
Association between Nafamostat Mesylate and In-Hospital Mortality in Patients with Coronavirus Disease 2019: A Multicenter Observational Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
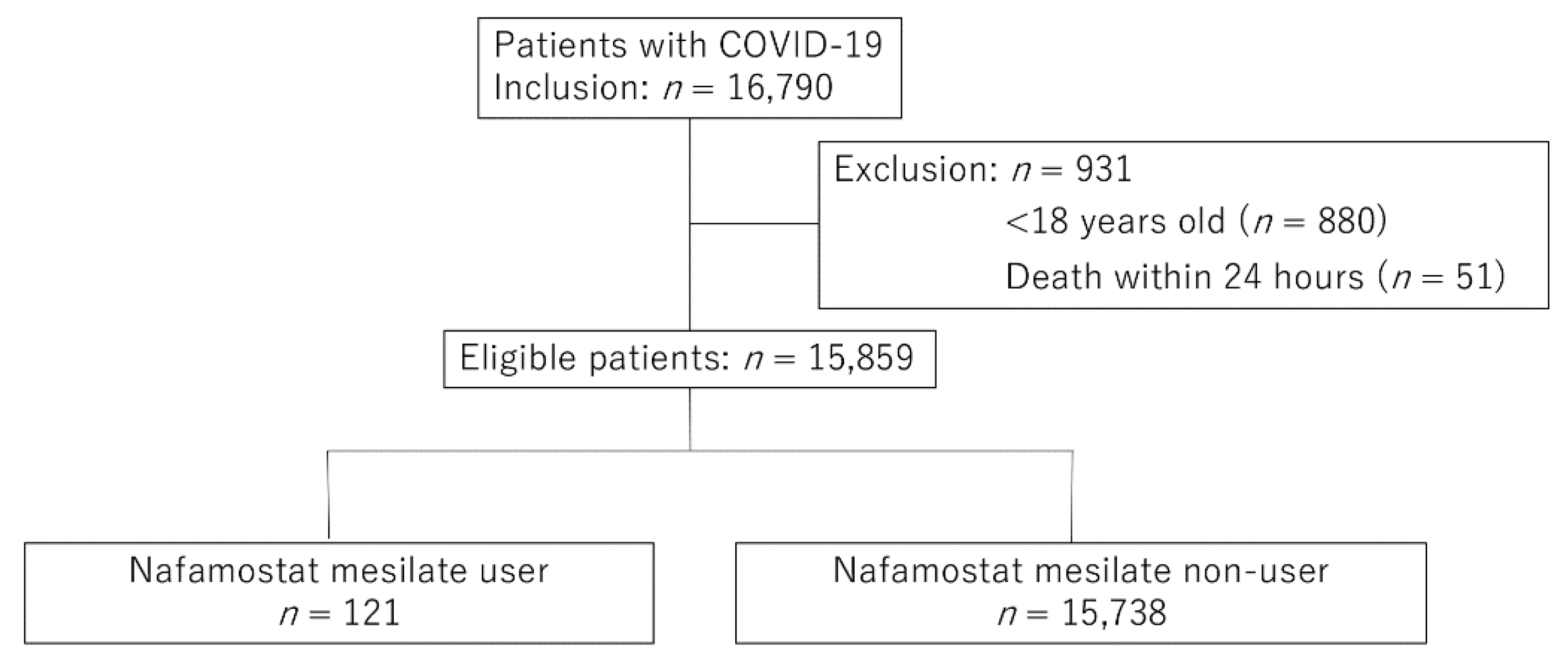
2.2. Study Participants and Exposure Variable
2.3. Outcome and Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, W.; Yoneda, T.; Koba, H.; Ueda, T.; Tsuji, N.; Ogawa, H.; Asakura, H. Potential mechanisms of nafamostat therapy for severe COVID-19 pneumonia with disseminated intravascular coagulation. Int. J. Infect. Dis. 2020, 102, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [Green Version]
- Cho, T.; Han, H.-S.; Jeong, J.; Park, E.-M.; Shim, K.-S. A Novel Computational Approach for the Discovery of Drug Delivery System Candidates for COVID-19. Int. J. Mol. Sci. 2021, 22, 2815. [Google Scholar] [CrossRef]
- Yamamoto, M.; Kiso, M.; Sakai-Tagawa, Y.; Iwatsuki-Horimoto, K.; Imai, M.; Takeda, M.; Kinoshita, N.; Ohmagari, N.; Gohda, J.; Semba, K.; et al. The Anticoagulant Nafamostat Potently Inhibits SARS-CoV-2 S Protein-Mediated Fusion in a Cell Fusion Assay System and Viral Infection In Vitro in a Cell-Type-Dependent Manner. Viruses 2020, 12, 629. [Google Scholar] [CrossRef] [PubMed]
- Iwasaka, S.; Shono, Y.; Tokuda, K.; Nakashima, K.; Yamamoto, Y.; Maki, J.; Nagasaki, Y.; Shimono, N.; Akahoshi, T.; Taguchi, T. Clinical improvement in a patient with severe coronavirus disease 2019 after administration of hydroxychloroquine and continuous hemodiafiltlation with nafamostat mesylate. J. Infect. Chemother. 2020, 26, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Doi, K.; the COVID-UTH Study Group; Ikeda, M.; Hayase, N.; Moriya, K.; Morimura, N. Nafamostat mesylate treatment in combination with favipiravir for patients critically ill with COVID-19: A case series. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef]
- Jang, S.; Rhee, J.-Y. Three cases of treatment with nafamostat in elderly patients with COVID-19 pneumonia who need oxygen therapy. Int. J. Infect. Dis. 2020, 96, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Zhuravel, S.V.; Khmelnitskiy, O.K.; Burlaka, O.O.; Gritsan, A.I.; Goloshchekin, B.M.; Kim, S.; Hong, K.Y. Nafamostat in hospitalized patients with moderate to severe COVID-19 pneumonia: A randomised Phase II clinical trial. EClinicalMedicine 2021, 41, 101169. [Google Scholar] [CrossRef]
