
Pelvic Fractures—An Underestimated Problem? Incidence and Mortality Risk after Pelvic Fracture in Austria, 2010–2018

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Austrian Social Health Insurance Fund
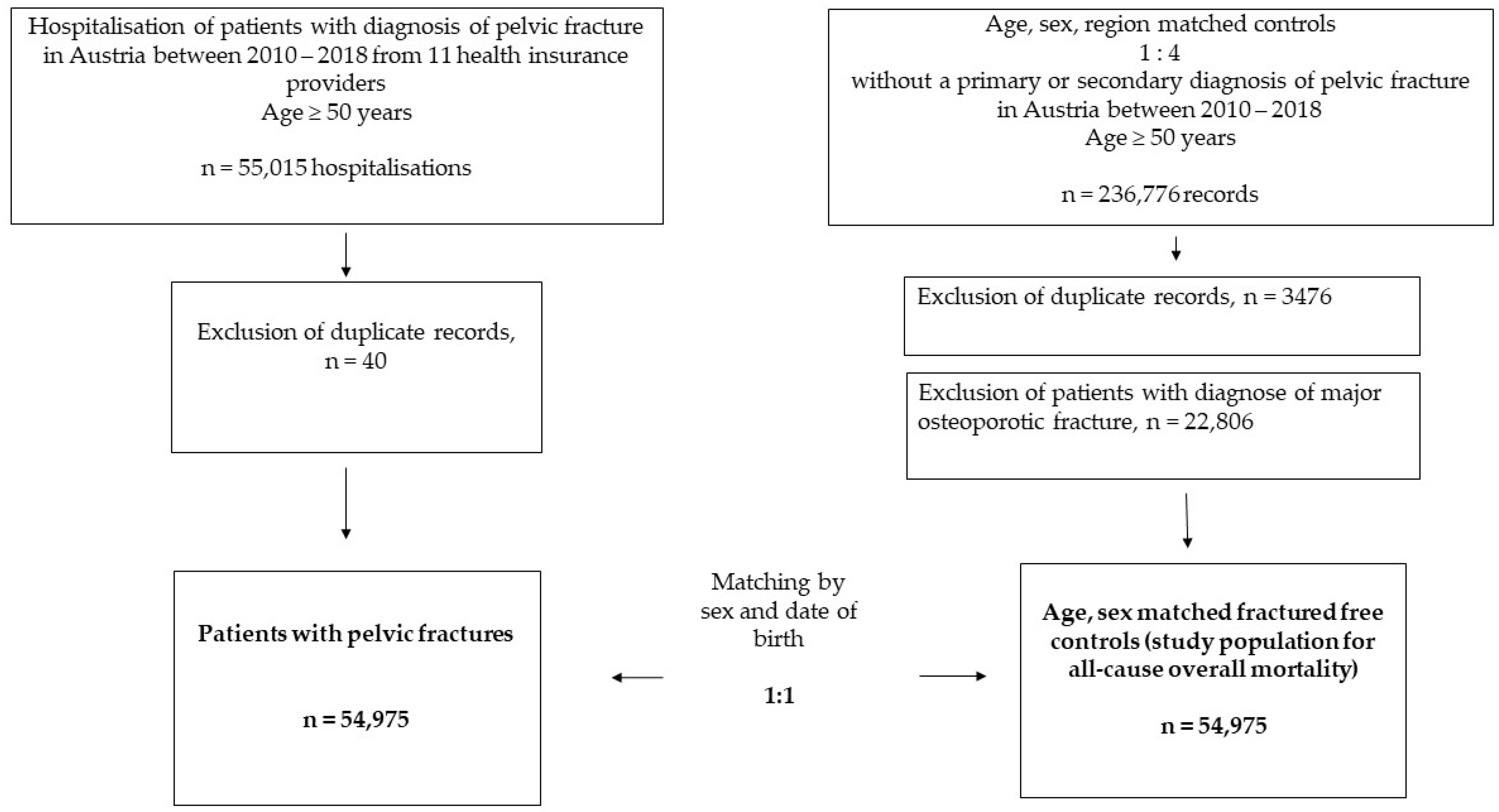
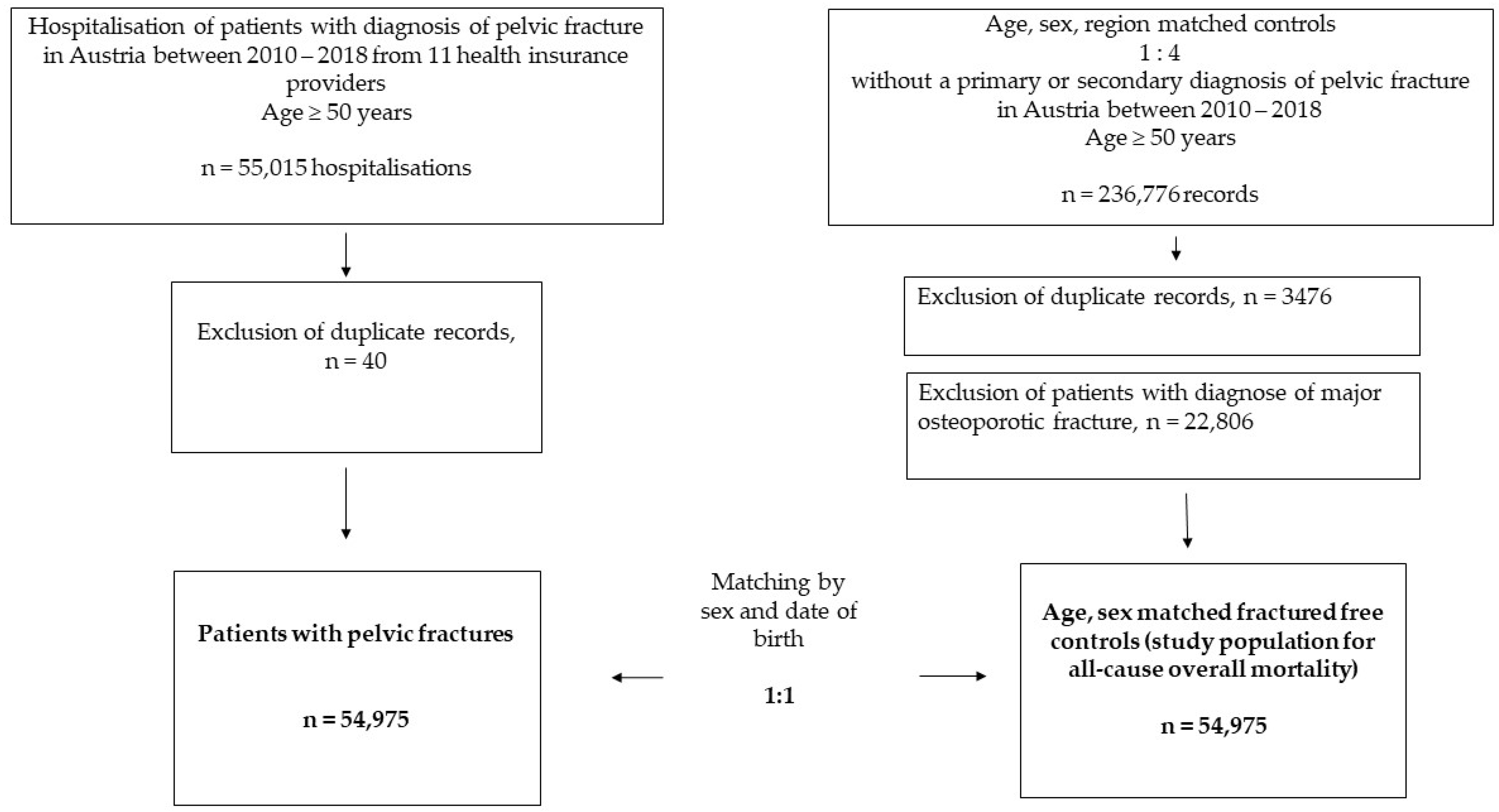
2.2. Study Design and Study Population
2.3. Cohort of Patients with Pelvic Fracture
2.4. Controls without Major Osteoporotic Fractures
2.5. Incidence Rates of Pelvic Fractures
2.6. Mortality
2.7. Recording of Covariates
2.8. Statistical Analyses
2.9. Sensitivity Analysis
3. Results
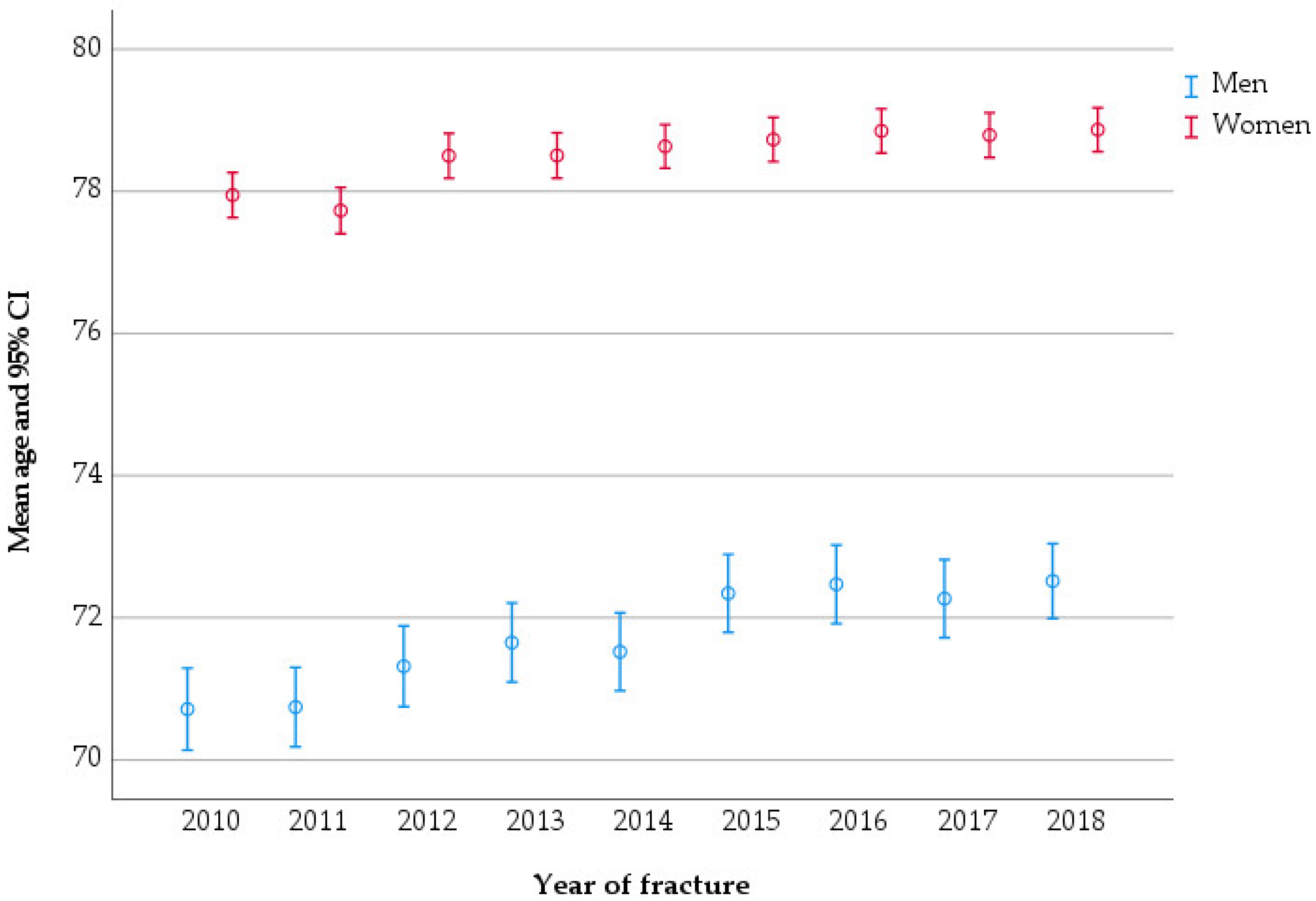
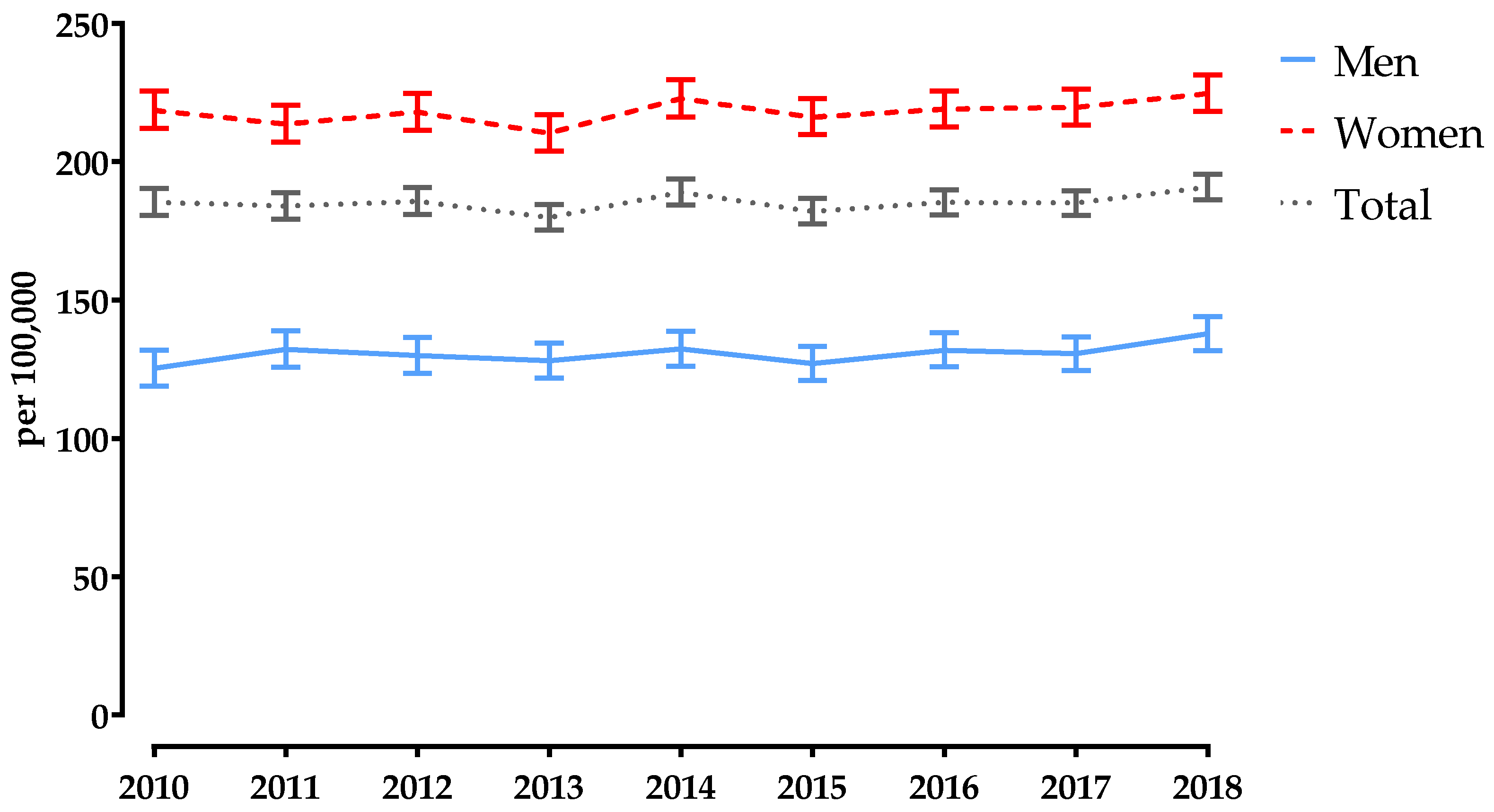
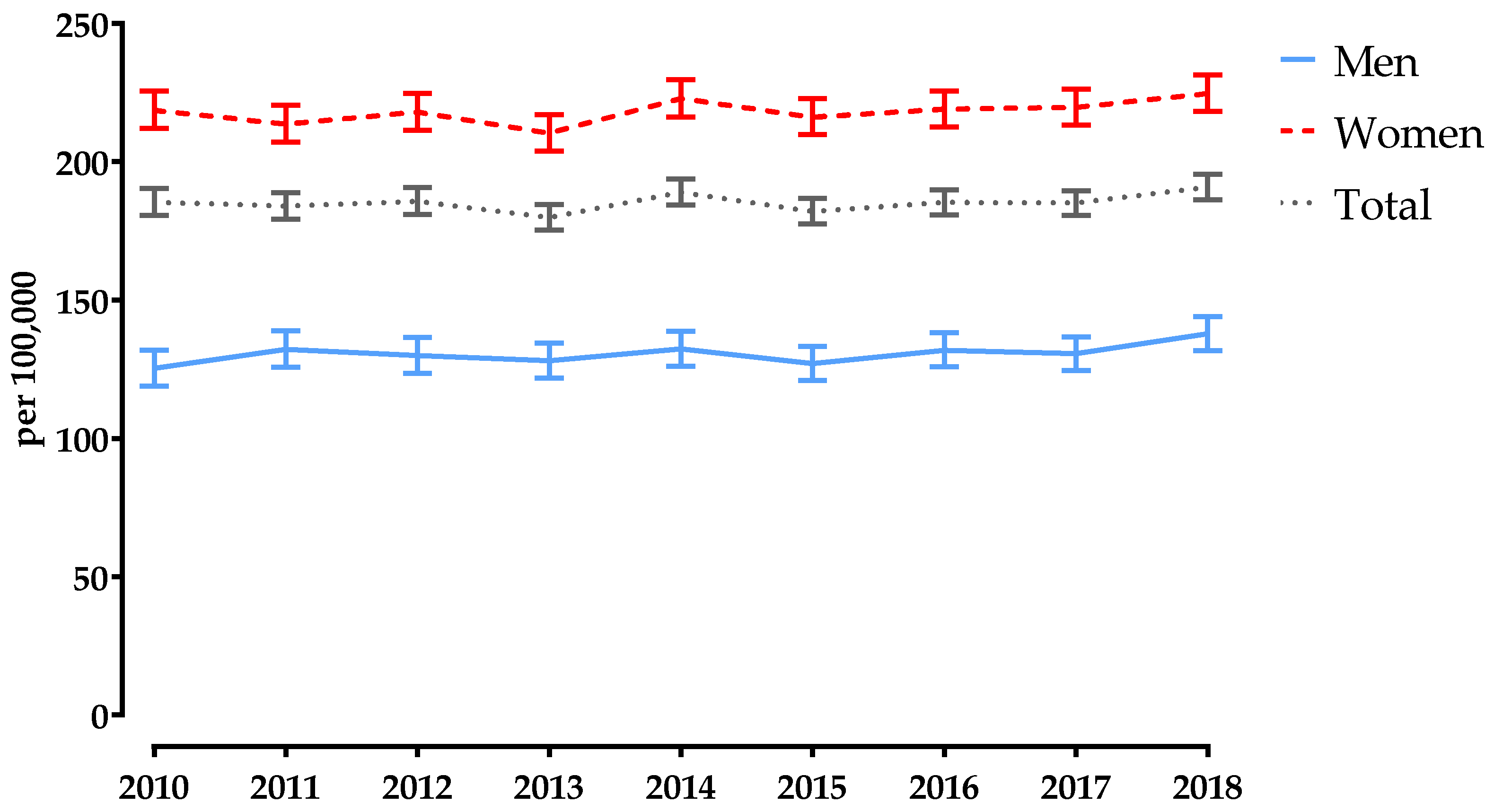
3.1. Age-Standardised Incidence Rate
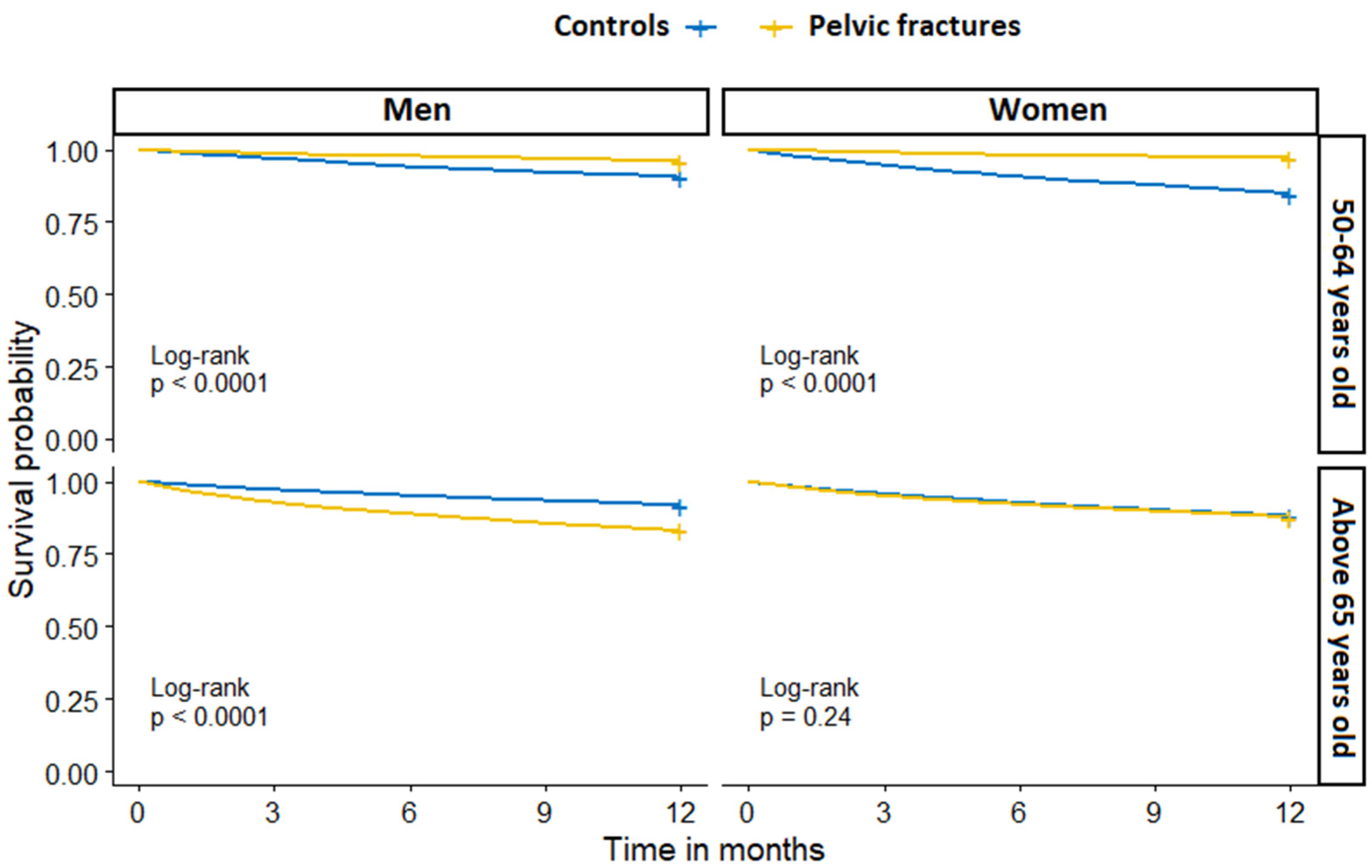
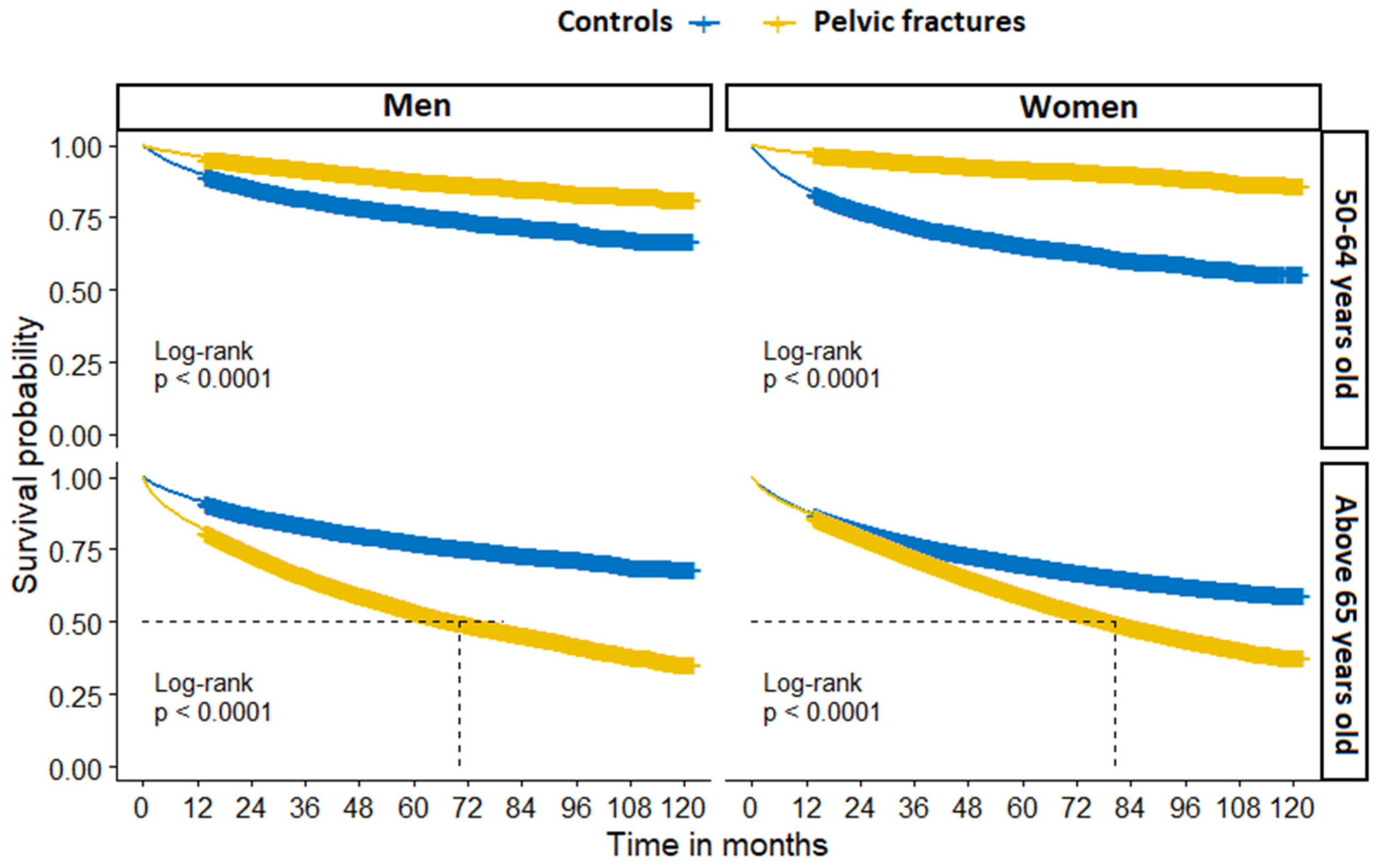
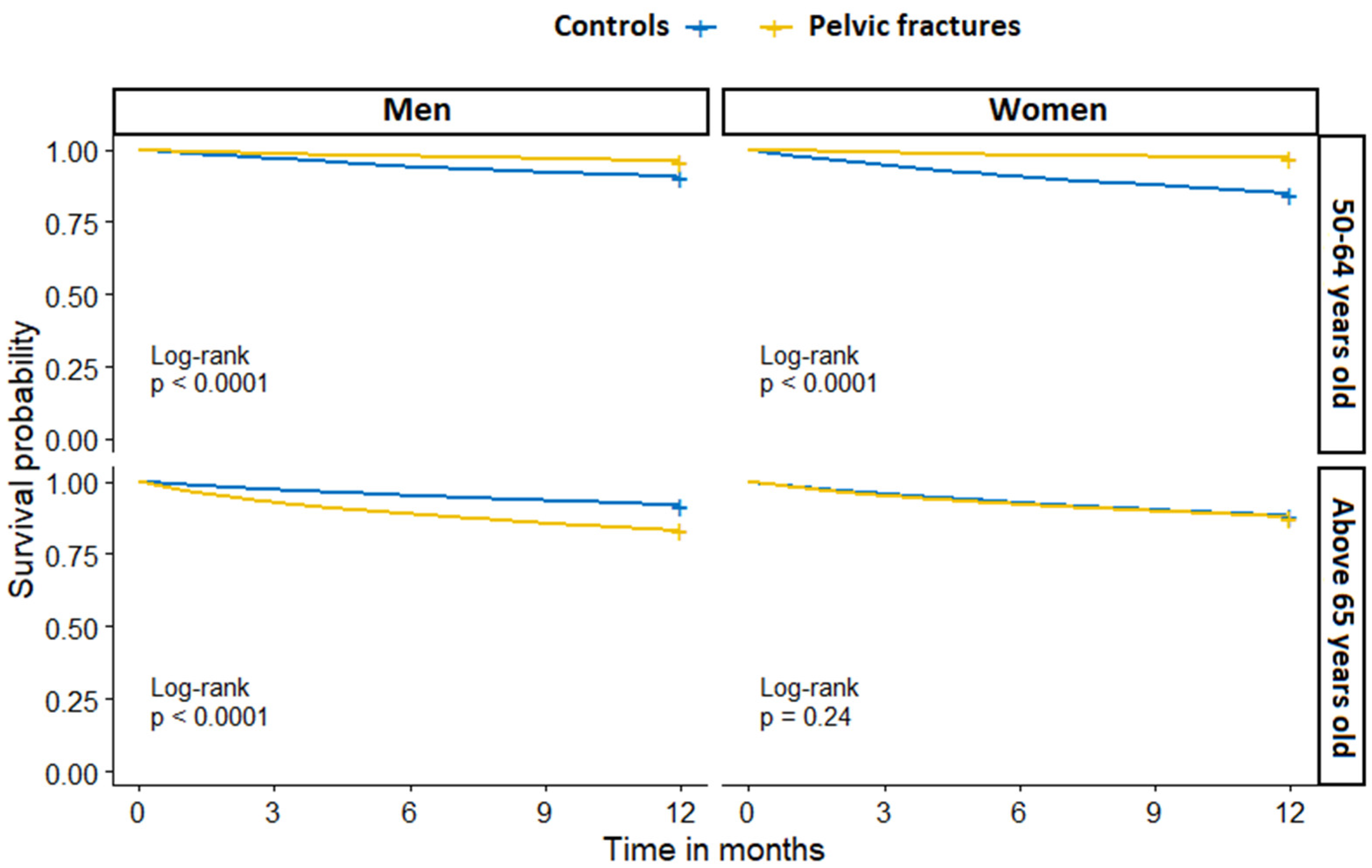
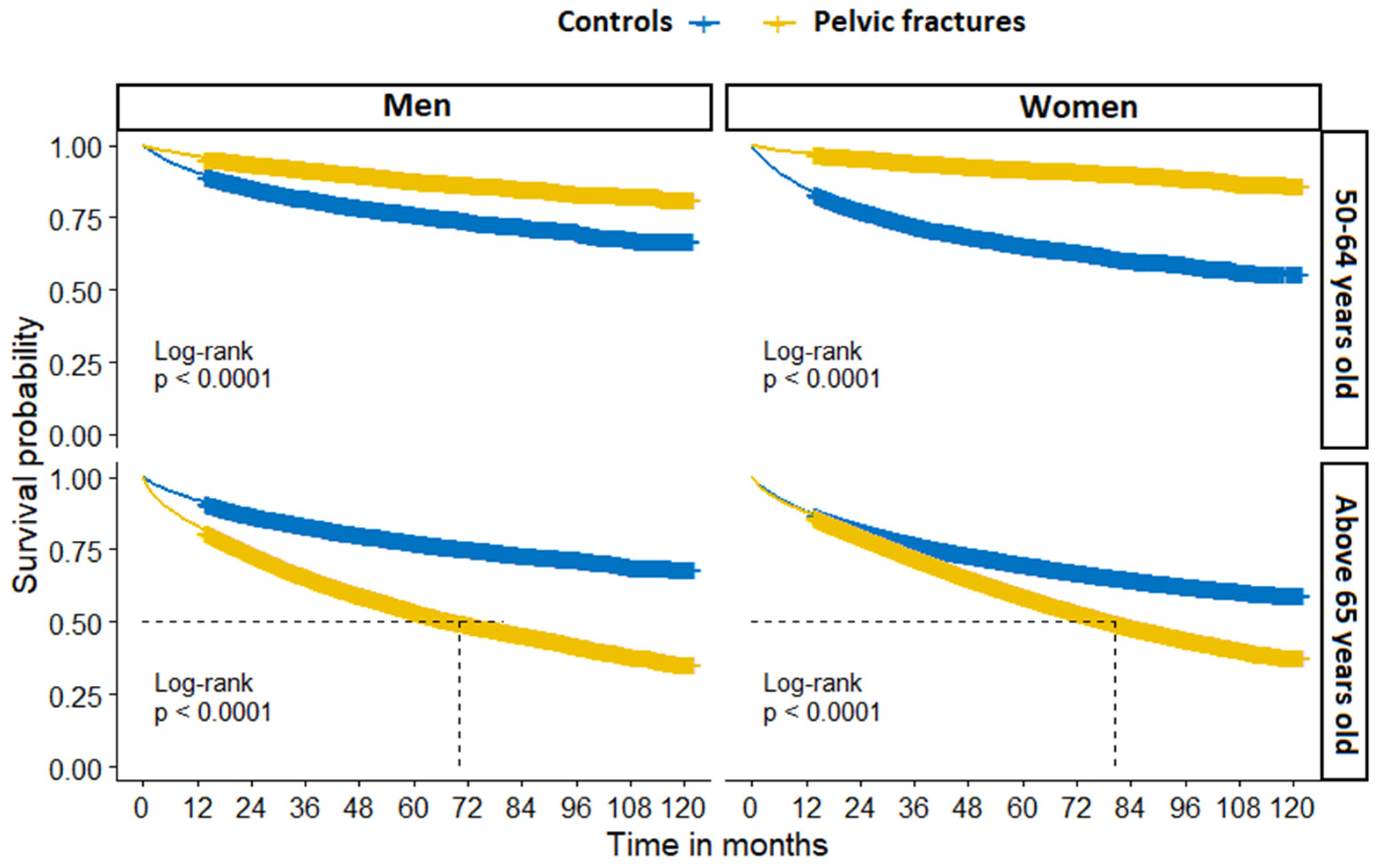
3.2. Mortality
3.3. Sensitivity Analysis
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, C.T.; Barton, D.W.; Piple, A.S.; Carmouche, J.J. Pelvic Fragility Fractures: An Opportunity to Improve the Undertreatment of Osteoporosis. JBJS 2021, 103, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Breuil, V.; Roux, C.H.; Carle, G.F. Pelvic fractures: Epidemiology, consequences, and medical management. Curr. Opin. Rheumatol. 