
Asymmetrical Handgrip Strength Is Associated with Lower Cognitive Performance in the Elderly


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurement of Cognitive Function
2.3. Measurement of HGS
2.4. Other Variables
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Participants
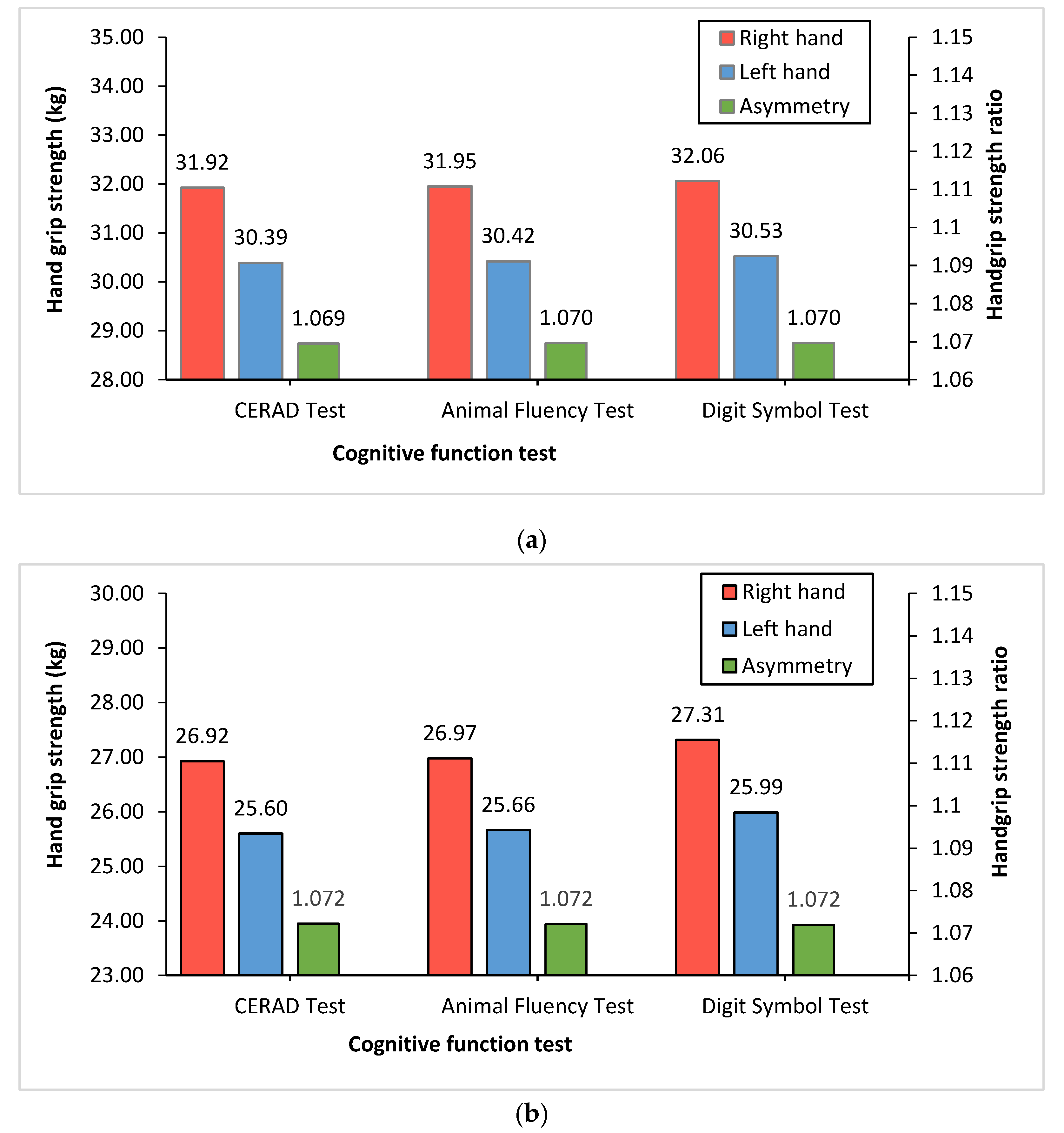
3.2. The Structures of Right and Left HGS and Handgrip Ratio
3.3. Correlation among HGS and Cognitive Function
3.4. The Estimated Beta Coefficients (SE) for the HGS
3.5. The Estimated Beta Coefficients (SE) for HGS Asymmetry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2009; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2010; 73p. [Google Scholar]
- Hebert, L.E.; Weuve, J.; Scherr, P.A.; Evans, D.A. Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology 2013, 80, 1778–1783. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.A.; McConnell, S.R. Cognitive health: An emerging public health issue. Alzheimer’s Dement. 2007, 3 (Suppl. S2), S70–S73. [Google Scholar] [CrossRef]
- Dong, X.; Li, S.; Sun, J.; Li, Y.; Zhang, D. Association of Coffee, Decaffeinated Coffee and Caffeine Intake from Coffee with Cognitive Performance in Older Adults: National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutrients 2020, 12, 840. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.; Luppa, M.; Maier, W.; Wagner, M.; Wolfsgruber, S.; Scherer, M.; Köhler, M.; Eisele, M.; Weyerer, S.; Werle, J.; et al. Assessing cognitive changes in the elderly: Reliable change indices for the Mini-Mental State Examination. Acta. Psychiatr. Scand. 2012, 126, 208–218. [Google Scholar] [CrossRef]
- Stewart, M.C.; Deary, I.J.; Fowkes, F.G.R.; Price, J.F. Relationship between lifetime smoking, smoking status at older age and human cognitive function. Neuroepidemiology 2006, 26, 83–92. [Google Scholar] [CrossRef]
- Hagger-Johnson, G.; Sabia, S.; Brunner, E.; Shipley, M.; Bobak, M.; Marmot, M.; Kivimaki, M.; Singh-Manoux, A. Combined impact of smoking and heavy alcohol use on cognitive decline in early old age: Whitehall II prospective cohort study. Br. J. Psychiatr. 2013, 203, 120–125. [Google Scholar] [CrossRef]
- Hu, M.; Yin, H.; Shu, X.; Jia, Y.; Leng, M.; Chen, L. Multi-angles of smoking and mild cognitive impairment: Is the association mediated by sleep duration? Neurol. Sci. 2019, 40, 1019–1027. [Google Scholar] [CrossRef]
- de Asteasu, M.L.S.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef]
- McGrath, R.; Clark, B.C.; Cesari, M.; Johnson, C.; Jurivich, D.A. Handgrip strength asymmetry is associated with future falls in older Americans. Aging Clin. Exp. Res. 2021, 33, 2461–2469. [Google Scholar] [CrossRef]
- Go, Y.J.; Lee, D.C.; Lee, H.J. Association between handgrip strength asymmetry and falls in elderly Koreans: A nationwide population-based cross-sectional study. Arch. Gerontol. Geriatr. 2021, 96, 104470. [Google Scholar] [CrossRef]
- Giampaoli, S.; Ferrucci, L.; Cecchi, F.; Noce, C.L.; Poce, A.; Dima, F.; Santaquilani, A.; Vescio, M.F.; Menotti, A. Hand-grip strength predicts incident disability in non-disabled older men. Age Ageing 1999, 28, 283–288. [Google Scholar] [CrossRef] [Green Version]
