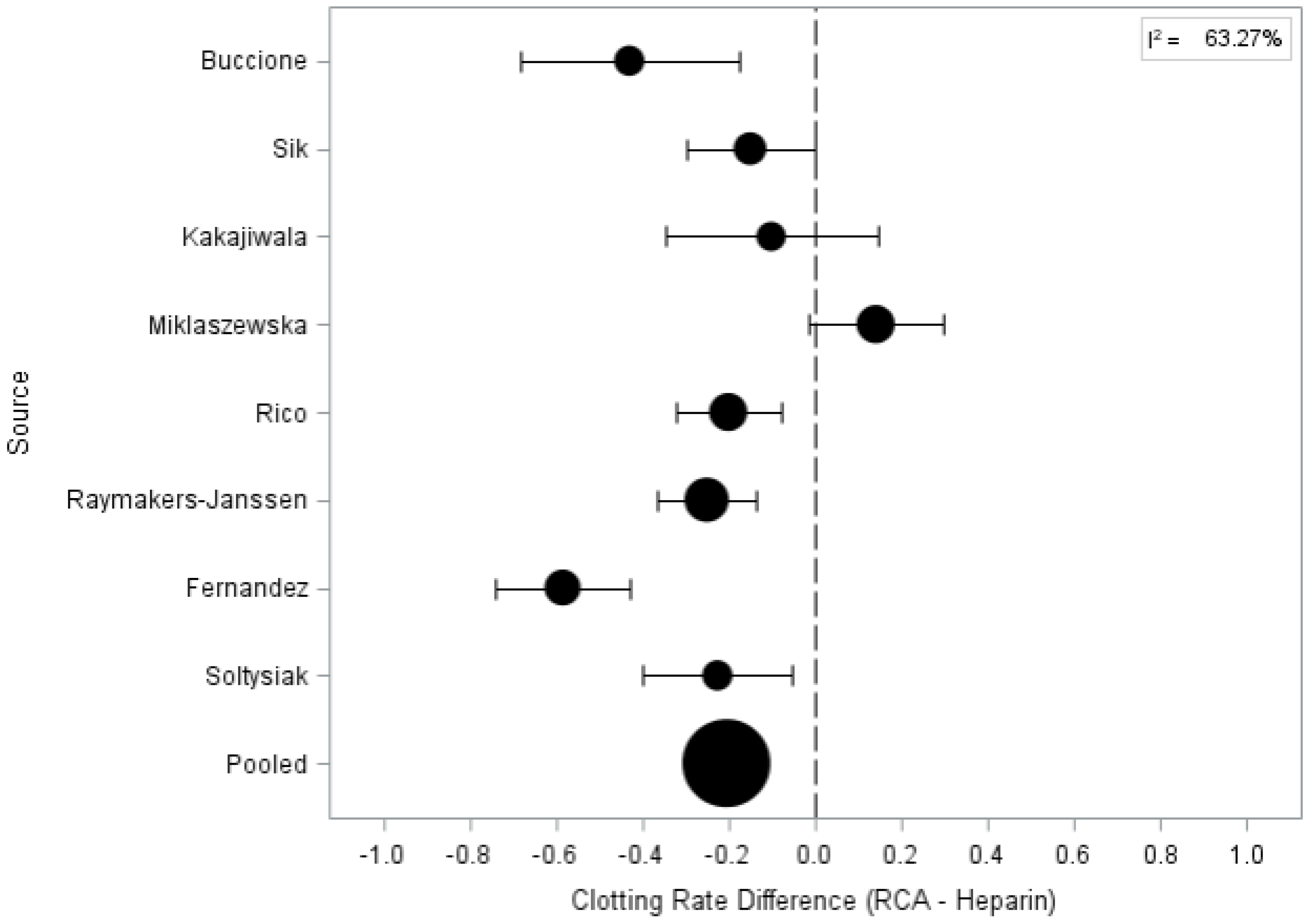
3.1. Circuit Life and Clotting Rate
3.2. Complications
3.3. Survival
3.4. Dialysis Targets
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kellum, J.A. Diagnostic Criteria for Acute Kidney Injury. Crit. Care Clin. 2015, 31, 621–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Fry, A.C. Management of Acute Renal Failure. Postgrad. Med. J. 2006, 82, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Blanco, F.C.; Ortega, G.; Qureshi, F.G. Renal Replacement Therapy in Children. Semin. Pediatr. Surg. 2015, 24, 25–31. [Google Scholar] [CrossRef]
- Symons, J.M.; Chua, A.N.; Somers, M.J.; Baum, M.A.; Bunchman, T.E.; Benfield, M.R.; Brophy, P.D.; Blowey, D.; Fortenberry, J.D.; Chand, D.; et al. Demographic Characteristics of Pediatric Continuous Renal Replacement Therapy: A Report of the Prospective Pediatric Continuous Renal Replacement Therapy Registry. Clin. J. Am. Soc. Nephrol. 2007, 2, 732–738. [Google Scholar] [CrossRef] [PubMed]
- del Castillo, J.; López-Herce, J.; Cidoncha, E.; Urbano, J.; Mencía, S.; Santiago, M.J.; Bellón, J.M. Circuit Life Span in Critically Ill Children on Continuous Renal Replacement Treatment: A Prospective Observational Evaluation Study. Crit. Care 2008, 12, R93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, T.K.; Neumayr, T.; Geile, K.; Doctor, A.; Hmeil, P. Citrate Anticoagulation during Continuous Renal Replacement Therapy in Pediatric Critical Care. Pediatr. Crit. Care Med. 2014, 15, 471–485. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. For the CONSORT Group CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Wang, H.; Wu, Z.; Jin, M.; Chen, Y.; Li, J.; Wei, Q.; Tao, S.; Zeng, Q. Continuous Renal-Replacement Therapy in Critically Ill Children: Practice Changes and Association with Outcome. Pediatr. Crit. Care Med. 2021, 22, E605–E612. [Google Scholar] [CrossRef] [PubMed]
- Buccione, E.; Guzzi, F.; Colosimo, D.; Tedesco, B.; Romagnoli, S.; Ricci, Z.; L’Erario, M.; Villa, G. Continuous Renal Replacement Therapy in Critically Ill Children in the Pediatric Intensive Care Unit: A Retrospective Analysis of Real-Life Prescriptions, Complications, and Outcomes. Front. Pediatr. 2021, 9, 696798. [Google Scholar] [CrossRef] [PubMed]
- Cortina, G.; McRae, R.; Chiletti, R.; Butt, W. The Effect of Patient- and Treatment-Related Factors on Circuit Lifespan During Continuous Renal Replacement Therapy in Critically Ill Children. Pediatr. Crit. Care Med. 2020, 21, 578–585. [Google Scholar] [CrossRef]
