
Urinary Peptides as Potential Non-Invasive Biomarkers for Lupus Nephritis: Results of the Peptidu-LUP Study

 , , , , and
, , , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics
2.2. Kidney Biopsy Pathological Analysis
2.3. Sample Preparation
2.4. CE-MS Analysis and Data Processing
2.5. Biomarker Selection and Modelling
3. Results
3.1. Patients’ Characteristics
3.2. Absence of Urinary Peptides Predicting Proliferative LN
3.3. The Urinary Peptidome Does Not Predict Glomerulosclerosis
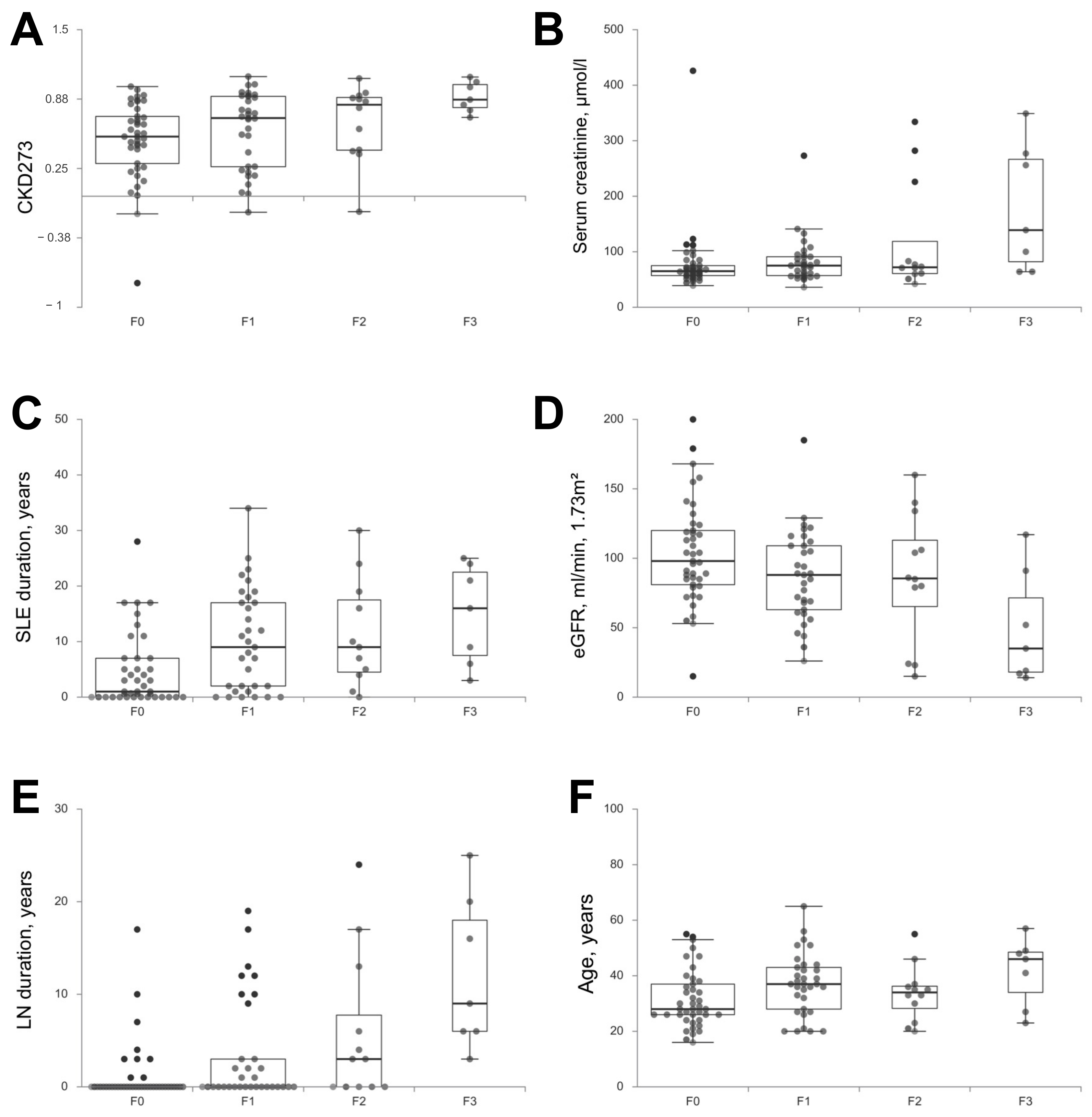
3.4. CKD273 Is Correlated to Tubulo-Interstitial Chronicity
3.5. LN 172 Is a Sensible Predictor for LN
3.6. The Urinary Peptidome Does Not Predict Early Remission
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Discovery Cohort | Validation Cohort | p | |
|---|---|---|---|
| Patients, n | 42 | 51 | |
| Women—n (%) | 40 (95.2) | 46 (90.2) | 0.45 |
| Mean age ± SD | 34 ± 7.7 | 36 ± 10 | 0.37 |
| Ethnicity—n (%) | 0.66 | ||
| European | 16 (38.1) | 24 (47.1) | 0.38 |
| North African | 10 (23.8) | 13 (25.5) | 1 |
| African | 11 (26.2) | 11 (21.6) | 0.78 |
| Asian | 5 (11.9) | 3 (5.9) | 0.46 |
| Characteristics at kidney biopsy | |||
| Serum creatinine—μmol/L, mean ± SD | 99.4 ± 55 | 86.8 ± 32 | 0.82 |
| eGFR—mL/min/1.73 m2, mean ± SD | 90.4 ± 32 | 92.3 ± 28.6 | 0.81 |
| UPCR—g/g, mean ± SD | 2.12 ± 1.25 | 2.53 ± 1.7 | 0.74 |
| SLE vintage | |||
| First flare of SLE—n (%) | 10 (23.8) | 11 (21.6) | 0.99 |
| Pre-existing SLE—n% | 32 (76.2) | 40 (78.4) | 0.99 |
| Disease duration—years, mean ± SD | 9.8 ± 7 | 11.33 ± 9.6 | 0.78 |
| First renal flare—n (%) | 22 (52.4) | 33 (64.7) | 0.32 |
| LN duration—years, mean ± SD | 6.6 ± 5 | 10.5 ± 8.2 | 0.22 |
| Kidney biopsies, n | |||
| Class, n (%) | 0.15 | ||
| I | 0 (0) | 1 (2.0) | 1 |
| II | 4 (9.5) | 2 (3.9) | 0.40 |
| III-A or -A/C ± V | 12 (28.6) | 10 (19.6) | 0.59 |
| III-C ± V | 2 (4.8) | 3 (5.9) | 1 |
| IV-A or -A/C ±V | 10 (23.8) | 23 (45.1) | 0.06 |
| IV-C ± V | 1 (2.4) | 1 (2.0) | 0.45 |
| Pure V | 12 (28.6) | 9 (17.6) | 0.32 |
| VI | 1 (2.4) | 2 (3.9) | 1 |
| IF/TA, n—(%) | 0.70 | ||
| F0 | 20 (44.6) | 21 (41.2) | 0.68 |
| F1 | 14 (33.3) | 19 (37.3) | 0.86 |
| F2 | 4 (9.5) | 8 (15.7) | 0.54 |
| F3 | 4 (9.5) | 3 (5.9) | 0.7 |
| Group | |||
| Active LN | 22(52.4) | 33 (64.7) | 0.36 |
| Non-active LN | 20 (47.6) | 18 (35.3) | 0.36 |
| Patients/center—n (%) | |||
| Marseille | 7 (16.7) | 30 (58.8) | <0.001 |
| Paris | 35 (83.3) | 18 (35.3) | <0.001 |
| Toulouse | 0 (0) | 3 (5.9) | 0.25 |
| Previous treatment for SLE—% | |||
| Hydroxychloroquine | 78.6 | 82.4 | 0.84 |
| Corticosteroids | 80.1 | 74.5 | 0.62 |
| MMF/Mycophenolic acid | 30.9 | 21.6 | 0.31 |
| Azathioprine | 16.7 | 21.6 | 0.74 |
| Cyclophosphamide | 35.7 | 31.4 | 0.82 |
| Rituximab | 4.8 | 11.8 | 0.29 |
| Other | 14.3 | 13.7 | 1 |
| Treatment for SLE at inclusion—% | |||
| Hydroxychloroquine | 66.7 | 70.6 | 0.86 |
| Corticosteroids | 76.2 | 66.7 | 0.44 |
| MMF/Mycophenolic acid | 21.4 | 13.7 | 0.48 |
| Azathioprine | 14.3 | 5.9 | 0.29 |
| Cyclophosphamide | 2.4 | 0 | 0.45 |
| Rituximab | 0 | 2 | 1 |
| Methotrexate | 2.4 | 2 | 1 |
| LN172+ | LN172− | p | |
|---|---|---|---|
| Patients, n (%) | 86 (92.5) | 7 (7.5) | |
| Women—n (%) | 80 (93) | 6 (85.7) | 0.43 |
| Mean age ± SD | 35 ± 11 | 36 ± 10 | 0.80 |
| Ethnicity—n (%) | 0.07 | ||
| European | 35 (40.7) | 5 (71.4) | 0.13 |
| North African | 22 (25.6) | 1 (14.3) | 0.67 |
| African | 21 (24.4) | 1 (14.3) | 1 |
| Asian | 8 (9.3) | 0 (0) | 1 |