- Lera, L.; Albala, C.; Leyton, B.; Márquez, C.; Angel, B.; Saguez, R.; Sánchez, H. Reference values of hand-grip dynamometry and the relationship between low strength and mortality in older Chileans. Clin. Interv. Aging 2018, 13, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Sternäng, O.; Reynolds, C.A.; Finkel, D.; Bravell, M.E.; Pedersen, N.; Aslan, A.K.D. Grip Strength and Cognitive Abilities: Associations in Old Age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2016, 71, 841–848. [Google Scholar] [CrossRef] [Green Version]
- Praetorius Björk, M.; Johansson, B.; Hassing, L.B. I forgot when I lost my grip-strong associations between cognition and grip strength in level of performance and change across time in relation to impending death. Neurobiol. Aging 2016, 38, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Vancampfort, D.; Stubbs, B.; Firth, J.; Smith, L.; Swinnen, N.; Koyanagi, A. Associations between handgrip strength and mild cognitive impairment in middle-aged and older adults in six low- and middle-income countries. Int. J. Geriatr. Psychiatr. 2019, 34, 609–616. [Google Scholar] [CrossRef]
- Goldberg, T.E.; Koppel, J.; Keehlisen, L.; Christen, E.; Dreses-Werringloer, U.; Conejero-Goldberg, C.; Gordon, M.L.; Davies, P. Performance-based measures of everyday function in mild cognitive impairment. Am. J. Psychiatr. 2010, 167, 845–853. [Google Scholar] [CrossRef] [Green Version]
- Rait, G.; Walters, K.; Bottomley, C.; Petersen, I.; Iliffe, S.; Nazareth, I. Survival of people with clinical diagnosis of dementia in primary care: Cohort study. BMJ 2010, 341, c3584. [Google Scholar] [CrossRef] [Green Version]
- Ling, C.H.; Taekema, D.; de Craen, A.J.; Gussekloo, J.; Westendorp, R.G.; Maier, A.B. Handgrip strength and mortality in the oldest old population: The Leiden 85-plus study. CMAJ 2010, 182, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- McGrath, R.; Vincent, B.; Hackney, K.J.; Robinson-Lane, S.; Downer, B.; Clark, B.C. The Longitudinal Associations of Handgrip Strength and Cognitive Function in Aging Americans. J. Am. Med. Dir. Assoc. 2020, 21, 634–639.e1. [Google Scholar] [CrossRef]
- Kim, G.R.; Sun, J.; Han, M.; Nam, C.M.; Park, S. Evaluation of the directional relationship between handgrip strength and cognitive function: The Korean Longitudinal Study of Ageing. Age Ageing 2019, 48, 426–432. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Association of muscle strength with the risk of Alzheimer disease and the rate of cognitive decline in community-dwelling older persons. Arch. Neurol. 2009, 66, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Larson, E.B.; Bowen, J.D.; Van Belle, G. Performance-based physical function and future dementia in older people. Arch. Intern. Med. 2006, 166, 1115–1120. [Google Scholar] [CrossRef] [Green Version]
- Okely, J.A.; Deary, I.J. Associations Between Declining Physical and Cognitive Functions in the Lothian Birth Cohort 1936. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1393–1402. [Google Scholar] [CrossRef] [Green Version]
