
Ayurveda in Knee Osteoarthritis—Secondary Analyses of a Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology of the Parent RCT
2.2. Statistics
- Model simplification: variables that are not important; i.e., that do not influence a model’s predictions, may be excluded from the model.
- Domain-knowledge-based model validation: identification of the most important variables may be helpful in assessing the validity of the model based on domain knowledge.
- Model exploration: comparison of variables’ importance in different models may help in discovering interrelations between the variables.
3. Results
3.1. Role of Nutritional Supplements in the Primary Outcome in the Ayurveda Group
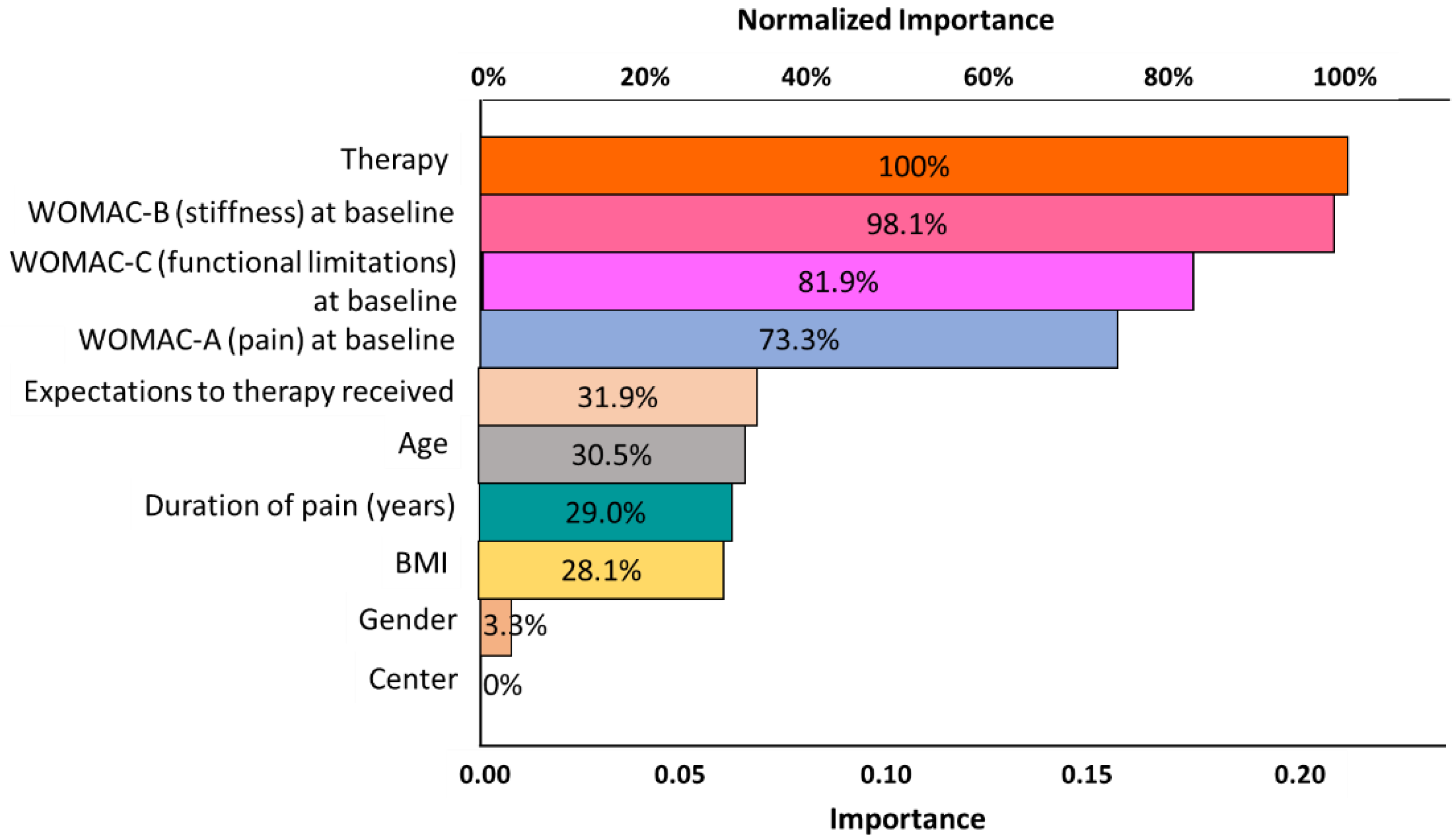
3.2. Importance of Multiple Independent Variables in the Primary Outcome
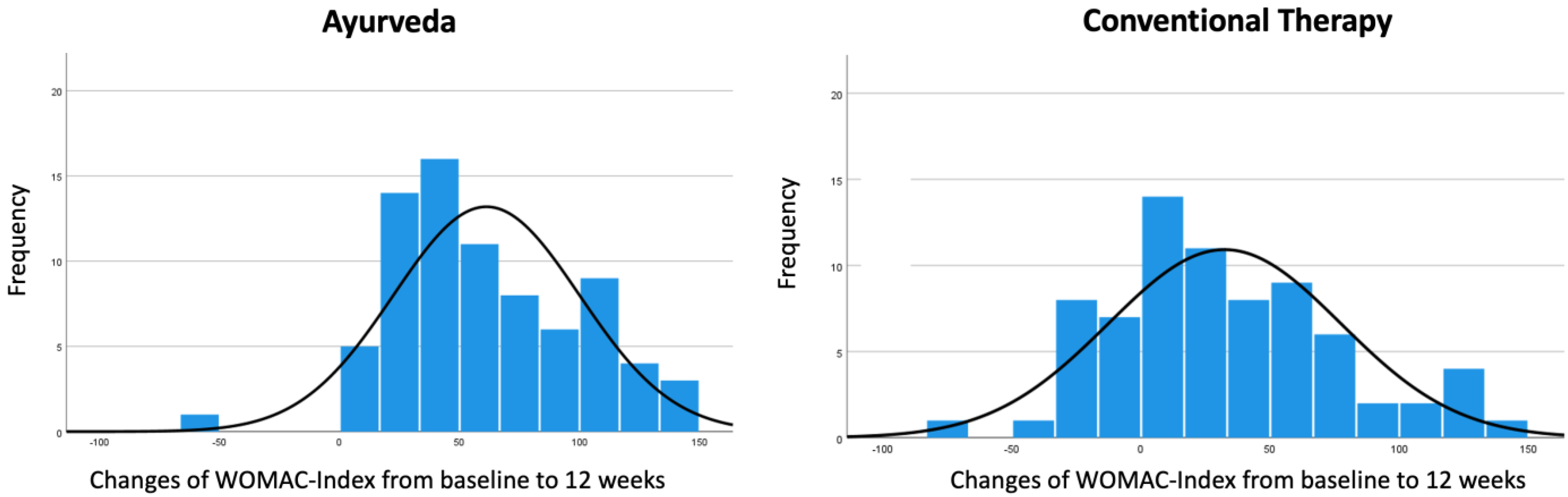
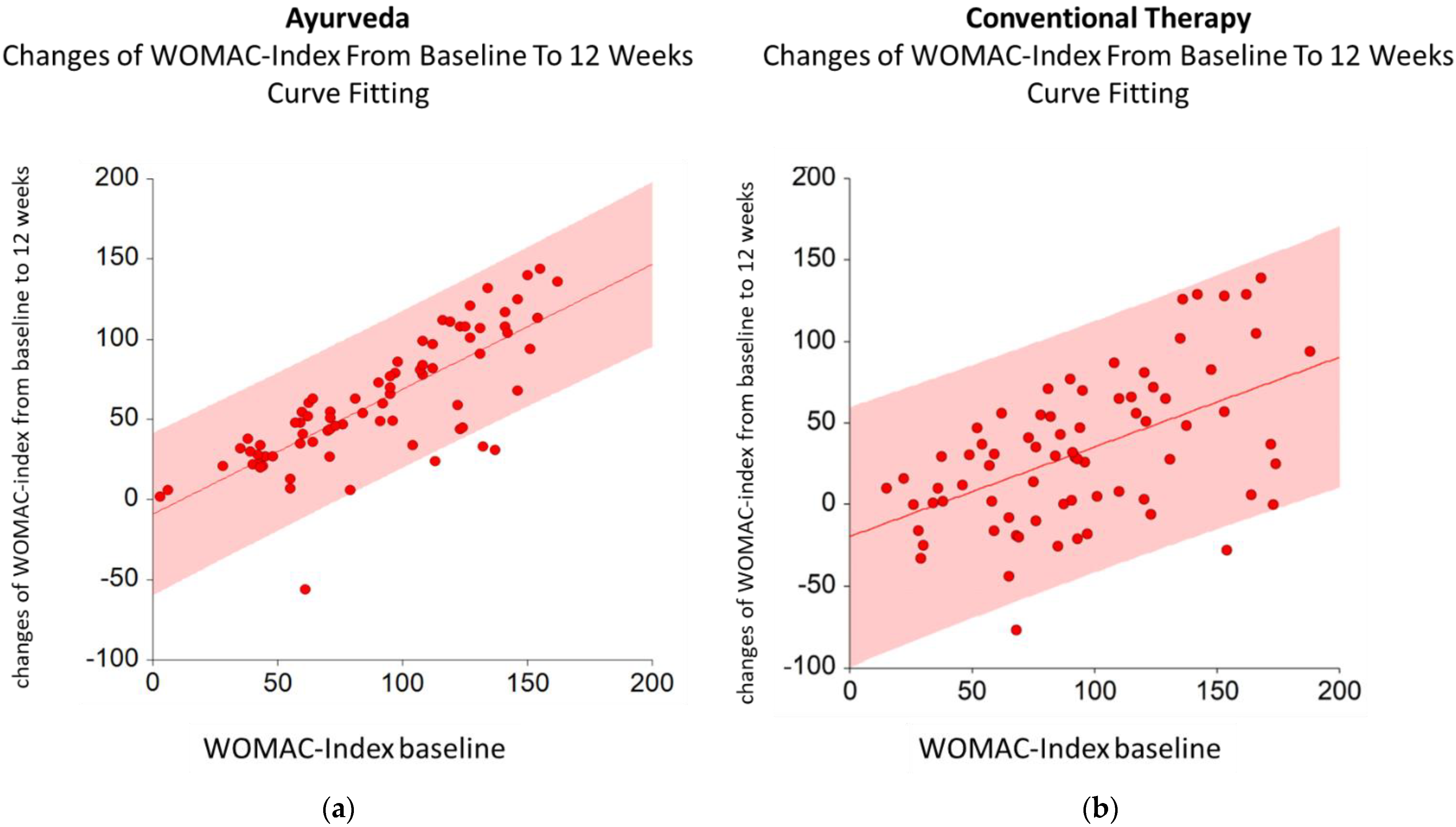
3.3. Significance of the WOMAC Index Subscales in the Therapeutic Effect
- Ayurveda: changes in WOMAC Index from baseline to 12 weeks = −2.30 + 1.03x (WOMAC-C baseline);
- Conventional therapy: changes in WOMAC Index from baseline to 12 weeks = −14.46 + 0.72x (WOMAC-C baseline).
3.4. Prediction of Clinical Improvement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaturvedi, S.; Patwardhan, B. Building bridges for integrative medicine. Lancet Psychiatry 2016, 3, 705–706. [Google Scholar] [CrossRef]
- Morandi, A.; Nambi, A.N.N. An Integrated View of Health and Well-Being—Bridging Indian and Western Knowledge; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Kessler, C.S.; Dhiman, K.S.; Kumar, A.; Ostermann, T.; Gupta, S.; Morandi, A.; Mittwede, M.; Stapelfeldt, E.; Spoo, M.; Icke, K.; et al. Effectiveness of an Ayurveda treatment approach in knee osteoarthritis—A randomized controlled trial. Osteoarthr. Cartil. 2018, 26, 620–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Benchmarks for Training in Traditional/Complementary and Alternative Medicine: Benchmarks for Training in Ayurveda. Available online: https://apps.who.int/iris/handle/10665/44352 (accessed on 26 April 2022).
