
Endurance Training Depletes Antioxidant System but Does Not Affect Endothelial Functions in Women with Abdominal Obesity: A Randomized Trial with a Comparison to Endurance-Strength Training

 ,
,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Issues
2.2. Study Population
2.3. Intervention
2.4. Study Outcomes
2.5. Graded Exercise Test (GXT)
2.6. Blood Pressure
2.7. Anthropometry Parameters and Body Composition
2.8. Arterial Stiffness
2.9. Biochemical Measurements
2.10. Randomization
2.11. Sample Size Calculation
2.12. Statistical Analysis
3. Results
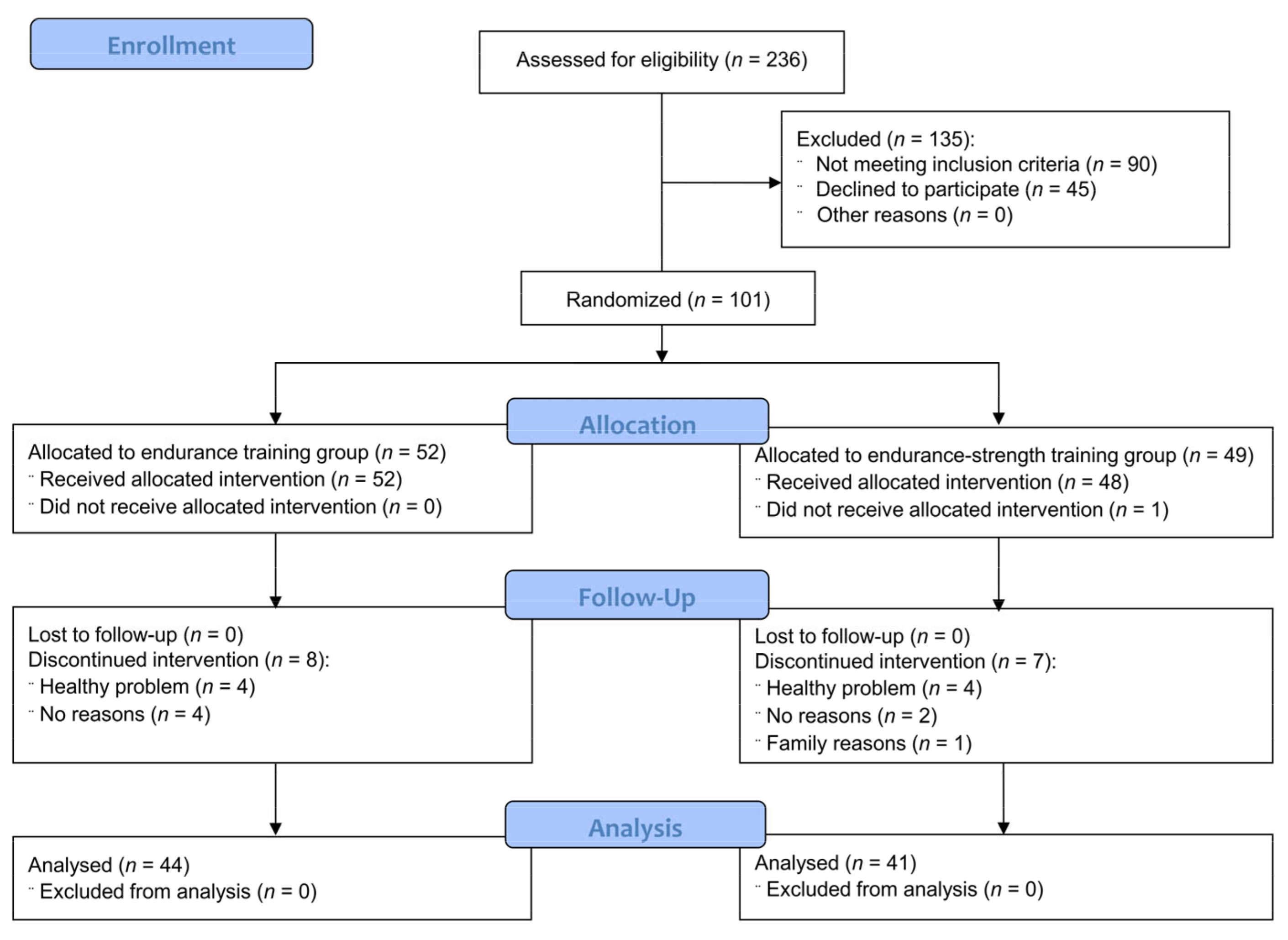
3.1. Participants Flow
3.2. Effects of Endurance and Endurance-Strength Training on Anthropometric Parameters, Endothelial Function, Arterial Stiffness, Antioxidant Status and Inflammatory Markers
3.3. Comparison of the Effect of Endurance and Endurance-Strength Training on Anthropometric Parameters, Endothelial Function, Arterial Stiffness, Antioxidant Status and Inflammatory Markers
3.4. Correlation between BMI and Changes in the Main Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, S.-Y.; Chang, H.-J.; Sung, J.; Kim, K.J.; Shin, S.; Cho, I.-J.; Shim, C.Y.; Hong, G.R.; Chung, N. The impact of obesity on subclinical coronary atherosclerosis according to the risk of cardiovascular disease. Obesity 2014, 22, 1762–1768. [Google Scholar] [CrossRef] [PubMed]
- Roever, L.S.; Resende, E.S.; Diniz, A.L.D.; Penha-Silva, N.; Veloso, F.C.; Casella-Filho, A.; Dourado, P.M.; Chagas, A.C. Abdominal obesity and association with atherosclerosis risk factors: The Uberlândia heart study. Medicine (Baltimore) 2016, 95, e1357. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Shimokawa, H.; Tang, E.H.C.; Feletou, M. Endothelial dysfunction and vascular disease. Acta Physiol. 2009, 196, 193–222. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, Y.; Lerman, A. Endothelial dysfunction and coronary artery disease: Assessment, prognosis, and treatment. Coron. Artery Dis. 2014, 25, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Widmer, J.R.; Lerman, A. Endothelial dysfunction and cardiovascular disease. Glob. Cardiol. Sci. Pract. 2014, 2014, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Kwaifa, I.K.; Bahari, H.; Yong, Y.K.; Noor, S.M. Endothelial dysfunction in obesity-induced inflammation: Molecular mechanisms and clinical implications. Biomolecules 2020, 10, 291. [Google Scholar] [CrossRef]
- Stanhewicz, A.E.; Wenner, M.M.; Stachenfeld, N.S. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1569–H1588. [Google Scholar] [CrossRef] [PubMed]
- Holder, S.M.; Brislane, Á.; Dawson, E.A.; Hopkins, N.D.; Hopman, M.T.E.; Cable, N.T.; Jones, H.; Schreuder, T.H.A.; Sprung, V.S.; Naylor, L.; et al. Relationship between endothelial function and the eliciting shear stress stimulus in women: Changes across the lifespan differ to men. J. Am. Heart Assoc. 2019, 8, e010994. [Google Scholar] [CrossRef]
- Suboc, T.M.; Dharmashankar, K.; Wang, J.; Ying, R.; Couillard, A.; Tanner, M.J.; Widlansky, M.E. Moderate obesity and endothelial dysfunction in humans: Influence of gender and systemic inflammation. Physiol. Rep. 2013, 1, e00058. [Google Scholar] [CrossRef]
- Seals, D.R.; Jablonski, K.L.; Donato, A.J. Aging and vascular endothelial function in humans. Clin. Sci. (Lond.) 2011, 120, 357–375. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Spiegelhalter, D.J.; Georgakopoulos, D.; Robinson, J.; Deanfield, J.E. Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women. J. Am. Coll. Cardiol. 1994, 2, 471–476. [Google Scholar] [CrossRef]
- Moreau, K.L.; Hildreth, K.L.; Meditz, A.L.; Deane, K.D.; Kohrt, W.M. Endothelial function is impaired across the stages of the menopause transition in healthy women. J. Clin. Endocrinol. Metab. 2012, 97, 4692–4700. [Google Scholar] [CrossRef]
- Storch, A.S.; Mattos, J.D.; Alves, R.; Galdino, I.S.; Rocha, H.N.M. Methods of endothelial function assessment: Description and applications. Int. J. Cardiovasc. Sci. 2017, 30, 262–273. [Google Scholar] [CrossRef]
- Al-Qaisi, M.; Kharbanda, R.K.; Mittal, T.K.; Donald, A.E. Measurement of endothelial function and its clinical utility for cardiovascular risk. Vasc. Health Risk Manag. 2008, 4, 647–652. [Google Scholar] [CrossRef]
- Leung, F.P.; Yung, L.M.; Laher, I.; Yao, X.; Chen, Z.Y.; Huang, Y. Exercise, vascular wall and cardiovascular diseases: An update (Part 1). Sports Med. 2008, 38, 1009–1024. [Google Scholar] [CrossRef]
- Rush, J.W.E.; Ford, R.J. Nitric oxide, oxidative stress and vascular endothelium in health and hypertension. Clin. Hemorheol. Microcirc. 2007, 37, 185–192. [Google Scholar]