- Collins, K.; Johnson, N.; Klawitter, L.; Waldera, R.; Stastny, S.; Kraemer, W.J.; Christensen, B.; McGrath, R. Handgrip Strength Asymmetry and Weakness are Differentially Associated with Functional Limitations in Older Americans. Int. J. Environ. Res. Public Health 2020, 17, 3231. [Google Scholar] [CrossRef]
- McGrath, R.; Cawthon, P.M.; Cesari, M.; Al Snih, S.; Clark, B.C. Handgrip Strength Asymmetry and Weakness Are Associated with Lower Cognitive Function: A Panel Study. J. Am. Geriatr. Soc. 2020, 68, 2051–2058. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/ (accessed on 16 March 2021).
- Brigola, A.G.; Rossetti, E.S.; Dos Santos, B.R.; Neri, A.L.; Zazzetta, M.S.; Inouye, K.; Pavarini, S.C.I. Relationship between cognition and frailty in elderly: A systematic review. Dement. Neuropsychol. 2015, 9, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, R.; Van Ancum, J.M.; Verlaan, S.; Scheerman, K.; Meskers, C.G.; Maier, A.B. Lower cognitive function in older patients with lower muscle strength and muscle mass. Dement. Geriatr. Cogn. Disord. 2018, 45, 243–250. [Google Scholar] [CrossRef]
- Raji, M.A.; Kuo, Y.-F.; Al Snih, S.; Markides, K.S.; Peek, M.K.; Ottenbacher, K. Cognitive status, muscle strength, and subsequent disability in older Mexican Americans. J. Am. Geriatr. Soc. 2005, 53, 1462–1468. [Google Scholar] [CrossRef]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal Muscle Health and Cognitive Function: A Narrative Review. Int. J. Mol. Sci. 2020, 22, 255. [Google Scholar] [CrossRef]
- Laurin, D.; Verreault, R.; Lindsay, J.; MacPherson, K.; Rockwood, K. Physical activity and risk of cognitive impairment and dementia in elderly persons. Arch. Neurol. 2001, 58, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Guimarães, F.C.; Amorim, P.; Dos Reis, F.F.; Bonoto, R.T.; De Oliveira, W.C.; Moura, T.A.D.S.; De Assis, C.L.; Palotás, A.; Lima, L.M. Physical activity and better medication compliance improve mini-mental state examination scores in the elderly. Dement. Geriatr. Cogn. Disord. 2015, 39, 25–31. [Google Scholar] [CrossRef]
- Ihira, H.; Sawada, N.; Inoue, M.; Yasuda, N.; Yamagishi, K.; Charvat, H.; Iwasaki, M.; Tsugane, S. Association Between Physical Activity and Risk of Disabling Dementia in Japan. JAMA Netw. Open 2022, 5, e224590. [Google Scholar] [CrossRef]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef] [Green Version]
- Licastro, F.; Pedrini, S.; Caputo, L.; Annoni, G.; Davis, L.J.; Ferri, C.; Casadei, V.; Grimaldi, L.M. Increased plasma levels of interleukin-1, interleukin-6 and alpha-1-antichymotrypsin in patients with Alzheimer’s disease: Peripheral inflammation or signals from the brain? J. Neuroimmunol. 2000, 103, 97–102. [Google Scholar] [CrossRef]
- Asoudeh, F.; Dashti, F.; Raeesi, S.; Heshmat, R.; Bidkhori, M.; Jalilian, Z.; Hashemi, R. Inflammatory cytokines and sarcopenia in Iranian adults-results from SARIR study. Sci. Rep. 2022, 12, 5471. [Google Scholar] [CrossRef]
