
Effect of Wearing Personal Protective Equipment (PPE) on CPR Quality in Times of the COVID-19 Pandemic—A Simulation, Randomised Crossover Trial

 , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Protocol
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 16 February 2021).
- Sultanian, P.; Lundgren, P.; Strömsöe, A.; Aune, S.; Bergström, G.; Hagberg, E.; Hollenberg, J.; Lindqvist, J.; Djärv, T.; Castelheim, A.; et al. Cardiac arrest in COVID-19: Characteristics and outcomes of in- and out-of-hospital cardiac arrest. A report from the Swedish registry for cardiopulmonary resuscitation. Eur. Heart J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Transmission of SARS-CoV-2: Implications for Infection Prevention Precautions. Available online: https://www.who.int/publications/i/item/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations (accessed on 15 December 2020).
- Couper, K.; Taylor-Phillips, S.; Grove, A.; Freeman, K.; Osokogu, O.; Court, R.; Mehrabian, A.; Morley, P.T.; Nolan, J.P.; Soar, J.; et al. COVID-19 in cardiac arrest and infection risk to rescuers: A systematic review. Resuscitation 2020, 151, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Monsieurs, K.G.; Bossaert, L.; Böttiger, B.W.; Greif, R.; Lott, C.; Madar, J.; Olasveengen, T.M.; Roehr, C.C.; Semeraro, F.; et al. European resuscitation council COVID-19 guidelines executive summary. Resuscitation 2020, 153, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Ashton, A.; McCluskey, A.; Gwinnutt, C.L.; Keenan, A.M. Effect of rescuer fatigue on performance of continuous external chest compressions over 3 min. Resuscitation 2002, 55, 151–155. [Google Scholar] [CrossRef]
- Hopkins, S.R.; Dominelli, P.B.; Davis, C.K.; Guenette, J.A.; Luks, A.M.; Molgat-Seon, Y.; Sá, R.C.; Sheel, A.W.; Swenson, E.R.; Stickland, M.K. Face masks and the cardiorespiratory response to physical activity in health and disease. Ann. Am. Thorac. Soc. 2020. [Google Scholar] [CrossRef]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castren, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Grasner, J.T.; Wenzel, V.; et al. European resuscitation council guidelines for resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [PubMed]
