
Evaluation of a Broad Panel of SARS-CoV-2 Serological Tests for Diagnostic Use

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Determination of Specificity of the Analysed Assays
3.2. SARS-CoV-2 Positive Panel
3.3. Determination of the Sensitivity of the Assays
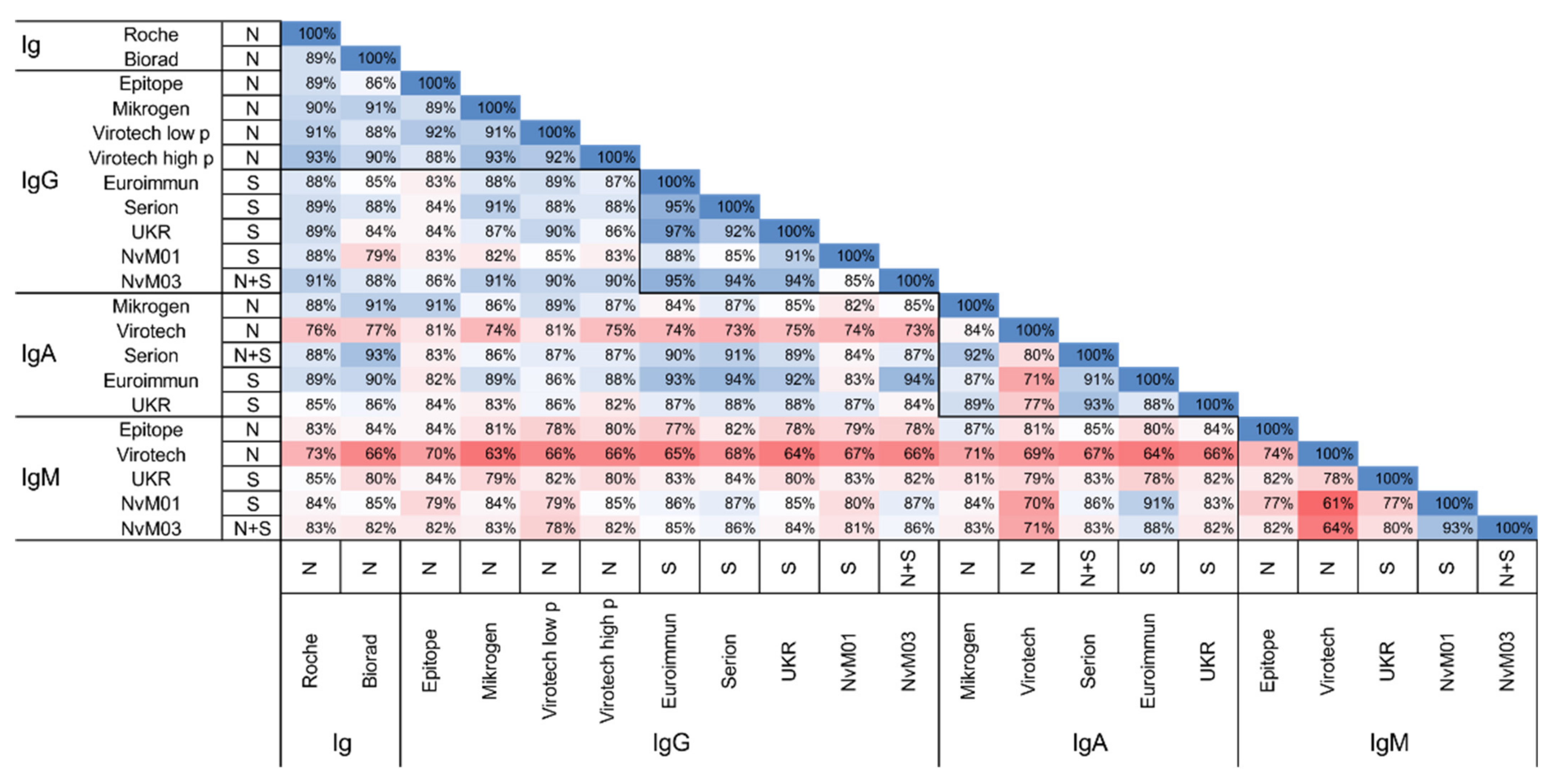
3.4. Agreement between the Different Serological Assays
3.5. Correlation with Neutralisation Titer
3.6. Evaluation of an Additional Panel of LFAs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vashist, S.K.; Luong, J.H.T. Immunoassays. In Handbook of Immunoassay Technologies; Internet; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1–18. Available online: https://linkinghub.elsevier.com/retrieve/pii/B9780128117620000013 (accessed on 16 February 2021).
