
Individual Lymphocyte Sensitivity to Steroids as a Reliable Biomarker for Clinical Outcome after Steroid Withdrawal in Japanese Renal Transplantation

Abstract
1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Subjects
2.3. GC Withdrawal Protocol
2.4. PBMC Isolation and Culture
2.5. Evaluation of the Effect of GCs on PBMC Proliferation Rate
2.6. Comparison of the IC50 Values between the “Clinical Event Group” and the “Event-Free Group”
2.7. Comparison of the Clinical Outcome between the PBMC High-Sensitivity Group and the PBMC Low-Sensitivity Group to GCs
2.8. Statistical Analysis
3. Results
3.1. The Recipient Characteristics
3.2. Comparison of the IC50 Values between the Clinical Event Group and the Event-Free Group Regarding Experience of Increase/Resumption of GC Administrations
3.3. Comparison of the IC50 Values between the Clinical Event Group and the Event-Free Group Regarding Incidence of AR
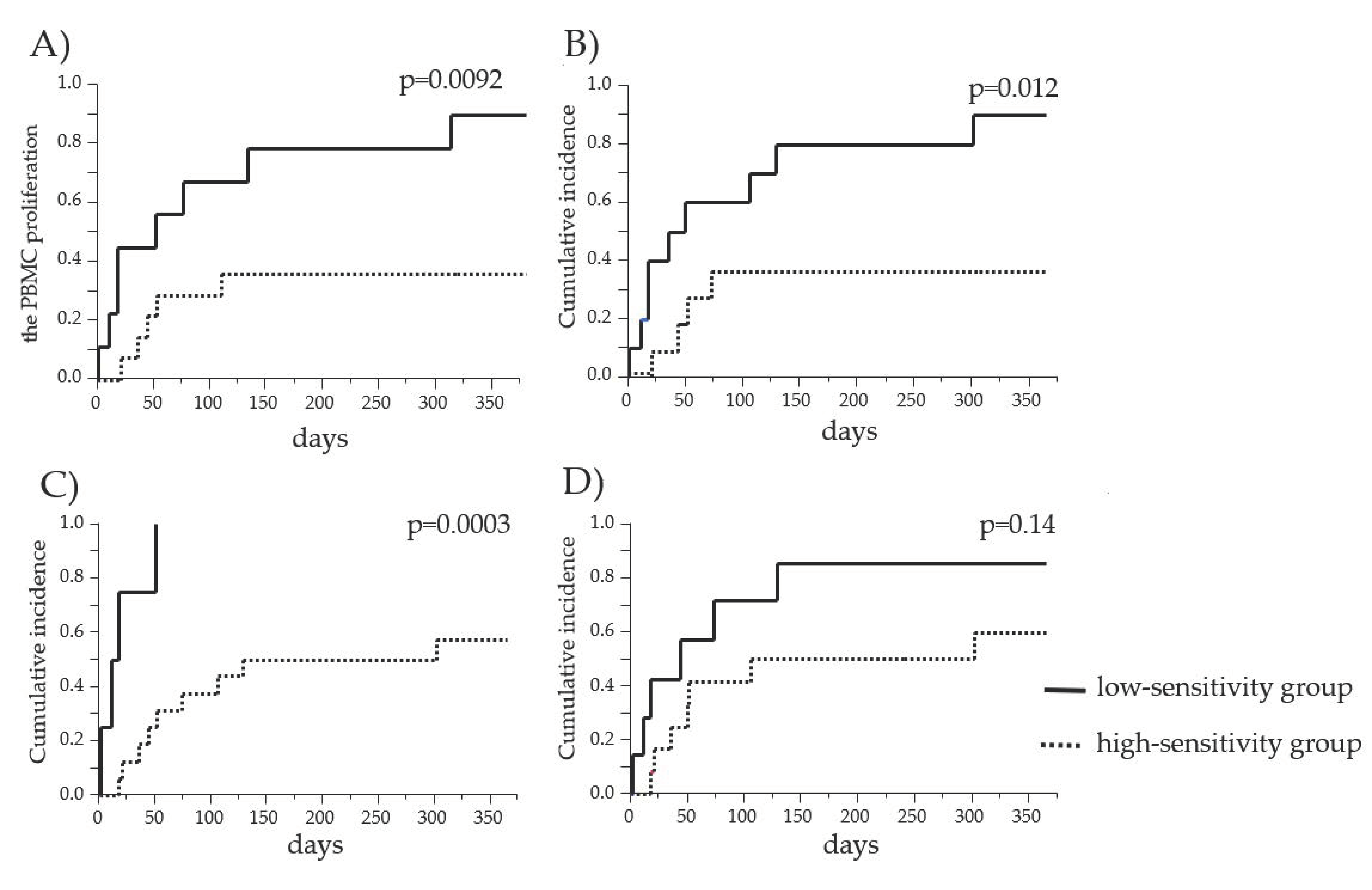
3.4. Comparison of the Cumulative Incidence of GC Increase/Resumption between the PBMC High-Sensitivity Group and the PBMC Low-Sensitivity Group to GCs
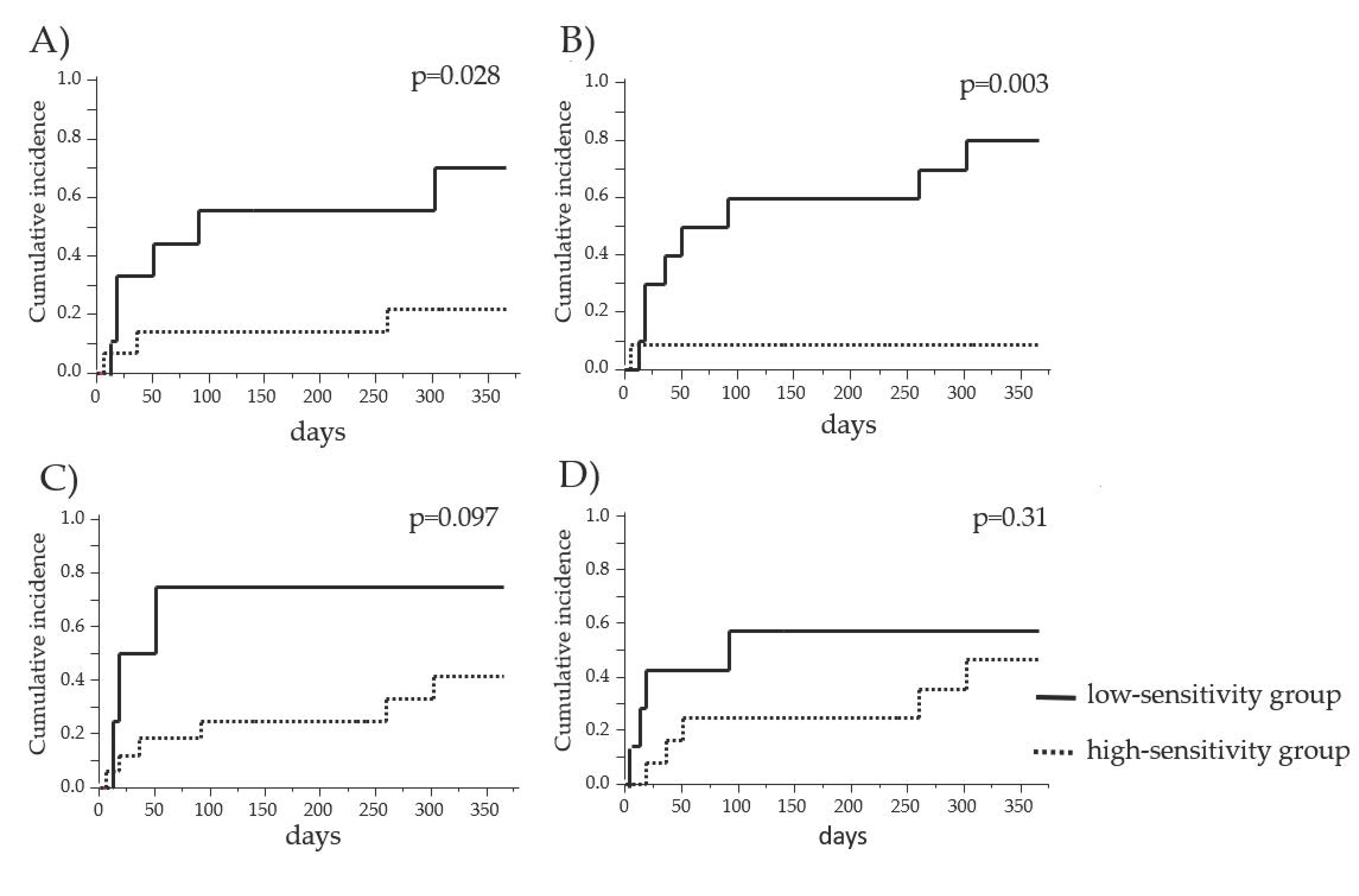
3.5. Comparison of the Cumulative Incidence of AR between the PBMC High-Sensitivity Group and the PBMC Low-Sensitivity Group to GCs
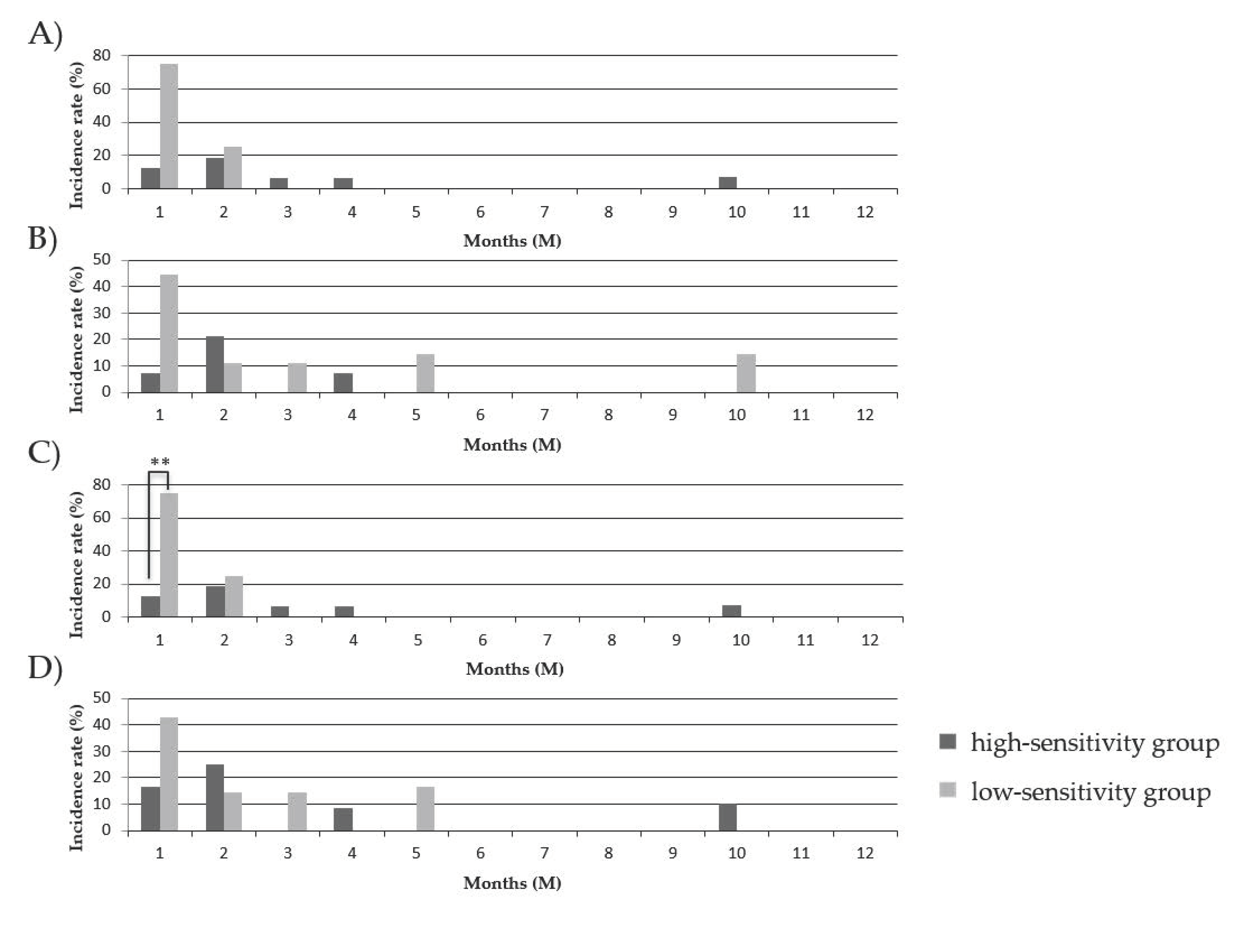