- Yamana, H.; Moriwaki, M.; Horiguchi, H.; Kodan, M.; Fushimi, K.; Yasunaga, H. Validity of diagnoses, procedures, and laboratory data in Japanese administrative data. J. Epidemiology 2017, 27, 476–482. [Google Scholar] [CrossRef]
- Suissa, S. Immortal time bias in pharmaco-epidemiology. Am. J. Epidemiol. 2008, 167, 492–499. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, K.; Wada, K.; Takahara, T.; Shirotani, T. Indications for Computed Tomography in Patients With Mild Head Injury. Neurol. Med. -Chir. 2007, 47, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, D.B.; Schenker, N. Multiple imputation in health-care databases: An overview and some applications. Stat. Med. 1991, 10, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Aloisio, K.M.; Micali, N.; Swanson, S.A.; Field, A.; Horton, N.J. Analysis of Partially Observed Clustered Data using Generalized Estimating Equations and Multiple Imputation. Stata Journal: Promot. Commun. Stat. Stata 2014, 14, 863–883. [Google Scholar] [CrossRef] [Green Version]
- Brookhart, M.A.; Schneeweiss, S.; Rothman, K.; Glynn, R.J.; Avorn, J.; Stürmer, T. Variable Selection for Propensity Score Models. Am. J. Epidemiol. 2006, 163, 1149–1156. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, P.R.; Rubin, D.B. Constructing a Control Group Using Multivariate Matched Sampling Methods That Incorporate the Propensity Score. Am. Stat. 1985, 39, 33–38. [Google Scholar]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.B. Propensity score methods. Am. J. Ophthalmol. 2010, 149, 7–9. [Google Scholar] [CrossRef]
- Doi, K.; Nishida, O.; Shigematsu, T.; Sadahiro, T.; Itami, N.; Iseki, K.; Yuzawa, Y.; Okada, H.; Koya, D.; Kiyomoto, H.; et al. The Japanese Clinical Practice Guideline for acute kidney injury 2016. J. Intensiv. Care 2018, 6, 48. [Google Scholar] [CrossRef] [Green Version]
- Attah, A.F.; Fagbemi, A.A.; Olubiyi, O.; Dada-Adegbola, H.; Oluwadotun, A.; Elujoba, A.; Babalola, C.P. Therapeutic Potentials of Antiviral Plants Used in Traditional African Medicine With COVID-19 in Focus: A Nigerian Perspective. Front. Pharmacol. 2021, 12, 596855. [Google Scholar] [CrossRef]
- Abduljabbar, M.H. Clinical efficacy of Nafamostat Mesylate in combination with Favipiravir for COVID-19 pneumonia treatment review article. Ann. Med. Surg. 2021, 68, 102560. [Google Scholar] [CrossRef] [PubMed]
- WHO. Update to living WHO guideline on drugs for COVID-19. BMJ 2021, 374, n1703. Available online: https://www.bmj.com/content/374/bmj.n1703.long (accessed on 6 November 2021).
