Corneal Culture in Infectious Keratitis: Effect of the Inoculation Method and Media on the Corneal Culture Outcome

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
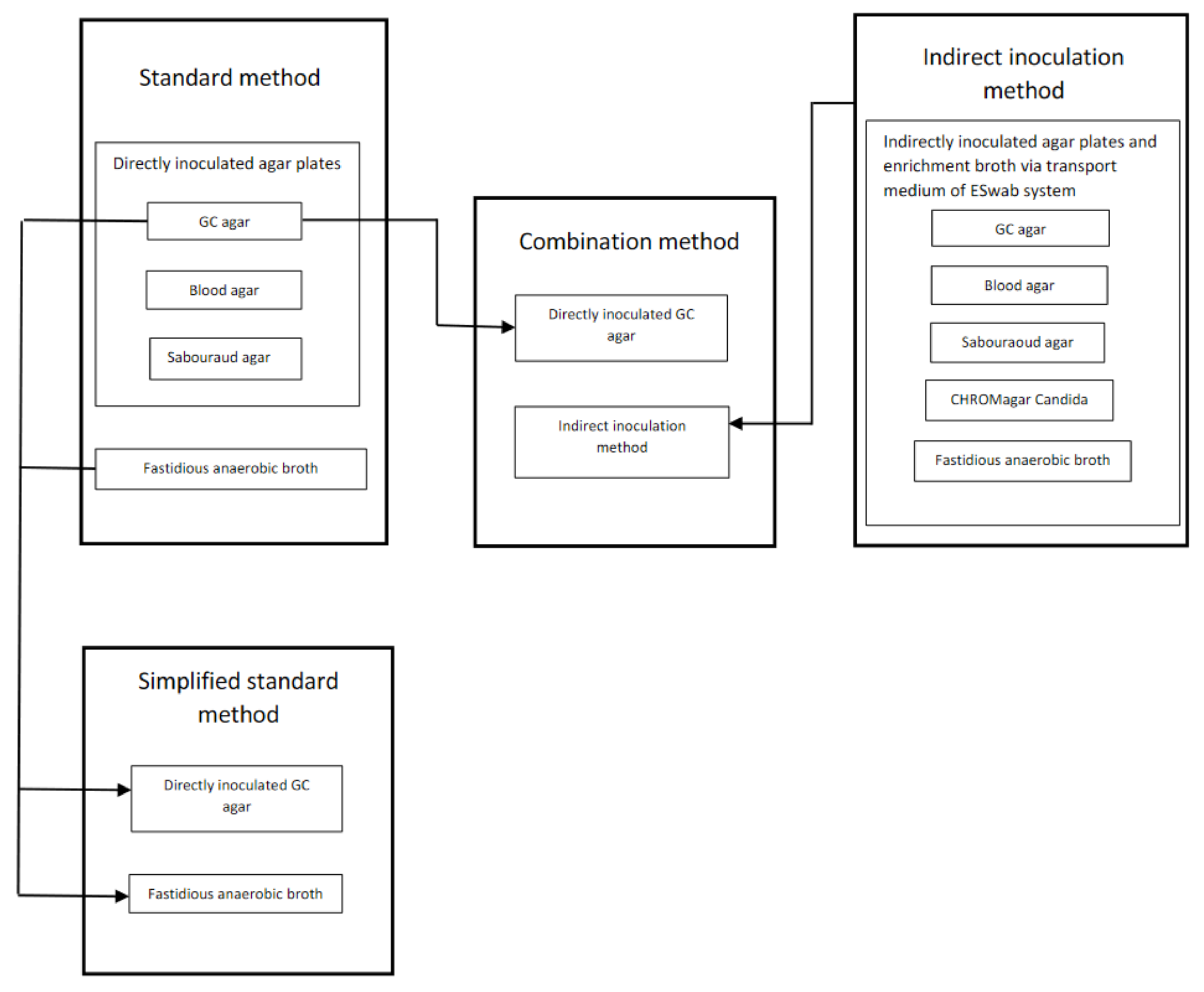
2.2. Corneal Sampling
2.3. Statistical Analysis
3. Results
3.1. Study Cohort
3.2. Comparison between a Multiple Sampling Method on Solid Media and Liquid Enrichment Media (Standard Method) and a Single Sampling Method Dispensed in Transport Media for Indirect Inoculation (Indirect Inoculation Method)
3.3. Evaluation of a Simplified Standard Method and a Combination Method of Corneal Culture
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Incubation Conditions for Culture Media, the Handling of the Sample in Transport Media and Contents of the Agar Plates
References
- Shah, A.; Sachdev, A.; Coggon, D.; Hossain, P. Geographic variations in microbial keratitis: An analysis of the peer-reviewed literature. Br. J. Ophthalmol. 2011, 95, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Camarena, J.C.; Graue-Hernandez, E.O.; Ortiz-Casas, M.; Ramirez-Miranda, A.; Navas, A.; Pedro-Aguilar, L.; Lopez-Espinosa, N.L.; Gaona-Juarez, C.; Bautista-Hernandez, L.A.; Bautista-de Lucio, V.M. Trends in Microbiological and Antibiotic Sensitivity Patterns in Infectious Keratitis: 10-Year Experience in Mexico City. Cornea 2015, 34, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Lichtinger, A.; Yeung, S.N.; Kim, P.; Amiran, M.D.; Iovieno, A.; Elbaz, U.; Ku, J.Y.; Wolff, R.; Rootman, D.S.; Slomovic, A.R. Shifting trends in bacterial keratitis in Toronto: An 11-year review. Ophthalmology 2012, 119, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Wilhelmus, K.R.; Schlech, B.A. Clinical and epidemiological advantages of culturing bacterial keratitis. Cornea 2004, 23, 38–42. [Google Scholar] [CrossRef]
- Jones, D.B.; Liesegang, T.J.; Robinson, N.M.; Washington, J.A. Laboratory Diagnosis of Ocular Infections; Washington, J.A., II, Ed.; American Society for Microbiology: Washington, DC, USA, 1981. [Google Scholar]
- McLeod, S.D.; DeBacker, C.M.; Viana, M.A. Differential care of corneal ulcers in the community based on apparent severity. Ophthalmology 1996, 103, 479–484. [Google Scholar] [CrossRef]
- McDonnell, P.J.; Nobe, J.; Gauderman, W.J.; Lee, P.; Aiello, A.; Trousdale, M. Community care of corneal ulcers. Am. J. Ophthalmol. 1992, 114, 531–538. [Google Scholar] [CrossRef]
- Tam, A.L.C.; Côté, E.; Saldanha, M.; Lichtinger, A.; Slomovic, A.R. Bacterial Keratitis in Toronto: A 16-Year Review of the Microorganisms Isolated and the Resistance Patterns Observed. Cornea 2017, 36, 1528–1534. [Google Scholar] [CrossRef]
- Whitcher, J.P.; Srinivasan, M.; Upadhyay, M.P. Corneal blindness: A global perspective. Bull. World Health Organ. 2001, 79, 214–221. [Google Scholar]
- Ung, L.; Bispo, P.J.M.; Shanbhag, S.S.; Gilmore, M.S.; Chodosh, J. The persistent dilemma of microbial keratitis: Global burden, diagnosis, and antimicrobial resistance. Surv. Ophthalmol. 2019, 64, 255–271. [Google Scholar] [CrossRef]
- Badenoch, P.R.; Coster, D.J. Antimicrobial activity of topical anaesthetic preparations. Br. J. Ophthalmol. 1982, 66, 364–367. [Google Scholar] [CrossRef]