- Abramson, J.L.; Vaccarino, V. Relationship between physical activity and inflammation among apparently healthy middle-aged and older US adults. Arch. Intern. Med. 2002, 162, 1286–1292. [Google Scholar] [CrossRef]
- Roberts, C.K.; Chen, A.K.; Barnard, R.J. Effect of a short-term diet and exercise intervention in youth on atherosclerotic risk factors. Atherosclerosis 2007, 191, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Duncker, D.J.; Bache, R.J. Regulation of coronary blood flow during exercise. Physiol. Rev. 2008, 88, 1009–1086. [Google Scholar] [CrossRef] [PubMed]
- Hilberg, T. Physical activity in the prevention of cardiovascular diseases. Epidemiology and mechanisms. Hamostaseologie 2008, 28, 9–12. [Google Scholar] [PubMed]
- Lippincott, M.F.; Desai, A.; Zalos, G.; Carlow, A.; De Jesus, J.; Blum, A.; Smith, K.; Rodrigo, M.; Patibandla, S.; Chaudhry, H.; et al. Predictors of endothelial function in employees with sedentary occupations in a worksite exercise program. Am. J. Cardiol. 2008, 102, 820–824. [Google Scholar] [CrossRef][Green Version]
- Fries, J.F. Measuring and monitoring success in compressing morbidity. Ann. Intern. Med. 2003, 139, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Penumetcha, M.; Santanam, N.; Liu, Y.-G.; Garelnabi, M.; Parthasarathy, S. Exercise might favor reverse cholesterol transport and lipoprotein clearance: Potential mechanism for its anti-atherosclerotic effects. Biochim. Biophys. Acta 2005, 1723, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Rahimianmashhad, Z.; Hosseini, S.R.A.; Rashidlamir, A.; Sardar, M.A.; Nekooei, S.; Giti, R. Comparison of the effects of aerobic and resistance exercises on arterial stiffness, endothelial function, carotid intima-media thickness, and inflammatory biomarkers in obese sedentary females. Int. Cardiovasc. Res. J. 2020, 14, 18–23. [Google Scholar]
- Ratajczak, M.; Skrypnik, D.; Bogdański, P.; Mądry, E.; Walkowiak, J.; Szulińska, M.; Maciaszek, J.; Kręgielska-Narożna, M.; Karolkiewicz, J. Effects of endurance and endurance-strength training on endothelial function in women with obesity: A randomized trial. Int. J. Environ. Res. Public Health 2019, 16, 4291. [Google Scholar] [CrossRef] [PubMed]
- Schjerve, I.E.; Tyldum, G.A.; Tjønna, A.E.; Stølen, T.; Loennechen, J.P.; Hansen, H.E.; Haram, P.M.; Heinrich, G.; Bye, A.; Najjar, S.M.; et al. Both aerobic endurance and strength training programmes improve cardiovascular health in obese adults. Clin. Sci. 2008, 115, 283–293. [Google Scholar] [CrossRef]
- Stensvold, D.; Tjønna, A.E.; Skaug, E.A.; Aspenes, S.; Stølen, T.; Wisløff, U.; Slørdahl, S.A. Strength training versus aerobic interval training to modify risk factors of metabolic syndrome. J. Appl. Physiol. 2010, 108, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Thomson, R.L.; Brinkworth, G.D.; Noakes, M.; Clifton, P.M.; Norman, R.J.; Buckley, J.D. The effect of diet and exercise on markers of endothelial function in overweight and obese women with polycystic ovary syndrome. Hum. Reprod. 2012, 27, 2169–2176. [Google Scholar] [CrossRef]
- Black, M.A.; Cable, N.T.; Thijssen, D.H.; Green, D.J. Impact of age, sex, and exercise on brachial artery flow-mediated dilatation. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H1109–H1116. [Google Scholar] [CrossRef]
- Green, D.J.; Swart, A.; Exterkate, A.; Naylor, L.H.; Black, M.A.; Cable, N.T.; Thijssen, D.H. Impact of age, sex and exercise on brachial and popliteal artery remodelling in humans. Atherosclerosis 2010, 210, 525–530. [Google Scholar] [CrossRef]
- Pierce, G.L.; Eskurza, I.; Walker, A.E.; Fay, T.N.; Seals, D.R. Sex-specific effects of habitual aerobic exercise on brachial artery flow-mediated dilation in middle-aged and older adults. Clin. Sci. (Lond.) 2011, 120, 13–23. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- DRKS—Deutsches Register Klinischer Studien (German Clinical Trials Register). Comparison of the Effects of Endurance and Endurance-Strength Training on the Endothelial Dysfunction in Women with Abdominal Obesity. DRKS-ID: DRKS00019832. Available online: https://www.drks.de/drks_web/setLocale_EN.do (accessed on 30 June 2020).
- American Council on Exercise. What Are the Guidelines for Percentage of Body Fat Loss? Ask the Expert Blog. Available online: https://www.acefitness.org/education-and-resources/lifestyle/blog/112/what-are-the-guidelines-for-percentage-of-body-fat-loss/ (accessed on 2 February 2021).
