
Antibody Response to mRNA Vaccines against SARS-CoV-2 with Chronic Kidney Disease, Hemodialysis, and after Kidney Transplantation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Yanay, N.B.; Freiman, S.; Shapira, M.; Wishahi, S.; Hamze, M.; Elhaj, M.; Zaher, M.; Armaly, Z. Experience with SARS-CoV-2 BNT162b2 mRNA vaccine in dialysis patients. Kidney Int. 2021, 99, 1496–1498. [Google Scholar] [CrossRef]
- Grupper, A.; Sharon, N.; Finn, T.; Cohen, R.; Israel, M.; Agbaria, A.; Rechavi, Y.; Schwartz, I.F.; Schwartz, D.; Lellouch, Y.; et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1037–1042. [Google Scholar] [CrossRef]
- Billany, R.E.; Selvaskandan, H.; Adenwalla, S.F.; Hull, K.L.; March, D.S.; Burton, J.O.; Bishop, N.C.; Carr, E.J.; Beale, R.; Tang, J.W.; et al. Seroprevalence of antibody to S1 spike protein following vaccination against COVID-19 in patients receiving hemodialysis: A call to arms. Kidney Int. 2021, 99, 1492–1494. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier-Vargas, G.; Cognard, N.; Olagne, J.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Moulin, B.; Fafi-Kremer, S.; et al. Low immunization rates among kidney transplant recipients who received 2 doses of the mRNA-1273 SARS-CoV-2 vaccine. Kidney Int. 2021, 99, 1498–1500. [Google Scholar] [CrossRef]
- Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Eisenberger, U.; Gaeckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 2021, 13, 756. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transplant. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Attias, P.; Sakhi, H.; Rieu, P.; Soorkia, A.; Assayag, D.; Bouhroum, S.; Nizard, P.; El Karoui, K. Antibody response to the BNT162b2 vaccine in maintenance hemodialysis patients. Kidney Int. 2021, 99, 1490–1492. [Google Scholar] [CrossRef]
- Cucchiari, D.; Egri, N.; Bodro, M.; Herrera, S.; Del Risco-Zevallos, J.; Casals-Urquiza, J.; Cofan, F.; Moreno, A.; Rovira, J.; Banon-Maneus, E.; et al. Cellular and humoral response after MRNA-1273 SARS-CoV-2 vaccine in kidney transplant recipients. Am. J. Transplant. 2021, 21, 2727–2739. [Google Scholar] [CrossRef]
- Rozen-Zvi, B.; Yahav, D.; Agur, T.; Zingerman, B.; Ben-Zvi, H.; Atamna, A.; Tau, N.; Mashraki, T.; Nesher, E.; Rahamimov, R. Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: A prospective cohort study. Clin. Microbiol. Infect. 2021, 27, 1173.e1–1173.e4. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Montez-Rath, M.E.; Han, J.; Garcia, P.; Cadden, L.; Hunsader, P.; Kerschmann, R.; Beyer, P.; Dittrich, M.; Block, G.A.; et al. Antibody Response to COVID-19 Vaccination in Patients Receiving Dialysis. J. Am. Soc. Nephrol. 2021, 32, 2435–2438. [Google Scholar] [CrossRef]