| Characteristics of kidney biopsy | |||
| Serum creatinine—μmol/L, mean ± SD | 80 ± 61 | 184.6 ± 114 | 0.003 |
| eGFR—mL/min/1.73 m2, mean ± SD | 94.9 ± 38 | 46.2 ± 29 | 0.001 |
| UPCR—g/g, mean ± SD | 2.29 ± 2.03 | 2.95 ± 2.48 | 0.79 |
| CKD—n (%) | 6 (7.0) | 3 (42.9) | 0.01 |
| Complement consumption (%) | 71.4 | 66.7 | 1 |
| Anti-DNA antibodies (%) | 86.3 | 85.7 | 1 |
| CKD273 score | 0.56 ± 0.35 | 0.86 ± 0.13 | 0.02 |
| SLE vintage | |||
| First flare of SLE—n (%) | 20 (23.3) | 1 (14.3) | 1 |
| Pre-existing SLE—n% | 66 (76.7) | 6 (85.7) | 1 |
| Disease duration—years, mean ± SD | 10.5 ± 8.6 | 11.7 ± 7.5 | 0.56 |
| First renal flare—n (%) | 53 (61.6) | 2 (28.6) | 0.11 |
| LN duration—years, mean ± SD | 8.0 ± 6.9 | 9.8 ± 7.8 | 0.58 |
| Kidney biopsies, n | |||
| Class, n (%) | 0.37 | ||
| I | 1 (1.2) | 0 (0) | 1 |
| II | 6 (7.0) | 0 (0) | 1 |
| III-A or -A/C ± V | 19 (22.1) | 3 (42.9) | 0.36 |
| III-C ± V | 5 (5.8) | 0 (0) | 1 |
| IV-A or -A/C ±V | 30 (34.9) | 3 (42.9) | 0.70 |
| IV-C ± V | 2 (1.2) | 0 (0) | 1 |
| V | 21 (24.4) | 0 (0) | 0.34 |
| VI | 2 (2.3) | 1 (1.2) | 0.21 |
| IF/TA, n—(%) | 0.16 | ||
| F0 | 40 (46.5) | 1 (14.3) | 0.13 |
| F1 | 30 (34.9) | 3 (42.9) | 0.70 |
| F2 | 10 (11.6) | 2 (28.6) | 0.22 |
| F3 | 6 (7.0) | 1 (14.3) | 0.43 |
| Group | |||
| Active LN | 49 (57.0) | 6 (85.7) | 0.23 |
| Non-active LN | 37 (43.0) | 1 (14.3) | 0.23 |
| Patients/center—n (%) | 0.18 | ||
| Marseille | 50 (58.1) | 3 (42.9) | 0.46 |
| Paris | 34 (39.5) | 3 (42.9) | 1 |
| Toulouse | 2 (2.3) | 1 (14.3) | 0.21 |
| Previous treatment for SLE—% | |||
| Hydroxychloroquine | 81.2 | 100 | 0.59 |
| Corticosteroids | 78.8 | 83.3 | 1 |
| MMF/Mycophenolic acid | 23.8 | 66.7 | 0.04 |
| Azathioprine | 17.9 | 50 | 0.09 |
| Cyclophosphamide | 32.1 | 66.7 | 0.18 |
| Rituximab | 7.1 | 33.3 | 0.09 |
| Other | 11.8 | 50 | 0.04 |
| Treatment for SLE at inclusion—% | |||
| Hydroxychloroquine | 69.4 | 83.3 | 0.67 |
| Corticosteroids | 71.8 | 83.3 | 1 |
| MMF/Mycophenolic acid | 16.7 | 33.3 | 0.29 |
| Azathioprine | 9.5 | 16.7 | 0.48 |
| Cyclophosphamide | 0 | 16.7 | 0.07 |
| Rituximab | 1.2 | 0 | 1 |
| Methotrexate | 2.4 | 0 | 1 |
| Relapse of LN | |||
| Total—n (%) | 19 (22.1) | 0 (0) | 0.33 |
| Renal function at last follow-up | |||
| Serum creatinine—μmol/L, mean ± SD | 70.7 ± 32.7 | 128.7 ± 109.8 | 0.064 |
| eGFR—mL/min/1.73 m2, mean ± SD | 104.8 ± 29.9 | 67.5 ± 32 | 0.004 |
| UPCR—g/g, mean ± SD | 0.42 ± 0.55 | 0.68 ± 1.52 | 0.17 |
References
- Cervera, R. Systemic lupus erythematosus in Europe at the change of the millennium: Lessons from the “Euro-Lupus Project”. Autoimmun. Rev. 2006, 5, 180–186. [Google Scholar] [CrossRef]
- Cervera, R.; Khamashta, M.A.; Font, J.; Sebastiani, G.D.; Gil, A.; Lavilla, P.; Mejía, J.C.; Aydintug, A.O.; Chwalinska-Sadowska, H.; de Ramón, E.; et al. Morbidity and Mortality in Systemic Lupus Erythematosus During a 10-Year Period. Medicine 2003, 82, 299–308. [Google Scholar] [CrossRef]
- Houssiau, F.A.; Vasconcelos, C.; D’Cruz, D.; Sebastiani, G.D.; Garrido, E.D.R.; Danieli, M.G.; Abramovicz, D.; Blockmans, D.; Cauli, A.; Direskeneli, H.; et al. The 10-year follow-up data of the Euro-Lupus Nephritis Trial comparing low-dose and high-dose intravenous cyclophosphamide. Ann. Rheum. Dis. 2009, 69, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; Ferrario, F.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004, 65, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Bertsias, G.K.; Tektonidou, M.; Amoura, Z.; Aringer, M.; Bajema, I.; Berden, J.H.M.; Boletis, J.; Cervera, R.; Doerner, T.; Doria, A.; et al. Joint European League Against Rheumatism and European Renal Association–European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann. Rheum. Dis. 2012, 71, 1771–1782. [Google Scholar] [CrossRef]