2016, 28, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Andrich, S.; Haastert, B.; Neuhaus, E.; Frommholz, K.; Arend, W.; Ohmann, C.; Grebe, J.; Vogt, A.; Brunoni, C.; Jungbluth, P.; et al. Health care utilization and excess costs after pelvic fractures among older people in Germany. Osteoporos. Int. 2021, 32, 2061–2072. [Google Scholar] [CrossRef]
- Kannus, P.; Palvanen, M.; Niemi, S.; Parkkari, J.; Järvinen, M. Epidemiology of osteoporotic pelvic fractures in elderly people in Finland: Sharp increase in 1970–1997 and alarming projections for the new millennium. Osteoporos. Int. 2000, 11, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P.; Parkkari, J.; Niemi, S.; Sievänen, H. Low-Trauma Pelvic Fractures in Elderly Finns in 1970–2013. Calcif. Tissue Int. 2015, 97, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Nanninga, G.L.; de Leur, K.; Panneman, M.J.; van der Elst, M.; Hartholt, K.A. Increasing rates of pelvic fractures among older adults: The Netherlands, 1986–2011. Age Ageing 2014, 43, 648–653. [Google Scholar] [CrossRef] [Green Version]
- Prieto-Alhambra, D.; Avilés, F.F.; Judge, A.; Van Staa, T.; Nogués, X.; Arden, N.K.; Díez-Pérez, A.; Cooper, C.; Javaid, M.K. Burden of pelvis fracture: A population-based study of incidence, hospitalisation and mortality. Osteoporos. Int. 2012, 23, 2797–2803. [Google Scholar] [CrossRef] [PubMed]
- Rinne, P.P.; Laitinen, M.K.; Kannus, P.; Mattila, V.M. The incidence of pelvic fractures and related surgery in the Finnish adult population: A nationwide study of 33,469 patients between 1997 and 2014. Acta Orthop. 2020, 91, 587–592. [Google Scholar] [CrossRef]
- Buller, L.T.; Best, M.J.; Quinnan, S.M. A Nationwide Analysis of Pelvic Ring Fractures: Incidence and Trends in Treatment, Length of Stay, and Mortality. Geriatr. Orthop. Surg. Rehabil. 2016, 7, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Marrinan, S.; Pearce, M.S.; Jiang, X.Y.; Waters, S.; Shanshal, Y. Admission for osteoporotic pelvic fractures and predictors of length of hospital stay, mortality and loss of independence. Age Ageing 2014, 44, 258–261. [Google Scholar] [CrossRef] [Green Version]