- Sık, G.; Demirbuga, A.; Annayev, A.; Citak, A. Regional Citrate versus Systemic Heparin Anticoagulation for Continuous Renal Replacement Therapy in Critically Ill Children. Int. J. Artif. Organs 2020, 43, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Kakajiwala, A.; Jemielita, T.; Hughes, J.Z.; Windt, K.; Denburg, M.; Goldstein, S.L.; Laskin, B. Membrane Pressures Predict Clotting of Pediatric Continuous Renal Replacement Therapy Circuits. Pediatr. Nephrol. 2017, 32, 1251–1261. [Google Scholar] [CrossRef]
- Miklaszewska, M.; Korohoda, P.; Zachwieja, K.; Kobylarz, K.; Stefanidis, C.J.; Sobczak, A.; Drozdz, D. Filter Size Not the Anticoagulation Method Is the Decisive Factor in Continuous Renal Replacement Therapy Circuit Survival. Kidney Blood Press. Res. 2017, 42, 327–337. [Google Scholar] [CrossRef]
- Rico, M.P.; Fernández Sarmiento, J.; Rojas Velasquez, A.M.; González Chaparro, L.S.; Gastelbondo Amaya, R.; Mulett Hoyos, H.; Tibaduiza, D.; Quintero Gómez, A.M. Regional Citrate Anticoagulation for Continuous Renal Replacement Therapy in Children. Pediatr. Nephrol. 2017, 32, 703–711. [Google Scholar] [CrossRef]
- Raymakers-Janssen, P.A.M.A.; Lilien, M.; van Kessel, I.A.; Veldhoen, E.S.; Wösten-van Asperen, R.M.; van Gestel, J.P.J. Citrate versus Heparin Anticoagulation in Continuous Renal Replacement Therapy in Small Children. Pediatr. Nephrol. 2017, 32, 1971–1978. [Google Scholar] [CrossRef]
- Zaoral, T.; Hladík, M.; Zapletalová, J.; Trávníček, B.; Gelnarová, E. Circuit Lifetime with Citrate Versus Heparin in Pediatric Continuous Venovenous Hemodialysis. Pediatr. Crit. Care Med. 2016, 17, e399–e405. [Google Scholar] [CrossRef]
- Fernández, S.N.; Santiago, M.J.; López-Herce, J.; García, M.; Del Castillo, J.; Alcaraz, A.J.; Bellón, J.M. Citrate Anticoagulation for CRRT in Children: Comparison with Heparin. Biomed Res. Int. 2014, 2014, 786301. [Google Scholar] [CrossRef]
- Soltysiak, J.; Warzywoda, A.; Kociński, B.; Ostalska-Nowicka, D.; Benedyk, A.; Silska-Dittmar, M.; Zachwieja, J. Citrate Anticoagulation for Continuous Renal Replacement Therapy in Small Children. Pediatr. Nephrol. 2014, 29, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Hongying, N. Efficacy and Safety of Regional Citrate Anticoagulation in Critically Ill Patients Undergoing Continuous Renal Replacement Therapy. Intensive Care Med. 2012, 38, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Garzotto, F.; Zaccaria, M.; Vidal, E.; Ricci, Z.; Lorenzin, A.; Neri, M.; Murer, L.; Nalesso, F.; Ruggeri, A.; Ronco, C. Choice of Catheter Size for Infants in Continuous Renal Replacement Therapy: Bigger Is Not Always Better. Pediatr. Crit. Care Med. 2019, 20, e170–e179. [Google Scholar] [CrossRef] [PubMed]