- Dörner, T.; Furie, R. Novel paradigms in systemic lupus erythematosus. Lancet 2019, 393, 2344–2358. [Google Scholar] [CrossRef]
- Hong, S.; Healy, H.; Kassianos, A.J. The Emerging Role of Renal Tubular Epithelial Cells in the Immunological Pathophysiology of Lupus Nephritis. Front. Immunol. 2020, 11, 578952. [Google Scholar] [CrossRef]
- Wilson, P.C.; Kashgarian, M.; Moeckel, G. Interstitial inflammation and interstitial fibrosis and tubular atrophy predict renal survival in lupus nephritis. Clin. Kidney J. 2018, 11, 207–218. [Google Scholar] [CrossRef]
- Espeli, M.; Bökers, S.; Giannico, G.; Dickinson, H.A.; Bardsley, V.; Fogo, A.B.; Smith, K.G. Local Renal Autoantibody Production in Lupus Nephritis. J. Am. Soc. Nephrol. 2010, 22, 296–305. [Google Scholar] [CrossRef]
- Narváez, J.; Ricse, M.; Gomà, M.; Mitjavila, F.; Fulladosa, X.; Capdevila, O.; Torras, J.; Juanola, X.; Pujol-Farriols, R.; Nolla, J.M. The value of repeat biopsy in lupus nephritis flares. Medicine 2017, 96, e7099. [Google Scholar] [CrossRef]
- Bataille, S.; Jourde, N.; Daniel, L.; Mondain, J.-R.; Faure, M.; Gobert, P.; Alcheikh-Hassan, Z.; Lankester, M.; Giaime, P.; Gaudart, J.; et al. Comparative Safety and Efficiency of Five Percutaneous Kidney Biopsy Approaches of Native Kidneys: A Multicenter Study. Am. J. Nephrol. 2012, 35, 387–393. [Google Scholar] [CrossRef]
- Soliman, S.; Mohan, C. Lupus nephritis biomarkers. Clin. Immunol. 2017, 185, 10–20. [Google Scholar] [CrossRef]
- Gulati, G.; Bennett, M.R.; Abulaban, K.; Song, H.; Zhang, X.; Ma, Q.; Brodsky, S.V.; Nadasdy, T.; Haffner, C.; Wiley, K.; et al. Prospective validation of a novel renal activity index of lupus nephritis. Lupus 2016, 26, 927–936. [Google Scholar] [CrossRef]
- Kitagawa, A.; Tsuboi, N.; Yokoe, Y.; Katsuno, T.; Ikeuchi, H.; Kajiyama, H.; Endo, N.; Sawa, Y.; Suwa, J.; Sugiyama, Y.; et al. Urinary levels of the leukocyte surface molecule CD11b associate with glomerular inflammation in lupus nephritis. Kidney Int. 2019, 95, 680–692. [Google Scholar] [CrossRef]
- Ding, Y.; Nie, L.-M.; Pang, Y.; Wu, W.-J.; Tan, Y.; Yu, F.; Zhao, M.-H. Composite urinary biomarkers to predict pathological tubulointerstitial lesions in lupus nephritis. Lupus 2018, 27, 1778–1789. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Bascands, J.-L.; Mischak, H.; Schanstra, J.P. The role of urinary peptidomics in kidney disease research. Kidney Int. 2016, 89, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Lacroix, C.; Caubet, C.; Siwy, J.; Zürbig, P.; Dakna, M.; Muller, F.; Breuil, B.; Stalmach, A.; Mullen, W.; et al. Fetal Urinary Peptides to Predict Postnatal Outcome of Renal Disease in Fetuses with Posterior Urethral Valves (PUV). Sci. Transl. Med. 2013, 5, 198ra106. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Buffin-Meyer, B.; Boizard, F.; Moussaoui, N.; Lescat, O.; Breuil, B.; Fedou, C.; Feuillet, G.; Casemayou, A.; Neau, E.; et al. Amniotic fluid peptides predict postnatal kidney survival in developmental kidney disease. Kidney Int. 2021, 99, 737–749. [Google Scholar] [CrossRef]
