
MRI-Based Quantitation of Hepatic Steatosis Does Not Predict Hypertrophy Rate after Portal Vein Embolization in Patients with Colorectal Liver Metastasis and Normal to Moderately Elevated Fat Fraction

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
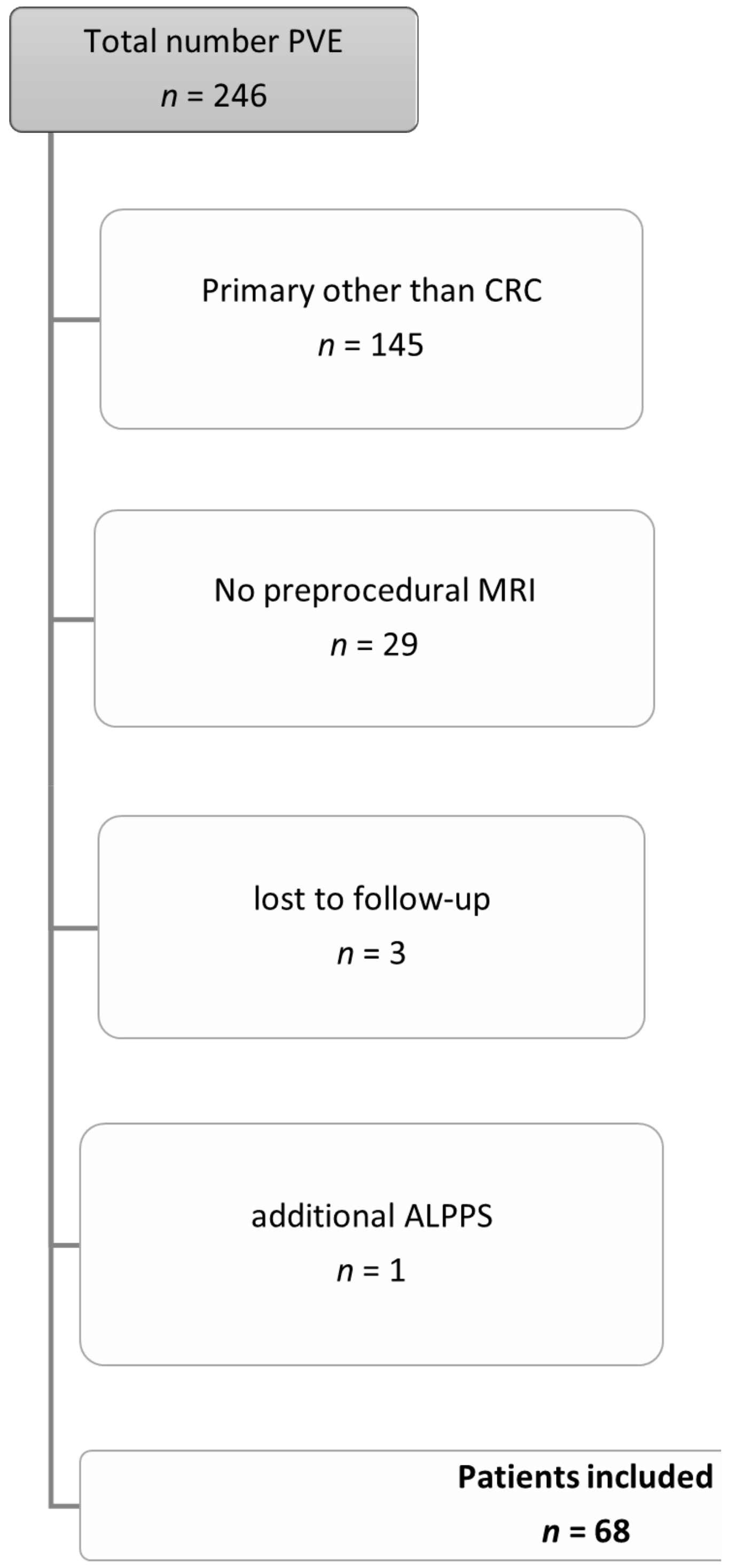
2.1. Patient Cohort
2.2. Preprocedural MRI-Protocol
2.3. Pre-/ and Postinterventional CT imaging
2.4. Portal Vein Embolization Procedure
2.5. Data Analysis
2.5.1. Determining hFF
2.5.2. Determining the Hypertrophy Rate of the FLR
2.6. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Volume of FLR
3.3. MRI Hepatic Fat Fraction
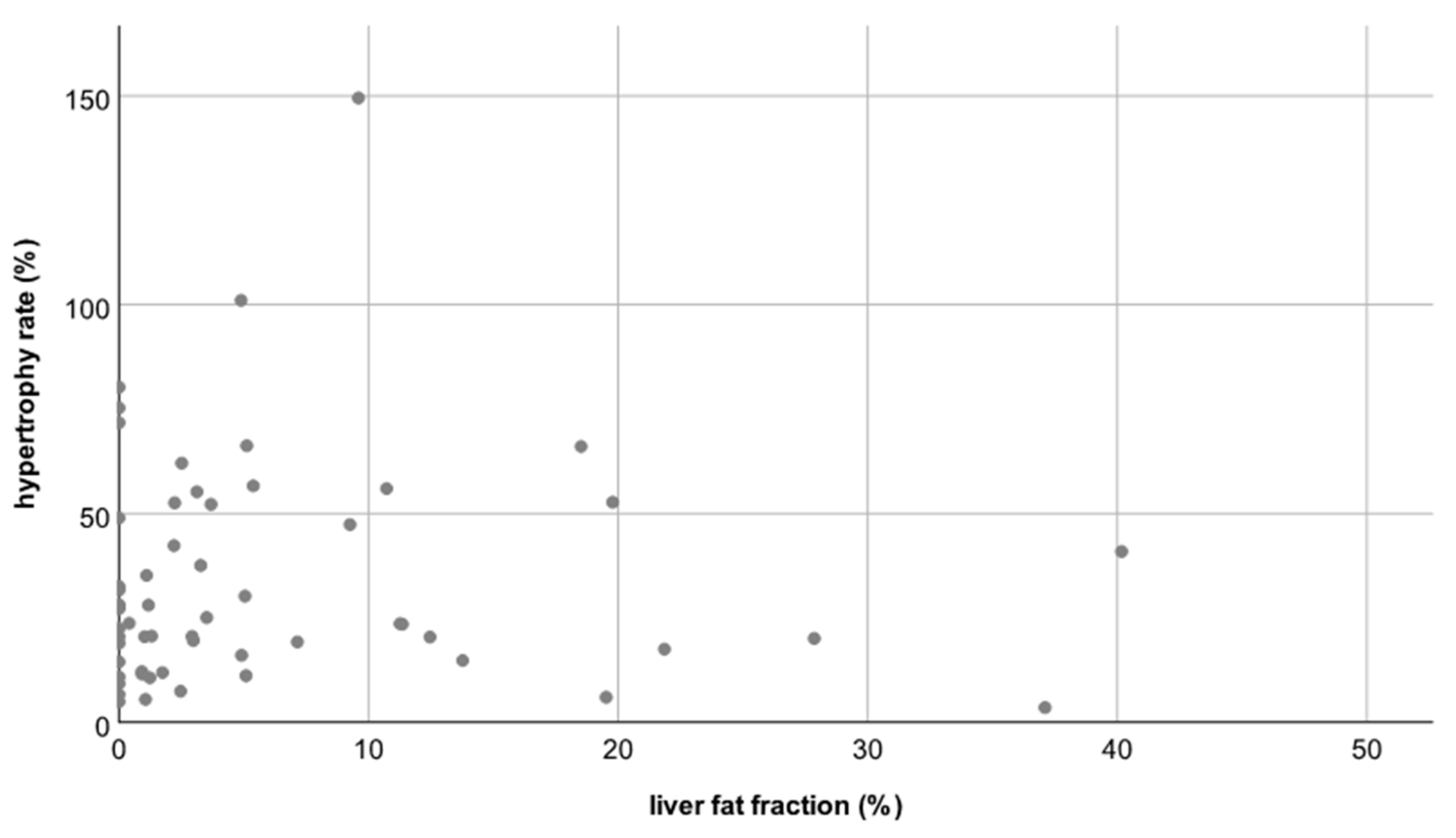
Hepatic Fat Fraction Versus Degree and Rate of Hypertrophy
3.4. History of Chemotherapy
3.5. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Engstrand, J.; Nilsson, H.; Strömberg, C.; Jonas, E.; Freedman, J. Colorectal cancer liver metastases–A population-based study on incidence, management and survival. BMC Cancer 2018, 18, 78. [Google Scholar] [CrossRef]
- Kopetz, S.; Chang, G.J.; Overman, M.J.; Eng, C.; Sargent, D.J.; Larson, D.W.; Grothey, A.; Vauthey, J.-N.; Nagorney, D.M.; McWilliams, R.R. Improved Survival in Metastatic Colorectal Cancer Is Associated With Adoption of Hepatic Resection and Improved Chemotherapy. J. Clin. Oncol. 2009, 27, 3677–3683. [Google Scholar] [CrossRef]
- Weiser, M.R.; Jarnagin, W.R.; Saltz, L.B. Colorectal cancer patients with oligometastatic liver disease: What is the optimal approach? Oncology 2013, 27, 1074–1078. [Google Scholar] [PubMed]
- Van Tuil, T.; Dhaif, A.A.; Te Riele, W.W.; van Ramshorst, B.; van Santvoort, H.C. Systematic Review and Meta-Analysis of Liver Resection for Colorectal Metastases in Elderly Patients. Dig Surg. 2019, 36, 111–123. [Google Scholar] [CrossRef]
- Barth, B.K.; Fischer, M.A.; Kambakamba, P.; Lesurtel, M.; Reiner, C.S. Liver-fat and liver-function indices derived from Gd-EOB-DTPA-enhanced liver MRI for prediction of future liver remnant growth after portal vein occlusion. Eur. J. Radiol. 