3.6. Comparison of the Onset Time of GC Increase/Resumption between the PBMC High-Sensitivity Group and the PBMC Low-Sensitivity Group to GCs
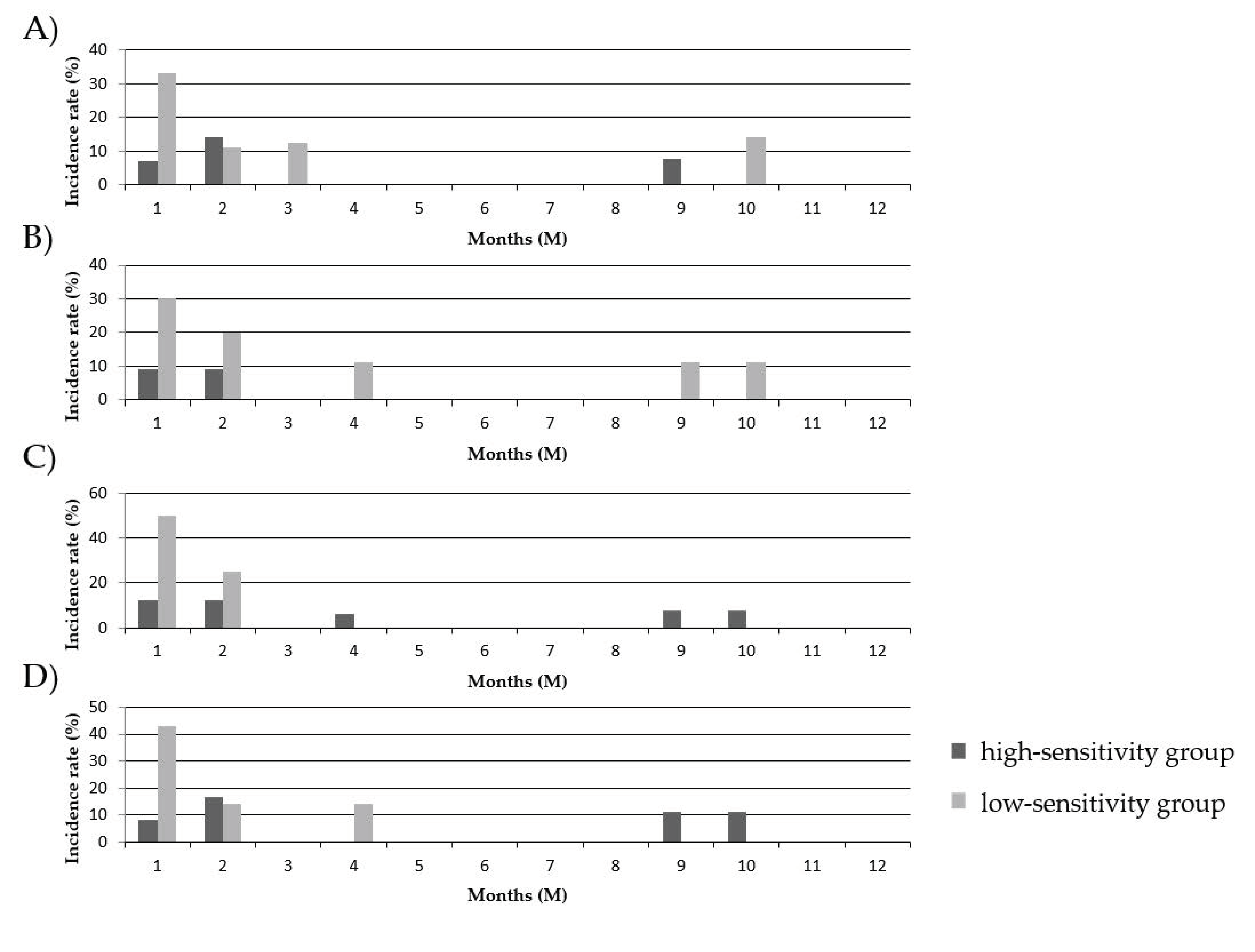
3.7. Comparison of the Onset Time of AR between the PBMC High-Sensitivity Group and the PBMC Low-Sensitivity Group to GCs
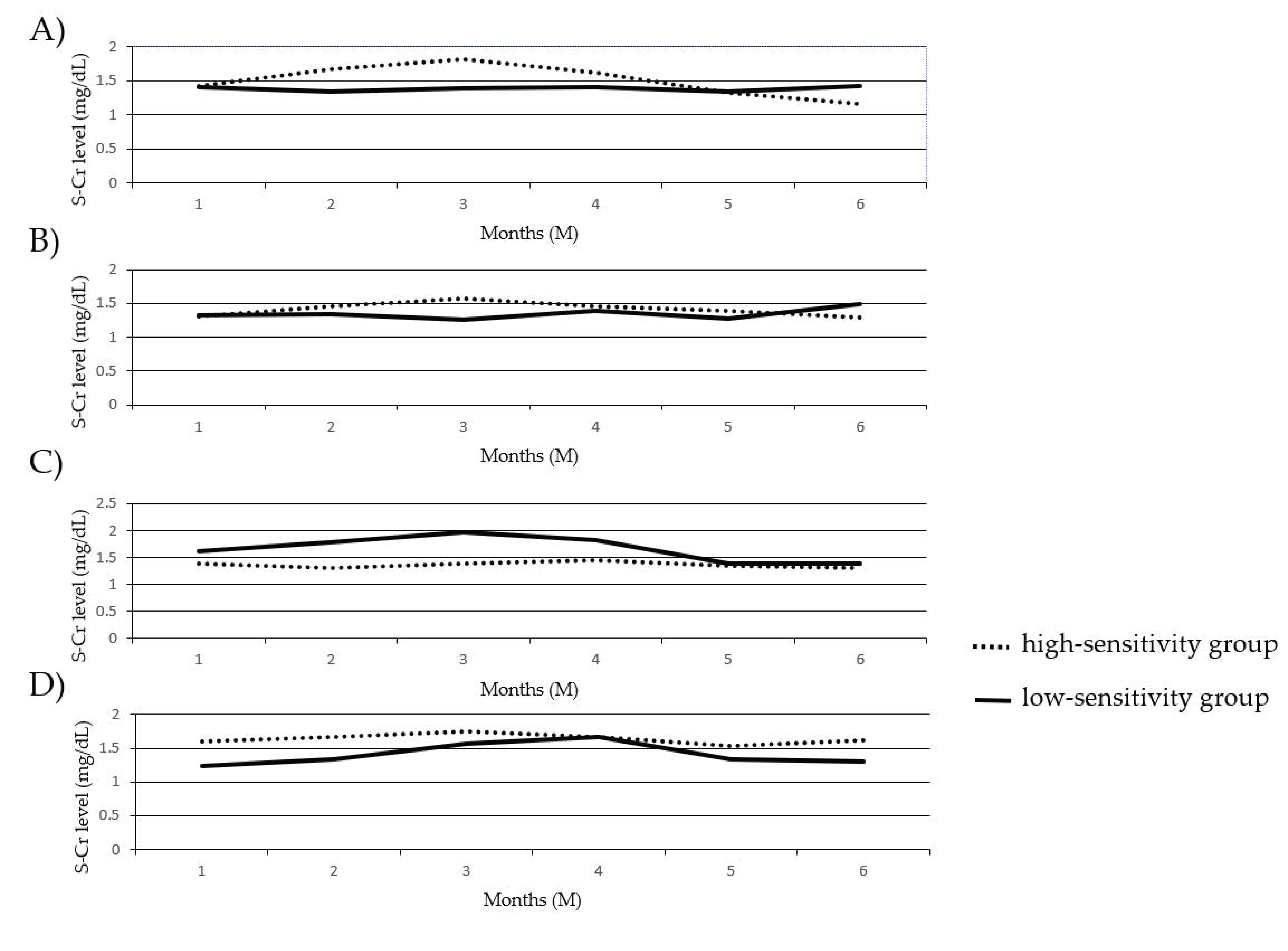
3.8. Comparison of the Change in S–Cr Levels between the PBMC High-Sensitivity Group and the PBMC Low-Sensitivity Group to GCs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Veenstra, D.L.; Best, J.H.; Hornberger, J.; Sulivan, S.D.; Hricik, D.E. Incidence and long-term cost of steroid-related side effects after renal transplantation. Am. J. Kidney Dis. 1999, 33, 829–839. [Google Scholar] [CrossRef]
- Zahir, N.; Mousa, D.; Taweel, A.A.; Ashrf, A.; Fahim, A.; Taqi, K.; Zahid, R.; Aslam, N. Prospective nonrandomized study with early steroid withdrawal (Day 5) postrenal transplant in low immunological risk patients: A singlecenter experience at prince sultan military medical city Riyadh. Saudi J. Kidney Dis. Transplant. 2019, 30, 1398–1406. [Google Scholar]
- Taber, D.J.; Hunt, K.J.; Gebregziabher, M.; Srinivas, T.; Chavin, K.D.; Baliga, P.K.; Egede, L.E. A Comparative Effectiveness Analysis of Early Steroid Withdrawal in Black Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2017, 12, 131–139. [Google Scholar] [CrossRef]