- Raina, R.; Agrawal, N.; Kusumi, K.; Pandey, A.; Tibrewal, A.; Botsch, A. A Meta-Analysis of Extracorporeal Anticoagulants in Pediatric Continuous Kidney Replacement Therapy. J. Intensive Care Med. 2022, 37, 0885066621992751. [Google Scholar] [CrossRef] [PubMed]
- Garzotto, F.; Zanella, M.; Ronco, C. The Evolution of Pediatric Continuous Renal Replacement Therapy. Nephron Clin. Pract. 2014, 127, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, S.M.; Alexander, S.R. Continuous Renal Replacement Therapy in Children. Pediatr. Nephrol. 2012, 27, 2007–2016. [Google Scholar] [CrossRef] [PubMed]
- John, J.C.; Taha, S.; Bunchman, T.E. Basics of Continuous Renal Replacement Therapy in Pediatrics. Kidney Res. Clin. Pract. 2019, 38, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Bunchman, T.E.; Donckerwolcke, R.A. Continuous Arterial-Venous Diahemofiltration and Continuous Veno-Venous Diahemofiltration in Infants and Children. Pediatr. Nephrol. 1994, 8, 96–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunchman, T.E.; Maxvold, N.J.; Brophy, P.D. Pediatric Convective Hemofiltration: Normocarb Replacement Fluid and Citrate Anticoagulation. Am. J. Kidney Dis. 2003, 42, 1248–1252. [Google Scholar] [CrossRef]
- Wu, M.-Y.; Hsu, Y.-H.; Bai, C.-H.; Lin, Y.-F.; Wu, C.-H.; Tam, K.-W. Regional Citrate Versus Heparin Anticoagulation for Continuous Renal Replacement Therapy: A Meta-Analysis of Randomized Controlled Trials. Am. J. Kidney Dis. 2012, 59, 810–818. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Population | Intervention | Comparison | Outcome | Study Types |
|---|---|---|---|---|
| Patients < 18 years old admitted in PICU undergoing continuous renal replacement therapy | Use of anticoagulation during CRRT (systemic with heparin or regional citrate anticoagulation) | Heparin vs. RCA | Circuit life (CL) OR clotting rate; Complications (bleeding, blood transfusion rate, electrolyte OR metabolic disturbances); Survival | Prospective and retrospective observational studies; randomized clinical trials |
| Source | Study Design | Country | Mean Age (Months) | Sample Size (N) (Citrate) | Sample Size (N) (Heparin) | Outcomes |
|---|---|---|---|---|---|---|
| Chen et al., 2021 [12] | Retrospective Observational | China | 48 | 107 | 49 | Reduced mortality rate with RCA at logistic regression analysis |
| Buccione et al., 2021 [13] | Retrospective Observational | Italy | 48 | 23 | 23 | RCA as a protective factor for clotting at multivariate Cox regression analysis |