- Andrich, S.; Haastert, B.; Neuhaus, E.; Neidert, K.; Arend, W.; Ohmann, C.; Grebe, J.; Vogt, A.; Jungbluth, P.; Thelen, S.; et al. Excess Mortality after Pelvic Fractures among Older People. J. Bone Miner. Res. 2017, 32, 1789–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muschitz, C.; Kocijan, R.; Baierl, A.; Dormann, R.; Feichtinger, X.; Haschka, J.; Szivak, M.; Muschitz, G.K.; Schanda, J.; Pietschmann, P.; et al. Preceding and subsequent high- and low-trauma fracture patterns-a 13-year epidemiological study in females and males in Austria. Osteoporos. Int. 2017, 28, 1609–1618. [Google Scholar] [CrossRef] [PubMed]
- Rollmann, M.F.; Herath, S.C.; Braun, B.J.; Holstein, J.H.; Pohlemann, T.; Menger, M.D.; Histing, T. In-hospital mortality of pelvic ring fractures in older adults now and then: A pelvic registry study. Geriatr. Gerontol. Int. 2019, 19, 24–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matityahu, A.; Elson, J.; Morshed, S.; Marmor, M. Survivorship and severe complications are worse for octogenarians and elderly patients with pelvis fractures as compared to adults: Data from the national trauma data bank. J. Osteoporos. 2012, 2012, 475739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimai, H.P.; Svedbom, A.; Fahrleitner-Pammer, A.; Pieber, T.; Resch, H.; Zwettler, E.; Chandran, M.; Borgström, F. Epidemiology