- Mullin, G.S.; Rubinfeld, R.S. The antibacterial activity of topical anesthetics. Cornea 1997, 16, 662–665. [Google Scholar] [CrossRef]
- Pelosini, L.; Treffene, S.; Hollick, E.J. Antibacterial activity of preservative-free topical anesthetic drops in current use in ophthalmology departments. Cornea 2009, 28, 58–61. [Google Scholar] [CrossRef]
- Das, S.; Sharma, S.; Kar, S.; Sahu, S.K.; Samal, B.; Mallick, A. Is inclusion of Sabouraud dextrose agar essential for the laboratory diagnosis of fungal keratitis? Indian J. Ophthalmol. 2010, 58, 281–286. [Google Scholar] [CrossRef]
- Waxman, E.; Chechelnitsky, M.; Mannis, M.J.; Schwab, I.R. Single culture media in infectious keratitis. Cornea 1999, 18, 257–261. [Google Scholar] [CrossRef]
- Benson, W.H.; Lanier, J.D. Comparison of techniques for culturing corneal ulcers. Ophthalmology 1992, 99, 800–804. [Google Scholar] [CrossRef]
- Jacob, P.; Gopinathan, U.; Sharma, S.; Rao, G.N. Calcium alginate swab versus Bard Parker blade in the diagnosis of microbial keratitis. Cornea 1995, 14, 360–364. [Google Scholar] [CrossRef]
- Kaye, S.; Sueke, H.; Romano, V.; Chen, J.Y.; Carnt, N.; Tuft, S.; Neal, T. Impression membrane for the diagnosis of microbial keratitis. Br. J. Ophthalmol. 2016, 100, 607–610. [Google Scholar] [CrossRef]
- Sagerfors, S.; Ejdervik-Lindblad, B.; Söderquist, B. Does the sampling instrument influence corneal culture outcome in patients with infectious keratitis? A retrospective study comparing cotton tipped applicator with knife blade. BMJ Open Ophthalmol. 2020, 5, e000363. [Google Scholar] [CrossRef]
- Kaye, S.B.; Rao, P.G.; Smith, G.; Scott, J.A.; Hoyles, S.; Morton, C.E.; Willoughby, C.; Batterbury, M.; Harvey, G. Simplifying collection of corneal specimens in cases of suspected bacterial keratitis. J. Clin. Microbiol. 2003, 41, 3192–3197. [Google Scholar] [CrossRef]
- McLeod, S.D.; Kumar, A.; Cevallos, V.; Srinivasan, M.; Whitcher, J.P. Reliability of transport medium in the laboratory evaluation of corneal ulcers. Am. J. Ophthalmol. 2005, 140, 1027–1031. [Google Scholar] [CrossRef]
- Stapleton, F.; Keay, L.; Edwards, K.; Naduvilath, T.; Dart, J.K.; Brian, G.; Holden, B.A. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology 2008, 115, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Pakzad-Vaezi, K.; Levasseur, S.D.; Schendel, S.; Mark, S.; Mathias, R.; Roscoe, D.; Holland, S.P. The corneal ulcer one-touch study: A simplified microbiological specimen collection method. Am. J. Ophthalmol. 2015, 159, 37–43.e1. [Google Scholar] [CrossRef] [PubMed]
- Fleiszig, S.M.; Efron, N. Microbial flora in eyes of current and former contact lens wearers. J. Clin. Microbiol. 1992, 30, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Lowry, R. VassarStats: Statistical Calculation Web Site. Available online: http://vassarstats.net/ (accessed on 31 August 2020).
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; Chapman and Hall: London, UK, 1991. [Google Scholar]