- Houlihan, C.F.; Beale, R. The complexities of SARS-CoV-2 serology. Lancet Infect. Dis. 2020, 20, 1350–1351. [Google Scholar] [CrossRef]
- Xiaojie, S.; Yu, L.; lei, Y.; Guang, Y.; Min, Q. Neutralizing antibodies targeting SARS-CoV-2 spike protein. Stem Cell Res. 2021, 50, 102125. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Wheatley, A.K.; Kent, S.J.; DeKosky, B.J. Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies. Nat. Microbiol. 2020, 5, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Glück, V.; Grobecker, S.; Tydykov, L.; Salzberger, B.; Glück, T.; Weidlich, T.; Bertok, M.; Gottwald, C.; Wenzel, J.J.; Gessner, A.; et al. SARS-CoV-2 directed antibodies persist for more than six months in a cohort withmild to moderate COVID-19. Infection 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Hähnel, V.; Peterhoff, D.; Bäuerlein, V.; Brosig, A.-M.; Pamler, I.; Johnson, C.; Bica, A.; Totir, M.; Ossner, T.; Stemmer, B.; et al. Manufacturing of convalescent plasma of COVID-19 patients: Aspects of quality. PLoS ONE 2020, 15, e0243967. [Google Scholar] [CrossRef]
- Peterhoff, D.; Glück, V.; Vogel, M.; Schuster, P.; Schütz, A.; Neubert, P.; Albert, V.; Frisch, S.; Kiessling, M.; Pervan, P.; et al. A highly specific and sensitive serological assay detects SARS-CoV-2 antibody levels in COVID-19 patients that correlate with neutralization. Infection 2021, 49, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Newcombe, R.G. Two-sided confidence intervals for the single proportion: Comparison of seven methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Whitman, J.D.; Hiatt, J.; Mowery, C.T.; Shy, B.R.; Yu, R.; Yamamoto, T.N.; Rathore, U.; Goldgof, G.M.; Whitty, C.; Woo, J.M.; et al. Evaluation of SARS-CoV-2 serology assays reveals a range of test performance. Nat. Biotechnol. 2020, 38, 1174–1183. [Google Scholar] [CrossRef]
- Interim Guidelines for COVID-19 Antibody Testing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html (accessed on 16 February 2021).
- Kohmer, N.; Toptan, T.; Pallas, C.; Karaca, O.; Pfeiffer, A.; Westhaus, S.; Widera, M.; Berger, A.; Hoehl, S.; Kammel, M.; et al. The Comparative Clinical Performance of Four SARS-CoV-2 Rapid Antigen Tests and Their Correlation to Infectivity In Vitro. J. Clin. Med. 2021, 10, 328. [Google Scholar] [CrossRef]
- Tré-Hardy, M.; Wilmet, A.; Beukinga, I.; Favresse, J.; Dogné, J.-M.; Douxfils, J.; Blairon, L. Analytical and clinical validation of an ELISA for specific SARS-CoV-2 IgG, IgA, and IgM antibodies. J. Med. Virol. 2021, 93, 803–811. [Google Scholar] [CrossRef]
- Nicol, T.; Lefeuvre, C.; Serri, O.; Pivert, A.; Joubaud, F.; Dubée, V.; Kouatchet, A.; Ducancelle, A.; Lunel-Fabiani, F.; le Guillou-Guillemette, H. Assessment of SARS-CoV-2 serological tests for the diagnosis of COVID-19 through the evaluation of three immunoassays: Two automated immunoassays (Euroimmun and Abbott) and one rapid lateral flow immunoassay (NG Biotech). J. Clin. Virol. 2020, 129, 104511. [Google Scholar] [CrossRef]
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Brief clinical evaluation of six high-throughput SARS-CoV-2 IgG antibody assays. J. Clin. Virol. 2020, 129, 104480. [Google Scholar] [CrossRef]