- Serrano, O.K.; Kandaswamy, R.; Gillingham, K.; Chinnakotla, S.; Dunn, T.B.; Finger, E.; Payne, W.; Ibrahim, H.; Kukla, A.; Spong, R.; et al. Rapid Discontinuation of prednisone in kidney transplant recipients: 15-year outcomes from the University of Minnesota. Transplantation 2017, 101, 2590–2598. [Google Scholar] [CrossRef]
- Soler, R.I.L.; Chan, R.; Martinolich, J.; Park, L.; Ata, A.; Chandolias, N.; Conti, D. Early steroid withdrawal results in improved patient and graft survival and lower risk of post-transplant cardiovascular risk profiles: A single-center 10-year experience. Clin. Transplant. 2017, 31, e12878. [Google Scholar] [CrossRef]
- Sierra, J.A.; Campos, E.R.; Munoz, E.C.; Carrillo, E.L.; Navarro, G.B.; Espinoza, G.E.; Lopez, L.O.; Gutierrez, C.J.; Perez, M.M.; Martinez, J.B.; et al. Early steroid withdrawal in recipients of a kidney transplant from a living donor: Experience of a single Mexican center. Transplant. Proc. 2016, 48, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Suszynski, T.M.; Gillingham, K.J.; Rizzari, M.D.; Dunn, T.B.; Payne, W.D.; Chinnakotla, S.; Finger, E.B.; Sutherland, D.E.R.; Najarian, J.S.; Prutt, T.L.; et al. Prospective randomized trial of maintenance immunosuppression with rapid discontinuation of prednisone in adult kidney transplantation. Am. J. Transplant. 2013, 13, 961–970. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Haller, M.C.; Kammer, M.; Kainz, A.; Baer, H.J.; Heinze, G.; Oberbauer, R. Steroid withdrawal after renal transplantation: A retorospective cohort study. BMC Med. 2017, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Haller, M.C.; Royuela, A.; Nagler, E.V.; Pascual, J.; Webster, A.C. Steroid avoidance or withdrawal for kidney transplant recipients. Cochrane Database Syst. Rev. 2016, 8, CD005632. [Google Scholar] [CrossRef]
- Pascual, J.; Quereda, C.; Zamora, J.; Hernandez, D. Steroid withdrawal in renal transplant patients on triple therapy with a calcineurin inhibitor and mycophenolate mofetil: A meta-analysis of randomized, controlled trials. Transplantation. 2004, 78, 1548–1556. [Google Scholar] [CrossRef]
- Hirano, T.; Oka, K.; Takeuchi, H.; Sakurai, E.; Kozaki, K.; Matsuno, N.; Kozaki, M.; Nagao, T. A comparison of prednisolone and methylprednisolone for renal transplantation. Clin. Transplant. 2000, 14, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Matsuno, N.; Hirano, T.; Gulimire, M.; Hama, K.; Nakamura, Y.; Iwamoto, H.; Toraishi, T.; Kawaguchi, T.; Okuyama, K.; et al. Steriod withdrawal based on lymphocyte sensitivity to Endogenous steroid in renal transplantation recipients. Biol. Pharm. Bull. 2011, 34, 1578–1583. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Haba, T.; Uchida, K.; Katayama, A.; Tominaga, Y.; Sato, T.; Watanabe, I.; Inagaki, H.; Kimata, T.; Goto, K.; Morozumi, K.; et al. Pharmacokinetics and pharmacodynamics of a chimeric interleukin-2 receptor monoclonal antibody, basiliximab, in renal taransplantation: A comparison between Japanese and non-Japanese patients. Transplant. Proc. 2001, 33, 3174–3175. [Google Scholar] [CrossRef]
- Leeaphorn, N.; Khankin, E.V.; Cardarelli, F.; Pavlakis, M. Recurrence of IgA nephropathy after kidney transplantation in steroid continuation versus early steroid-withdrawal regimens: A retrospective analysis of the UNOS/OPTN database. Transpl. Int. 2018, 2, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Kukla, A.; Chen, E.; Spong, R.; Weber, M.; Shahawi, Y.E.; Gillingham, K.; Matas, A.; Ibrahim, H.N. Recurrent Glomerulonephritis under rapid discontinuation of steroids. Transplantation 2011, 91, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- Leffell, M.S.; Steinberg, A.G.; Bias, W.B.; Machan, C.H.; Zachary, A.A. The distribution of HLA antigens and phenotypes among donors and patients in the UNOS registry. Transplantation 1994, 58, 1119–1130. [Google Scholar] [CrossRef]
- Kerman, R.H.; Kimball, P.M.; Buren, C.T.; Lewis, R.M.; Kahan, B.D. Possible contribution of pretransplant immune responder status to renal allograft survival differences of black versus white recipients. Transplantation 1991, 51, 338–342. [Google Scholar] [CrossRef]