- Desveaux, C.; Klein, J.; Leruez-Ville, M.; Ramirez-Torres, A.; Lacroix, C.; Breuil, B.; Froment, C.; Bascands, J.-L.; Schanstra, J.P.; Ville, Y. Identification of Symptomatic Fetuses Infected with Cytomegalovirus Using Amniotic Fluid Peptide Biomarkers. PLoS Pathog. 2016, 12, e1005395. [Google Scholar] [CrossRef] [PubMed]
- Good, D.M.; Zürbig, P.; Argilés, À.; Bauer, H.W.; Behrens, G.; Coon, J.J.; Dakna, M.; Decramer, S.; Delles, C.; Dominiczak, A.F.; et al. Naturally Occurring Human Urinary Peptides for Use in Diagnosis of Chronic Kidney Disease. Mol. Cell. Proteom. 2010, 9, 2424–2437. [Google Scholar] [CrossRef] [PubMed]
- Pontillo, C.; Zhang, Z.-Y.; Schanstra, J.P.; Jacobs, L.; Zürbig, P.; Thijs, L.; Ramírez-Torres, A.; Heerspink, H.J.; Lindhardt, M.; Klein, R.; et al. Prediction of Chronic Kidney Disease Stage 3 by CKD273, a Urinary Proteomic Biomarker. Kidney Int. Rep. 2017, 2, 1066–1075. [Google Scholar] [CrossRef] [PubMed]
- Schanstra, J.P.; Zürbig, P.; Alkhalaf, A.; Argiles, A.; Bakker, S.J.; Beige, J.; Bilo, H.J.; Chatzikyrkou, C.; Dakna, M.; Dawson, J.; et al. Diagnosis and Prediction of CKD Progression by Assessment of Urinary Peptides. J. Am. Soc. Nephrol. 2015, 26, 1999–2010. [Google Scholar] [CrossRef] [PubMed]
- Haubitz, M.; Wittke, S.; Weissinger, E.M.; Walden, M.; Rupprecht, H.D.; Floege, J.; Haller, H.; Mischak, H. Urine protein patterns can serve as diagnostic tools in patients with IgA nephropathy. Kidney Int. 2005, 67, 2313–2320. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wittke, S.; Mischak, H.; Walden, M.; Kolch, W.; Rädler, T.; Wiedemann, K. Discovery of biomarkers in human urine and cerebrospinal fluid by capillary electrophoresis coupled to mass spectrometry: Towards new diagnostic and therapeutic approaches. Electrophoresis 2005, 26, 1476–1487. [Google Scholar] [CrossRef]
- Weissinger, E.M.; Wittke, S.; Kaiser, T.; Haller, H.; Bartel, S.; Krebs, R.; Golovko, I.; Rupprecht, H.D.; Haubitz, M.; Hecker, H.; et al. Proteomic patterns established with capillary electrophoresis and mass spectrometry for diagnostic purposes. Kidney Int. 2004, 65, 2426–2434. [Google Scholar] [CrossRef]
- Varghese, S.A.; Powell, T.B.; Budisavljevic, M.N.; Oates, J.C.; Raymond, J.R.; Almeida, J.S.; Arthur, J.M. Urine Biomarkers Predict the Cause of Glomerular Disease. J. Am. Soc. Nephrol. 2007, 18, 913–922. [Google Scholar] [CrossRef]
- Zhang, X.; Jin, M.; Wu, H.; Nadasdy, T.; Nadasdy, G.; Harris, N.; Green-Church, K.; Nagaraja, H.; Birmingham, D.J.; Yu, C.-Y.; et al. Biomarkers of lupus nephritis determined by serial urine proteomics. Kidney Int. 2008, 74, 799–807. [Google Scholar] [CrossRef]
- Suzuki, M.; Ross, G.F.; Wiers, K.; Nelson, S.; Bennett, M.; Passo, M.H.; Devarajan, P.; Brunner, H.I. Identification of a urinary proteomic signature for lupus nephritis in children. Pediatr. Nephrol. 2007, 22, 2047–2057. [Google Scholar] [CrossRef]
- Suzuki, M.; Wiers, K.; Brooks, E.B.; Greis, K.D.; Haines, K.; Klein-Gitelman, M.S.; Olson, J.; Onel, K.; O’Neil, K.M.; Silverman, E.D.; et al. Initial Validation of a Novel Protein Biomarker Panel for Active Pediatric Lupus Nephritis. Pediatr. Res. 2009, 65, 530–536. [Google Scholar] [CrossRef]
- Oates, J.; Varghese, S.; Bland, A.M.; Taylor, T.P.; Self, S.E.; Stanislaus, R.; Almeida, J.S.; Arthur, J.M. Prediction of urinary protein markers in lupus nephritis. Kidney Int. 2005, 68, 2588–2592. [Google Scholar] [CrossRef][Green Version]