2016, 85, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Capussotti, L.; Muratore, A.; Baracchi, F.; Lelong, B.; Ferrero, A.; Regge, D.; Delpero, J.R. Portal Vein Ligation as an Efficient Method of Increasing the Future Liver Remnant Volume in the Surgical Treatment of Colorectal Metastases. Arch. Surg. 2008, 143, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Tschuor, C.; Croome, K.; Sergeant, G.; Cano, V.; Schadde, E.; Ardiles, V.; Slankamenac, K.; Clariá, R.; de Santibaňes, E.; Hernandez-Alejandro, R.; et al. Salvage parenchymal liver transection for patients with insufficient volume increase after portal vein occlusion—An extension of the ALPPS approach. Eur. J. Surg. Oncol. 2013, 39, 1230–1235. [Google Scholar] [CrossRef] [PubMed]
- Van Lienden, K.P.; van den Esschert, J.W.; de Graaf, W.; Bipat, S.; Lameris, J.S.; van Gulik, T.M.; van Delden, O.M. Portal vein embolization before liver resection: A systematic review. Cardiovasc. Interv. Radiol. 2013, 36, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Morris-Stiff, G.; Tan, Y.-M.; Vauthey, J. Hepatic complications following preoperative chemotherapy with oxaliplatin or irinotecan for hepatic colorectal metastases. Eur. J. Surg. Oncol. 2008, 34, 609–614. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Pamecha, V.; Levene, A.; Grillo, F.; Woodward, N.; Dhillon, A.P.; Davidson, B.R. Effect of portal vein embolisation on the growth rate of colorectal liver metastases. Br. J. Cancer 2009, 100, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Pommier, R.; Ronot, M.; Cauchy, F.; Gaujoux, S.; Fuks, D.; Faivre, S.; Belghiti, J.; Vilgrain, V. Colorectal Liver Metastases Growth in the Embolized and Non-Embolized Liver After Portal Vein Embolization: Influence of Initial Response to Induction Chemotherapy. Ann. Surg. Oncol. 2014, 21, 3077–3083. [Google Scholar] [CrossRef]
- Simoneau, E.; Aljiffry, M.; Salman, A.; Abualhassan, N.; Cabrera, T.; Valenti, D.; El Baage, A.; Jamal, M.; Kavan, P.; Al-Abbad, S.; et al. Portal vein embolization stimulates tumour growth in patients with colorectal cancer liver metastases. HPB 2012, 14, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Reeder, S.B.; Sirlin, C.B. Quantification of Liver Fat with Magnetic Resonance Imaging. Magn. Reson. Imaging Clin. North Am. 2010, 18, 337–357. [Google Scholar] [CrossRef]