- Pérez-García, F.; Pérez-Tanoira, R.; Iglesias, M.E.; Romanyk, J.; Arroyo, T.; Gómez-Herruz, P.; González, R.; García, S.L.; Cuadros-González, J. Comparative evaluation of six immunoassays for the detection of antibodies against SARS-CoV-2. J. Virol. Methods 2021, 289, 114047. [Google Scholar] [CrossRef]
- Brochot, E.; Demey, B.; Handala, L.; François, C.; Duverlie, G.; Castelain, S. Comparison of different serological assays for SARS-CoV-2 in real life. J. Clin. Virol. 2020, 130, 104569. [Google Scholar] [CrossRef] [PubMed]
- Dörschug, A.; Schwanbeck, J.; Hahn, A.; Hillebrecht, A.; Blaschke, S.; Mese, K.; Groß, U.; Dierks, S.; Frickmann, H.; Zautner, A.E. Comparison of Five Serological Assays for the Detection of SARS-CoV-2 Antibodies. Diagnostics 2021, 11, 78. [Google Scholar] [CrossRef]
- Van Praet, J.T.; Coene, A.-S.; Van De Moortele, K.; Descheemaeker, P.; Reynders, M. Comparison of four commercial SARS-CoV-2 IgG immuno-assays in RT-PCR negative patients with suspect CT findings. Infection 2021, 49, 145–148. [Google Scholar] [CrossRef]
- Nilsson, A.C.; Holm, D.K.; Justesen, U.S.; Gorm-Jensen, T.; Andersen, N.S.; Øvrehus, A.; Johansen, I.S.; Michelsen, J.; Sprogøe, U.; Lillevang, S.T. Comparison of six commercially available SARS-CoV-2 antibody assays-Choice of assay depends on intended use. Int. J. Infect. Dis. 2021, 103, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Bundschuh, C.; Wiesinger, K.; Gabriel, C.; Clodi, M.; Mueller, T.; Dieplinger, B. Comparison of the Elecsys® Anti-SARS-CoV-2 immunoassay with the EDITM enzyme linked immunosorbent assays for the detection of SARS-CoV-2 antibodies in human plasma. Clin. Chim. Acta 2020, 509, 18–21. [Google Scholar] [CrossRef]
- Nguyen, N.N.; Mutnal, M.B.; Gomez, R.R.; Pham, H.N.; Nguyen, L.T.; Koss, W.; Rao, A.; Arroliga, A.C.; Wang, L.; Wang, D.; et al. Correlation of ELISA method with three other automated serological tests for the detection of anti-SARS-CoV-2 antibodies. PLoS ONE 2020, 15, e0240076. [Google Scholar] [CrossRef] [PubMed]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef]
- Andrey, D.O.; Cohen, P.; Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Guessous, I.; Stringhini, S.; et al. Head-to-Head Accuracy Comparison of Three Commercial COVID-19 IgM/IgG Serology Rapid Tests. J. Clin. Med. 2020, 9, 2369. [Google Scholar] [CrossRef]
- Schaffner, A.; Risch, L.; Aeschbacher, S.; Risch, C.; Weber, M.C.; Thiel, S.L.; Jüngert, K.; Pichler, M.; Grossmann, K.; Wohlwend, N.; et al. Characterization of a Pan-Immunoglobulin Assay Quantifying Antibodies Directed against the Receptor Binding Domain of the SARS-CoV-2 S1-Subunit of the Spike Protein: A Population-Based Study. J. Clin. Med. 2020, 9, 3989. [Google Scholar] [CrossRef] [PubMed]
- Gillot, C.; Douxfils, J.; Cadrobbi, J.; Laffineur, K.; Dogné, J.-M.; Elsen, M.; Eucher, C.; Melchionda, S.; Modaffarri, É.; Tré-Hardy, M.; et al. An Original ELISA-Based Multiplex Method for the Simultaneous Detection of 5 SARS-CoV-2 IgG Antibodies Directed against Different Antigens. J. Clin. Med. 2020, 9, 3752. [Google Scholar] [CrossRef] [PubMed]
- Vanshylla, K.; Di Cristanziano, V.; Kleipass, F.; Dewald, F.; Schommers, P.; Gieselmann, L.; Gruell, H.; Schlotz, M.; Ercanoglu, M.S.; Stumpf, R.; et al. Kinetics and Correlates of the Neutralizing Antibody Response to SARS-CoV-2 [Internet]. Immunology. Available online: http://biorxiv.org/lookup/doi/10.1101/2021.01.26.428207 (accessed on 16 February 2021).