- Mosley, K.; Tam, F.W.K.; Edwards, R.J.; Crozier, J.; Pusey, C.D.; Lightstone, L. Urinary proteomic profiles distinguish between active and inactive lupus nephritis. Rheumatology 2006, 45, 1497–1504. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pejchinovski, M.; Siwy, J.; Mullen, W.; Mischak, H.; Petri, M.A.; Burkly, L.C.; Wei, R. Urine peptidomic biomarkers for diagnosis of patients with systematic lupus erythematosus. Lupus 2018, 27, 6–16. [Google Scholar] [CrossRef]
- Wei, R.; Gao, B.; Shih, F.; Ranger, A.; Dearth, A.; Mischak, H.; Siwy, J.; Wisniacki, N.; Petri, M.; Burkly, L.C. Alterations in urinary collagen peptides in lupus nephritis subjects correlate with renal dysfunction and renal histopathology. Nephrol. Dial. Transplant. 2017, 32, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Siwy, J.; Zürbig, P.; Argiles, A.; Beige, J.; Haubitz, M.; Jankowski, J.; Julian, B.A.; Linde, P.G.; Marx, D.; Mischak, H.; et al. Noninvasive diagnosis of chronic kidney diseases using urinary proteome analysis. Nephrol. Dial. Transplant. 2016, 32, 2079–2089. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American college of rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Orbai, A.-M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Haas, M. The Revised (2013) Banff Classification for Antibody-Mediated Rejection of Renal Allografts: Update, Difficulties, and Future Considerations. Arab. Archaeol. Epigr. 2016, 16, 1352–1357. [Google Scholar] [CrossRef]
- Theodorescu, D.; Wittke, S.; Ross, M.M.; Walden, M.; Conaway, M.; Just, I.; Mischak, H.; Frierson, H.F. Discovery and validation of new protein biomarkers for urothelial cancer: A prospective analysis. Lancet Oncol. 2006, 7, 230–240. [Google Scholar] [CrossRef]
- Mischak, H.; Vlahou, A.; Ioannidis, J.P. Technical aspects and inter-laboratory variability in native peptide profiling: The CE–MS experience. Clin. Biochem. 2013, 46, 432–443. [Google Scholar] [CrossRef]
- Jantos-Siwy, J.; Schiffer, E.; Brand, K.; Schumann, G.; Rossing, K.; Delles, C.; Mischak, H.; Metzger, J. Quantitative Urinary Proteome Analysis for Biomarker Evaluation in Chronic Kidney Disease. J. Proteome Res. 2009, 8, 268–281. [Google Scholar] [CrossRef]
- Pontillo, C.; Mischak, H. Urinary peptide-based classifier CKD273: Towards clinical application in chronic kidney disease. Clin. Kidney J. 2017, 10, 192–201. [Google Scholar] [CrossRef]
- Magalhães, P.; Pejchinovski, M.; Markoska, K.; Banasik, M.; Klinger, M.; Švec-Billá, D.; Rychlík, I.; Rroji, M.; Restivo, A.; Capasso, G.; et al. Association of kidney fibrosis with urinary peptides: A path towards non-invasive liquid biopsies? Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tofte, N.; Lindhardt, M.; Adamova, K.; Bakker, S.J.L.; Beige, J.; Beulens, J.W.J.; Birkenfeld, A.L.; Currie, G.; Delles, C.; Dimos, I.; et al. Early detection of diabetic kidney disease by urinary proteomics and subsequent intervention with spironolactone to delay progression (PRIORITY): A prospective observational study and embedded randomised placebo-controlled trial. Lancet Diabetes Endocrinol. 2020, 8, 301–312. [Google Scholar] [CrossRef]
- Lindhardt, M.; Persson, F.; Currie, G.; Pontillo, C.; Beige, J.; Delles, C.; Von Der Leyen, H.; Mischak, H.; Navis, G.; Noutsou, M.; et al. Proteomic prediction and Renin angiotensin aldosterone system Inhibition prevention of early diabetic nephRopathy in TYpe 2 diabetic patients with normoalbuminuria (PRIORITY): Essential study design and rationale of a randomised clinical multicentre trial. BMJ Open 2016, 6, e010310. [Google Scholar] [CrossRef] [PubMed]