- Nielsen, S.E.; Gertsen, J.B.; Kjaersgaard, M.; Ivarsen, A.; Hjortdal, J. New diagnostic tool in bacterial keratitis is not superior to traditional agar plates. Acta Ophthalmol. 2016, 94, e671–e672. [Google Scholar] [CrossRef]
- Bourcier, T.; Thomas, F.; Borderie, V.; Chaumeil, C.; Laroche, L. Bacterial keratitis: Predisposing factors, clinical and microbiological review of 300 cases. Br. J. Ophthalmol. 2003, 87, 834–838. [Google Scholar] [CrossRef]
- Tan, S.Z.; Walkden, A.; Au, L.; Fullwood, C.; Hamilton, A.; Qamruddin, A.; Armstrong, M.; Brahma, A.K.; Carley, F. Twelve-year analysis of microbial keratitis trends at a UK tertiary hospital. Eye 2017, 31, 1229–1236. [Google Scholar] [CrossRef]
- Armstrong, M. The laboratory investigation of infective keratitis. Br. J. Biomed. Sci. 1994, 51, 65–72. [Google Scholar]
- Schonheyder, H.C.; Pedersen, J.K.; Naeser, K. Experience with a broth culture technique for diagnosis of bacterial keratitis. Acta Ophthalmol. Scand. 1997, 75, 592–594. [Google Scholar] [CrossRef]


{kind=link}
| Age in years, median (range) | 44.0 (18–84) | |
| Male sex, n (%) | 53 (56.4%) | |
| Right eye, n (%) | 49 (52%) | |
| Days with symptoms prior to culture a, median (range) | 3.0 (0.5–61) | |
| Largest diameter b (mm), median (range) | 1.0 (0.1–8.0) | |
| Lesion area b (mm2), median (range) | 0.8 (0.01–50.2) | |
| Topical antibiotic prior to corneal culture, n (%) | 15 (16%) | |
| Risk factors for keratitis | Contact lens wear, n (%) | 67 (71.3%) |
| Ocular surface disease, n (%) | 13 (13.8%) | |
| No identified risk factor, n (%) | 7 (7.4%) | |
| Prior ocular surgery, n (%) | 4 (4.3%) | |
| Trauma, n (%) | 3 (3.2%) | |
| BCVA c at time of corneal culture, median (range) | 0.9 (0.001–1.0) |
| Agreement, Cohen’s Kappa (95% CI) | Method Difference | p-Value f | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| H | Number of microorganisms isolated by standard method and indirect inoculation method | Number of microorganisms isolated by standard method only | Number of microorganisms isolated by indirect inoculation method only | Number of culture negative readings by both standard method and indirect inoculation method | Agreement between standard method and indirect inoculation method | Positive agreement between standard method and indirect inoculation method | Negative agreement between standard method and indirect inoculation method | Proportion of culture positive readings using standard method | Proportion of culture positive readings using indirect inoculation method | ||
| Total | 30 | 59 | 28 | 1669 | 0.38 (0.28–0.49) | 0.41 (0.30–0.52) | 0.97 (0.97–0.98) | 0.0498 | 0.0325 | 0.001169 | |
| Comparison of detected microorganisms according to lesion size a | Large (largest diameter ≥1.0 mm) b | 16 | 43 | 20 | 1595 | 0.32 (0.19–0.44) | 0.33 (0.22–0.47) | 0.98 (0.97–0.99) | 0.0352 | 0.0215 | 0.005152 |
| Small (largest diameter ≤0.9 mm) c | 12 | 15 | 8 | 709 | 0.50 (0.32–0.67) | 0.5 (0.31–0.69) | 0.98 (0.97–0.99) | 0.0363 | 0.0269 | 0.21004 | |
| Comparison of detected microorganisms according to presumed pathogenicity | Potentially pathogenic d | 7 | 11 | 4 | 1200 | 0.48 (0.25–0.70) | 0.47 (0.25–0.70) | 0.99 (0.99–1.0) | 0.0147 | 0.009 | 0.118469 |