- Kaiser, R.A.; Haller, M.C.; Apfalter, P.; Kerschner, H.; Cejka, D. Comparison of BNT162b2 (Pfizer–BioNtech) and mRNA-1273 (Moderna) SARS-CoV-2 mRNA vaccine immunogenicity in dialysis patients. Kidney Int. 2021, 100, 697–698. [Google Scholar] [CrossRef]
- Van Praet, J.; Reynders, M.; de Bacquer, D.; Viaene, L.; Schoutteten, M.; Caluwé, R.; Doubel, P.; Heylen, L.; De Bel, A.V.; Van Vlem, B.; et al. Predictors and Dynamics of the Humoral and Cellular Immune Response to SARS-CoV-2 mRNA Vaccines in Hemodialysis Patients: A Multicenter Observational Study. J. Am. Soc. Nephrol. 2021, 32, 3208–3220. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Dębska-Ślizień, A.; Ślizień, Z.; Muchlado, M.; Kubanek, A.; Piotrowska, M.; Dąbrowska, M.; Tarasewicz, A.; Chamienia, A.; Biedunkiewicz, B.; Renke, M.; et al. Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study-The COViNEPH Project. Vaccines 2021, 9, 1165. [Google Scholar] [CrossRef]
- Kantauskaite, M.; Müller, L.; Kolb, T.; Fischer, S.; Hillebrandt, J.; Ivens, K.; Andree, M.; Luedde, T.; Orth, H.M.; Adams, O.; et al. Intensity of mycophenolate mofetil treatment is associated with an impaired immune response to SARS-CoV-2 vaccination in kidney transplant recipients. Am. J. Transplant. 2021, 1–6. [Google Scholar] [CrossRef]
- Chavarot, N.; Ouedrani, A.; Marion, O.; Leruez-Ville, M.; Vilain, E.; Baaziz, M.; Del Bello, A.; Burger, C.; Sberro-Soussan, R.; Martinez, F.; et al. Poor Anti-SARS-CoV-2 Humoral and T-cell Responses After 2 Injections of mRNA Vaccine in Kidney Transplant Recipients Treated with Belatacept. Transplantation 2021, 105, e94–e95. [Google Scholar] [CrossRef] [PubMed]
- Terrec, F.; Jouve, T.; Malvezzi, P.; Janbon, B.; Naciri Bennani, H.; Rostaing, L.; Noble, J. Belatacept Use after Kidney Transplantation and Its Effects on Risk of Infection and COVID-19 Vaccine Response. J. Clin. Med. 2021, 10, 5159. [Google Scholar] [CrossRef] [PubMed]
- Moor, M.B.; Suter-Riniker, F.; Horn, M.P.; Aeberli, D.; Amsler, J.; Möller, B.; Njue, L.M.; Medri, C.; Angelillo-Scherrer, A.; Borradori, L.; et al. Humoral and cellular responses to mRNA vaccines against SARS-CoV-2 in patients with a history of CD20 B-cell-depleting therapy (RituxiVac): An investigator-initiated, single-centre, open-label study. Lancet Rheumatol. 2021, 3, e789–e797. [Google Scholar] [CrossRef]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambuehl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Gansevoort, R.T.; Hilbrands, L.B. CKD is a key risk factor for COVID-19 mortality. Nat. Rev. Nephrol. 2020, 16, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-J.; Lee, T.H.; Tian, Y.-C.; Lee, C.-C.; Fan, P.-C.; Chang, C.-H. Immunogenicity Rates after SARS-CoV-2 Vaccination in People with End-stage Kidney Disease: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2131749. [Google Scholar] [CrossRef]
