
Comparison of the Effects of Laparoscopic and Open Surgery on Postoperative Acute Kidney Injury in Patients with Colorectal Cancer: Propensity Score Analysis


Abstract
1. Introduction
2. Experimental Section
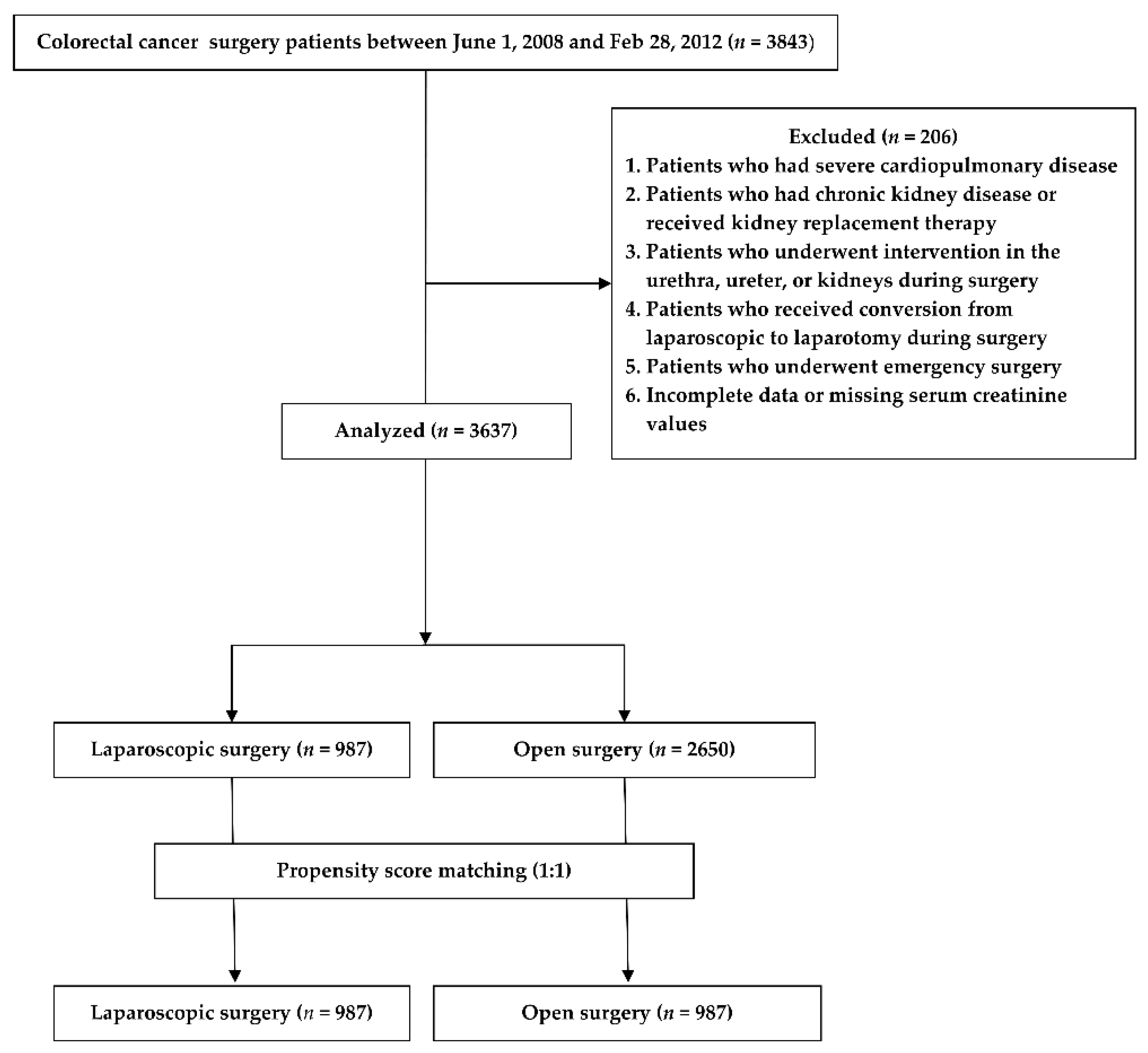
2.1. Study Design and Patient Population
2.2. General Anesthesia and Surgical Technique
2.3. Clinical Data Collection and Outcome Assessments
2.4. Primary and Secondary Outcomes
2.5. Statistical Analysis
3. Results
3.1. Primary Outcomes
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Levin, A.S.; Bilous, R.W.; Coresh, J. Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. (2011) 2013, 3, 19–62. [Google Scholar]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.; Kim, S.C.; Kim, M.G.; Jo, S.K.; Cho, W.Y.; Kim, H.K. The incidence and risk factors of acute kidney injury after hepatobiliary surgery: A prospective observational study. BMC Nephrol. 2014, 15, 169. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.E.; Kirwan, C.J.; Pearse, R.M.; Prowle, J.R. Incidence and associations of acute kidney injury after major abdominal surgery. Intensive Care Med. 2016, 42, 521–530. [Google Scholar] [CrossRef]
- Lameire, N.H.; Bagga, A.; Cruz, D.; De Maeseneer, J.; Endre, Z.; Kellum, J.A.; Liu, K.D.; Mehta, R.L.; Pannu, N.; Van Biesen, W.; et al. Acute kidney injury: An increasing global concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Allardyce, R.A.; Bagshaw, P.F.; Frampton, C.M.; Frizelle, F.A.; Hewett, P.J.; Rieger, N.A.; Smith, J.S.; Solomon, M.J.; Stevenson, A.R. Australasian Laparoscopic Colon Cancer Study shows that elderly patients may benefit from lower postoperative complication rates following laparoscopic versus open resection. Br. J. Surg. 2010, 97, 86–91. [Google Scholar] [CrossRef]
- Li, H.; Han, X.; Su, L.; Zhu, W.; Xu, W.; Li, K.; Zhao, Q.; Yang, H.; Liu, H. Laparoscopic radical gastrectomy versus traditional open surgery in elderly patients with gastric cancer: Benefits and complications. Mol. Clin. Oncol. 2014, 2, 530–534. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Story, D.; Letis, A.; Klemz, K.; Matalanis, G.; Seevanayagam, S.; Dragun, D.; Seeliger, E.; Mertens, P.R.; et al. Effect of mean arterial pressure, haemoglobin and blood transfusion during cardiopulmonary bypass on post-operative acute kidney injury. Nephrol. Dial. Transplant. 2012, 27, 153–160. [Google Scholar] [CrossRef]
- Huang, S.; Li, Z.; Zou, N.; Dai, T.; Cao, X.L.; Jia, Z.; Peng, W.P.; Yang, N.; Jia, R.F.; Zuo, M.Z. Comparison of Postoperative Acute Kidney Injury Between Laparoscopic and Laparotomy Procedures in Elderly Patients Undergoing Colorectal Surgery. Surg. Laparosc. Endosc. Percutan Tech. 2020, 31, 160–164. [Google Scholar] [CrossRef]