- Working Standard NIBSC Anti-SARS-CoV-2 Antibody Diagnostic Calibrant NIBSC Code: 20/162; Instructions for use (Version 1.0, Dated 30 July 2020); National Institute for Biological Standards and Control: Hertfordshire, UK, 2020.
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.O.; Finkin, S.; Schaefer-Babajew, D.; Cipolla, M.; Gaebler, C.; Lieberman, J.A.; et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature 2021. Available online: http://www.nature.com/articles/s41586-021-03324-6 (accessed on 16 February 2021). [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B. SARS-CoV-2 immunity: Review and applications to phase 3 vaccine candidates. Lancet 2020, 396, 1595–1606. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Provider | Format | Product Name | Antigen | Isotype |
|---|---|---|---|---|
| Roche Diagnostics, Mannheim, Germany (ROCHE) | ECLIA | Cobas Ig Elecsys Anti-SARS-CoV-2 | N | pan-Ig |
| Bio-Rad, Marnes-la-Coquette, France (Bio-Rad) | ELISA | Platelia SARS-CoV-2 Total Ab Assay | N | pan-Ig |
| Epitope Diagnostics, San Diego, CA, USA (Epitope) | ELISA | EDI Novel Coronavirus COVID-19 IgG, IgM ELISA Kit | N | IgG, IgM |
| Mikrogen GmbH, Neuried, Germany (Mikrogen) | ELISA | recomWell SARS-CoV-2 IgG, IgA | N | IgG, IgA |
| Virotech, Rüsselsheim, Germany (Viorotech) | ELISA | VIROTECH SARS-CoV-2 IgG, IgM, IgA ELISA | N | IgG, IgM, IgA |
| EUROIMMUN AG, Lübeck, Germany (Euroimmun) | ELISA | Anti-SARS-CoV-2-ELISA IgG, IgA | S | IgG, IgA |
| Institute Virion/Serion GmbH, Würzburg, Germany (Serion) | ELISA | Serion ELISA agile SARS-CoV-2 IgA, IgG (prototype) | IgG: S IgA: S, N | IgG, IgA |
| University Hospital Regensburg, Regensburg, Germany (UKR) | ELISA | SARS-CoV-2-ELISA IgG, IgM, IgA | S | IgG, IgM, IgA |
| Nal van Minden GmbH, Moers, Germany (NvM01, NvM03, NvM05) | LFA | NADAL COVID-19 IgG/IgM 243001 | S | IgG & IgM |
| NADAL COVID-19 IgG/IgM 243003 | S, N | IgG & IgM | ||
| NADAL COVID-19 IgG/IgM 243005 | S, N | IgG & IgM | ||
| Zecen, Taizhou, China (ZECEN) | LFA | SARS-CoV-2 IgG/IgM Rapid Test | n.s. | IgG & IgM |
| Elabscience Biotechnology, Wuhan, China (ELABSCIENCE) | LFA | UNCOV-40 | n.s. | IgG & IgM |
| Genrui Biotech, Shenzhen, China (Genrui) | LFA | 2019-nCoV IgG/IgM | n.s. | IgG & IgM |
| Encode, Zhuhai, China (Encode) | LFA | SARS-CoV-2 IgG/IgM Rapid Test | n.s. | IgG & IgM |
| Boson Biotech, Xiamen, China (Boson) | LFA | Rapid 2019-nCoV IgG/IgM Test Card | n.s. | IgG & IgM |
| Dialab, Wr Neudorf, Austria (Dialab) | LFA | DIAQUICK Covid-19 IgG/IgM Cassette | n.s. | IgG & IgM |