- Jamka, M.; Bogdański, P.; Krzyżanowska-Jankowska, P.; Karolkiewicz, J.; Mądry, R.; Lisowska, A.; Walkowiak, J.; Mądry, E. Comparison of the effects of endurance and endurance-strength training programmes on the level of endothelial dysfunction in women with abdominal obesity: Study protocol for a randomised controlled trial. J. Med. Sci. 2020, 88, 266–272. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Palatini, P.; Parati, G.; O’Brien, E.; Januszewicz, A.; Lurbe, E.; Persu, A.; Mancia, G.; Kreutz, R.; European Society of Hypertension Council and the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J. Hypertens. 2021. [Google Scholar] [CrossRef]
- World Health Organization. Global Database on Body Mass Index. Available online: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html (accessed on 7 January 2017).
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Tsikas, D. Simultaneous derivatization and quantification of the nitric oxide metabolites nitrite and nitrate in biological fluids by gas chromatography/mass spectrometry. Anal. Chem. 2000, 72, 4064–4072. [Google Scholar] [CrossRef] [PubMed]
- Skrypnik, D.; Bogdański, P.; Mądry, E.; Karolkiewicz, J.; Ratajczak, M.; Kryściak, J.; Pupek-Musialik, D.; Walkowiak, J. Effects of endurance and endurance strength training on body composition and physical capacity in women with abdominal obesity. Obes. Facts. 2015, 8, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Sanal, E.; Ardic, F.; Kirac, S. Effects of aerobic or combined aerobic resistance exercise on body composition in overweight and obese adults: Gender differences. A randomized intervention study. Eur. J. Phys. Rehabil. Med. 2013, 49, 1–11. [Google Scholar] [PubMed]
- AbouAssi, H.; Slentz, C.A.; Mikus, C.R.; Tanner, C.J.; Bateman, L.A.; Willis, L.H.; Shields, A.T.; Piner, L.W.; Penry, L.E.; Kraus, E.A.; et al. The effects of aerobic, resistance, and combination training on insulin sensitivity and secretion in overweight adults from STRRIDE AT/RT: A randomized trial. J. Appl. Physiol. 2015, 118, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.S.; Dhaliwal, S.S.; Hills, A.P.; Pal. S. The effect of 12 weeks of aerobic, resistance or combination exercise training on cardiovascular risk factors in the overweight and obese in a randomized trial. BMC Public Health 2012, 12, 704. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Dias, S.; Strasser, B.; Hoffmann, G. Impact of different training modalities on anthropometric and metabolic characteristics in overweight/obese subjects: A systematic review and network meta-analysis. PLoS ONE 2013, 8, e82853. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hill, J.O.; Jacobsen, D.J.; Potteiger, J.; Sullivan, D.K.; Johnson, S.L.; Heelan, K.; Hise, M.; Fennessey, P.V.; Sonko, B.; et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: The Midwest Exercise Trial. Arch. Intern. Med. 2003, 163, 1343–1350. [Google Scholar] [CrossRef]
- Geer, E.B.; Shen, W. Gender differences in insulin resistance, body composition, and energy balance. Gend. Med. 2009, 6 (Suppl. 1), 60–75. [Google Scholar] [CrossRef]
- Beck, D.T.; Martin, J.S.; Casey, D.P.; Braith, R.W. Exercise training improves endothelial function in resistance arteries of young prehypertensives. J. Hum. Hypertens. 2014, 28, 303–309. [Google Scholar] [CrossRef]
- Cohen, N.D.; Dunstan, D.W.; Robinson, C.; Vulikh, E.; Zimmet, P.Z.; Shaw, J.E. Improved endothelial function following a 14-month resistance exercise training program in adults with type 2 diabetes. Diabetes Res. Clin. Pract. 2008, 79, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.G.; Schofield, R.S.; Lennon, S.L.; Pierce, G.L.; Nichols, W.W.; Braith, R.W. Effect of exercise training on endothelial function in men with coronary artery disease. Am. J. Cardiol. 2004, 93, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Di Francescomarino, S.; Sciartilli, A.; Di Valerio, V.; Di Baldassarre, A.; Gallina, S. The effect of physical exercise on endothelial function. Sport Med. 2009, 39, 797–812. [Google Scholar] [CrossRef]
- Fuchsjäger-Mayrl, G.; Pleiner, J.; Wiesinger, G.F.; Sieder, A.E.; Quittan, M.; Nuhr, M.J.; Francesconi, C.; Seit, H.P.; Francesconi, M.; Schmetterer, L.; et al. Exercise training improves vascular endothelial function in patients with type 1 diabetes. Diabetes Care 2002, 25, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Olson, T.P.; Dengel, D.R.; Leon, A.S.; Schmitz, K.H. Moderate resistance training and vascular health in overweight women. Med. Sci. Sport Exerc. 2006, 38, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Østergård, T.; Nyholm, B.; Hansen, T.K.; Rasmussen, L.M.; Ingerslev, J.; Sørensen, K.E.; Bøtker, H.E.; Saltin, B.; Schmitz, O. Endothelial function and biochemical vascular markers in first-degree relatives of type 2 diabetic patients: The effect of exercise training. Metabolism 2006, 55, 1508–1515. [Google Scholar] [CrossRef]