- Liu, A.; Woodside, K.; Augustine, J.; Sarabu, N. Racial disparity in kidney transplant survival relates to late rejection and is dependent of steroid withdrawal. Clin. Transplant. 2018, 32, e13380. [Google Scholar] [CrossRef]
- Padiyar, A.; Augustine, J.J.; Bodziak, K.A.; Aeder, M.; Schulak, J.A.; Hricik, D.F. Influence of African-American ethnicity on acute rejection after early steroid withdrawal in primary kidney transplant recipients. Transplant. Proc. 2010, 42, 1643–1647. [Google Scholar] [CrossRef]
- Woodle, E.S.; First, M.R.; Pirsch, J.; Shihab, F.; Gaber, A.O.; Van Veldhuisen, P. Corticosteroid Withdrawal Study Group. A prospective, randomized, double-blind, placebo-controlled multicenter trial comparing early (7 day) corticosteroid cessation versus long-term, low-dose corticosteroid therapy. Ann. Surg. 2008, 248, 564–577. [Google Scholar] [CrossRef]
- Hricik, D.E.; Augustine, J.J.; Knauss, T.C.; Bodziak, K.A.; Aeder, M.; Siegel, C.; Schulak, J.A. Long-term graft outcomes after steroid withdrawal in African American kidney transplant recipients receiving sirolimus and tacrolimus. Transplantation 2007, 83, 277–281. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD or Number | |
|---|---|
| Age (yr) | 47.5 ± 12.0 |
| Male/female | 17/7 |
| Body weight (kg) | 62.3 ± 14.7 |
| First/second graft | 24/0 |
| Living related/cadaveric donor | 23/1 |
| ABO blood type compatible/incompatible | 22/2 |