- Moon, Y.J.; Jun, I.G.; Kim, K.H.; Kim, S.O.; Song, J.G.; Hwang, G.S. Comparison of acute kidney injury between open and laparoscopic liver resection: Propensity score analysis. PLoS ONE 2017, 12, e0186336. [Google Scholar] [CrossRef]
- Cisek, L.J.; Gobet, R.M.; Peters, C.A. Pneumoperitoneum produces reversible renal dysfunction in animals with normal and chronically reduced renal function. J. Endourol. 1998, 12, 95–100. [Google Scholar] [CrossRef]
- Ben-David, B.; Croitoru, M.; Gaitini, L. Acute renal failure following laparoscopic cholecystectomy: A case report. J. Clin. Anesth. 1999, 11, 486–489. [Google Scholar] [CrossRef]
- Briscoe, J.H.; Bahal, V. Acute renal failure following laparoscopic cholecystectomy. BMJ Case Rep. 2012, 2012, bcr2012006427. [Google Scholar] [CrossRef]
- Miki, Y.; Iwase, K.; Kamiike, W.; Taniguchi, E.; Sakaguchi, K.; Sumimura, J.; Matsuda, H.; Nagai, I. Laparoscopic cholecystectomy and time-course changes in renal function. The effect of the retraction method on renal function. Surg. Endosc. 1997, 11, 838–841. [Google Scholar] [CrossRef]
- Nishio, S.; Takeda, H.; Yokoyama, M. Changes in urinary output during laparoscopic adrenalectomy. BJU Int. 1999, 83, 944–947. [Google Scholar] [CrossRef]
- Micali, S.; Silver, R.I.; Kaufman, H.S.; Douglas, V.D.; Marley, G.M.; Partin, A.W.; Moore, R.G.; Kavoussi, L.R.; Docimo, S.G. Measurement of urinary N-acetyl-beta-D-glucosaminidase to assess renal ischemia during laparoscopic operations. Surg. Endosc. 1999, 13, 503–506. [Google Scholar] [CrossRef]
- Park, Y.S.; Jun, I.G.; Go, Y.; Song, J.G.; Hwang, G.S. Comparison of acute kidney injury between open and laparoscopic pylorus-preserving pancreaticoduodenectomy: Propensity score analysis. PLoS ONE 2018, 13, e0202980. [Google Scholar] [CrossRef]
- Lee, B.R.; Cadeddu, J.A.; Molnar-Nadasdy, G.; Enriquez, D.; Nadasdy, T.; Kavoussi, L.R.; Ratner, L.E. Chronic effect of pneumoperitoneum on renal histology. J. Endourol. 1999, 13, 279–282. [Google Scholar] [CrossRef]
- Argalious, M.Y.; Makarova, N.; Leone, A.; Cywinski, J.; Farag, E. Association of Body Mass Index and Postoperative Acute Kidney Injury in Patients Undergoing Laparoscopic Surgery. Ochsner J. 2017, 17, 224–232. [Google Scholar]
- James, M.T.; Grams, M.E.; Woodward, M.; Elley, C.R.; Green, J.A.; Wheeler, D.C.; de Jong, P.; Gansevoort, R.T.; Levey, A.S.; Warnock, D.G.; et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Diabetes Mellitus, and Hypertension With Acute Kidney Injury. Am. J. Kidney Dis. 2015, 66, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef]