of hip fractures in Austria: Evidence for a change in the secular trend. Osteoporos. Int. 2011, 22, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Dimai, H.P.; Reichardt, B.; Zitt, E.; Concin, H.; Malle, O.; Fahrleitner-Pammer, A.; Svedbom, A.; Brozek, W. Thirty years of hip fracture incidence in Austria: Is the worst over? Osteoporos. Int. 2021, 33, 97–104. [Google Scholar] [CrossRef]
- Federal Ministry of Labour, Social Affairs, Health and Consumer Protection. The Austrian Health Care System. Key Facts; Federal Ministry: Vienna, Austria, 2019; p. 36. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Austria: Country Health Profile 2019; European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- Dimai, H.P.; Svedbom, A.; Fahrleitner-Pammer, A.; Pieber, T.; Resch, H.; Zwettler, E.; Thaler, H.; Szivak, M.; Amrein, K.; Borgström, F. Epidemiology of proximal humeral fractures in Austria between 1989 and 2008. Osteoporos. Int. 2013, 24, 2413–2421. [Google Scholar] [CrossRef]
- Dimai, H.P.; Svedbom, A.; Fahrleitner-Pammer, A.; Resch, H.; Muschitz, C.; Thaler, H.; Szivak, M.; Amrein, K.; Borgström, F. Epidemiology of distal forearm fractures in Austria between 1989 and 2010. Osteoporos. Int. 2014, 25, 2297–2306. [Google Scholar] [CrossRef]