- Kwon, H.R.; Min, K.W.; Ahn, H.J.; Seok, H.G.; Lee, J.H.; Park, G.S.; Han, K.A. Effects of aerobic exercise vs. resistance training on endothelial function in women with type 2 diabetes mellitus. Diabetes Metab. J. 2001, 35, 364–373. [Google Scholar] [CrossRef]
- Chia, P.Y.; Teo, A.; Yeo, T.W. Overview of the assessment of endothelial function in humans. Front. Med. (Lausanne) 2020, 7, 542567. [Google Scholar] [CrossRef] [PubMed]
- Alexander, Y.; Osto, E.; Schmidt-Trucksäss, A.; Shechter, M.; Trifunovic, D.; Duncker, D.J.; Aboyans, V.; Bäck, M.; Badimon, L.; Cosentino, F.; et al. Endothelial function in cardiovascular medicine: A consensus paper of the European Society of Cardiology Working Groups on Atherosclerosis and Vascular Biology, Aorta and Peripheral Vascular Diseases, Coronary Pathophysiology and Microcirculation, and Thrombosis. Cardiovasc. Res. 2021, 117, 29–42. [Google Scholar] [CrossRef] [PubMed]
- McClean, C.; Harris, R.A.; Brown, M.; Brown, J.C.; Davison, G.W. Effects of exercise intensity on postexercise endothelial function and oxidative stress. Oxid. Med. Cell Longev. 2015, 2015, 723679. [Google Scholar] [CrossRef]
- Palmefors, H.; DuttaRoy, S.; Rundqvist, B.; Börjesson, M. The effect of physical activity or exercise on key biomarkers in atherosclerosis—A systematic review. Atherosclerosis 2014, 235, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Montero, D.; Vinet, A.; Roberts, C.K. Effect of combined aerobic and resistance training versus aerobic training on arterial stiffness. Int. J. Cardiol. 2015, 178, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Bohn, L.; Ramoa, A.; Silva, G.; Silva, N.; Abreu, S.M.; Ribeiro, F.; Boutouyrie, P.; Laurent, S.; Oliveira, J. Sedentary behavior and arterial stiffness in adults with and without metabolic syndrome. Int. J. Sports Med. 2017, 38, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Masuhara, M.; Ikuta, K. Home-based resistance training improves arterial stiffness in healthy premenopausal women. Eur. J. Appl. Physiol. 2009, 107, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Park, S.Y.; Seo, D.Y.; Sanchez-Gonzalez, M.A.; Baek, Y.H. Combined resistance and endurance exercise training improves arterial stiffness, blood pressure, and muscle strength in postmenopausal women. Menopause 2011, 18, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Zaydun, G.; Tomiyama, H.; Hashimoto, H.; Arai, T.; Koji, Y.; Yambe, M.; Motobe, K.; Hori, S.; Yamashina, A. Menopause is an independent factor augmenting the age-related increase in arterial stiffness in the early postmenopausal phase. Atherosclerosis 2006, 184, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Onur, E.; Kabaroğlu, C.; Günay, Ö.; Var, A.; Yilmaz, Ö.; Dündar, P.; Tikiz, C.; Güvenç, Y.; Yüksel, H. The beneficial effects of physical exercise on antioxidant status in asthmatic children. Allergol. Immunopathol. (Madr.) 2011, 39, 90–95. [Google Scholar] [CrossRef]
- Simioni, C.; Zauli, G.; Martelli, A.M.; Vitale, M.; Sacchetti, G.; Gonelli, A.; Neri, L.M. Oxidative stress: Role of physical exercise and antioxidant nutraceuticals in adulthood and aging. Oncotarget 2018, 9, 17181–17198. [Google Scholar] [CrossRef]
- Leeuwenburgh, C.; Heinecke, J.W. Oxidative stress and antioxidants in exercise. Curr. Med. Chem. 2001, 8, 829–838. [Google Scholar] [CrossRef]
- Fisher-Wellman, K.; Bloomer, R.J. Acute exercise and oxidative stress: A 30 year history. Dyn. Med. 2009, 8, 1. [Google Scholar] [CrossRef]
- De Oliveira, V.N.; Bessa, A.; Jorge, M.L.M.P.; da Silva Oliveira, R.J.; de Mello, M.T.; De Agostini, G.G.; Jorge, P.T.; Espindola, F.S. The effect of different training programs on antioxidant status, oxidative stress, and metabolic control in type 2 diabetes. Appl. Physiol. Nutr. Metab. 2012, 37, 334–344. [Google Scholar] [CrossRef]
- Azizbeigi, K.; Stannard, S.R.; Atashak, S.; Mosalman Haghighi, M. Antioxidant enzymes and oxidative stress adaptation to exercise training: Comparison of endurance, resistance, and concurrent training in untrained males. J. Exerc. Sci. Fit. 2014, 12, 1–6. [Google Scholar] [CrossRef]
- García-López, D.; Häkkinen, K.; Cuevas, M.J.; Lima, E.; Kauhanen, A.; Mattila, M.; Sillanpää, E.; Ahtiainen, J.P.; Karavirta, L.; Almar, M.; et al. Effects of strength and endurance training on antioxidant enzyme gene expression and activity in middle-aged men. Scand. J. Med. Sci. Sports 2007, 17, 595–604. [Google Scholar] [CrossRef]
- Linke, A.; Adams, V.; Schulze, P.C.; Erbs, S.; Gielen, S.; Fiehn, E.; Möbius-Winkler, S.; Schubert, A.; Schuler, G.; Hambrecht, R. Antioxidative effects of exercise training in patients with chronic heart failure: Increase in radical scavenger enzyme activity in skeletal muscle. Circulation 2005, 111, 1763–1770. [Google Scholar] [CrossRef] [PubMed]