- Bang, J.Y.; Kim, S.O.; Kim, S.G.; Song, J.G.; Kang, J.; Kim, J.W.; Ha, S. Impact of the serum albumin level on acute kidney injury after cerebral artery aneurysm clipping. PLoS ONE 2018, 13, e0206731. [Google Scholar] [CrossRef] [PubMed]
- Margarson, M.P.; Soni, N. Serum albumin: Touchstone or totem? Anaesthesia 1998, 53, 789–803. [Google Scholar] [CrossRef] [PubMed]
- Kashy, B.K.; Podolyak, A.; Makarova, N.; Dalton, J.E.; Sessler, D.I.; Kurz, A. Effect of hydroxyethyl starch on postoperative kidney function in patients having noncardiac surgery. Anesthesiology 2014, 121, 730–739. [Google Scholar] [CrossRef]
- Myburgh, J.A.; Finfer, S.; Bellomo, R.; Billot, L.; Cass, A.; Gattas, D.; Glass, P.; Lipman, J.; Liu, B.; McArthur, C.; et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N. Engl. J. Med. 2012, 367, 1901–1911. [Google Scholar] [CrossRef]
- Myles, P.S.; Bellomo, R.; Corcoran, T.; Forbes, A.; Peyton, P.; Story, D.; Christophi, C.; Leslie, K.; McGuinness, S.; Parke, R.; et al. Restrictive versus Liberal Fluid Therapy for Major Abdominal Surgery. N. Engl. J. Med. 2018, 378, 2263–2274. [Google Scholar] [CrossRef] [PubMed]
- Joosten, A.; Delaporte, A.; Mortier, J.; Ickx, B.; Van Obbergh, L.; Vincent, J.L.; Cannesson, M.; Rinehart, J.; Van der Linden, P. Long-term Impact of Crystalloid versus Colloid Solutions on Renal Function and Disability-free Survival after Major Abdominal Surgery. Anesthesiology 2019, 130, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.P.; Salunke, B.G. Fluid Overload and Acute Kidney Injury. Indian J. Crit. Care. Med. 2020, 24, S94–s97. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, L.; Li, M.; Churilov, L.; Armellini, A.; Gibney, M.; Hewitt, T.; Tan, C.O.; Robbins, R.; Tremewen, D.; Christophi, C.; et al. Associations of fluid amount, type, and balance and acute kidney injury in patients undergoing major surgery. Anaesth. Intensive Care 2018, 46, 79–87. [Google Scholar] [CrossRef]
- Johannes, T.; Mik, E.G.; Nohé, B.; Unertl, K.E.; Ince, C. Acute decrease in renal microvascular PO2 during acute normovolemic hemodilution. Am. J. Physiol. Renal. Physiol. 2007, 292, F796–F803. [Google Scholar] [CrossRef]
- Howard, D.P.; Datta, G.; Cunnick, G.; Gatzen, C.; Huang, A. Surgical site infection rate is lower in laparoscopic than open colorectal surgery. Colorectal. Dis. 2010, 12, 423–427. [Google Scholar] [CrossRef]