| Chemtron Biotech Co, Shanghai, China (Chemtron) | LFA | Chemtrue 2019-nCoV IgM/IgG | n.s. | IgG & IgM |
| RapiGEN, Anyang, Korea (RapiGEN) | LFA | Covid-19 IgG+IgM Duo | n.s. | IgG & IgM |
| Microprofit Biotech Co, Shenzhen, China (Microprofit) | LFA | fluorecare SARS-CoV-2 IgG IgM | n.s. | IgG & IgM |
| Abnova, Taipeh, Taiwan (Abnova) | LFA | COVID-19 Human IgM/IgG Rapid Test | n.s. | IgG & IgM |
| Türklab, Izmir, Turkey (Türklab) | LFA | SARS-CoV-2 IgM/IgG Ab Test | n.s. | IgG & IgM |
| AmonMed Biotechnology; Xiamen, China (AmonMed) | LFA | COVID-19 IgM/IgG | n.s. | IgG & IgM |
| Affimedix, Hayward, USA (Affimedix) | LFA | TestNOW-Covid-19 IgG/IgM | n.s. | IgG & IgM |
| Provider, Isotype (Antigen) | Sensitivity Manufacturer | Specificity Manufacturer | Sensitivity (CI95%); Ratio as Determined (n = 101) | Sensitivity (CI95%); Ratio as Determined (n = 89) | Specificity (CI95%); Ratio as Determined (n = 60) |
|---|---|---|---|---|---|
| Roche, Ig (N) | 0–6 d: 65.5% 7–13 d: 88.1% ≥14 d: 100% | 99.8% | 0–5 d: 53.3% (36.1–69.8); 16/30 6–10 d: 76.7% (59.1–88.2); 23/30 >10 d: 80.5% (66–89.8); 33/41 | 66.7% (46.7–82); 16/24 85.2% (67.5–94.1); 23/27 86.8% (72.7–94.3); 33/38 | 100% (94–100); 60/60 |
| Bio–Rad, Ig (N) | ≤8 d: 73% 9–10 d: 100% 11–20 d: 97% 21–42 d: 100% | 99.6% | 0–5 d: 73.3% (55.6–85.8); 22/30 6–10 d: 86.7% (70.3–94.7); 26/30 >10 d: 75.6% (60.7–86.2); 31/41 | 91.7% (74.2–97.7); 22/24 96.3% (81.7–99.3); 26/27 81.6% (66.6–90.8); 31/38 | 96.7% (88.6–99.1); 58/60 |
| Epitope, IgG (N) | 100% | 100% | 0–5 d: 53.3% (36.1–69.8); 16/30 6–10 d: 73.3% (55.6–85.8); 22/30 >10 d: 70.7% (55.5–82.4); 29/41 | 66.7% (46.7–82); 16/24 81.5% (63.3–91.8); 22/27 76.3% (60.8–87); 29/38 | 100% (94–100); 60/60 |
| Epitope, IgM (N) | 45% | 100% | 0–5 d: 63.3% (45.5–78.1); 19/30 6–10 d: 80% (62.7–90.5); 24/30 >10 d: 58.5% (43.4–72.2); 24/41 | 79.2% (59.5–90.8); 19/24 88.9% (71.9–96.2); 24/27 63.2% (47.3–76.6); 24/38 | 100% (94–100); 60/60 |
| Mikrogen, IgG (N) | <12 d: 86% 12–23 d: 100% >23 d: 100% | 98.7% | 0–5 d: 66.7% (48.8–80.8); 20/30 6–10 d: 76.7% (59.1–88.2); 23/30 >10 d: 85.4% (71.6–93.1); 35/41 | 83.3% (64.2–93.3); 20/24 85.2% (67.5–94.1); 23/27 92.1% (79.2–97.3); 35/38 | 98.3% (91.1–99.7); 59/60 |
| Mikrogen, IgA (N) | <12 d: 50% 12–23 d: 95% >23 d: 67% | 99.3% | 0–5 d: 66.7% (48.8–80.8); 20/30 6–10 d: 76.7% (59.1–88.2); 23/30 >10 d: 70.7% (55.5–82.4); 29/41 | 83.3% (64.2–93.3); 20/24 85.2% (67.5–94.1); 23/27 76.3% (60.8–87); 29/38 | 96.7% (88.6–99.1); 58/60 |