- AYUSH. General Guidelines for Clinical Evaluation of Ayurvedic Interventions. Available online: https://www.ayush.gov.in/docs/clinical_evaluation.pdf (accessed on 26 April 2022).
- World Health Organization. Legal Status of Traditional Medicine and Complementary/Alternative Medicine: A Worldwide Review. Available online: https://apps.who.int/iris/handle/10665/42452 (accessed on 26 April 2022).
- World Health Organization. WHO Guidelines on Developing Consumer Information on Proper Use of Traditional, Complementary and Alternative Medicine. Available online: https://apps.who.int/iris/handle/10665/42957 (accessed on 26 April 2022).
- World Health Organization. General Guidelines for Methodologies on Research and Evaluation of Traditional Medicine. Available online: https://apps.who.int/iris/handle/10665/66783 (accessed on 26 April 2022).
- World Health Organization. WHO Traditional Medicine Strategy 2014–2023. Available online: http://www.who.int/medicines/publications/traditional/trm_strategy14_23/en/ (accessed on 26 April 2022).
- ADAVED. Ayurveda Dachverband Deutschland—Ayurveda Association Germany. Available online: http://ayurveda-dachverband.de/ (accessed on 26 April 2022).
- DÄGAM. Deutsche Ärztegesellschaft für Ayurveda-Medizin e.V.—German Medical Association for Ayurveda Medicine e.V. Available online: https://www.daegam.de (accessed on 26 April 2022).
- NAMA. National Ayurvedic Medical Association. Available online: http://www.ayurvedanama.org/ (accessed on 26 April 2022).
- AAPNA. Available online: https://www.aapna.org (accessed on 26 April 2022).
- Sujatha, V. Globalisation of South Asian Medicines: Knowledge, Power, Structure and Sustainability. Soc. Cult. South Asia 2020, 6, 7–30. [Google Scholar] [CrossRef]
- Keßler, C.S. Habilitationsschrift—Ayurveda, Yoga, Meditation—Traditionelle Indische Medizin und ihr Bezug zu den fünf Säulen der Naturheilkunde. Available online: https://refubium.fu-berlin.de/bitstream/handle/fub188/27783/Habilitation_Kessler_Bibversion.pdf?sequence=1&isAllowed=y (accessed on 26 April 2022).
- Boon, H.; Verhoef, M.; O’Hara, D.; Findlay, B.; Majid, N. Integrative healthcare: Arriving at a working definition. Altern. Health Med. 2004, 10, 48–56. [Google Scholar]
- Esch, T.; Brinkhaus, B. Neue Definitionen der Integrativen Medizin: Alter Wein in neuen Schläuchen? Complement. Med. Res. 2020, 27, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Caspi, O.; Sechrest, L.; Pitluk, H.C.; Marshall, C.L.; Bell, I.R.; Nichter, M. On the definition of complementary, alternative, and integrative medicine: Societal mega-stereotypes vs. the patients’ perspectives. Altern. Health Med. 2003, 9, 58–62. [Google Scholar]
- Rees, L.; Weil, A. Integrated medicine. Bmj 2001, 322, 119–120. [Google Scholar] [CrossRef]
- WHO. WHO Benchmarks for the Training of Ayurveda. Available online: https://www.who.int/publications/i/item/9789240042711 (accessed on 28 February 2022).
- WHO. WHO Benchmarks for the Practice of Ayurveda. Available online: https://www.who.int/publications/i/item/9789240042674 (accessed on 28 February 2022).