- Veldkamp, R.; Kuhry, E.; Hop, W.C.; Jeekel, J.; Kazemier, G.; Bonjer, H.J.; Haglind, E.; Påhlman, L.; Cuesta, M.A.; Msika, S.; et al. Laparoscopic surgery versus open surgery for colon cancer: Short-term outcomes of a randomised trial. Lancet Oncol. 2005, 6, 477–484. [Google Scholar]
- Yang, Z.F.; Wu, D.Q.; Wang, J.J.; Lv, Z.J.; Li, Y. Short- and long-term outcomes following laparoscopic vs. open surgery for pathological T4 colorectal cancer: 10 years of experience in a single center. World J. Gastroenterol. 2018, 24, 76–86. [Google Scholar] [CrossRef]
- Zhou, S.; Wang, X.; Zhao, C.; Liu, Q.; Zhou, H.; Zheng, Z.; Zhou, Z.; Wang, X.; Liang, J. Laparoscopic vs. open colorectal cancer surgery in elderly patients: Short- and long-term outcomes and predictors for overall and disease-free survival. BMC Surg. 2019, 19, 137. [Google Scholar] [CrossRef]
- Song, K.B.; Kim, S.C.; Hwang, D.W.; Lee, J.H.; Lee, D.J.; Lee, J.W.; Park, K.M.; Lee, Y.J. Matched Case-Control Analysis Comparing Laparoscopic and Open Pylorus-preserving Pancreaticoduodenectomy in Patients with Periampullary Tumors. Ann. Surg. 2015, 262, 146–155. [Google Scholar] [CrossRef]
- Bonjer, H.J.; Deijen, C.L.; Abis, G.A.; Cuesta, M.A.; van der Pas, M.H.; de Lange-de Klerk, E.S.; Lacy, A.M.; Bemelman, W.A.; Andersson, J.; Angenete, E.; et al. A randomized trial of laparoscopic versus open surgery for rectal cancer. N. Engl. J. Med. 2015, 372, 1324–1332. [Google Scholar] [CrossRef]


{kind=link}
| Unmatched Sample | Matched Sample | |||||||
|---|---|---|---|---|---|---|---|---|
| Laparoscopic Surgery (n = 987) | Open Surgery (n = 2650) | p | SMD | Laparoscopic Surgery (n = 987) | Open Surgery (n = 987) | p | SMD | |
| Preoperative variables | ||||||||
| Age; years | 59.11 (11.21) | 59.92 (11.23) | 0.052 | 0.072 | 59.11(11.21) | 58.99 (11.22) | 0.011 | |
| Sex; male | 601 (60.9) | 1631 (61.5) | 0.718 | 0.013 | 601 (60.9) | 604 (61.2) | 0.006 | |
| BMI; kg·m−2 | 23.99 (3.00) | 23.75 (3.14) | 0.038 | 0.078 | 23.99 (3.00) | 24.00 (3.10) | 0.004 | |
| DM | 142 (14.4) | 392 (14.8) | 0.759 | 0.011 | 142 (14.4) | 139 (14.1) | 0.009 | |
| HTN | 335 (33.9) | 872 (32.9) | 0.555 | 0.022 | 335 (33.9) | 324 (32.8) | 0.024 | |
| ASA status | 0.006 | 0.127 | 0.021 | |||||
| ASA 1 | 254 (25.7) | 606 (22.9) | 254 (25.7) | 256 (25.9) | ||||
| ASA 2 | 722 (73.2) | 1974 (74.5) | 722 (73.2) | 722 (73.2) | ||||
| ASA 3 | 11 (1.1) | 70 (2.6) | 11 (1.1) | 9 (0.9) | ||||
| Albumin; g·dL−1 | 3.94 (0.40) | 3.81 (0.47) | <0.001 | 0.294 | 3.94 (0.40) | 3.94 (0.41) | <0.001 | |