- Kolesnikova, L.; Semenova, N.; Madaeva, I.; Suturina, L.; Solodova, E.; Grebenkina, L.; Darenskaya, M. Antioxidant status in peri- and postmenopausal women. Maturitas 2015, 81, 83–87. [Google Scholar] [CrossRef]
- Giannopoulou, I.; Fernhall, B.; Carhart, R.; Weinstock, R.S.; Baynard, T.; Figueroa, A.; Kanaley, J.A. Effects of diet and/or exercise on the adipocytokine and inflammatory cytokine levels of postmenopausal women with type 2 diabetes. Metabolism 2005, 54, 866–875. [Google Scholar] [CrossRef]
- Jorge, M.L.M.P.; de Oliveira, V.N.; Resende, N.M.; Paraiso, L.F.; Calixto, A.; Diniz, A.L.D.; Resende, E.S.; Ropelle, E.R.; Carvalheira, J.B.; Espindola, F.S.; et al. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adipocytokines, and muscle insulin signaling in patients with type 2 diabetes mellitus. Metabolism 2011, 60, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Libardi, C.A.; de Souza, G.V.; Cavaglieri, C.R.; Madruga, V.A.; Chacon-Mikahil, M.P.T. Effect of resistance, endurance, and concurrent training on TNF-α, IL-6, and CRP. Med. Sci. Sports Exerc. 2012, 44, 50–56. [Google Scholar] [CrossRef]
- Trøseid, M.; Lappegård, K.T.; Claudi, T.; Damås, J.K.; Mørkrid, L.; Brendberg, R.; Mollnes, T.E. Exercise reduces plasma levels of the chemokines MCP-1 and IL-8 in subjects with the metabolic syndrome. Eur. Heart J. 2004, 25, 349–355. [Google Scholar] [CrossRef]
- Adamopoulos, S.; Parissis, J.; Kroupis, C.; Georgiadis, M.; Karatzas, D.; Karavolias, G.; Koniavitou, K.; Coats, A.J.; Kremastinos, D.T. Physical training reduces peripheral markers of inflammation in patients with chronic heart failure. Eur. Heart J. 2001, 22, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Nakaji, S.; Yamada, M.; Totsuka, M.; Sato, K.; Sugawara, K. Systemic inflammatory response to exhaustive exercise. Cytokine kinetics. Exerc. Immunol. Rev. 2002, 8, 6–48. [Google Scholar] [PubMed]
- Nascimento, D.D.C.; Durigan, R.D.C.M.; Tibana, R.A.; Durigan, J.L.Q.; Navalta, J.W.; Prestes, J. The Response of Matrix Metalloproteinase-9 and -2 to Exercise. Sports Med. 2014, 45, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Rullman, E.; Norrbom, J.; Strömberg, A.; Wågsäter, D.; Rundqvist, H.; Haas, T.; Gustafsson, T. Endurance exercise activates matrix metalloproteinases in human skeletal muscle. J. Appl. Physiol. 2009, 106, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Scheede-Bergdahl, C.; Bergdahl, A.; Schjerling, P.; Qvortrup, K.; Koskinen, S.O.; Dela, F. Exercise-induced regulation of matrix metalloproteinases in the skeletal muscle of subjects with type 2 diabetes. Diabetes Vasc. Dis. Res. 2014, 11, 324–334. [Google Scholar] [CrossRef]
- Souza, M.V.; Leite, R.D.; Souza Lino, A.D.; Marqueti, R.D.C.; Bernardes, C.F.; Araújo, H.S.; Bouskela, E.; Shiguemoto, G.E.; Andrade Perez, S.E.; Kraemer-Aguiar, L.G. Resistance training improves body composition and increases matrix metalloproteinase 2 activity in biceps and gastrocnemius muscles of diet-induced obese rats. Clinics (Sao Paulo) 2014, 69, 265–270. [Google Scholar] [CrossRef]
- Shon, S.-M.; Park, J.-H.; Nahrendorf, M.; Schellingerhout, D.; Kim, J.-Y.; Kang, B.-T.; Jeong, S.W.; Kim, E.J.; Ryu, J.H.; Kim, K.; et al. Exercise attenuates matrix metalloproteinase activity in preexisting atherosclerotic plaque. Atherosclerosis 2011, 216, 67–73. [Google Scholar] [CrossRef]
- Rullman, E.; Rundqvist, H.; Wågsäter, D.; Fischer, H.; Eriksson, P.; Sundberg, C.J.; Jansson, E.; Gustafsson, T. A single bout of exercise activates matrix metalloproteinase in human skeletal muscle. J. Appl. Physiol. 2007, 102, 2346–2351. [Google Scholar] [CrossRef]
- Lu, Y.; Zhou, S.; Dreyer, R.P.; Spatz, E.S.; Geda, M.; Lorenze, N.P.; D’Onofrio, G.; Lichtman, J.H.; Spertus, J.A.; Ridker, P.M.; et al. Sex differences in inflammatory markers and health status among young adults with acute myocardial infarction: Results from the VIRGO (Variation in Recovery: Role of Gender on Outcomes of Young Acute Myocardial Infarction Patients) study. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003470. [Google Scholar] [CrossRef]
- Cartier, A.; Côté, M.; Lemieux, I.; Pérusse, L.; Tremblay, A.; Bouchard, C.; Després, J.P. Sex differences in inflammatory markers: What is the contribution of visceral adiposity? Am. J. Clin. Nutr. 2009, 89, 1307–1314. [Google Scholar] [CrossRef]
- Woo, J.S.; Derleth, C.; Stratton, J.R.; Levy, W.C. The influence of age, gender, and training on exercise efficiency. J. Am. Coll. Cardiol. 2006, 47, 1049–1057. [Google Scholar] [CrossRef]


{kind=link}
| Endurance Training (n = 52) | Endurance-Strength Training (n = 49) | p | |||
|---|---|---|---|---|---|
| Mean ± SD (95% CI) | Median (Q1–Q3) | Mean ± SD (95% CI) | Median (Q1–Q3) | ||