- Reeder, S.B.; Cruite, I.; Hamilton, G.; Sirlin, C.B. Quantitative Assessment of Liver Fat with Magnetic Resonance Imaging and Spectroscopy. J. Magn. Reson Imaging 2011, 34, 729–749. [Google Scholar] [CrossRef]
- Busuttil, R.W.; Tanaka, K. The utility of marginal donors in liver transplantation. Liver Transpl. 2003, 9, 651–663. [Google Scholar] [CrossRef]
- Shindoh, J.; Truty, M.J.; Aloia, T.A.; Curley, S.A.; Zimmitti, G.; Huang, S.Y.; Mahvash, A.; Gupta, S.; Wallace, M.J.; Vauthey, J.-N. Kinetic Growth Rate after Portal Vein Embolization Predicts Posthepatectomy Outcomes: Toward Zero Liver-Related Mortality in Patients with Colorectal Liver Metastases and Small Future Liver Remnant. J. Am. Coll. Surg. 2013, 216, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Schadde, E. Hypertrophy and Liver Function in ALPPS: Correlation with Morbidity and Mortality. Visc. Med. 2017, 33, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Schnitzbauer, A.A.; Lang, S.A.; Goessmann, H.; Nadalin, S.; Baumgart, J.; Farkas, S.A.; Fichtner-Feigl, S.; Lorf, T.; Goralcyk, A.; Hörbelt, R.; et al. Right Portal Vein Ligation Combined With In Situ Splitting Induces Rapid Left Lateral Liver Lobe Hypertrophy Enabling 2-Staged Extended Right Hepatic Resection in Small-for-Size Settings. Ann. Surg. 2012, 255, 405–414. [Google Scholar] [CrossRef]
- Isfordink, C.; Samim, M.; Braat, M.; Almalki, A.; Hagendoorn, J.; Rinkes, I.B.; Molenaar, I. Portal vein ligation versus portal vein embolization for induction of hypertrophy of the future liver remnant: A systematic review and meta-analysis. Surg. Oncol. 2017, 26, 257–267. [Google Scholar] [CrossRef]
- Geisel, D.; Raabe, P.; Lüdemann, L.; Malinowski, M.; Stockmann, M.; Seehofer, D.; Pratschke, J.; Hamm, B.; Denecke, T. Gd-EOB-DTPA-enhanced MRI for monitoring future liver remnant function after portal vein embolization and extended hemihepatectomy: A prospective trial. Eur. Radiol. 2016, 27, 3080–3087. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25 (Suppl. 3), iii1–iii9. [Google Scholar] [CrossRef] [PubMed]