- Hoffmann, M.; Schroeder, S.; Kleine-Weber, H.; Müller, M.A.; Drosten, C.; Pöhlmann, S. Nafamostat Mesylate Blocks Activation of SARS-CoV-2: New Treatment Option for COVID-19. Antimicrob. Agents Chemother. 2020, 64, e00754-20. [Google Scholar] [CrossRef] [Green Version]
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda, A.; Suzuki, K.; Endo, M.; et al. Clinical epidemiology of hospitalized patients with COVID-19 in Japan: Report of the COVID-19 REGISTRY JAPAN. Clin. Infect. Dis. 2020, 73, e3677–e3689. [Google Scholar] [CrossRef]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, L.; Garg, S.; O’Halloran, A.; Whitaker, M.; Pham, H.; Anderson, E.J.; Armistead, I.; Bennett, N.M.; Billing, L.; Como-Sabetti, K.; et al. Risk Factors for Intensive Care Unit Admission and In-hospital Mortality Among Hospitalized Adults Identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clin. Infect. Dis. 2020, 72, e206–e214. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Unmatched Group | ||
|---|---|---|
| Nafamostat Mesylate | Control | |
| Number of patients | 121 | 15,738 |
| Age (years), mean ± SD 1 | 69.9 ± 15.0 | 61.8 ± 22.2 |
| Male (%) | 68.6 | 57.1 |
| Charlson comorbidity index (%) | ||
| 0 | 43.8 | 52.1 |
| 1 | 9.9 | 9.1 |
| 2 | 25.6 | 16.4 |
| 3 | 8.3 | 5.8 |
| ≥4 | 12.4 | 16.6 |
| Diabetes mellitus (%) | 40.5 | 22.5 |
| Ischemic heart disease (%) | 5.8 | 7.7 |
| Cirrhosis (%) | 0.8 | 1.4 |
| Chronic lung disease (%) | 18.2 | 17.9 |
| Cancer (%) | 12.4 | 13.5 |
| Chronic kidney disease (%) | 24.8 | 6.4 |
| Body mass index (%) | ||
| <18.5 | 10.4 | 16.3 |
| 18.5–25.0 | 59.1 | 58.0 |
| 25–30 | 20.0 | 19.1 |
| ≥30 | 10.4 | 6.6 |
| Smoking (%) | 35.9 | 34.1 |
| Japan Coma Scale (%) | ||
| 0 (clear) | 66.1 | 83.9 |
| 1–3 (delirium) | 22.3 | 12.7 |
| 10–30 (somnolence) | 4.1 | 2.3 |
| 100–300 (coma) | 7.4 | 1.1 |
| VKA 2 (%) | 1.7 | 1.5 |
| DOAC 3 (%) | 4.1 | 4.3 |
| Antiplatelet (%) | 9.1 | 6.1 |
| Interhospital transfer (%) | 16.5 | 5.9 |
| Number of beds (%) | ||
| <200 | 2.5 | 6.5 |
| 200–400 | 33.9 | 56.6 |
| ≥400 | 63.6 | 36.9 |
| ICU 4 admission (%) | 37.2 | 4.6 |
| Nafamostat Mesylate | Control | |
|---|---|---|
| Initial antibiotics (%) | 25.6 | 7.8 |
| Heparin (%) | 14.0 | 2.6 |
| Daluteparin (%) | 0.8 | 0.1 |
| Dobutamine (%) | 2.5 | 0.2 |
| Noradrenalin (%) | 14.9 | 1.0 |
| Vasopressin (%) | 4.1 | 0.1 |