- Beom, J.H.; Kim, M.J.; You, J.S.; Lee, H.S.; Kim, J.H.; Park, Y.S.; Shin, D.M.; Chung, H.S. Evaluation of the quality of cardiopulmonary resuscitation according to vehicle driving pattern, using a virtual reality ambulance driving system: A prospective, cross-over, randomised study. BMJ Open 2018, 8, e023784. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.P.; de Wang, Y. Objective assessment of increase in breathing resistance of N95 respirators on human subjects. Ann. Occup. Hyg. 2011, 55, 917–921. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Davis, B.A.; Tsen, L.C. Wearing an N95 respiratory mask: An unintended exercise benefit? Anesthesiology 2020, 133, 684–686. [Google Scholar] [CrossRef] [PubMed]
- Epstein, D.; Korytny, A.; Isenberg, Y.; Marcusohn, E.; Zukermann, R.; Bishop, B.; Minha, S.A.; Raz, A.; Miller, A. Return to training in the COVID-19 era: The physiological effects of face masks during exercise. Scand. J. Med. Sci. Sports 2021, 31, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Rebmann, T.; Carrico, R.; Wang, J. Physiologic and other effects and compliance with long-term respirator use among medical intensive care unit nurses. Am. J. Infect. Control 2013, 41, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Hightower, D.; Thomas, S.H.; Stone, C.K.; Dunn, K.; March, J.A. Decay in quality of closed-chest compressions over time. Ann. Emerg. Med. 1995, 26, 300–303. [Google Scholar] [CrossRef]
- Ochoa, F.J.; Ramalle-Gómara, E.; Lisa, V.; Saralegui, I. The effect of rescuer fatigue on the quality of chest compressions. Resuscitation 1998, 37, 149–152. [Google Scholar] [CrossRef]
- Sahu, A.K.; Suresh, S.; Mathew, R.; Aggarwal, P.; Nayer, J. Impact of personal protective equipment on the effectiveness of chest compression—A systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 39, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lu, K.-Z.; Yi, B.; Chen, Y. Chest compression with personal protective equipment during cardiopulmonary resuscitation: A randomized crossover simulation study. Medicine 2016, 95, e3262. [Google Scholar] [CrossRef] [PubMed]