- Lindhardt, M.; Persson, F.; Zürbig, P.; Stalmach, A.; Mischak, H.; De Zeeuw, D.; Heerspink, H.L.; Klein, R.; Orchard, T.; Porta, M.; et al. Urinary proteomics predict onset of microalbuminuria in normoalbuminuric type 2 diabetic patients, a sub-study of the DIRECT-Protect 2 study. Nephrol. Dial. Transplant. 2016, 32, 1866–1873. [Google Scholar] [CrossRef]
- Rijnink, E.C.; Teng, Y.O.; Wilhelmus, S.; Almekinders, M.; Wolterbeek, R.; Cransberg, K.; Bruijn, J.A.; Bajema, I.M. Clinical and Histopathologic Characteristics Associated with Renal Outcomes in Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Obrișcă, B.; Jurubiță, R.; Andronesi, A.; Sorohan, B.; Achim, C.; Bobeica, R.; Gherghiceanu, M.; Mandache, E.; Ismail, G. Histological predictors of renal outcome in lupus nephritis: The importance of tubulointerstitial lesions and scoring of glomerular lesions. Lupus 2018, 27, 1455–1463. [Google Scholar] [CrossRef]
- Hsieh, C.; Chang, A.; Brandt, D.; Guttikonda, R.; Utset, T.O.; Clark, M.R. Predicting outcomes of lupus nephritis with tubulointerstitial inflammation and scarring. Arthritis Rheum. 2011, 63, 865–874. [Google Scholar] [CrossRef]
- Leatherwood, C.; Speyer, C.B.; Feldman, C.H.; D’Silva, K.; Gómez-Puerta, J.A.; Hoover, P.J.; Waikar, S.S.; McMahon, G.M.; Rennke, H.G.; Costenbader, K.H. Clinical characteristics and renal prognosis associated with interstitial fibrosis and tubular atrophy (IFTA) and vascular injury in lupus nephritis biopsies. Semin. Arthritis Rheum. 2019, 49, 396–404. [Google Scholar] [CrossRef]
- Pagni, F.; Galimberti, S.; Galbiati, E.; Rebora, P.; Pietropaolo, V.; Pieruzzi, F.; Smith, A.J.; Ferrario, F. Tubulointerstitial lesions in lupus nephritis: International multicentre study in a large cohort of patients with repeat biopsy. Nephrology 2016, 21, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Mavragani, C.P.; Fragoulis, G.E.; Somarakis, G.; Drosos, A.; Tzioufas, A.G.; Moutsopoulos, H.M. Clinical and Laboratory Predictors of Distinct Histopathogical Features of Lupus Nephritis. Medicine 2015, 94, e829. [Google Scholar] [CrossRef] [PubMed]
- Mejia-Vilet, J.M.; Parikh, S.V.; Song, H.; Fadda, P.; Shapiro, J.P.; Ayoub, I.; Yu, L.; Zhang, J.; Uribe-Uribe, N.; Rovin, B.H. Immune gene expression in kidney biopsies of lupus nephritis patients at diagnosis and at renal flare. Nephrol. Dial. Transplant. 2019, 34, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Almaani, S.; Prokopec, S.D.; Zhang, J.; Yu, L.; Avila-Casado, C.; Wither, J.; Scholey, J.W.; Alberton, V.; Malvar, A.; Parikh, S.V.; et al. Rethinking Lupus Nephritis Classification on a Molecular Level. J. Clin. Med. 2019, 8, 1524. [Google Scholar] [CrossRef] [PubMed]
- Arazi, A.; Rao, D.A.; Berthier, C.C.; Davidson, A.; Liu, Y.; Hoover, P.J.; Chicoine, A.; Eisenhaure, T.M.; Jonsson, A.H.; Li, S.; et al. The immune cell landscape in kidneys of patients with lupus nephritis. Nat. Immunol. 2019, 20, 902–914. [Google Scholar] [CrossRef]
- Abedini, A.; Zhu, Y.O.; Chatterjee, S.; Halasz, G.; Devalaraja-Narashimha, K.; Shrestha, R.; Balzer, M.S.; Park, J.; Zhou, T.; Ma, Z.; et al. Urinary Single-Cell Profiling Captures the Cellular Diversity of the Kidney. J. Am. Soc. Nephrol. 2021, 32, 614–627. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, D.J.; Irshaid, F.; Nagaraja, H.N.; Zou, X.; Tsao, B.P.; Wu, H.; Yu, C.Y.; Hebert, L.A.; Rovin, B.H. The complex nature of serum C3 and C4 as biomarkers of lupus renal flare. Lupus 2010, 19, 1272–1280. [Google Scholar] [CrossRef]