- Grupper, A.; Katchman, E.; Ben-Yehoyada, M.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Shashar, M.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Kidney transplant recipients vaccinated before transplantation maintain superior humoral response to SARS-CoV-2 vaccine. Clin. Transplant. 2021, 35, e14478. [Google Scholar] [CrossRef]
- Blanchard-Rohner, G.; Enriquez, N.; Lemaître, B.; Cadau, G.; Combescure, C.; Giostra, E.; Hadaya, K.; Meyer, P.; Gasche-Soccal, P.M.; Berney, T.; et al. Usefulness of a systematic approach at listing for vaccine prevention in solid organ transplant candidates. Am. J. Transplant. 2019, 19, 512–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Westhoff, T.H.; Seibert, F.S.; Anft, M.; Blazquez-Navarro, A.; Skrzypczyk, S.; Zgoura, P.; Meister, T.L.; Pfaender, S.; Stumpf, J.; Hugo, C.; et al. A third vaccine dose substantially improves humoral and cellular SARS-CoV-2 immunity in renal transplant recipients with primary humoral nonresponse. Kidney Int. 2021, 100, 1135–1136. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients with Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef]
- Masset, C.; Kerleau, C.; Garandeau, C.; Ville, S.; Cantarovich, D.; Hourmant, M.; Kervella, D.; Houzet, A.; Guillot-Gueguen, C.; Guihard, I.; et al. A third injection of the BNT162b2 mRNA COVID-19 vaccine in kidney transplant recipients improves the humoral immune response. Kidney Int. 2021, 100, 1132–1135. [Google Scholar] [CrossRef] [PubMed]
- Bensouna, I.; Caudwell, V.; Kubab, S.; Acquaviva, S.; Pardon, A.; Vittoz, N.; Dogan-Firat, B.; Hanafi, L.; Faucon, A.L.; Housset, P. SARS-CoV-2 Antibody Response After a Third Dose of the BNT162b2 Vaccine in Patients Receiving Maintenance Hemodialysis or Peritoneal Dialysis. Am. J. Kidney Dis. 2021; in press. [Google Scholar]
- Dekervel, M.; Henry, N.; Torreggiani, M.; Pouteau, L.-M.; Imiela, J.-P.; Mellaza, C.; Garnier, A.S.; Dujardin, A.; Asfar, M.; Ducancelle, A.; et al. Humoral response to a third injection of BNT162b2 vaccine in patients on maintenance haemodialysis. Clin. Kidney J. 2021, 14, 2349–2355. [Google Scholar] [CrossRef] [PubMed]
- Alejo, J.L.; Mitchell, J.; Chiang, T.P.-Y.; Abedon, A.T.; Boyarsky, B.J.; Avery, R.K.; Tobian, A.A.R.; Levan, M.L.; Massie, A.B.; Garonzik-Wang, J.M.; et al. Antibody Response to a Fourth Dose of a SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Transplantation 2021, 105, e280. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.-S.