- Malysz, M.; Dabrowski, M.; Böttiger, B.W.; Smereka, J.; Kulak, K.; Szarpak, A.; Jaguszewski, M.; Filipiak, K.J.; Ladny, J.R.; Ruetzler, K.; et al. Resuscitation of the patient with suspected/confirmed COVID-19 when wearing personal protective equipment: A randomized multicenter crossover simulation trial. Cardiol. J. 2020, 27, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Kienbacher, C.L.; Grafeneder, J.; Tscherny, K.; Krammel, M.; Fuhrmann, V.; Niederer, M.; Neudorfsky, S.; Herbich, K.; Schreiber, W.; Herkner, H.; et al. The use of personal protection equipment does not impair the quality of cardiopulmonary resuscitation: A prospective triple-cross over randomised controlled non-inferiority trial. Resuscitation 2021, 160, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.Y.; Wong, P.; Teo, L.M.; Ho, V.K. Resuscitation during the COVID-19 pandemic: Lessons learnt from high-fidelity simulation. Resuscitation 2020, 152, 89–90. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Mean ± SD or n (%) |
|---|---|
| Age, years | 40 ± 1.6 |
| Female participants | 13 (38%) |
| Height, m | 1.75 ± 0.09 |
| Body weight, kg | 77 ± 14 |
| BMI | 24.3 ± 5.6 |
| EMS experience, years | 12.0 ± 10.7 |
| Parameter | Without PPE | With PPE |
|---|---|---|
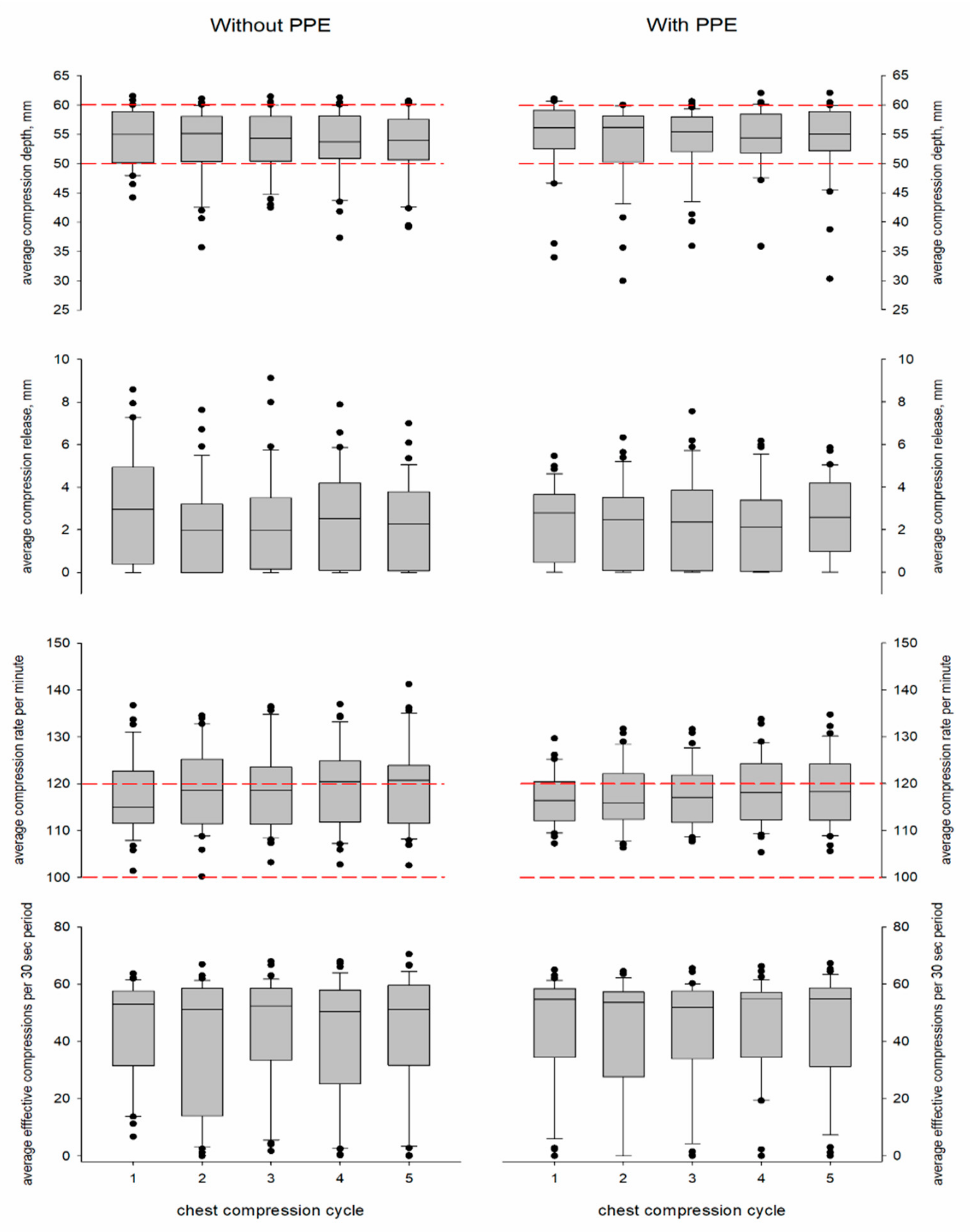
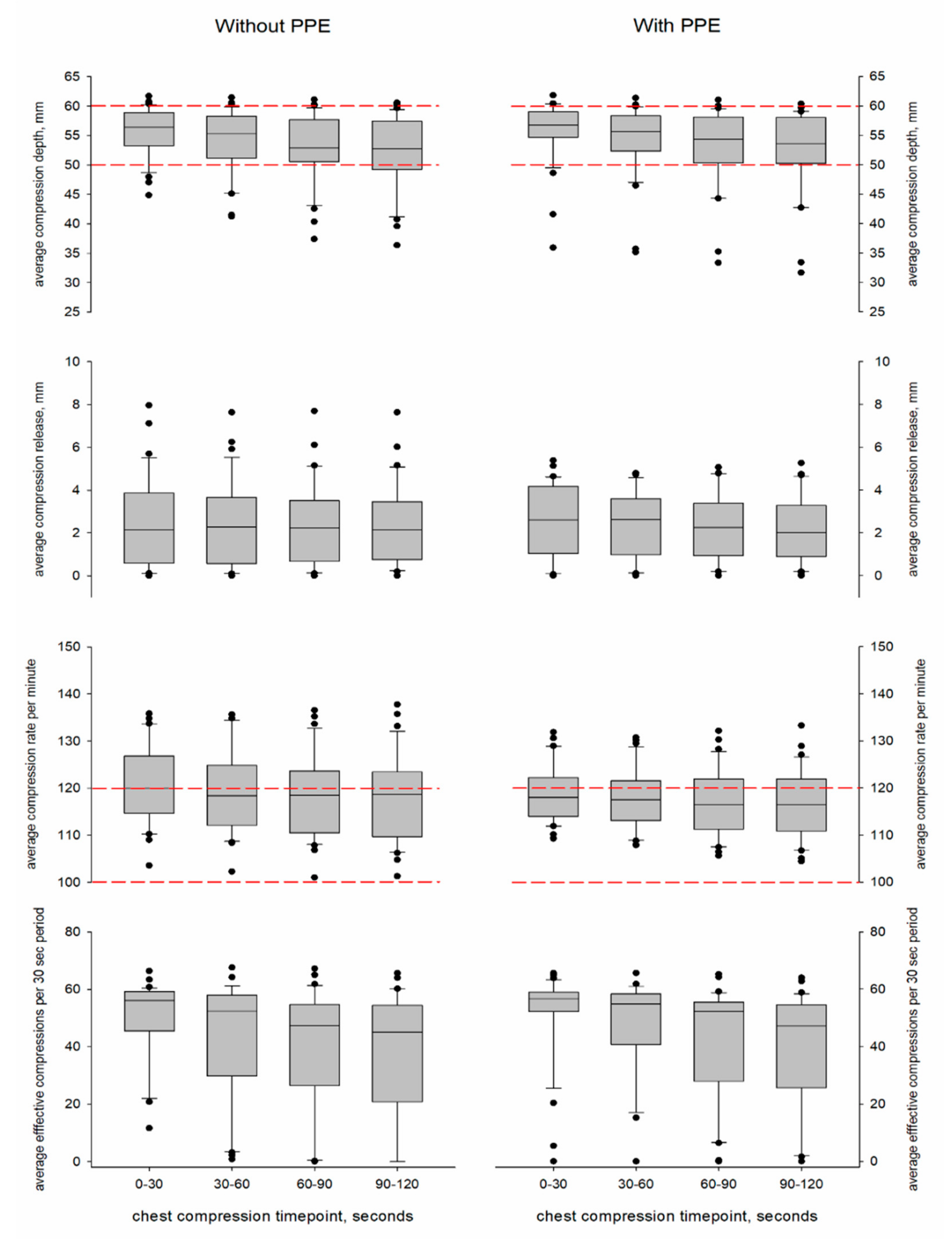
| Compression depth, mm | 54 ± 5 | 54 ± 6 |
| Release, mm | 2 ± 2 | 2 ± 2 |
| Rate per minute | 119 ± 9 | 118 ± 6 |
| Effective chest compressions, number | 43 ± 18 | 45 ± 17 |
| Compression Parameter | Intercept | PPE | Cycle Number | Timepoint | PPE Sequence Order | Weight | Gender | Timepoint * PPE | Timepoint * Gender | Timepoint * Weight | Cycle Number * PPE | Cycle Number * Gender | Cycle Number * Weight | PPE * Gender |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Depth | <0.001 | 1.000 | 0.002 | <0.001 | 1.000 | 0.604 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 0.054 | 1.000 | 1.000 |
| Release | <0.001 | 1.000 | 0.462 | 0.054 | 1.000 | 1.000 | 1.000 | 0.826 | 1.000 | 0.695 | 0.989 | † | † | 1.000 |
| Rate | <0.001 | 0.229 | <0.001 | <0.001 | 0.197 | 0.101 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 0.769 | 0.597 | 1.000 |