| Virotech, IgG (N) | 0–5 d: 7.7% (low p) 6–8 d: 28.6% (low p) 9–11 d: 47.1% (low p) ≥12 d: 100% (low p) | 100% (low p) | 0–5 d: 60% (42.3–75.4); 18/30 6–10 d: 70% (52.1–83.3); 21/30 >10 d: 78% (63.3–88); 32/41 | 70.8% (50.8–85.1); 17/24 77.8% (59.2–89.4); 21/27 84.2% (69.6–92.6); 32/38 | 98.3% (91.1–99.7); 59/60 |
| 0–5 d: 7.7% (high p) 6–8 d: 35.7% (high p) 9–11 d: 58.8% (high p) ≥12 d: 100% (high p) | 99.8% (high p) | 0–5 d: 73.3% (55.6–85.8); 22/30 6–10 d: 76.7% (59.1–88.2); 23/30 >10 d: 82.9% (68.7–91.5); 34/41 | 83.3% (64.2–93.3); 20/24 85.2% (67.5–94.1); 23/27 89.5% (75.9–95.8); 34/38 | 96.7% (88.6–99.1); 58/60 | |
| Virotech, IgA (N) | 0–5 d: 7.7% 6–8 d: 50% 9–11 d: 64.7% ≥12 d 76.5% | 100% | 0–5 d: 63.3% (45.5–78.1); 19/30 6–10 d: 56.7% (39.2–72.6); 17/30 >10 d: 48.8% (34.3–63.5); 20/41 | 79.2% (59.5–90.8); 19/24 63% (44.2–78.5); 17/27 52.6% (37.3–67.5); 20/38 | 100% (94–100); 60/60 |
| Virotech, IgM (N) | 0–5 d: 0% 6–8 d: 42.9% 9–11 d: 41.2% ≥12 d 70.7% | 100% | 0–5 d: 36.7% (21.9–54.5); 11/30 6–10 d: 50% (33.2–66.9); 15/30 >10 d: 46.3% (32.1–61.3); 19/41 | 45.8% (27.9–64.9); 11/24 55.6% (37.3–72.4); 15/27 50% (34.9–65.2); 19/38 | 98.3% (91.1–99.7); 59/60 |
| Euroimmun, IgG (S) | ≤10 d 22.4% <10–20 d 87.5% ≥21 d 100% | 99.3% | 0–5 d: 56.7% (39.2–72.6); 17/30 6–10 d: 70% (52.1–83.3); 21/30 >10 d: 87.8% (74.5–94.7); 36/41 | 70.8% (50.8–85.1); 17/24 77.8% (59.2–89.4); 21/27 94.7% (82.7–98.5); 36/38 | 100% (94–100); 60/60 |
| Euroimmun, IgA (S) | >10 d: 60.2% <10 d: 98.6% | 92% | 0–5 d: 70% (52.1–83.3); 21/30 6–10 d: 80% (62.7–90.5); 24/30 >10 d: 87.8% (74.5–94.7); 36/41 | 87.5% (69–95.7); 21/24 88.9% (71.9–96.2); 24/27 94.7% (82.7–98.5); 36/38 | 93.3% (84.1–97.4); 56/60 |
| Serion, IgG (S) | 96.2% | 99.2% | 0–5 d: 60% (42.3–75.4); 18/30 6–10 d: 76.7% (59.1–88.2); 23/30 >10 d: 82.9% (68.7–91.5); 34/41 | 75% (55.1–88); 18/24 85.2% (67.5–94.1); 23/27 89.5% (75.9–95.8); 34/38 | 100% (94–100); 60/60 |
| Serion, IgA (S, N) | 96.3% | 99% | 0–5 d: 70% (52.1–83.3); 21/30 6–10 d: 73.3% (55.6–85.8); 22/30 >10 d: 75.6% (60.7–86.2); 31/41 | 87.5% (69–95.7); 21/24 81.5% (63.3–91.8); 22/27 81.6% (66.6–90.8); 31/38 | 100% (94–100); 60/60 |
| UKR, IgG (S) | >10 d: 96% | 99.3% | 0–5 d: 56.7% (39.2–72.6); 17/30 6–10 d: 66.7% (48.8–80.8); 20/30 >10 d: 87.8% (74.5–94.7); 36/41 | 70.8% (50.8–85.1); 17/24 74.1% (55.3–86.8); 20/27 94.7% (82.7–98.5); 36/38 | 100% (94–100); 60/60 |
| UKR, IgA (S) | >10 d: 92% | 99.3% | 0–5 d: 60% (42.3–75.4); 18/30 6–10 d: 73.3% (55.6–85.8); 22/30 >10 d: 70.7% (55.5–82.4); 29/41 | 75% (55.1–88); 18/24 81.5% (63.3–91.8); 22/27 76.3% (60.8–87); 29/38 | 98.3% (91.1–99.7); 59/60 |