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Froelke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC Immune-response Study: The Immunogenicity, Tolerability, and Safety of COVID-19 Vaccination in Patients with Chronic Kidney Disease, on Dialysis, or Living with a Kidney Transplant. Transplantation, 2021; in press. [Google Scholar]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Vaquera, S.M.; Mantecón, C.J.J.; Useche, G.; Sánchez Márquez, M.G.; Carnerero, M.; Jaldo Rodríguez, M.-T.; Ramos, P.M.; et al. Safety and immediate humoral response of COVID-19 vaccines in chronic kidney disease patients: The SENCOVAC study. Nephrol. Dial. Transplant. 2021; in press. [Google Scholar]
- Thieme, C.J.; Blazquez-Navarro, A.; Safi, L.; Kaliszczyk, S.; Paniskaki, K.; Neumann, I.E.; Schmidt, K.; Stockhausen, M.; Hoerstrup, J.; Cinkilic, O.; et al. Impaired Humoral but Substantial Cellular Immune Response to Variants of Concern B1.1.7 and B.1.351 in Hemodialysis Patients after Vaccination with BNT162b2. J. Am. Soc. Nephrol. 2021, 32, 2725–2727. [Google Scholar] [CrossRef]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D. Humoral and cellular immune response and safety of two-dose SARS-CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 12, 3980–3989. [Google Scholar] [CrossRef]
- Pedersen, R.M.; Bang, L.L.; Tornby, D.S.; Kierkegaard, H.; Nilsson, A.C.; Johansen, I.S.; Bistrup, C.; Jensen, T.G.; Justesen, U.S.; Andersen, T.E. The SARS-CoV-2-neutralizing capacity of kidney transplant recipients 4 weeks after receiving a second dose of the BNT162b2 vaccine. Kidney Int. 2021, 100, 1129–1131. [Google Scholar] [CrossRef]
- Hod, T.; Ben-David, A.; Olmer, L.; Levy, I.; Ghinea, R.; Mor, E.; Lustig, Y.; Rahav, G. Humoral Response of Renal Transplant Recipients to the BNT162b2 SARS-CoV-2 mRNA Vaccine Using Both RBD IgG and Neutralizing Antibodies. Transplantation 2021, 105, e234–e243. [Google Scholar] [CrossRef]
- Connolly, C.; Koenig, D.; Ravi, S.; Azar, A.; Kant, S.; Dalal, M.; Duchen, J.; Seo, P.; Antiochos, B.; Paik, J.P.; et al. Correspondence on “SARS-CoV-2 vaccination in rituximab-treated patients: Evidence for impaired humoral but inducible cellular immune response” by Bonelli et al. Ann. Rheum. Dis. 2021, 80, e164. [Google Scholar] [CrossRef] [PubMed]
- Kronbichler, A.; Geetha, D.; Smith, R.M.; Egan, A.C.; Bajema, I.M.; Schönemarck, U.; Mahr, A.; Anders, H.J.; Bruchfeld, A.; Cid, M.C.; et al. The COIVD-19 pandemic and ANCA-associated vasculitis—Reports from the EUVAS meeting and EUVAS education forum. Autoimmun. Rev. 2021, 20, 102986. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.J.; Hall, J.A.; Zaidi, A.; Andrews, N.J.; Dunbar, J.K.; Dabrera, G. Effect of vaccination on household transmission of SARS-CoV-2 in England. N. Engl. J. Med. 2021, 385, 759–760. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| CKD (n = 160) | HD (n = 206) | KTR (n = 216) | |