| Cortina et al., 2020 [14] | Retrospective Observational | Australia | 61.2 | 61 | 161 | No statistical difference in CL between heparin and RCA at multivariate logistic regression analysis |
| Sik et al., 2019 [15] | Retrospective Observational | Turkey | 72 | 19 | 26 | Median CL was significantly longer for RCA at univariate regression analysis. |
| Kakajiwala et al., 2017 [16] | Retrospective Observational | United States of America | 141.6 | 26 | 26 | Lower risk of clotting with Heparin anticoagulation at univariate Cox regression analysis. |
| Miklaszewska et al., 2017 [17] | Retrospective Observational | Poland | 116.7 | 8 | 32 | No differences in the survival rate between the groups |
| Rico et al., 2017 [18] | Retrospective Observational | Colombia | 1 to 216 | 17 | 15 | Median CL prolonged with RCA at univariate and bivariate regression analysis. |
| Raymakers-Janssen et al., 2017 [19] | Prospective Observational | Netherlands | 15 | 14 | 6 | Median CL was higher with RCA at log-rank |
| Zaoral et al., 2016 [20] | Crossover Trial | Czech Republic | 84 | 63 | 63 | RCA prolongs CL at the Wilcoxon paired test |
| Fernandez et al., 2014 [21] | Prospective Observational | Spain | 34.5 | 12 | 24 | Prolonged CL with RCA at Kaplan–Meier survival analysis |
| Soltysiak et al., 2014 [22] | Retrospective Observational | Poland | 19.7 | 16 | 14 | Higher CL was observed with RCA at Kaplan–Meier survival analysis. |
| Source | N Sessions | Circuit Life (h) | Clotting Rate (%) | |||
|---|---|---|---|---|---|---|
| RCA | Heparin | RCA | Heparin | RCA | Heparin | |
| Buccione et al., 2021 [13] | 11 | 72 | N/A | N/A | 18.2 | 60.6 |
| Cortina et al., 2020 [14] | 132 | 355 | 29.3 [25.8–33.1] | 23.8 [19.5–29.2] | N/A | N/A |
| Sik et al., 2019 [15] | 44 | 57 | 53 [40–70] | 40.25 [22.75–53.5] | 11.36 | 26.31 |
| Kakajiwala et al., 2017 [16] | 22 | 51 | N/A | N/A | 39.2 | 51 |
| Miklaszewska et al., 2017 [17] (HF20/ST60/ST100) | 36 | 15 | 41 ± 25.9 | 33.3 ± 23.8 | 43.9 | 29.8 |
| 15 | 46 | 57 ± 23.5 | 53.1 ± 23.8 | |||
| 15 | 23 | 69.7 ± 8.2 | 57.2 ± 23.3 | |||
| Rico et al., 2017 [18] | 80 | 70 | 72 [48–96] | 18 [12–24] | 70 | 90 |
| Raymakers-Janssen et al., 2017 [19] | 105 | 121 | 45.2 [37.5–52.8] | 21 [14.5–27.5] | 17.1 | 42 |
| Zaoral et al., 2016 [20] | 111 | 111 | 41 [35–51.75] | 36 [31–40] | N/A | N/A |
| Fernandez et al., 2014 [21] | 34 | 96 | 48 [31.0–93.7] | 31.0 [15.5–71.0] | 18.8 | 76.4 |
| Soltysiak et al., 2014 [22] | 43 | 41 | 58.04 ± 51.18 | 37.64 ± 32.51 | 11.63 | 34.15 |
| Source | Clotting Rate Difference | 95% CI |
|---|---|---|
| Buccione | −0.429 | 0.684–0.175 |