- Brouquet, A.; Benoist, S.; Julie, C.; Penna, C.; Beauchet, A.; Rougier, P.; Nordlinger, B. Risk factors for chemotherapy-associated liver injuries: A multivariate analysis of a group of 146 patients with colorectal metastases. Surgery 2009, 145, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Choti, M.A. Chemotherapy-Associated Hepatotoxicity: Do We Need to Be Concerned? Ann. Surg. Oncol. 2009, 16, 2391–2394. [Google Scholar] [CrossRef] [PubMed]
- Schulze-Hagen, M.; Truhn, D.; Duong, F.; Keil, S.; Pedersoli, F.; Kuhl, C.K.; Lurje, G.; Neumann, U.; Isfort, P.; Bruners, P.; et al. Correlation Between Sarcopenia and Growth Rate of the Future Liver Remnant After Portal Vein Embolization in Patients with Colorectal Liver Metastases. Cardiovasc. Interv. Radiol. 2020, 43, 875–881. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Scanner | 1.5 T Achieva/Ingenia; Philipps Healthcare, Best, The Netherlands | ||
|---|---|---|---|
| Pulse sequence type | 2D T1w GRE (In- and opposed-phase) | 2D T2w TSE | |
| Orientation | axial | axial | |
| Acquisition matrix | 304 | 480 | |
| Field of view | 380 | 380 | |
| Section thickness | 6 mm | 5 mm | |
| TR | 176 | 2200 | |
| TE | IP: 2.3 | OP: 4.6 | 90 |
| Breath compensation | Breath hold | Respiratory triggering | |
| Type of Scanner | Somatom Flash, Siemens Medical System, Forchheim, Germany |
|---|---|
| Contrast agent | Non-ionic contrast agent (Ultravist 370, Bayer Schering Pharma AG, Berlin, Germany) |
| Dose of contrast agent | 1 mL/kg body weight |
| Orientation | axial |
| Acquisition time | Arterial phase: 15 s Portal vein phase: 70 s Late phase: 300 s |
| Section thickness | 5/1 mm 1/0.7 mm |
| Tube voltage | 120 kV |
| Pitch factor | 0.6 |
| Section collimation | 128 mm |
| Patient Demographics of All 57 Patients | |
|---|---|
| Age, y (mean, SD) | 60 ± 10 |
| Gender (M, F) | 45:23 |
| Liver Tumor (number) | |
| Colorectal liver metastases | 68 |
| Left-sided primary | 50 |
| Right-sided primary | 18 |
| Initial overall tumor mass before PVE, mL (mean, SD) | 80 ± 205 |
| Pre-interventional chemotherapy (number) | 53 |
| FOLFOX | 22 |
| FOLFIRINOX | 28 |
| Capecitabine monotherapy | 1 |
| Unknown | 2 |