|---|---|---|---|
| Age (years) | 63.1 (53.5–74.5) | 69.5 (57.5–78.6) | 59.9 (50.7–68.5) |
| Female (n, %) | 66 (41) | 66 (32) | 69 (32) |
| BMI (kg/m2) | 25.6 (23.3–29.3) | 24.9 (22.2–28.4) | 24.8 (21.7–27.8) |
| Primary renal disease (n, %) | |||
| Diabetic nephropathy | 14 (9) | 45 (22) | 28 (13) |
| Glomerulonephritis | 64 (40) | 35 (17) | 71 (33) |
| Other | 49 (31) | 55 (27) | 77 (36) |
| Unknown | 3 (2) | 23 (11) | 11 (5) |
| Vascular nephropathy | 30 (19) | 48 (23) | 29 (13) |
| Comorbidities (n) | |||
| Cardiovascular disease | 45 | 98 | 92 |
| Cerebrovascular disease | 16 | 33 | 34 |
| Active or former malignancy | 13 | 35 | 53 |
| Diabetes mellitus | 36 | 77 | 79 |
| Comedication (n, %) | |||
| Treatment with RAAS inhibitors | 83 (52) | 62 (30) | 93 (43) |
| High-dose glucocorticoid treatment during last year (≥1 mg/kg) | 6 (4) | 4 (2) | 16 (7) |
| Tacrolimus | - | 7 (3) | 152 (70) |
| Cyclosporine A | - | 1 (0.5) | 38 (18) |
| Azathioprine | - | 0 | 33 (15) |
| Mycophenolic acid | - | 2 (1) | 148 (69) |
| Belatacept | - | 0 | 14 (6) |
| Glucocorticoids | - | 8 (4) | 178 (82) |
| mTor inhibitors | - | 0 | 11 (5) |
| Rituximab | 30 (19) | - | - |
| Time between 1st vaccination and rituximab (days) | 242 (127–324) | 2 (1–4) | 2 (1–3) |
| Classes of antihypertensive drugs (n) | 2 (1–3) | ||
| Laboratory values | |||
| Albumin (g/dL) | 4.0 (3.7–4.3) | 3.8 (3.4–4.1) | |
| Hemoglobin (g/dL) | 132 (117–141) | 111 (105–120) | 4.1 (3.9–4.4) |
| C-reactive protein (mg/dL) | 0.20 (0.09–0.46) | 0.33 (0.16–0.95) | 134 (122–146) |
| eGFR (mL/min/1.73 m2) | 29.9 (19.8–49.9) | - | 0.19 (0.08–0.40) |
| CKD (n = 160) | HD (n = 206) | KTR (n = 216) | |
|---|---|---|---|
| Type of antibody measurement (n, %) | |||
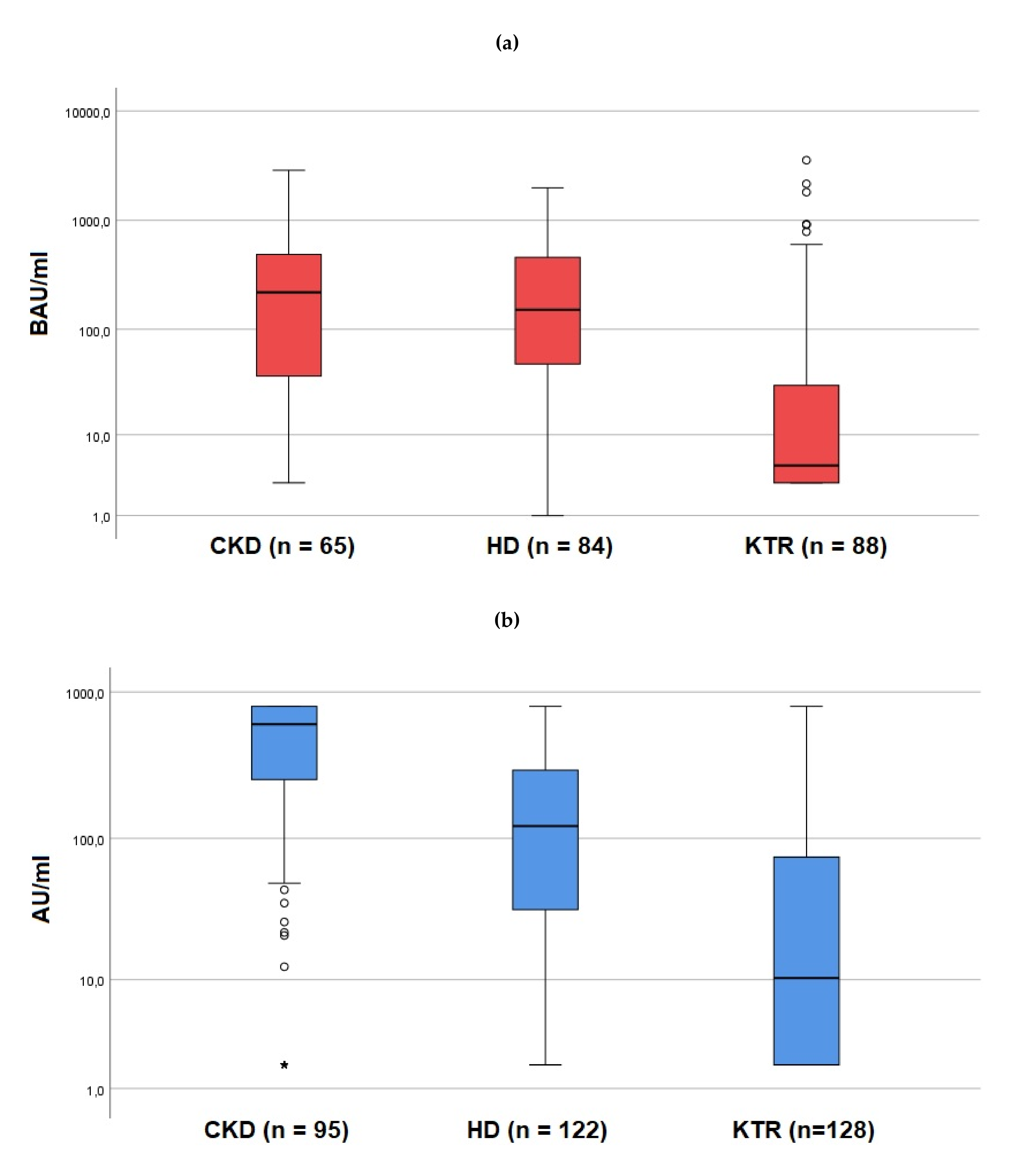
| Abbott SARS-CoV-2 IgG II Quant Assay | 65 (40.6) | 84 (40.8) | 88 (40.7) |
| Liaison® SARS-CoV-2 S1/S2 IgG | 95 (59.4) | 122 (59.2) | 128 (59.3) |
| Vaccine (n, %) | |||
| BNT162b2 | 93 (58.1) | 198 (96.1) | 106 (49.1) |
| mRNA-1273 | 67 (41.9) | 8 (3.9) | 110 (50.9) |
| Results of antibody measurement | |||
| Abbott SARS-CoV-2 IgG II Quant Assay titer (BAU/mL) | 230.3 (48.3–497.6) | 151.6 (47.7–458.4) | 4.75 (3.0–30.2) |
| Liaison® SARS-CoV-2 S1/S2 IgG titer (AU/mL) | 602.0 (252.5–800.0) | 121.5 (32.0–293.0) | 10.3 (1.9–74.3) |
| Non-response (n, %) | 20 (12.5) | 25 (12.1) | 108 (50.0) |
| Time between 1st vaccination and AB measurement (days) | 91 (90–96) | 91 (88–94) | 91 (90–95) |
| OR (95% CI) | p-Value | |
|---|---|---|
| Glomerulonephritis | 1.53 (0.24–9.75) | 0.651 |
| Rituximab treatment | 27.20 (5.12–144.63) | <0.001 |