| Anthropometric parameter | |||||
| Age (years) | 55 ± 7 (53–57) | 55 (50–60) | 55 ± 7 (53–58) | 54 (50–60) | 0.84 |
| Weight (kg) | 96.0 ± 15.1 (91.7–100.2) | 93.4 (84.9–104.9) | 93.2 ± 13.9 (89.2–97.2) | 91.0 (82.4–101.8) | 0.41 |
| BMI (kg/m2) | 35.87 ± 4.43 (34.63–37.10) | 35.64 (32.07–38.00) | 35.98 ± 5.10 (34.52–37.45) | 35.42 (31.79–39.10) | 0.86 |
| Waist circumference (cm) | 110 ± 10 (107–113) | 109 (103–114) | 110 ± 10 (107–113) | 108 (103–117) | 1.00 |
| Endothelial function parameters | |||||
| ADMA (nmol/mL) | 1.66 ± 1.47 (1.25–2.07) | 0.98 (0.44–2.90) | 1.38 ± 1.35 (0.99–1.77) | 0.59 (0.40–2.26) | 0.25 |
| eNOS (U/L) | 29.19 ± 28.03 (21.39–37.00) | 20.97 (14.17–32.73) | 24.86 ± 23.18 (18.21–31.52) | 18.76 (14.43–27.23) | 0.75 |
| HCY (µmmol/L) | 10.86 ± 2.73 (10.10–11.62) | 11.03 (9.12–12.46) | 10.70 ± 2.87 (9.87–11.52) | 10.21 (8.94–11.61) | 0.26 |
| NO2 (µmol/L) | 1.42 ± 0.28 (1.34–1.39) | 1.36 (1.19–1.66) | 1.40 ± 0.30 (1.31–1.48) | 1.38 (1.22–1.55) | 0.66 |
| NO3 (µmol/L) | 36.69 ± 17.70 (31.76–41.61) | 31.37 (24.59–43.69) | 36.44 ± 16.04 (31.84–41.05) | 31.98 (27.22–40.49) | 0.58 |
| PAI-1 (ng/mL) | 118.9 ± 33.0 (109.7–128.1) | 119.6 (91.5–134.7) | 119.1 ± 40.5 (107.5–130.7) | 115.0 (86.0–141.0) | 0.97 |
| sVCAM-1 (ng/mL) | 808.95 ± 203.90 (752.19–865.72) | 750.00 (685.50–872.45) | 808.42 ± 257.65 (734.41–882.42) | 764.70 (651.00–876.00) | 0.92 |
| VEGF (pg/mL) | 485 ± 278 (408–563) | 436 (266–601) | 471 ± 258 (397.36–545.54) | 431 (239–638) | 0.80 |
| Arterial stiffness | |||||
| PWA SP (mmHg) | 129 ± 12 (126–133) | 129 (120–138) | 131 ± 17 (126–136) | 130 (122–138) | 0.88 |
| PWA PP (mmHg) | 42 ± 11 (39–45) | 31 (37–47) | 44 ± 14 (39–48) | 42 (35–51) | 0.76 |
| PWA AIx | 31 ± 14 (27–35) | 30 (22–36) | 30 ± 14 (26–34) | 30 (19–39) | 1.00 |
| PWA AP (mmHg) | 13 ± 6 (12–15) | 13 (9–18) | 134 ± 8 (11–20) | 13 (7–19) | 0.99 |
| PWV (m/s) | 7.1 ± 1.2 (6.8–7.5) | 7.0 (6.3–7.9) | 6.7 ± 1.2 (6.4–7.1) | 6.5 (5.8–7.5) | 0.08 |
| Antioxidant status parameters | |||||
| GSH (µmol/L) | 20.60 ± 25.97 (13.37–27.83) | 13.22 (9.69–23.14) | 24.83 ± 72.27 (4.01–45.64) | 11.47 (6.69–20.54) | 0.44 |
| SOD (U/mL) | 3.44 ± 2.03 (2.87–4.00) | 3.48 (1.75–4.31) | 3.12 ± 1.24 (2.76–3.47) | 2.92 (2.13–4.19) | 0.42 |
| TAS (ng/mL) | 674 ± 865 (433–915) | 242 (184–675) | 577 ± 809 (346–810) | 195 (166–370) | 0.35 |
| Inflammatory markers | |||||
| hs-CRP (mg/L) | 3.99 ± 3.97 (2.88–5.09) | 2.95 (1.10–5.35) | 4.16 ± 4.08 (2.99–5.33) | 2.30 (1.70–4.80) | 0.95 |
| hs-IL-6 (pg/mL) | 2.32 ± 2.07 (1.75–2.90) | 1.85 (1.22–2.58) | 2.05 ± 1.52 (1.61–2.48) | 1.57 (1.33–2.31) | 0.45 |
| hs-IL-8 (pg/mL) | 33.80 ± 26.17 (26.51–41.09) | 23.52 (18.60–42.94) | 31.61 ± 33.34 (22.03–41.18) | 22.45 (13.01–34.27) | 0.39 |
| MCP-1 (pg/mL) | 415.51 ± 189.20 (362.83–468.18) | 402.55 (296.80–532.85) | 416.42 ± 165.19 (368.97–463.87)) | 367.85 (298.05–495.35) | 0.91 |
| MMP-2 (ng/mL) | 209.30 ± 48.38 (195.83–222.77) | 203.37 (177.00–236.74) | 207.60 ± 54.71 (191.89–223.32) | 201.00 (176.54–231.72) | 0.38 |
| MMP-9 (ng/mL) | 746.7 ± 292.9 (665.1–828.2) | 736.3 (522.1–936.0) | 767.3 ± 412.3 (648.9–885.7) | 682.7 (467.6–841.5) | 0.86 |
| TNF-α (pg/mL) | 43 ± 55 (27–58) | 15 (11–46) | 33 ± 46 (19–46) | 12 (10–19) | 0.30 |
| Endurance Training (n = 44) | p | Endurance-Strength Training (n = 41) | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | |||||||
| Mean ± SD (95% CI) | Median (Q1–Q3) | Mean ± SD (95% CI) | Median (Q1–Q3) | Mean ± SD (95% CI) | Median (Q1–Q3) | Mean ± SD (95% CI) | Median (Q1–Q3) | |||
| Anthropometric parameter | ||||||||||
| Weight (kg) | 94.6 ± 14.8 (90.1–99.1) | 90.4 (83.6–101.7) | 93.4 ± 14.5 (89.0–97.8) | 90.1 (82.1–99.3) | <0.001 | 93.3 ± 13.4 (89.1–97.5) | 93.1 (82.4–101.8) | 92.1 ± 13.9 (87.8–96.5) | 90.7 (82.1–102.7) | 0.03 |
| BMI (kg/m2) | 35.45 ± 4.51 (34.07–36.82) | 34.41 (31.63–37.46) | 35.00 ± 4.32 (33.69–36.32) | 34.31 (31.30–37.49) | <0.001 | 35.72 ± 4.63 (34.25–37.18) | 35.42 (31.60–39.06) | 35.26 ± 4.74 (33.76–36.76) | 34.35 (31.52–38.83) | 0.02 |
| Waist circumference (cm) | 109 ± 10 (106–112) | 109 (103–113) | 106 ± 10 (103–109) | 103 (98–111) | <0.001 | 109 ± 9 (106–112) | 107 (103–117) | 105 ± 9 (102–108) | 105 (98–112) | <0.001 |
| Endothelial function parameters | ||||||||||
| ADMA (nmol/mL) | 1.54 ± 1.39 (1.12–1.97) | 0.94 (0.41–2.50) | 1.47 ± 1.43 (1.04–1.91) | 0.79 (0.41–2.35) | 0.16 | 1.39 ± 1.43 (0.94–1.85) | 0.56 (0.38–2.32) | 1.52 ± 1.45 (1.06–1.98) | 0.69 (0.38–2.67) | 0.80 |
| eNOS (U/L) | 28.24 ± 30.27 (19.03–37.44) | 18.74 (13.69–28.48) | 27.03 ± 36.67 (15.88–38.18) | 16.37 (13.55–25.16) | 0.01 | 24.99 ± 24.63 (17.21–32.76) | 17.56 (14.43–25.89) | 25.86 ± 24.58 (18.10–33.62) | 18.22 (13.79–28.61) | 0.93 |
| HCY (µmmol/L) | 11.08 ± 2.79 (10.23–11.93) | 11.18 (9.25–12.59) | 10.72 ± 2.55 (9.95–11.50) | 10.11 (8.99–12.56) | 0.29 | 10.82 ± 3.03 (9.87–11.78) | 10.25 (8.55–11.80) | 10.86 ± 3.28 (9.82–11.89) | 10.85 (8.99–12.20) | 0.69 |