| Steroids | ||
| Dexamethasone (%) | 19.0 | 4.9 |
| Other steroids (%) | 19.8 | 6.1 |
| Blood transfusion (%) | ||
| Red blood cells (%) | 4.1 | 0.9 |
| Platelets (%) | 1.7 | 0.1 |
| Fresh frozen plasma (%) | 2.5 | 0.0 |
| Oxygen therapy (%) | 47.9 | 26.3 |
| NPPV 1 (%) | 1.7 | 0.3 |
| Mechanical ventilation (%) | 19.8 | 1.7 |
| IRRT 2 (%) | 17.4 | 1.3 |
| CRRT 3 (%) | 10.7 | 0.1 |
| ECMO 4 (%) | 2.5 | 0.1 |
| Effect Estimate | p-Value | |
|---|---|---|
| In-hospital mortality | ||
| No nafamostat mesylate | 1 (Reference) | |
| Nafamostat mesylate | 1.27 (0.61–2.64) | 0.52 |
| Sensitivity analyses (in-hospital mortality) | ||
| No nafamostat mesylate | 1 (Reference) | |
| Nafamostat mesylate | ||
| Exclusion of patients undergoing IRRT 1 or CRRT 2 | 1.03 (0.39–2.71) | 0.94 |
| Complete cases | 1.32 (0.62–2.82) | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inokuchi, R.; Kuno, T.; Komiyama, J.; Uda, K.; Miyamoto, Y.; Taniguchi, Y.; Abe, T.; Ishimaru, M.; Adomi, M.; Tamiya, N.; et al. Association between Nafamostat Mesylate and In-Hospital Mortality in Patients with Coronavirus Disease 2019: A Multicenter Observational Study. J. Clin. Med. 2022, 11, 116. https://doi.org/10.3390/jcm11010116
Inokuchi R, Kuno T, Komiyama J, Uda K, Miyamoto Y, Taniguchi Y, Abe T, Ishimaru M, Adomi M, Tamiya N, et al. Association between Nafamostat Mesylate and In-Hospital Mortality in Patients with Coronavirus Disease 2019: A Multicenter Observational Study. Journal of Clinical Medicine. 2022; 11(1):116. https://doi.org/10.3390/jcm11010116
Chicago/Turabian StyleInokuchi, Ryota, Toshiki Kuno, Jun Komiyama, Kazuaki Uda, Yoshihisa Miyamoto, Yuta Taniguchi, Toshikazu Abe, Miho Ishimaru, Motohiko Adomi, Nanako Tamiya, and et al. 2022. "Association between Nafamostat Mesylate and In-Hospital Mortality in Patients with Coronavirus Disease 2019: A Multicenter Observational Study" Journal of Clinical Medicine 11, no. 1: 116. https://doi.org/10.3390/jcm11010116
APA StyleInokuchi, R., Kuno, T., Komiyama, J., Uda, K., Miyamoto, Y., Taniguchi, Y., Abe, T., Ishimaru, M., Adomi, M., Tamiya, N., & Iwagami, M. (2022). Association between Nafamostat Mesylate and In-Hospital Mortality in Patients with Coronavirus Disease 2019: A Multicenter Observational Study. Journal of Clinical Medicine, 11(1), 116. https://doi.org/10.3390/jcm11010116