| Days between 1st vaccination and Rituximab (per day) | 0.98 (0.96–1.00) | 0.020 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Glomerulonephritis | 2.87 (0.95–8.70) | 0.062 |
| High-dose glucocorticoid treatment during last year (≥1 mg/kg) | 6.36 (0.67–60.44) | 0.107 |
| Treatment with tacrolimus or cyclosporine A | 14.85 (2.68–82.43) | 0.002 |
| Glucocorticoids | 1.90 (0.25–14.49) | 0.537 |
| Hemoglobin (per g/dL) | 0.97 (0.95–1.01) | 0.098 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Age (per year) | 1.06 (1.03–1.09) | <0.001 |
| Type of vaccination | ||
| BNT162b2 | Ref. | - |
| mRNA-1273 | 0.41 (0.20-0.83) | 0.014 |
| Cerebrovascular disease | 3.11 (0.99–9.76) | 0.052 |
| CMV reactivation during the last 6 months | 1.22 (0.47–3.18) | 0.681 |
| Basis of immunosuppression | ||
| Antimetabolite and/or steroids | Ref. | - |
| Cyclosporine A | 0.89 (0.06–14.23) | 0.934 |
| Tacrolimus | 1.59 (0.11–22.38) | 0.730 |
| mTOR inhibitors | 0.31 (0.01–10.42) | 0.512 |
| Belatacept | 11.01 (0.45–269.68) | 0.142 |
| Antimetabolites | ||
| No antimetabolites | Ref. | - |
| Azathioprine | 0.73 (0.18–2.92) | 0.652 |
| Mycophenolic acid | 6.61 (2.31–18.86) | <0.001 |
| Glucocorticoids | 4.95 (1.48–16.57) | 0.010 |
| Hemoglobin (per g/dL) | 0.97 (0.95–0.99) | <0.001 |
| Time since last KT (per year) | 0.99 (0.94–1.04) | 0.660 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchwinkler, L.; Solagna, C.A.; Messner, J.; Pirklbauer, M.; Rudnicki, M.; Mayer, G.; Kerschbaum, J. Antibody Response to mRNA Vaccines against SARS-CoV-2 with Chronic Kidney Disease, Hemodialysis, and after Kidney Transplantation. J. Clin. Med. 2022, 11, 148. https://doi.org/10.3390/jcm11010148
Buchwinkler L, Solagna CA, Messner J, Pirklbauer M, Rudnicki M, Mayer G, Kerschbaum J. Antibody Response to mRNA Vaccines against SARS-CoV-2 with Chronic Kidney Disease, Hemodialysis, and after Kidney Transplantation. Journal of Clinical Medicine. 2022; 11(1):148. https://doi.org/10.3390/jcm11010148
Chicago/Turabian StyleBuchwinkler, Lukas, Claire Anne Solagna, Janosch Messner, Markus Pirklbauer, Michael Rudnicki, Gert Mayer, and Julia Kerschbaum. 2022. "Antibody Response to mRNA Vaccines against SARS-CoV-2 with Chronic Kidney Disease, Hemodialysis, and after Kidney Transplantation" Journal of Clinical Medicine 11, no. 1: 148. https://doi.org/10.3390/jcm11010148
APA StyleBuchwinkler, L., Solagna, C. A., Messner, J., Pirklbauer, M., Rudnicki, M., Mayer, G., & Kerschbaum, J. (2022). Antibody Response to mRNA Vaccines against SARS-CoV-2 with Chronic Kidney Disease, Hemodialysis, and after Kidney Transplantation. Journal of Clinical Medicine, 11(1), 148. https://doi.org/10.3390/jcm11010148