| Sik | −0.150 | 0.297–0.002 |
| Kakajiwala | −0.101 | 0.348–0.146 |
| Miklaszewska | 0.142 | −0.013–0.296 |
| Rico | −0.200 | 0.323–0.077 |
| Raymakers-Janssen | −0.250 | 0.364–0.136 |
| Fernandez | −0.584 | 0.738–0.430 |
| Soltysiak | −0.225 | 0.399–0.051 |
| POOLED | −0.204 | 0.265–0.144 |
| Complications | p-Value | Complication | ||
|---|---|---|---|---|
| Source | RCA | Heparin | ||
| Sik et al., 2019 [15] | 7.01% | 6.41% | 0.956 | Metabolic alkalosis |
| 12.28% | 2.56% | <0.05 | Hypocalcemia | |
| 14.03% | 10.25% | <0.05 | Hypernatremia | |
| 0.8 [0.3–2.0] | 1.65 [0.5–2.38] | 0.32 | Units of RBC transfused | |
| Rico et al., 2017 [18] | 30% | 32.6% | 0.605 | Severe bleeding events |
| Raymakers-Janssen et al., 2017 [19] | 3 [2.0–5.0] | 6.5 [1.5–23.8] | 0.12 | Units of RBC transfused |
| Zaoral et al., 2016 [20] | 0.17 [0.0–1.0] | 0.36 [0.0–2.0] | 0.003 | Units of RBC transfused |
| Fernandez et al., 2014 [21] | 45.5% | 0% | <0.01 | Hypochloremia |
| 27.3% | 0% | 0.045 | Hypomagnesemia | |
| 0% | 27.8 | 0.06 | Hypophosphatemia | |
| Soltysiak et al., 2014 [22] | 18.75% | 0% | N/A | Hyponatremia |
| Soltysiak et al., 2014 [22] | 18.75% | 14.3% | N/A | Hypernatremia |
| 12.5% | 21.4% | N/A | Hyperkalemia | |
| 62.5% | 28.6% | N/A | Hypokalemia | |
| 43.75% | 64.3% | N/A | Hypercalcemia | |
| 43.75% | 0% | N/A | Hypocalcemia | |
| 43.75% | 42.9% | N/A | Metabolic acidosis | |
| 25% | 14.3% | N/A | Metabolic alkalosis | |
| Source | Time-Point | Survival Rate (%) | p-Value | |
|---|---|---|---|---|
| RCA | Heparin | |||
| Chen et al., 2021 [12] | PICU discharge | 53.2 | 34.7 | 0.031 * |
| Sik et al., 2019 [15] | PICU discharge | 68.42 | 69.23 | 0.954 |
| Miklaszewska et al., 2017 [17] | PICU discharge | 62.5 | 34.4 | N/A |
| Rico et al., 2017 [18] | PICU discharge | 83.3 | 81.2 | 0.859 |
| Raymakers-Janssen et al., 2017 [19] | PICU discharge | 50 | 50 | N/A |
| Fernandez et al., 2014 [21] | PICU discharge | 25 | 25 | N/A |
| Soltysiak et al., 2014 [22] | Hospital discharge | 37.5 | 14.3 | N/A |
| Qb (mL/min) | Dialysate (mL/h) | Heparin Dose (IU/kg/h) | Net Ultrafiltration (mL/h) | Replacement (mL/min) | Citrate (mmol/L) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Source | RCA | Heparin | RCA | Heparin | RCA | Heparin | RCA | Heparin | RCA | Heparin | RCA | Heparin |
| Buccione et al., 2021 [13] | 60 (40–80) | 60 (40–80) | 400 (200–600) | 400 (200–600) | N/A | 13.9 | 40 (25–70) | 40 (25–70) | 200 (50–400) | 200 (50–400) | N/A | N/A |