| NO2 (µmol/L) | 1.42 ± 0.30 (1.33–1.52) | 1.34 (1.19–1.71) | 1.47 ± 0.31 (1.38–1.57) | 1.44 (1.26–1.73) | 0.48 | 1.43 ± 0.30 (1.33–1.52) | 1.39 (1.23–1.57) | 1.48 ± 0.28 (1.39–1.56) | 1.47 (1.30–1.62) | 0.30 |
| NO3 (µmol/L) | 37.55 ± 18.52 (31.92–43.19) | 31.37 (24.77–44.08) | 41.71 ± 32.46 (31.84–51.58) | 29.44 (25.57–43.23) | 0.79 | 37.26 ± 16.22 (32.14–42.38) | 32.46 (27.92–40.49) | 42.57 ± 22.20 (35.57–49.58) | 34.48 (27.38–56.65) | 0.41 |
| PAI-1 (ng/mL) | 118.5 ± 32.4 (108.6–128.3) | 119.6 (93.9–134.7) | 118.9 ± 35.8 (108.0–129.7) | 119.6 (91.2–137.8) | 0.66 | 121.4 ± 42.0 (108.2–134.7) | 117.0 (86.0–148.0) | 118.5 ± 36.8 (106.9–130.1) | 121.9 (89.2–145.1) | 0.87 |
| sVCAM-1 (ng/mL) | 795.03 ± 190.49 (737.12–852.95) | 738.00 (674.50–863.00) | 821.86 ± 213.00 (757.10–886.62) | 806.50 (684.50–914.50) | 0.24 | 811.39 ± 268.55 (726.62–896.15) | 777.00 (651.00–867.00) | 843.33 ± 317.13 (743.24–943.44) | 801.00 (719.00–911.00) | 0.27 |
| VEGF (pg/mL) | 475 ± 268 (393–556) | 408 (266–597) | 459 ± 265 (379–540) | 407 (257–566) | 0.16 | 482 ± 256 (401–563) | 432 (239–638) | 492 ± 275 (405–579) | 455 (250–660) | 0.40 |
| Arterial stiffness | ||||||||||
| PWA SP (mmHg) | 130 ± 12 (126–134) | 130 (120–139) | 125 ± 14 (120–129) | 123 (117–132) | <0.001 | 130 ± 18 (125–136) | 130 (121–137) | 125 ± 11 (121–129) | 126 (117–132) | 0.06 |
| PWA PP (mmHg) | 42 ± 12 (38–45) | 41 (36–47) | 40 ± 10 (37–43) | 39 (32–44) | 0.10 | 42 ± 14 (38–47) | 40 (35–48) | 40 ± 9 (38–43) | 40 (34–46) | 0.80 |
| PWA AIx | 32 ± 14 (27–36) | 30 (22–37) | 29 ± 12 (25–32) | 30 (21–35) | 0.38 | 29 ± 14 (25–33) | 29 (19–37) | 34 ± 21 (27–41) | 34 (24–41) | 0.26 |
| PWA AP (mmHg) | 13 ± 6 (12–15) | 13 (9–18) | 12 ± 8 (10–15) | 11 (8–15) | 0.17 | 13 ± 7 (10–15) | 12 (7–16) | 15 ± 14 (11–20) | 13 (7–20) | 0.23 |
| PWV (m/s) | 7.1 ± 1.3 (6.7–7.6) | 7.1 (6.2–7.9) | 6.5 ± 0.8 (6.3–6.8) | 6.5 (5.8–7.3) | <0.001 | 6.8 ± 1.2 (6.4–7.2) | 6.6 (5.8–7.5) | 6.7 ± 1.4 (6.2–7.2) | 6.4 (5.7–7.4) | 0.16 |
| Antioxidant status parameters | ||||||||||
| GSH (µmol/L) | 22.71 ± 27.72 (14.29–31.14) | 15.26 (10.34–24.52) | 20.02 ± 28.54 (11.34–28.70) | 12.90 (8.82–18.51) | 0.003 | 28.42 ± 78.86 (3.53–53.31) | 13.33 (7.02–24.36) | 30.27 ± 85.48 (3.29–57.25) | 16.27 (7.53–23.52) | 0.22 |
| SOD (U/mL) | 3.81 ± 1.98 (3.20–4.41) | 3.78 (2.60–4.59) | 3.98 ± 2.12 (3.34–4.63) | 3.78 (2.49–4.78) | 0.50 | 3.26 ± 1.15 (2.90–3.62) | 3.03 (2.35–4.19) | 3.21 ± 1.63 (2.69–3.73) | 2.76 (2.05–4.19) | 0.78 |
| TAS (ng/mL) | 675 ± 872 (410–940) | 252 (196–585) | 601 ± 824 (348 to 854) | 218 (180–381) | <0.001 | 672 ± 854 (402–941) | 210 (179–605) | 643 ± 879 (366–920) | 194 (166–440) | 0.63 |
| Inflammatory markers | ||||||||||
| hs-CRP (mg/L) | 3.87 ± 3.76 (2.73–5.02) | 2.75 (1.60–4.85) | 4.34 ± 4.63 (2.94–5.75) | 2.75 (1.60–4.85) | 0.80 | 3.95 ± 3.85 (2.74–5.17) | 2.30 (1.70–4.60) | 4.22 ± 4.29 (2.86–5.57) | 2.60 (1.70–4.20) | 0.39 |
| hs-IL-6 (pg/mL) | 2.19 ± 1.54 (1.72–2.66) | 1.85 (1.25–2.58) | 2.34 ± 1.60 (1.86–2.83) | 1.98 (1.24–3.14) | 0.30 | 1.78 ± 0.91 (1.49–2.06) | 1.50 (1.29–1.94) | 2.16 ± 1.14 (1.80–2.53) | 1.83 (1.51–2.64) | 0.03 |
| hs-IL-8 (pg/mL) | 33.08 ± 26.3 (25.08–41.08))0 | 23.24 (17.35–42.94) | 24.15 ± 24.73 (16.63–31.66) | 17.52 (13.09–23.06) | 0.009 | 32.64 ± 36.11 (21.25–44.04) | 22.14 (12.72–29.08) | 30.72 ± 29.51 (21.40–40.03) | 18.47 (14.01–34.35) | 0.82 |
| MCP-1 (pg/mL) | 427.72 ± 196.66 (367.93–487.51) | 414.63 (300.73–550.72) | 458.13 ± 219.54 (391.38–524.88) | 453.85 (297.10–527.73) | 0.07 | 425.55 ± 166.35 (373.04–478.05) | 407.05 (324.65–495.35) | 481.52 ± 119.58 (421.05–542.00) | 465.90 (350.15–589.03) | 0.007 |
| MMP-2 (ng/mL) | 209.03 ± 51.59 (193.34–224.71) | 205.14 (169.00–238.09) | 204.42 ± 53.10 (188.28–220.56) | 205.04 (164.50–238.14) | 0.36 | 201.97 ± 54.56 (184.75–219.20) | 198.00 (169.00–219.00) | 184.88 ± 47.97 (169.74–200.02) | 175.96 (155.24–204.00) | 0.003 |
| MMP-9 (ng/mL) | 759.7 ± 281.4 (674.2–845.3) | 746.3 (567.0–936.0) | 670.4 ± 263.3 (590.3–750.4) | 628.3 (501.8–883.0) | 0.04 | 778.0 ± 374.8 (659.7–896.3) | 696.5 (521.0–918.0) | 881.2 ± 450.3 (739.1–1023.4) | 786.0 (577.3–962.0) | 0.05 |
| TNF-α (pg/mL) | 40 ± 52 (24–56) | 15 (12–33) | 36 ± 48 (22–51) | 14 (11–29) | 0.003 | 38 ± 49 (22–53) | 13 (11–33) | 40 ± 51 (24–56) | 12 (11–34) | 0.63 |
| Endurance Training (n = 44) | Endurance-Strength Training (n = 41) | p | |||
|---|---|---|---|---|---|
| Mean ± SD (95% CI) | Median (Q1–Q3) | Mean ± SD (95% CI) | Median (Q1–Q3) | ||
| Anthropometric parameter | |||||
| Δ Weight (kg) | −1.2 ± 2.0 (−1.8–−0.5) | −1.0 (−2.3–−0.1) | −1.1 ± 2.8 (−2.0–−0.3) | −0.7 (−3.3–1.2) | 0.80 |
| Δ BMI (kg/m2) | −0.45 ± 0.78 (−0.68–−0.21) | −0.37 (−0.82–−0.05) | −0.46 ± 1.06 (−0.79–−0.12) | −0.31 (−1.33–0.45) | 0.88 |