- Muschitz, C.; Hummer, M.; Grillari, J.; Hlava, A.; Birner, A.H.; Hemetsberger, M.; Dimai, H.P. Epidemiology and economic burden of fragility fractures in Austria. Osteoporos. Int. 2021, 33, 637–647. [Google Scholar] [CrossRef]
- Thomasius, F.; Baum, E.; Bernecker, P.; Böcker, W.; Brabant, T.; Clarenz, P.; Demary, W.; Dimai, H.P.; Engelbrecht, M.; Engelke, K.; et al. DVO Leitlinie 2017 zur Prophylaxe, Diagnostik und Therapie der Osteoporose bei postmenopausalen Frauen und Männern. Osteologie 2018, 27, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, A.; Major, G.; Holliday, E.; Attia, J.; Bogduk, N. Evidence of effectiveness of a fracture liaison service to reduce the re-fracture rate. Osteoporos. Int. 2016, 27, 873–879. [Google Scholar] [CrossRef] [Green Version]
- Walters, S.; Khan, T.; Ong, T.; Sahota, O. Fracture liaison services: Improving outcomes for patients with osteoporosis. Clin. Interv. Aging 2017, 12, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- STATcube—Statistische Datenbank. Statistik Austria. Available online: https://www.statistik.at/web_de/services/statcube/index.html (accessed on 13 May 2022).