| Effective CCs | <0.001 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 0.541 | 1.000 | 1.000 | 0.540 | 1.000 |
| Subjective Parameter | PPE | Compression Parameter * | Correlation | p-Value |
|---|---|---|---|---|
| Fatigue | No | Depth | −0.121 | 1.000 |
| Release | −0.003 | 1.000 | ||
| Rate | 0.213 | 1.000 | ||
| Effective CCs | −0.007 | 1.000 | ||
| Yes | Depth | −0.040 | 1.000 | |
| Release | −0.041 | 1.000 | ||
| Rate | −0.016 | 1.000 | ||
| Effective CCs | −0.049 | 1.000 | ||
| Performance | No | Depth | 0.222 | 1.000 |
| Release | −0.274 | 0.977 | ||
| Rate | 0.078 | 1.000 | ||
| Effective CCs | 0.200 | 1.000 | ||
| Yes | Depth | 0.080 | 1.000 | |
| Release | 0.103 | 1.000 | ||
| Rate | 0.463 | 0.061 | ||
| Effective CCs | 0.065 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rauch, S.; van Veelen, M.J.; Oberhammer, R.; Dal Cappello, T.; Roveri, G.; Gruber, E.; Strapazzon, G. Effect of Wearing Personal Protective Equipment (PPE) on CPR Quality in Times of the COVID-19 Pandemic—A Simulation, Randomised Crossover Trial. J. Clin. Med. 2021, 10, 1728. https://doi.org/10.3390/jcm10081728
Rauch S, van Veelen MJ, Oberhammer R, Dal Cappello T, Roveri G, Gruber E, Strapazzon G. Effect of Wearing Personal Protective Equipment (PPE) on CPR Quality in Times of the COVID-19 Pandemic—A Simulation, Randomised Crossover Trial. Journal of Clinical Medicine. 2021; 10(8):1728. https://doi.org/10.3390/jcm10081728
Chicago/Turabian StyleRauch, Simon, Michiel Jan van Veelen, Rosmarie Oberhammer, Tomas Dal Cappello, Giulia Roveri, Elisabeth Gruber, and Giacomo Strapazzon. 2021. "Effect of Wearing Personal Protective Equipment (PPE) on CPR Quality in Times of the COVID-19 Pandemic—A Simulation, Randomised Crossover Trial" Journal of Clinical Medicine 10, no. 8: 1728. https://doi.org/10.3390/jcm10081728
APA StyleRauch, S., van Veelen, M. J., Oberhammer, R., Dal Cappello, T., Roveri, G., Gruber, E., & Strapazzon, G. (2021). Effect of Wearing Personal Protective Equipment (PPE) on CPR Quality in Times of the COVID-19 Pandemic—A Simulation, Randomised Crossover Trial. Journal of Clinical Medicine, 10(8), 1728. https://doi.org/10.3390/jcm10081728