- Modi. Valedictory Address at 6th World Ayurveda Congress by Prime Minister Narendra Modi. J. Ayurveda Integr. Med. 2014, 5, 201–204. [Google Scholar]
- Furst, D.E.; Venkatraman, M.M.; McGann, M.; Manohar, P.R.; Booth-LaForce, C.; Sarin, R.; Sekar, P.G.; Raveendran, K.G.; Mahapatra, A.; Gopinath, J.; et al. Double-blind, randomized, controlled, pilot study comparing classic ayurvedic medicine, methotrexate, and their combination in rheumatoid arthritis. J. Clin. Rheumatol. 2011, 17, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Furst, D.E.; Venkatraman, M.M.; Krishna Swamy, B.G.; McGann, M.; Booth-Laforce, C.; Ram Manohar, P.; Sarin, R.; Mahapatra, A.; Krishna Kumar, P.R. Well controlled, double-blind, placebo-controlled trials of classical Ayurvedic treatment are possible in rheumatoid arthritis. Ann. Rheum. Dis. 2011, 70, 392–393. [Google Scholar] [CrossRef]
- Kumar, S.; Rampp, T.; Kessler, C.; Jeitler, M.; Dobos, G.J.; Ludtke, R.; Meier, L.; Michalsen, A. Effectiveness of Ayurvedic Massage (Sahacharadi Taila) in Patients with Chronic Low Back Pain: A Randomized Controlled Trial. J. Altern. Complement. Med. 2017, 23, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Kessler, C.S.; Morandi, A.; Kumar, A.; Dhiman, K.S.; Gupta, S.; Icke, K.; Bühner, C.; Stapelfeldt, E.; Wischnewsky, M.; Kronpaß, L.; et al. Reliability of Ayurvedic Diagnosis for Knee Osteoarthritis Patients: A Nested Diagnostic Study Within a Randomized Controlled Trial. J. Altern. Complement. Med. 2019, 25, 910–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witt, C.M.; Michalsen, A.; Roll, S.; Morandi, A.; Gupta, S.; Rosenberg, M.; Kronpaß, L.; Stapelfeldt, E.; Hissar, S.; Müller, M.; et al. Comparative effectiveness of a complex Ayurvedic treatment and conventional standard care in osteoarthritis of the knee—Study protocol for a randomized controlled trial. Trials 2013, 14, 149. [Google Scholar] [CrossRef]
- Kessler, C.S.; Ostermann, T.; Meier, L.; Stapelfeldt, E.; Schutte, S.; Duda, J.; Michalsen, A. Additive Complex Ayurvedic Treatment in Patients with Fibromyalgia Syndrome Compared to Conventional Standard Care Alone: A Nonrandomized Controlled Clinical Pilot Study (KAFA Trial). Evid. Based Complement. Altern. Med. 2013, 2013, 751403. [Google Scholar] [CrossRef] [PubMed]
- Kessler, C.S.; Pinders, L.; Michalsen, A.; Cramer, H. Ayurvedic interventions for osteoarthritis: A systematic review and meta-analysis. Rheumatol. Int. 2015, 35, 211–232. [Google Scholar] [CrossRef]
- Bellamy, N. WOMAC Osteoarthritis Index User Guide. Version V; WOMAC: Brisbane, Australia, 2002. [Google Scholar]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Stucki, G.; Meier, D.; Stucki, S.; Michel, B.A.; Tyndall, A.G.; Dick, W.; Theiler, R. Evaluation of a German version of WOMAC (Western Ontario and McMaster Universities) Arthrosis Index. Z. Rheumatol. 1996, 55, 40–49. [Google Scholar]
- Freund, Y.; Schapire, R.E. A Decision-Theoretic Generalization of On-Line Learning and an Application to Boosting. J. Comput. Syst. Sci. 1997, 55, 119–139. [Google Scholar] [CrossRef] [Green Version]