| The number of HLA mismatches | 2.7 ± 1.1 |
| Immunosuppressive drugs | |
| G-Cs (MPSL/PSL) | 24/0 |
| CNI (CYA/TAC) | 14/10 |
| Antimetabolites (MMF/MIZ/AZ + MIZ) | 18/5/1 |
| Monoclonal antibody (Bx/Bx + Rx) | 22/2 |
| Time Point | GCs | The Clinical Event Groupthe IC50 Value (IC25, IC75) ng/mL | The Event-Free Groupthe IC50 Value (IC25, IC75) ng/mL | p-Value | ||
|---|---|---|---|---|---|---|
| Before transplantation | COR | 5758 (171, 11,727) | n = 13 | 93 (51, 358) | n = 9 | 0.042 |
| MPSL | 164.5 (12.0, 540.9) | n = 13 | 2.46 (2.2, 4.9) | n = 7 | 0.0049 | |
| After transplantation | COR | 620(55, 6349) | n = 13 | 62 (35, 524) | n = 6 | 0.19 |
| MPSL | 19.8 (5.9, 44.4) | n = 13 | 4.0 (0.1, 49.5) | n = 5 | 0.18 | |
| Time Point | GCs | The Clinical Event Group the IC50 Value (IC25, IC75) ng/mL | The Event-Free Group the IC50 Value (IC25, IC75) ng/mL | p-Value | ||
|---|---|---|---|---|---|---|
| Before transplantation | COR | 9529 (255, 12,884) | n = 9 | 93 (51, 495) | n = 11 | 0.011 |
| MPSL | 175.6 (44.4, 950.9) | n = 9 | 3.0 (2.3, 153.8) | n = 9 | 0.0071 | |
| After transplantation | COR | 620 (151, 8751) | n = 9 | 62 (26, 820) | n = 8 | 0.083 |
| MPSL | 19.8 (14.1, 305.3) | n = 9 | 4.0 (0.1, 29.1) | n = 7 | 0.08 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okihara, M.; Takeuchi, H.; Kikuchi, Y.; Akashi, I.; Kihara, Y.; Konno, O.; Iwamoto, H.; Oda, T.; Tanaka, S.; Unezaki, S.; et