| UKR, IgM (S) | >10 d: 98% | 99.3% | 0–5 d: 50% (33.2–66.9); 15/30 6–10 d: 66.7% (48.8–80.8); 20/30 >10 d: 58.5% (43.4–72.2); 24/41 | 62.5% (42.7–78.8); 15/24 74.1% (55.3–86.8); 20/27 63.2% (47.3–76.6); 24/38 | 100% (94–100); 60/60 |
| NvM01 IgG (S) | 97.4% | 99.3% | 0–5 d: 50% (33.2–66.9); 15/30 6–10 d: 63.3% (45.5–78.1); 19/30 >10 d: 78% (63.3–88); 32/41 | 62.5% (42.7–78.8); 15/24 70.4% (51.5–84.2); 19/27 84.2% (69.6–92.6); 32/38 | 100% (94–100); 60/60 |
| NvM01 IgM (S) | 86.8% | 98.6% | 0–5 d: 70% (52.1–83.3); 21/30 6–10 d: 86.7% (70.3–94.7); 26/30 >10 d: 85.4% (71.6–93.1); 35/41 | 87.5% (69–95.7); 21/24 96.3% (81.7–99.3); 26/27 92.1% (79.2–97.3); 35/38 | 100% (94–100); 60/60 |
| NvM03 IgG (S, N) | 98.8% | 98.7% | 0–5 d: 60% (42.3–75.4); 18/30 6–10 d: 76.7% (59.1–88.2); 23/30 >10 d: 87.8% (74.5–94.7); 36/41 | 75% (55.1–88); 18/24 85.2% (67.5–94.1); 23/27 92.1% (79.2–97.3); 35/38 | 100% (94–100); 60/60 |
| NvM03 IgM (S, N) | 93.7% | 99.1% | 0–5 d: 70% (52.1–83.3); 21/30 6–10 d: 83.3% (66.4–92.7); 25/30 >10 d: 80.5% (66–89.8); 33/41 | 83.3% (64.2–93.3); 20/24 92.6% (76.6–97.9); 25/27 86.8% (72.7–94.3); 33/38 | 95% (86.3–98.3); 57/60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werner, M.; Pervan, P.; Glück, V.; Zeman, F.; Koller, M.; Burkhardt, R.; Glück, T.; Wenzel, J.J.; Schmidt, B.; Gessner, A.; et al. Evaluation of a Broad Panel of SARS-CoV-2 Serological Tests for Diagnostic Use. J. Clin. Med. 2021, 10, 1580. https://doi.org/10.3390/jcm10081580
Werner M, Pervan P, Glück V, Zeman F, Koller M, Burkhardt R, Glück T, Wenzel JJ, Schmidt B, Gessner A, et al. Evaluation of a Broad Panel of SARS-CoV-2 Serological Tests for Diagnostic Use. Journal of Clinical Medicine. 2021; 10(8):1580. https://doi.org/10.3390/jcm10081580
Chicago/Turabian StyleWerner, Maren, Philip Pervan, Vivian Glück, Florian Zeman, Michael Koller, Ralph Burkhardt, Thomas Glück, Jürgen J. Wenzel, Barbara Schmidt, André Gessner, and et al. 2021. "Evaluation of a Broad Panel of SARS-CoV-2 Serological Tests for Diagnostic Use" Journal of Clinical Medicine 10, no. 8: 1580. https://doi.org/10.3390/jcm10081580
APA StyleWerner, M., Pervan, P., Glück, V., Zeman, F., Koller, M., Burkhardt, R., Glück, T., Wenzel, J. J., Schmidt, B., Gessner, A., & Peterhoff, D. (2021). Evaluation of a Broad Panel of SARS-CoV-2 Serological Tests for Diagnostic Use. Journal of Clinical Medicine, 10(8), 1580. https://doi.org/10.3390/jcm10081580