- Cummings, S.R.; Eastell, R. Stop (mis)classifying fractures as high- or low-trauma or as fragility fractures. Osteoporos. Int. 2020, 31, 1023–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, A. comorbidity: An R package for computing comorbidity scores. J. Open Source Softw. 2018, 3, 648. [Google Scholar] [CrossRef] [Green Version]
- van Walraven, C.; Austin, P.C.; Jennings, A.; Quan, H.; Forster, A.J. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med. Care 2009, 47, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Menendez, M.E.; Neuhaus, V.; van Dijk, C.N.; Ring, D. The Elixhauser comorbidity method outperforms the Charlson index in predicting inpatient death after orthopaedic surgery. Clin. Orthop. Relat. Res. 2014, 472, 2878–2886. [Google Scholar] [CrossRef] [Green Version]
- R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Großschädl, F.; Stronegger, W.J. Long-term trends (1973–14) for obesity and educational inequalities among Austrian adults: Men in the fast lane. Eur. J. Public Health 2019, 29, 790–796. [Google Scholar] [CrossRef]
- Tang, X.; Liu, G.; Kang, J.; Hou, Y.; Jiang, F.; Yuan, W.; Shi, J. Obesity and risk of hip fracture in adults: A meta-analysis of prospective cohort studies. PLoS ONE 2013, 8, e55077. [Google Scholar] [CrossRef]
- Andrich, S.; Haastert, B.; Neuhaus, E.; Neidert, K.; Arend, W.; Ohmann, C.; Grebe, J.; Vogt, A.; Jungbluth, P.; Rösler, G.; et al. Epidemiology of Pelvic Fractures in Germany: Considerably High Incidence Rates among Older People. PLoS ONE 2015, 10, e0139078. [Google Scholar] [CrossRef]
- Curtis, E.M.; van der Velde, R.; Moon, R.J.; van den Bergh, J.P.; Geusens, P.; de Vries, F.; van Staa, T.P.; Cooper, C.; Harvey, N.C. Epidemiology of fractures in the United Kingdom 1988-2012: Variation with age, sex, geography, ethnicity and socioeconomic status. Bone 2016, 87, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeek, D.O.; Ponsen, K.J.; Fiocco, M.; Amodio, S.; Leenen, L.P.H.; Goslings, J.C. Pelvic fractures in the Netherlands: Epidemiology, characteristics and risk factors for in-hospital mortality in the older and younger population. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, L.; de Jongh, M.A.C.; de Munter, L.; Edwards, M.; Lansink, K.W.W. Prognostic factors and quality of life after pelvic fractures. The Brabant Injury Outcome Surveillance (BIOS) study. PLoS ONE 2020, 15, e0233690. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, E.P.; Moed, B.R. Venous thromboembolism after hospital discharge in pelvic and acetabular fracture patients treated operatively. J. Orthop. Surg. 2019, 27, 2309499019832815. [Google Scholar] [CrossRef] [PubMed]
- Oberkircher, L.; Ruchholtz, S.; Rommens, P.M.; Hofmann, A.; Bücking, B.; Krüger, A. Osteoporotic Pelvic Fractures. Dtsch. Arztebl. Int. 2018, 115, 70–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abernathy, B.R.; Schroder, L.K.; Bohn, D.C.; Switzer, J.A. Low-Energy Pelvic Ring Fractures: A Care Conundrum. Geriatr. Orthop. Surg. Rehabil. 2021, 12, 2151459320985406. [Google Scholar] [CrossRef]
- Lundin, N.; Huttunen, T.T.; Enocson, A.; Marcano, A.I.; Felländer-Tsai, L.; Berg, H.E. Epidemiology and mortality of pelvic and femur fractures—A nationwide register study of 417,840 fractures in Sweden across 16 years: Diverging trends for potentially lethal fractures. Acta Orthop. 2021, 92, 323–328. [Google Scholar] [CrossRef]
- Reito, A.; Kuoppala, M.; Pajulammi, H.; Hokkinen, L.; Kyrölä, K.; Paloneva, J. Mortality and comorbidity after non-operatively managed, low-energy pelvic fracture in patients over age 70: A comparison with an age-matched femoral neck fracture cohort and general population. BMC Geriatr. 2019, 19, 315. [Google Scholar] [CrossRef]
- Brozek, W.; Reichardt, B.; Kimberger, O.; Zwerina, J.; Dimai, H.P.; Kritsch, D.; Klaushofer, K.; Zwettler, E. Mortality after hip fracture in Austria 2008–2011. Calcif. Tissue Int. 2014, 95, 257–266. [Google Scholar] [CrossRef]
- Liow, M.H.L.; Ganesan, G.; Chen, J.D.Y.; Koh, J.S.B.; Howe, T.S.; Yong, E.L.; Kramer, M.S.; Tan, K.B. Excess mortality after hip fracture: Fracture or pre-fall comorbidity? Osteoporos. Int. 2021, 32, 2485–2492. [Google Scholar] [CrossRef]
- Feichtinger, X.; Kocijan, R.; Mittermayr, R.; Baierl, A.; Schanda, J.; Wakolbinger, R.; Resch, H.; Fialka, C.; Muschitz, C. Fracture patterns in patients with multiple fractures: The probability of multiple fractures and the most frequently associated regions. Eur. J. Trauma Emerg. Surg. 2020, 46, 1151–1158. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pelvic Fracture | Controls | p-Value a | |||||
|---|---|---|---|---|---|---|---|