- Mok, C.C.; Ying, K.Y.; Tang, S.; Leung, C.Y.; Lee, K.W.; Ng, W.L.; Wong, R.W.S.; Lau, C.S. Predictors and outcome of renal flares after successful cyclophosphamide treatment for diffuse proliferative lupus glomerulonephritis. Arthritis Rheum. 2004, 50, 2559–2568. [Google Scholar] [CrossRef]
- Linnik, M.D.; Hu, J.Z.; Heilbrunn, K.R.; Strand, V.; Hurley, F.L.; Joh, T. LJP 394 Investigator Consortium Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheum. 2005, 52, 1129–1137. [Google Scholar] [CrossRef]
- Steiman, A.J.; Gladman, D.D.; Ibañez, M.; Urowitz, M.B. Prolonged Serologically Active Clinically Quiescent Systemic Lupus Erythematosus: Frequency and Outcome. J. Rheumatol. 2010, 37, 1822–1827. [Google Scholar] [CrossRef] [PubMed]
- Gensous, N.; Marti, A.; Barnetche, T.; Blanco, P.; Lazaro, E.; Seneschal, J.; Truchetet, M.-E.; Duffau, P.; Richez, C. Predictive biological markers of systemic lupus erythematosus flares: A systematic literature review. Arthritis Res. 2017, 19, 238. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, M.; Azzato, F.; Toblli, J.E.; De Rosa, G.; Fuentes, F.; Nagaraja, H.N.; Nash, R.; Rovin, B.H. A prospective observational cohort study highlights kidney biopsy findings of lupus nephritis patients in remission who flare following withdrawal of maintenance therapy. Kidney Int. 2018, 94, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Piñeiro, G.J.; Arrizabalaga, P.; Solé, M.; Abellana, R.M.; Espinosa, G.; Cervera, R. Repeated Renal Biopsy—A Predictive Tool to Assess the Probability of Renal Flare in Lupus Nephritis. Am. J. Nephrol. 2016, 44, 439–446. [Google Scholar] [CrossRef]


| Characteristics | |
|---|---|
| Patients, n | 93 |
| Women—n (%) | 86 (92.4) |
| Age—years | 35 ± 11 |
| Range—years | 19–58 |
| Ethnicity—n (%) | |
| European | 40 (43) |
| North African | 23 (24.7) |
| African | 23 (23.7) |
| Asian | 8 (8.6) |
| Characteristics at kidney biopsy | |
| Serum creatinine—μmol/L | 92.1 ± 68.5 |
| eGFR—mL/min/1.73 m2 | 91.4 ± 39.2 |
| UPCR—g/g | 2.34 ± 2.23 |
| SLE vintage | |
| First flare of SLE—n (%) | 21 (22.6) |
| Pre-existing SLE—n% | 72 (77.4) |
| Disease duration—years | 10.6 ± 8.5 |
| First renal flare—n (%) | 55 (59.1) |
| LN duration—years | 8.2 ± 6.9 |
| Kidney biopsies—n (%) | 93 |
| Class ISN/RPS 2003 | |
| I | 1 (1.1) |
| II | 6 (6.5) |
| III-A or -A/C ± V | 22 (23.7) |
| III-C ±V | 5 (5.4) |
| IV-A or -A/C ± V | 33 (35.5) |
| IV-C ±V | 2 (2.2) |
| Pure V | 21 (22.6) |
| VI | 3 (3.2) |
| Group | |
| Active LN | 55 (59.1) |
| Non-active LN | 38 (40.9) |
| IF/TA | |
| F0 | 41 (44.1) |
| F1 | 33 (35.5) |
| F2 | 12 (12.9) |
| F3 | 7 (7.5) |
| Previous treatment for SLE (%) | |
| Hydroxychloroquine | 80.6 |
| Corticosteroids | 77.4 |
| MMF/Mycophenolic acid | 25.8 |
| Azathioprine | 19.4 |
| Cyclophosphamide | 33.3 |
| Rituximab | 8.6 |
| Other | 14 |
| Treatment for SLE at inclusion (%) | |
| Hydroxychloroquine | 68.8 |
| Corticosteroids | 70.1 |
| MMF/Mycophenolic acid | 17.2 |
| Azathioprine | 9.7 |
| Cyclophosphamide | 1.1 |
| Rituximab | 1.1 |
| Other | 2.2 |
| Patients/center—n (%) | |
| Marseille | 37 (39.8) |
| Paris | 53 (57) |
| Toulouse | 3 (3.2) |
| Discovery Cohort | Validation Cohort | p | |
|---|---|---|---|
| Follow-up—months, median [IQR] | 63.5 (51–69) | 32 (24–39) | <0.001 |
| Renal function at M24 | |||
| Serum creatinine—μmol/L, mean ± SD | 64.8 ± 12.5 | 75.3 ± 19.9 | 0.12 |
| eGFR—mL/min/1.73 m2, mean ± SD | 109 ± 22.1 | 96.6 ± 23.8 | 0.12 |
| UPCR—g/g, mean ± SD | 0.55 ± 0.57 | 0.42 ± 0.36 | 0.73 |