- Clement, N.D.; Bardgett, M.; Weir, D.; Holland, J.; Gerrand, C.; Deehan, D.J. What is the Minimum Clinically Important Difference for the WOMAC Index After TKA? Clin. Orthop. Relat. Res. 2018, 476, 2005–2014. [Google Scholar] [CrossRef]
- Kaptchuk, T.J.; Miller, F.G. Placebo Effects in Medicine. N. Engl. J. Med. 2015, 373, 8–9. [Google Scholar] [CrossRef]
- Moseley, J.B.; O’Malley, K.; Petersen, N.J.; Menke, T.J.; Brody, B.A.; Kuykendall, D.H.; Hollingsworth, J.C.; Ashton, C.M.; Wray, N.P. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N. Engl. J. Med. 2002, 347, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Chen, J.; Hu, Q.S.; Huang, Q.; Ma, J.; Pei, F.X.; Shen, B.; Kraus, V.B. Meta-analysis of pain and function placebo responses in pharmacological osteoarthritis trials. Arthritis Res. Ther. 2019, 21, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Q.; Zhao, J.; Guo, W. Efficacy of massage therapy in improving outcomes in knee osteoarthritis: A systematic review and meta-analysis. Complement. Clin. Pract. 2022, 46, 101522. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Huang, L.; Sun, M.; Xu, G.; He, J.; Zhou, Z.; Huang, F.; Liu, Y.; Liang, F. Acupuncture for Knee Osteoarthritis: A Systematic Review of Randomized Clinical Trials with Meta-Analyses and Trial Sequential Analyses. BioMed Res. Int. 2022, 2022, 6561633. [Google Scholar] [CrossRef]
- Liang, Y.; Xu, Y.; Zhu, Y.; Ye, H.; Wang, Q.; Xu, G. Efficacy and Safety of Chinese Herbal Medicine for Knee Osteoarthritis: Systematic Review and Meta-analysis of Randomized Controlled Trials. Phytomed. Int. J. Phytother. Phytopharm. 2022, 100, 154029. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Callahan, L.F. Clinical relevance of Tai Chi on pain and physical function in adults with knee osteoarthritis: An ancillary meta-analysis of randomized controlled trials. Sci. Prog. 2022, 105, 368504221088375. [Google Scholar] [CrossRef]
- Lauche, R.; Cramer, H.; Langhorst, J.; Dobos, G. A systematic review and meta-analysis of medical leech therapy for osteoarthritis of the knee. Clin. J. Pain 2014, 30, 63–72. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Therapy | Mean | Std. Error | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | Significance | ||||
| WOMAC Index from baseline to 12 weeks | Ayurveda | 46.7 | 6.7 | 33.5 | 59.9 | |
| Conventional therapy | 26.4 | 6.7 | 13.2 | 39.7 | ||
| Difference (Ayurveda—conventional therapy) | 20.3 | 9.5 | 1.5 | 39.0 | 0.034 | |
| WOMAC Index from baseline to 12 months | Ayurveda | 34.7 | 7.0 | 20.8 | 48.6 | |
| Conventional therapy | 25.4 | 7.6 | 10.3 | 40.6 | ||
| Difference (Ayurveda—conventional therapy) | 9.3 | 10.4 | −29.8 | 10.3 | 0.375 | |
| Model | F | df | Significance | Partial Eta Squared | Observed Power | |
|---|---|---|---|---|---|---|
| 12 weeks | Corrected model | 8.09 | 19 | <0.001 | 0.54 | 100.0% |
| Therapy | 7.43 | 1 | 0.007 | 0.054 | 77.2% | |
| Functional limitations at baseline | 11 | 1 | 0.001 | 0.078 | 91.0% | |
| 12 months | Corrected model | 4.63 | 19 | <0.001 | 0.44 | 100.0% |
| Therapy | 1.9 | 1 | 0.171 | 0.017 | 27.7% | |
| Functional limitations at baseline | 5.95 | 1 | 0.016 | 0.051 | 67.7% |
| Tests of Between-Subject Effects | |||||||