| All n = 54,975 | Men, n (%) 16,022 (29.1) | Women, n (%) 38,953 (70.9) | All n = 54,975 | Men, n (%) 16,022 (29.1) | Women, n (%) 38,953 (70.9) | ||
| Age, mean (SD) | 76.6 (11.4) | 72.0 (12.0) | 78.5 (10.6) | 76.6 (11.4) | 72.0 (12.0) | 78.5 (10.6) | 1 |
| Age group, n (%) | 1 | ||||||
| 50–64 | 9552 (17.4%) | 4873 (30.4) | 4679 (12.0) | 9552 (17.4%) | 4873 (30.4) | 4679 (12.0) | |
| 65–79 | 19,549 (35.6) | 6279 (39.2) | 13,270 (34.1) | 19,549 (35.6) | 6279 (39.2) | 13,270 (34.1) | |
| ≥80 | 25,874 (47.1) | 4870 (30.4) | 21,004 (53.9) | 25,874 (47.1) | 4870 (30.4) | 21,004 (53.9) | |
| ECI score, mean (SD) | 8.2 (9.5) | 8.8 (10.0) | 8.0 (9.2) | 6.5 (8.4) | 7.1 (8.9) | 6.3 (8.2) | <0.001 |
| ECI, n (%) | |||||||
| <0 | 2978 (5.4) | 609 (3.8) | 2369 (6.1) | 1682 (3.1) | 315 (2.0) | 1367 (3.5) | |
| 0 | 15,908 (28.9) | 5107 (31.9) | 10,801 (27.7) | 12,090 (22.0) | 2992 (18.7) | 9098 (23.4) | |
| 1–4 | 5433 (9.9) | 1428 (8.9) | 4005 (10.3) | 3874 (7.0) | 1063 (6.6) | 2811 (7.2) | |
| ≥5 | 30,620 (55.7) | 8866 (55.3) | 21,754 (55.8) | 15,781 (28.7) | 4052 (25.3) | 11,729 (30.1) | |
| Not known/missing | 36 (0.1) | 12 (0.1) | 24 (0.1) | 21,548 (39.2) | 7600 (47.4) | 13,948 (35.8) | |
| Deceased, n (%) | 21,018 (38.2) | 5947 (37.1) | 15,071 (38.7) | 14,973 (27.2) | 3548 (22.1) | 11,425 (29.3) | <0.001 |
| Zero follow-up time, n (%) | 964 (0.9) | 427 (44.3) | 537 (55.7) | NA | NA | NA | |
| Follow-up time in months b, median (Interquartile range IQR) | 43.9 (22.7–73.4) | 43.2 (21.5–74.7) | 44.2 (23.2–73.1) | 44.3 (22.9–72.6) | 47.4 (25.1–77.0) | 42.9 (22.0–71.0) | 0.64 |
| Pelvic Fractures | Controls | |||||
|---|---|---|---|---|---|---|
| Age Group | All | Men | Women | All | Men | Women |
| 50–64 | 3.4% (n = 324) | 4.0% (n = 194) | 2.8% (n = 130) | 12.4% (n = 1181) | 9.6% (n = 467) | 15.3% (n = 714) |
| 65+ | 13.4% (n = 5951) | 16.9% (n = 1826) | 12.2% (n = 4125) | 11.0% (n = 4996) | 8.1% (n = 899) | 12.0% (n = 4097) |
| Total | 11.6 (n = 6275) | 13.0% (n = 2020) | 11.1% (n = 4255) | 11.2 (n = 6177) | 8.5% (n = 1366) | 12.4% (n = 4811) |
| Overall Mortality | ||||||||
|---|---|---|---|---|---|---|---|---|
| Age Group | Sex | Deaths | Follow-Up | Mortality Rate per 1000 PY | Model 1 | Model 2 | Model 3 | |
| 50–64 | Men | Controls | 1136 | 21,095.9 | 53.8 | Reference | Reference | Reference |
| PF | 587 | 24,554.9 | 23.9 | 0.46 (0.42–0.51) *** | 0.47 (0.42–0.51) *** | 0.32 (0.28–0.35) *** | ||
| Women | Controls | 1527 | 17,443.7 | 87.5 | Reference | Reference | Reference | |
| PF | 393 | 24,535.8 | 16.02 | 0.20 (0.18–0.23) *** | 0.20 (0.18–0.23) *** | 0.19 (0.17–0.21) *** | ||
| Total | Controls | 2663 | 38,539.7 | 69.1 | Reference | Reference | Reference | |
| PF | 980 | 49,090.7 | 20.0 | 0.31 (0.29–0.33) *** | 0.31 (0.29–0.34) *** | 0.25 (0.23–0.27) *** | ||
| 65+ | Men | Controls | 2412 | 48,513.7 | 49.7 | Reference | Reference | Reference |
| PF | 4933 | 39,508.0 | 124.9 | 2.44 (2.33–2.57) *** | 2.66 (2.53–2.79) *** | 1.36 (1.29–1.43) *** | ||
| Women | Controls | 9898 | 137,874.1 | 71.8 | Reference | Reference | Reference | |
| PF | 14,141 | 134,288.6 | 105.3 | 1.78 1 (1.72–1.83) *** | 1.79 1 (1.74–1.85) *** | 1.15 1 (1.10–1.19) *** | ||
| Total | Controls | 12,310 | 186,387.8 | 66.0 | Reference | Reference | Reference | |
| PF | 19,074 | 173,796.6 | 109.7 | 1.65 (1.62–1.69) *** | 1.75 (1.71–1.79) *** | 1.15 (1.12–1.17) *** | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behanova, M.; Haschka, J.; Reichardt, B.; Dimai, H.-P.; Resch, H.; Zwerina, J.; Kocijan, R. Pelvic Fractures—An Underestimated Problem? Incidence and Mortality Risk after Pelvic Fracture in Austria, 2010–2018. J. Clin. Med. 2022, 11, 2834. https://doi.org/10.3390/jcm11102834
Behanova M, Haschka J, Reichardt B, Dimai H-P, Resch H, Zwerina J, Kocijan R. Pelvic Fractures—An Underestimated Problem? Incidence and Mortality Risk after Pelvic Fracture in Austria, 2010–2018. Journal of Clinical Medicine. 2022; 11(10):2834. https://doi.org/10.3390/jcm11102834
Chicago/Turabian StyleBehanova, Martina, Judith Haschka, Berthold Reichardt, Hans-Peter Dimai, Heinrich Resch, Jochen Zwerina, and Roland Kocijan. 2022. "Pelvic Fractures—An Underestimated Problem? Incidence and Mortality Risk after Pelvic Fracture in Austria, 2010–2018" Journal of Clinical Medicine 11, no. 10: 2834. https://doi.org/10.3390/jcm11102834
APA StyleBehanova, M., Haschka, J., Reichardt, B., Dimai, H.-P., Resch, H., Zwerina, J., & Kocijan, R. (2022). Pelvic Fractures—An Underestimated Problem? Incidence and Mortality Risk after Pelvic Fracture in Austria, 2010–2018. Journal of Clinical Medicine, 11(10), 2834. https://doi.org/10.3390/jcm11102834