| Cortina et al., 2020 [14] | 96 (16–400) | 96 (16–400) | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Sik et al., 2019 [15] | 60 (50–80) | 60 (50–80) | 700 (500–900) | 500 (350–800) | N/A | N/A | N/A | N/A | N/A | N/A | 4 (4–5) | N/A |
| Miklaszewska et al., 2017 [17](HF20/ST60/ST100) | 3.5/kg (.5) | 3.5/kg (.5) | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| 2.1/kg (1.5) | 2.1/kg (1.5) | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |||
| 2/kg (.9) | 2/kg (.9) | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |||
| Rico et al., 2017 [18] | 3.4/kg | 3.5/kg | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Zaoral et al., 2016 [20] | 90 (70–100) | 90 (70–100) | 60.34/kg (48.5–118.5) | 53.57/kg (38–85) | N/A | 15 (13.2–17.9) | N/A | N/A | N/A | N/A | N/A | N/A |
| Fernandez et al., 2014 [21] | 3.2/kg (2–3.8) | 5/kg (3.8–5.6) | 325 (50–600) | 300 (140–500) | N/A | 15 (12–25) | 75 (50–97.5) | 60 (50–90) | 50 (0–50) | 300 (140–500) | 2.6 (2.3–2.9) | N/A |
| Soltysiak et al., 2014 [22] | 3.49/kg ± 1.56 | 2.88/kg ± 0.80 | 52.32/kg ± 35.63 | 71.71/kg ± 39.39 | N/A | 17 ± 10 | N/A | N/A | N/A | N/A | 4.05 ± 2.30 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buccione, E.; Bambi, S.; Rasero, L.; Tofani, L.; Piazzini, T.; Della Pelle, C.; El Aoufy, K.; Ricci, Z.; Romagnoli, S.; Villa, G. Regional Citrate Anticoagulation and Systemic Anticoagulation during Pediatric Continuous Renal Replacement Therapy: A Systematic Literature Review. J. Clin. Med. 2022, 11, 3121. https://doi.org/10.3390/jcm11113121
Buccione E, Bambi S, Rasero L, Tofani L, Piazzini T, Della Pelle C, El Aoufy K, Ricci Z, Romagnoli S, Villa G. Regional Citrate Anticoagulation and Systemic Anticoagulation during Pediatric Continuous Renal Replacement Therapy: A Systematic Literature Review. Journal of Clinical Medicine. 2022; 11(11):3121. https://doi.org/10.3390/jcm11113121
Chicago/Turabian StyleBuccione, Emanuele, Stefano Bambi, Laura Rasero, Lorenzo Tofani, Tessa Piazzini, Carlo Della Pelle, Khadija El Aoufy, Zaccaria Ricci, Stefano Romagnoli, and Gianluca Villa. 2022. "Regional Citrate Anticoagulation and Systemic Anticoagulation during Pediatric Continuous Renal Replacement Therapy: A Systematic Literature Review" Journal of Clinical Medicine 11, no. 11: 3121. https://doi.org/10.3390/jcm11113121
APA StyleBuccione, E., Bambi, S., Rasero, L., Tofani, L., Piazzini, T., Della Pelle, C., El Aoufy, K., Ricci, Z., Romagnoli, S., & Villa, G. (2022). Regional Citrate Anticoagulation and Systemic Anticoagulation during Pediatric Continuous Renal Replacement Therapy: A Systematic Literature Review. Journal of Clinical Medicine, 11(11), 3121. https://doi.org/10.3390/jcm11113121