|---|---|---|---|---|---|---|---|
| Dependent Variable: Changes in WOMAC Index from Baseline to 12 Weeks | |||||||
| Source | Type III Sum of Squares | df | F | Sig. | Partial Eta Squared | Observed Power | |
| Model I | WOMAC Index baseline | 108,356.6 | 1 | 104.0 | <0.001 | 0.413 | 100.0% |
| Therapy | 37,834.5 | 1 | 36.3 | <0.001 | 0.197 | 100.0% | |
| Model II | WOMAC-A pain baseline | 82,636.9 | 1 | 68.0 | <0.001 | 0.315 | 100.0% |
| Therapy | 37,968.6 | 1 | 31.2 | <0.001 | 0.171 | 100.0% | |
| Model III | WOMAC-B stiffness baseline | 67,526.4 | 1 | 51.2 | <0.001 | 0.257 | 100.0% |
| Therapy | 34,093.8 | 1 | 25.9 | <0.001 | 0.149 | 99.9% | |
| Model IV | WOMAC-C functional limitations baseline | 104,845.2 | 1 | 98.4 | <0.001 | 0.399 | 100.0% |
| Therapy | 37,328.5 | 1 | 35.0 | <0.001 | 0.191 | 100.0% | |
| Model V | WOMAC-A pain baseline | 2122.2 | 1 | 2.0 | 0.158 | 0.014 | 29.1% |
| WOMAC-B stiffness baseline | 1630.1 | 1 | 1.5 | 0.216 | 0.010 | 23.5% | |
| WOMAC-C functional limitations baseline | 12,576.4 | 1 | 11.9 | 0.001 | 0.076 | 92.9% | |
| Therapy | 37,786.1 | 1 | 35.8 | <0.001 | 0.197 | 100.0% | |
| Model VI | WOMAC-A pain baseline | 616.4 | 1 | 0.6 | 0.430 | 0.006 | 12.3% |
| WOMAC-B stiffness baseline | 4302.8 | 1 | 4.4 | 0.039 | 0.041 | 54.6% | |
| WOMAC-C functional limitations baseline | 11,001.1 | 1 | 11.2 | 0.001 | 0.097 | 91.3% | |
| Age | 53.4 | 1 | 0.1 | 0.816 | 0.001 | 5.6% | |
| Duration of pains (years) | 35.9 | 1 | 0.0 | 0.849 | 0.000 | 5.4% | |
| BMI | 802.1 | 1 | 0.8 | 0.368 | 0.008 | 14.6% | |
| Therapy | 14,222.4 | 1 | 14.5 | <0.001 | 0.122 | 96.5% | |
| Gender | 36.1 | 1 | 0.0 | 0.848 | 0.000 | 5.4% | |
| Expectations for Ayurveda | 9572.7 | 4 | 2.4 | 0.051 | 0.086 | 68.2% | |
| Expectations for conventional therapy | 2068.5 | 4 | 0.5 | 0.716 | 0.020 | 17.3% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kessler, C.S.; Jeitler, M.; Dhiman, K.S.; Kumar, A.; Ostermann, T.; Gupta, S.; Morandi, A.; Mittwede, M.; Stapelfeldt, E.; Spoo, M.; et al. Ayurveda in Knee Osteoarthritis—Secondary Analyses of a Randomized Controlled Trial. J. Clin. Med. 2022, 11, 3047. https://doi.org/10.3390/jcm11113047
Kessler CS, Jeitler M, Dhiman KS, Kumar A, Ostermann T, Gupta S, Morandi A, Mittwede M, Stapelfeldt E, Spoo M, et al. Ayurveda in Knee Osteoarthritis—Secondary Analyses of a Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(11):3047. https://doi.org/10.3390/jcm11113047
Chicago/Turabian StyleKessler, Christian S., Michael Jeitler, Kartar S. Dhiman, Abhimanyu Kumar, Thomas Ostermann, Shivenarain Gupta, Antonio Morandi, Martin Mittwede, Elmar Stapelfeldt, Michaela Spoo, and et al. 2022. "Ayurveda in Knee Osteoarthritis—Secondary Analyses of a Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 11: 3047. https://doi.org/10.3390/jcm11113047
APA StyleKessler, C. S., Jeitler, M., Dhiman, K. S., Kumar, A., Ostermann, T., Gupta, S., Morandi, A., Mittwede, M., Stapelfeldt, E., Spoo, M., Icke, K., Michalsen, A., Witt, C. M., & Wischnewsky, M. B. (2022). Ayurveda in Knee Osteoarthritis—Secondary Analyses of a Randomized Controlled Trial. Journal of Clinical Medicine, 11(11), 3047. https://doi.org/10.3390/jcm11113047