- Meng, S.J.; Yu, L.J. Oxidative stress, molecular inflammation and sarcopenia. Int. J. Mol. Sci. 2010, 11, 1509–1526. [Google Scholar] [CrossRef] [Green Version]
- Mariani, E.; Polidori, M.; Cherubini, A.; Mecocci, P. Oxidative stress in brain aging, neurodegenerative and vascular diseases: An overview. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2005, 827, 65–75. [Google Scholar] [CrossRef]
- Yildiz, Z.; Eren, N.; Orcun, A.; Gokyigit, F.M.; Turgay, F.; Celebi, L.G. Serum apelin-13 levels and total oxidant/antioxidant status of patients with Alzheimer’s disease. Aging Med. 2021, 4, 201–205. [Google Scholar] [CrossRef]
- Phillips, C.; Baktir, M.A.; Srivatsan, M.; Salehi, A. Neuroprotective effects of physical activity on the brain: A closer look at trophic factor signaling. Front. Cell Neurosci. 2014, 8, 170. [Google Scholar] [CrossRef] [Green Version]
- Mufson, E.J.; Binder, L.; Counts, S.E.; DeKosky, S.T.; Detoledo-Morrell, L.; Ginsberg, S.D.; Ikonomovic, M.D.; Perez, S.E.; Scheff, S.W. Mild cognitive impairment: Pathology and mechanisms. Acta. Neuropathol. 2012, 123, 13–30. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y.N.; Yoon, S.S. Sarcopenia: Neurological point of view. J. Bone Metab. 2017, 24, 83–89. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| 60–69 Years-Old (n = 1446) | ≥70 Years-Old (n = 1283) | p-Value | |||
|---|---|---|---|---|---|
| Sex | 0.6618 | ||||
| Male | 703 | (53.4) | 613 | (46.6) | |
| Female | 743 | (52.6) | 670 | (47.4) | |
| Race/Ethnicity | <0.0001 | ||||
| White | 506 | (38.7) | 801 | (61.3) | |
| Black | 422 | (65.4) | 223 | (34.6) | |
| Hispanic | 362 | (70.2) | 154 | (29.8) | |
| Others | 156 | (59.8) | 105 | (40.2) | |
| Income, USD | 0.1979 | ||||
| <20,000 | 362 | (50.9) | 349 | (49.1) | |
| ≥20,000 | 1084 | (53.7) | 934 | (46.3) | |
| Cigarette smoking | <0.0001 | ||||
| Current smoker | 257 | (73.9) | 91 | (26.2) | |
| Former smoker | 507 | (48.8) | 532 | (51.2) | |
| Never smoker | 682 | (50.8) | 660 | (49.2) | |
| Alcohol drinking | <0.0001 | ||||
| Drinker | 1024 | (55.7) | 813 | (44.3) | |
| Non-drinker | 422 | (47.3) | 470 | (52.7) | |
| Moderate recreational activities for at least 10 min | 0.0126 | ||||
| Yes | 588 | (56.0) | 462 | (44.0) | |
| No | 858 | (51.1) | 821 | (48.9) | |
| Body Mass Index (kg/m2) | 0.0047 | ||||
| Underweight (<18.5) | 19 | (46.3) | 22 | (53.7) | |
| Normal weight (18.5–24.9) | 358 | (51.1) | 342 | (48.9) | |
| Overweight (25–29.9) | 477 | (49.9) | 478 | (50.1) | |
| Obese (≥30) | 592 | (57.3) | 441 | (42.7) | |
| Diabetes | 0.9511 | ||||
| Yes | 361 | (53.1) | 319 | (46.9) | |
| No | 1085 | (53.0) | 964 | (47.1) | |
| Hypertension | <0.0001 | ||||
| Yes | 840 | (49.3) | 864 | (50.7) | |
| No | 606 | (59.1) | 419 | (40.9) | |
| Pearson Correlation Coefficients (p-Value) | ||||||
|---|---|---|---|---|---|---|
| 60–69 Years-Old | ≥70 Years-Old | |||||
| CERAD Test | AFT | DSST | CERAD Test | AFT | DSST | |
| Right hand | −0.033 (0.2006) | 0.081 (0.0018) | 0.002 (0.9519) | 0.047 (0.0846) | 0.187 (<0.0001) | 0.104 (0.0002) |