| Degree of Hypertrophy | Correlation Coefficient |
|---|---|
| Age | R = −0.20 |
| Gender | R = 0.03 |
| Liver fat fraction | R = −0.04 |
| Chemotherapy treatment | R = 0.20 |
| Initial tumor mass | R = 0.02 |
| Laterality of primary CRC | R = −0.03 |
| Kinetic Growth Rate per Week | Correlation Coefficient |
|---|---|
| Age | R = −0.24 (p = 0.04) ** |
| Gender | R = −0.19 |
| Liver fat fraction | R = −0.15 |
| Chemotherapy treatment | R = −0.07 |
| Initial tumor mass | R = −0.08 |
| Laterality of primary CRC | R = −0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hitpass, L.; Amygdalos, I.; Sieben, P.; Raaff, V.; Lang, S.; Bruners, P.; Kuhl, C.K.; Barabasch, A. MRI-Based Quantitation of Hepatic Steatosis Does Not Predict Hypertrophy Rate after Portal Vein Embolization in Patients with Colorectal Liver Metastasis and Normal to Moderately Elevated Fat Fraction. J. Clin. Med. 2021, 10, 2003. https://doi.org/10.3390/jcm10092003
Hitpass L, Amygdalos I, Sieben P, Raaff V, Lang S, Bruners P, Kuhl CK, Barabasch A. MRI-Based Quantitation of Hepatic Steatosis Does Not Predict Hypertrophy Rate after Portal Vein Embolization in Patients with Colorectal Liver Metastasis and Normal to Moderately Elevated Fat Fraction. Journal of Clinical Medicine. 2021; 10(9):2003. https://doi.org/10.3390/jcm10092003
Chicago/Turabian StyleHitpass, Lea, Iakovos Amygdalos, Paul Sieben, Vanessa Raaff, Sven Lang, Philipp Bruners, Christiane K. Kuhl, and Alexandra Barabasch. 2021. "MRI-Based Quantitation of Hepatic Steatosis Does Not Predict Hypertrophy Rate after Portal Vein Embolization in Patients with Colorectal Liver Metastasis and Normal to Moderately Elevated Fat Fraction" Journal of Clinical Medicine 10, no. 9: 2003. https://doi.org/10.3390/jcm10092003
APA StyleHitpass, L., Amygdalos, I., Sieben, P., Raaff, V., Lang, S., Bruners, P., Kuhl, C. K., & Barabasch, A. (2021). MRI-Based Quantitation of Hepatic Steatosis Does Not Predict Hypertrophy Rate after Portal Vein Embolization in Patients with Colorectal Liver Metastasis and Normal to Moderately Elevated Fat Fraction. Journal of Clinical Medicine, 10(9), 2003. https://doi.org/10.3390/jcm10092003