| Δ Waist circumference (cm) | −4 ± 6 (−5–−2) | −4 (−7–−2) | −4 ± 5 (−5–−2) | −4 (−6–−2) | 0.80 |
| Endothelial function parameters | |||||
| Δ ADMA (nmol/mL) | −0.07 ± 0.29 (−0.15–0.02) | −0.03 (−0.18–0.06) | 0.12 ± 0.79 (−0.13–0.37) | −0.02 (−0.06–0.11) | 0.22 |
| Δ eNOS (U/L) | −1.21 ± 9.37 (−4.05–1.64) | −0.70 (−3.47–0.58) | 0.87 ± 9.0 (−1.98–3.72) | −0.75 (−2.87–2.89) | 0.23 |
| Δ HCY (µmmol/L) | −0.36 ± 1.88 (−0.93–0.21) | −0.28 (−1.39–0.97) | 0.04 ± 1.98 (−0.59–0.66) | 0.10 (−1.37–1.26) | 0.29 |
| Δ NO2 (µmol/L) | 0.05 ± 0.41 (−0.08–0.17) | 0.06 (−0.28–0.38) | 0.05 ± 0.42 (−0.09–0.18) | 0.02 (−0.11–0.33) | 0.86 |
| Δ NO3 (µmol/L) | 4.15 ± 35.06 (−6.51–14.81) | 0.10 (−6.58–5.99) | 5.31 ± 23.87 (−2.22–12.85) | 0.54 (−6.36–13.18) | 0.76 |
| Δ PAI-1 (ng/mL) | 0.4 ± 26.1 (−7.5–8.3) | 1.0 (−9.7–13.2) | −2.9 ± 27.4 (−11.60–5.72) | −3.0 (−7.0–12.0) | 0.74 |
| Δ sVCAM-1 (ng/mL) | 26.83 ± 144.23 (−17.02–70.68) | 21.50 (−60.75–114.75) | 31.95 ± 146.05 (−14.15–78.05) | 6.00 (−53.35–117.00) | 0.98 |
| Δ VEGF (pg/mL) | −15 ± 88 (−42–11) | −12 (−72–35) | 10 ± 93 (−19–39) | 9 (−22–56) | 0.10 |
| Arterial stiffness | |||||
| Δ PWA SP (mmHg) | −5 ± 11 (−8–−1) | −6 (−12–−1) | −5 ± 15 (−10–0) | −2 (−8–2) | 0.20 |
| Δ PWA PP (mmHg) | −2 ± 10 (−5–1) | −3 (−8–3) | −2 ± 14 (−6–2) | 1 (−10–5) | 0.43 |
| Δ PWA AIx | −3 ± 15 (−8–1) | 0 (−13–5) | 5 ± 20 (−1–11) | 2 (−5–12) | 0.14 |
| Δ PWA AP (mmHg) | −5 ± 9 (−8–2) | −4 (−9–0) | −9 ± 15 (−13–4) | −7 (−14–1) | 0.16 |
| Δ PWV (m/s) | −0.6 ± 1.2 (−1.0–0.2) | −0.4 (−0.8–0.0) | −0.2 ± 1.6 (−0.8–0.3) | −0.1 (−0.4–0.1) | 0.06 |
| Antioxidant status parameters | |||||
| Δ GSH (µmol/L) | −2.70 ± 6.08 (−4.54–−0.85) | −2.50 (−6.02–0.11) | 1.85 ± 8.87 (−0.96–4.65) | 0.74 (−1.99–4.65) | 0.003 |
| Δ SOD (U/mL) | 0.18 ± 1.46 (−0.27–0.62) | −0.13 (−0.84–1.46) | −0.05 ± 1.31 (−0.47–0.36) | −0.07 (−0.84–0.96) | 0.65 |
| Δ TAS (ng/mL) | −74 ± 187 (−131–−17) | −29 (−65–−10) | −29 ± 265 (−112–55) | −2 (−28–18) | 0.002 |
| Inflammatory markers | |||||
| Δ hs-CRP (mg/L) | 0.47 ± 2.86 (−0.40–1.34) | −0.08 (−1.45–1.25) | 0.27 ± 2.99 (−0.68–1.21) | −0.30 (−1.00–0.60) | 0.60 |
| Δ hs-IL-6 (pg/mL) | 0.16 ± 1.79 (−0.39–0.70) | 0.30 (−0.41–0.78) | 0.39 ± 1.11 (0.04–0.74) | 0.36 (−0.23–0.70) | 0.51 |
| Δ hs-IL-8 (pg/mL) | −8.93 ± 36.93 (−20.16–2.30) | −3.75 (−18.37–1.83) | −1.93 ± 47.51 (−16.92–13.07) | −1.07 (−8.07–8.93) | 0.11 |
| Δ MCP-1 (pg/mL) | 30.41 ± 98.70 (0.40–60.42) | 27.15 (−38.28–83.45) | 55.98 ± 123.00 (−17.15–94.80) | 48.75 (−36.25–126.75) | 0.38 |
| Δ MMP-2 (ng/mL) | −4.61 ± 27.68 (−13.02–3.81) | −2.97 (−23.02–15.61) | −17.10 ± 36.06 (−28.48–−5.71) | −15.00 (−34.00–3.00) | 0.07 |
| Δ MMP-9 (ng/mL) | −89.4 ± 258.4 (−167.9–−10.8) | −75.0 (−267.2–103.8) | 103.2 ± 329.3 (−0.7–207.2) | 117.0 (−63.3–254.0) | 0.003 |
| Δ TNF-α (pg/mL) | −3 ± 12 (−7–0) | −1 (−3–0) | 2 ± 16 (−3–7) | 0 (−1–1) | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamka, M.; Bogdański, P.; Krzyżanowska-Jankowska, P.; Miśkiewicz-Chotnicka, A.; Karolkiewicz, J.; Duś-Żuchowska, M.; Mądry, R.; Lisowska, A.; Gotz-Więckowska, A.; Iskakova, S.; et al. Endurance Training Depletes Antioxidant System but Does Not Affect Endothelial Functions in Women with Abdominal Obesity: A Randomized Trial with a Comparison to Endurance-Strength Training. J. Clin. Med. 2021, 10, 1639. https://doi.org/10.3390/jcm10081639
Jamka M, Bogdański P, Krzyżanowska-Jankowska P, Miśkiewicz-Chotnicka A, Karolkiewicz J, Duś-Żuchowska M, Mądry R, Lisowska A, Gotz-Więckowska A, Iskakova S, et al. Endurance Training Depletes Antioxidant System but Does Not Affect Endothelial Functions in Women with Abdominal Obesity: A Randomized Trial with a Comparison to Endurance-Strength Training. Journal of Clinical Medicine. 2021; 10(8):1639. https://doi.org/10.3390/jcm10081639
Chicago/Turabian StyleJamka, Małgorzata, Paweł Bogdański, Patrycja Krzyżanowska-Jankowska, Anna Miśkiewicz-Chotnicka, Joanna Karolkiewicz, Monika Duś-Żuchowska, Radosław Mądry, Aleksandra Lisowska, Anna Gotz-Więckowska, Saule Iskakova, and et al. 2021. "Endurance Training Depletes Antioxidant System but Does Not Affect Endothelial Functions in Women with Abdominal Obesity: A Randomized Trial with a Comparison to Endurance-Strength Training" Journal of Clinical Medicine 10, no. 8: 1639. https://doi.org/10.3390/jcm10081639
APA StyleJamka, M., Bogdański, P., Krzyżanowska-Jankowska, P., Miśkiewicz-Chotnicka, A., Karolkiewicz, J., Duś-Żuchowska, M., Mądry, R., Lisowska, A., Gotz-Więckowska, A., Iskakova, S., Walkowiak, J., & Mądry, E. (2021). Endurance Training Depletes Antioxidant System but Does Not Affect Endothelial Functions in Women with Abdominal Obesity: A Randomized Trial with a Comparison to Endurance-Strength Training. Journal of Clinical Medicine, 10(8), 1639. https://doi.org/10.3390/jcm10081639