| Commensals e | 23 | 48 | 24 | 469 | 0.32 (0.20–0.44) | 0.39 (0.28–0.52) | 0.93 (0.90–0.95) | 0.1259 | 0.0833 | 0.00631 | |
| Agreement, Cohen’s Kappa (95% CI) | Method Difference | p-Value c | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of microorganisms isolated by both methods: standard method and either simplified standard method or combination method | Number of microorganisms isolated by standard method only | Number of microorganisms isolated by either simplified standard method only or combination method only | Number of culture negative readings from both methods: standard method and either simplified standard method or combination method | Agreement between standard method and either simplified standard method or combination method | Positive agreement between standard method and either simplified standard method or combination method | Negative agreement between standard method and either simplified standard method or combination method | Proportion of microorganisms detected by standard method | Proportion of microorganisms detected by either simplified standard method or combination method | ||
| Simplified standard method a | ||||||||||
| Total | 77 | 12 | 0 | 1415 | 0.92 (0.88–0.97) | 0.93 (0.85–0.97) | 1.0 (0.99–1.0) | 0.0592 | 0.0512 | 0.00049 |
| Potentially pathogenic d | 17 | 1 | 0 | 1016 | 0.97 (0.91–1) | 0.94 (0.74–0.99) | 1.0 (0.99–1.0) | 0.0174 | 0.0164 | 1.00 |
| Commensals e | 60 | 11 | 0 | 399 | 0.90 (0.85–0.96) | 0.91 (0.82–0.96) | 0.99 (0.97–0.99) | 0.1511 | 0.1277 | 0.00977 |
| Combination method b | ||||||||||
| Total | 56 | 33 | 28 | 1669 | 0.63 (0.54–0.72) | 0.64 (0.54–0.74) | 0.98 (0.97–0.99) | 0.0498 | 0.047 | 0.60892 |
| Potentially pathogenic d | 13 | 5 | 4 | 1200 | 0.74 (0.57–0.90) | 0.72 (0.49–0.88) | 1.0 (0.99–1.0) | 0.0147 | 0.0139 | 1.00 |
| Commensals e | 42 | 28 | 24 | 469 | 0.57 (0.47–0.68) | 0.62 (0.51–0.73) | 0.95 (0.92–0.96) | 0.1259 | 0.1188 | 0.67781 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sagerfors, S.; Karakoida, C.; Sundqvist, M.; Ejdervik Lindblad, B.; Söderquist, B. Corneal Culture in Infectious Keratitis: Effect of the Inoculation Method and Media on the Corneal Culture Outcome. J. Clin. Med. 2021, 10, 1810. https://doi.org/10.3390/jcm10091810
Sagerfors S, Karakoida C, Sundqvist M, Ejdervik Lindblad B, Söderquist B. Corneal Culture in Infectious Keratitis: Effect of the Inoculation Method and Media on the Corneal Culture Outcome. Journal of Clinical Medicine. 2021; 10(9):1810. https://doi.org/10.3390/jcm10091810
Chicago/Turabian StyleSagerfors, Susanna, Chrysoula Karakoida, Martin Sundqvist, Birgitta Ejdervik Lindblad, and Bo Söderquist. 2021. "Corneal Culture in Infectious Keratitis: Effect of the Inoculation Method and Media on the Corneal Culture Outcome" Journal of Clinical Medicine 10, no. 9: 1810. https://doi.org/10.3390/jcm10091810
APA StyleSagerfors, S., Karakoida, C., Sundqvist, M., Ejdervik Lindblad, B., & Söderquist, B. (2021). Corneal Culture in Infectious Keratitis: Effect of the Inoculation Method and Media on the Corneal Culture Outcome. Journal of Clinical Medicine, 10(9), 1810. https://doi.org/10.3390/jcm10091810