| Left hand | −0.36 (0.1647) | 0.079 (0.0022) | −0.015 (0.5637) | 0.080 (0.0033) | 0.192 (<0.0001) | 0.101 (0.0003) |
| Asymmetric | 0.052 (0.0358) | 0.064 (0.0093) | 0.070 (0.0048) | 0.096 (0.0002) | 0.073 (0.0051) | 0.068 (0.0110) |
| Unadjusted | Adjusted a | |||||||
|---|---|---|---|---|---|---|---|---|
| 60–69 Years-Old | ≥70 Years-Old | 60–69 Years-Old | ≥70 Years-Old | |||||
| Beta (SE) | p-Value | Beta (SE) | p-Value | Beta (SE) | p-Value | Beta (SE) | p-Value | |
| CERAD test | ||||||||
| Right hand | −0.004 (0.004) | 0.3475 | 0.006 (0.006) | 0.3319 | 0.011 (0.008) | 0.1849 | 0.026 (0.006) | 0.0001 |
| Left hand | −0.005 (0.005) | 0.2630 | 0.010 (0.006) | 0.1074 | 0.009 (0.008) | 0.2489 | 0.035 (0.007) | <0.0001 |
| AFT | ||||||||
| Right hand | 0.046 (0.020) | 0.0266 | 0.118 (0.023) | <0.0001 | 0.055 (0.029) | 0.0628 | 0.090 (0.034) | 0.0138 |
| Left hand | 0.040 (0.019) | 0.0454 | 0.124 (0.022) | <0.0001 | 0.033 (0.034) | 0.3512 | 0.108 (0.038) | 0.0074 |
| DSST | ||||||||
| Right hand | 0.003 (0.042) | 0.9415 | 0.247 (0.054) | <0.0001 | 0.308 (0.075) | 0.0003 | 0.243 (0.053) | <0.0001 |
| Left hand | −0.042 (0.038) | 0.2793 | 0.243 (0.053) | <0.0001 | 0.342 (0.083) | 0.0003 | 0.322 (0.082) | 0.0004 |
| Unadjusted | Adjusted a | |||||||
|---|---|---|---|---|---|---|---|---|
| 60–69 Years-Old | ≥70 Years-Old | 60–69 Years-Old | ≥70 Years-Old | |||||
| Beta (SE) | p-Value | Beta (SE) | p-Value | Beta (SE) | p-Value | Beta (SE) | p-Value | |
| CERAD test | ||||||||
| Symmetric | Reference | Reference | Reference | Reference | ||||
| Asymmetric | −0.211 (0.125) | 0.1248 | −0.337 (0.076) | <0.0001 | −0.174 (0.121) | 0.1601 | −0.226 (0.084) | 0.0117 |
| AFT | ||||||||
| Symmetric | Reference | Reference | Reference | Reference | ||||
| Asymmetric | −0.636 (0.401) | 0.1226 | −0.841 (0.358) | 0.0251 | −0.066 (0.402) | 0.8709 | −0.384 (0.370) | 0.3071 |
| DSST | ||||||||
| Symmetric | Reference | Reference | Reference | Reference | ||||
| Asymmetric | −2.620 (0.969) | 0.0109 | −2.053 (0.990) | 0.0462 | −1.178 (0.776) | 0.1387 | −0.491 (1.005) | 0.6282 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.-Y.; Lee, S.; Min, J.-Y.; Min, K.-B. Asymmetrical Handgrip Strength Is Associated with Lower Cognitive Performance in the Elderly. J. Clin. Med. 2022, 11, 2904. https://doi.org/10.3390/jcm11102904
Choi J-Y, Lee S, Min J-Y, Min K-B. Asymmetrical Handgrip Strength Is Associated with Lower Cognitive Performance in the Elderly. Journal of Clinical Medicine. 2022; 11(10):2904. https://doi.org/10.3390/jcm11102904
Chicago/Turabian StyleChoi, Ju-Young, Sohyae Lee, Jin-Young Min, and Kyoung-Bok Min. 2022. "Asymmetrical Handgrip Strength Is Associated with Lower Cognitive Performance in the Elderly" Journal of Clinical Medicine 11, no. 10: 2904. https://doi.org/10.3390/jcm11102904
APA StyleChoi, J.-Y., Lee, S., Min, J.-Y., & Min, K.-B. (2022). Asymmetrical Handgrip Strength Is Associated with Lower Cognitive Performance in the Elderly. Journal of Clinical Medicine, 11(10), 2904. https://doi.org/10.3390/jcm11102904