al. Individual Lymphocyte Sensitivity to Steroids as a Reliable Biomarker for Clinical Outcome after Steroid Withdrawal in Japanese Renal Transplantation. J. Clin. Med. 2021, 10, 1670. https://doi.org/10.3390/jcm10081670
Okihara M, Takeuchi H, Kikuchi Y, Akashi I, Kihara Y, Konno O, Iwamoto H, Oda T, Tanaka S, Unezaki S, et al. Individual Lymphocyte Sensitivity to Steroids as a Reliable Biomarker for Clinical Outcome after Steroid Withdrawal in Japanese Renal Transplantation. Journal of Clinical Medicine. 2021; 10(8):1670. https://doi.org/10.3390/jcm10081670
Chicago/Turabian StyleOkihara, Masaaki, Hironori Takeuchi, Yukiko Kikuchi, Isao Akashi, Yu Kihara, Osamu Konno, Hitoshi Iwamoto, Takashi Oda, Sachiko Tanaka, Sakae Unezaki, and et al. 2021. "Individual Lymphocyte Sensitivity to Steroids as a Reliable Biomarker for Clinical Outcome after Steroid Withdrawal in Japanese Renal Transplantation" Journal of Clinical Medicine 10, no. 8: 1670. https://doi.org/10.3390/jcm10081670
APA StyleOkihara, M., Takeuchi, H., Kikuchi, Y., Akashi, I., Kihara, Y., Konno, O., Iwamoto, H., Oda, T., Tanaka, S., Unezaki, S., & Hirano, T. (2021). Individual Lymphocyte Sensitivity to Steroids as a Reliable Biomarker for Clinical Outcome after Steroid Withdrawal in Japanese Renal Transplantation. Journal of Clinical Medicine, 10(8), 1670. https://doi.org/10.3390/jcm10081670