| Renal function at last follow-up | |||
| Serum creatinine—μmol/L, mean ± SD | 73.5 ± 23.1 | 76.2 ± 20.8 | 0.31 |
| eGFR—mL/min/1.73 m2, mean ± SD | 106.8 ± 26 | 96.1 ± 19.6 | 0.22 |
| UPCR—g/g, mean ± SD | 0.56 ± 0.55 | 0.37 ± 0.35 | 0.44 |
| Relapse of LN | |||
| Total—n (%) | 11 (26.2) | 8 (15.7) | 0.21 |
| Early relapse <M24—n (%) | 5 (11.9) | 8 (15.7) | 1 |
| Time until relapse—months, mean ± SD | 29.3 ± 19.6 | 12.3 ± 3.6 | 0.016 |
| CKD (eGFR < 60 mL/min/1.73 m2) | |||
| Total, n (%) | 6 (14.3) | 6 (11.8) | 0.56 |
| New onset CKD at last follow-up | 2 (4.8) | 1 (2) | 0.58 |
| New onset CKD at M24 | 0 | 0 | NS |
| Time until CKD—months, mean ± SD | 27.5 ± 1.5 | 35 | NS |
| ESKD | |||
| At M24—n (%) | 2 (4.8) | 0 | NS |
| At the end of follow up—n (%) | 3 (7.1) | 2 (3.9) | NS |
| Time until ESKD—months, mean± SD | 17.3 ± 8.4 | 23 ± 11 | 0.55 |
| Death—n (%) | 3 (7) | 1 (2) | |
| Time until death—months mean± SD | 26.3 ± 13.1 | 39 | NS |
| Active LN | Non-Active LN | p | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|---|
| Peptidomic | No profile | NA | NA | NA | NA | ||
| Complement consumption (%) | 84 | 46.1 | 0.001 | 0.84 | 0.54 | 0.78 | 0.64 |
| Anti-DNA antibodies (%) | 95.8 | 71.9 | 0.007 | 0.96 | 0.28 | 0.67 | 0.82 |
| Hematuria (%) | 53.1 | 40.0 | 0.37 | 0.53 | 0.60 | 0.68 | 0.44 |
| Pyuria (%) | 64.3 | 33.3 | 0.03 | 0.64 | 0.67 | 0.77 | 0.52 |
| Mean eGFR (mL/min/1.73 m2) | 82.7 ± 31 | 104.4 ± 47 | 0.01 | NA | NA | NA | NA |
| Mean UPCR (g/g) | 2.63 ± 2.3 | 1.97 ± 1.7 | 0.09 | NA | NA | NA | NA |
| Mean serum creatinine (μmol/L) | 96.7 ± 71 | 87.1 ± 71 | 0.01 | NA | NA | NA | NA |
| Parameter | r | p |
|---|---|---|
| Peptidomic | No profile | |
| CKD273 | 0.314 | 0.0015 |
| SLE duration | 0.408 | <0.0001 |
| LN duration | 0.450 | <0.0001 |
| Age | 0.231 | 0.026 |
| Serum creatinine | 0.274 | 0.008 |
| eGFR (MDRD) | −0.290 | 0.005 |
| UPCR | 0.164 | 0.121 |
| Hematuria | −0.031 | 0.783 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tailliar, M.; Schanstra, J.P.; Dierckx, T.; Breuil, B.; Hanouna, G.; Charles, N.; Bascands, J.-L.; Dussol, B.; Vazi, A.; Chiche, L.; et al. Urinary Peptides as Potential Non-Invasive Biomarkers for Lupus Nephritis: Results of the Peptidu-LUP Study. J. Clin. Med. 2021, 10, 1690. https://doi.org/10.3390/jcm10081690
Tailliar M, Schanstra JP, Dierckx T, Breuil B, Hanouna G, Charles N, Bascands J-L, Dussol B, Vazi A, Chiche L, et al. Urinary Peptides as Potential Non-Invasive Biomarkers for Lupus Nephritis: Results of the Peptidu-LUP Study. Journal of Clinical Medicine. 2021; 10(8):1690. https://doi.org/10.3390/jcm10081690
Chicago/Turabian StyleTailliar, Maxence, Joost P. Schanstra, Tim Dierckx, Benjamin Breuil, Guillaume Hanouna, Nicolas Charles, Jean-Loup Bascands, Bertrand Dussol, Alain Vazi, Laurent Chiche, and et al. 2021. "Urinary Peptides as Potential Non-Invasive Biomarkers for Lupus Nephritis: Results of the Peptidu-LUP Study" Journal of Clinical Medicine 10, no. 8: 1690. https://doi.org/10.3390/jcm10081690
APA StyleTailliar, M., Schanstra, J. P., Dierckx, T., Breuil, B., Hanouna, G., Charles, N., Bascands, J.-L., Dussol, B., Vazi, A., Chiche, L., Siwy, J., Faguer, S., Daniel, L., Daugas, E., Jourde-Chiche, N., & on behalf of the Groupe Coopératif sur le Lupus Rénal (GCLR). (2021). Urinary Peptides as Potential Non-Invasive Biomarkers for Lupus Nephritis: Results of the Peptidu-LUP Study. Journal of Clinical Medicine, 10(8), 1690. https://doi.org/10.3390/jcm10081690