| Creatinine; mg·dL−1 | 0.80 (0.18) | 0.79 (0.18) | 0.303 | 0.038 | 0.80 (0.18) | 0.80 (0.17) | 0.018 | |
| Intraoperative variables | ||||||||
| Lowest MBP; mm/Hg | 72.45 (8.96) | 70.30(8.87) | <0.001 | 72.45 (8.96) | 71.13 (8.70) | 0.001 | ||
| Operation time; min | 180.55 (58.25) | 172.76 (71.57) | <0.001 | 180.55 (58.25) | 168.81 (68.21) | <0.001 | ||
| Total fluids; mL/kg | 24.28 (19.40–29.68) | 25.76 (20.37–32.87) | <0.001 | 24.28 (19.40–29.68) | 25.32 (19.72–31.98) | 0.001 | ||
| Crystalloid; mL/kg | 18.23 (13.99–23.60) | 19.19 (14.34–26.86) | <0.001 | 18.23 (13.99–23.60) | 18.64 (14.00–25.82) | 0.018 | ||
| Colloid; mL/kg | 7.06 (0.00–8.34) | 7.35 (0.00–8.92) | <0.001 | 7.06 (0.00–8.34) | 7.17 (0.00–8.79) | 0.004 | ||
| Colloid use | 694 (70.3) | 1947 (73.8) | 0.06 | 694 (70.3) | 719 (72.8) | 0.231 | ||
| RBC transfusion | 2 (0.20) | 118 (4.5) | <0.001 | 2 (0.20) | 36 (3.60) | <0.001 | ||
| Urine output; mL/kg/h | 1.95 (0.96–3.25) | 1.27 (0.68–2.37) | <0.001 | 1.95 (0.96–3.25) | 1.30 (0.71–2.35) | <0.001 | ||
| Inotropes | 0 (0.0) | 15 (0.6) | 0.016 | 0 (0.0) | 8 (0.8) | 0.008 | ||
| Diuretics | 0 (0.0) | 21 (0.8) | 0.002 | 0 (0.0) | 4 (0.4) | 0.124 | ||
| Unmatched | Matched | |||||
|---|---|---|---|---|---|---|
| Laparoscopic Surgery (n = 987) | Open Surgery (n = 2650) | p-Value | Laparoscopic Surgery (n = 987) | Open Surgery (n = 987) | p-Value | |
| AKI | 87 (8.8) | 242 (9.1) | 0.816 | 87 (8.8) | 76 (7.7) | 0.406 |
| ICU admission | 6 (0.6) | 102 (3.8) | <0.001 | 6 (0.6) | 25 (2.5) | 0.001 |
| Postoperative complications | 2 (0.2) | 35 (1.3) | 0.001 | 2 (0.2) | 15 (1.5) | 0.002 |
| 1-year mortality | 1 (0.1) | 25 (0.9) | 0.006 | 1 (0.1) | 9 (0.9) | 0.021 |
| Hospital stay | 6.89 (3.31) | 8.78 (7.60) | <0.001 | 6.89 (3.31) | 8.61 (7.12) | <0.001 |
| Unmatched | Matched | |||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted OR (95%CI) | p-Value | Adjusted OR * (95%CI) | p-Value | Unadjusted OR ** (95%CI) | p-Value | Adjusted OR ** (95%CI) | p-Value | |
| AKI | 0.96 (0.74–1.24) | 0.767 | 0.97 (0.74–1.27) | 0.829 | 1.16 (0.84–1.59) | 0.361 | 1.17 (0.84–1.62) | 0.355 |
| Hospital stay (>14 days) | 0.38 (0.26–0.56) | <0.001 | 0.46 (0.30–0.70) | <0.001 | 0.45 (0.29–0.70) | <0.001 | 0.46 (0.29–0.74) | 0.001 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Laparoscopic surgery | 0.96 | 0.74–1.24 | 0.767 | 0.97 | 0.74–1.27 | 0.829 |
| Age | 1.01 | 1.00–1.02 | 0.015 | 1.00 | 0.99–1.02 | 0.467 |
| BMI | 1.04 | 1.00–1.08 | 0.044 | 1.04 | 1.00–1.09 | 0.035 |
| DM | 1.76 | 1.33–2.33 | <0.001 | 1.58 | 1.18–2.13 | 0.002 |
| HTN | 1.51 | 1.20–1.91 | <0.001 | 1.40 | 1.06–1.84 | 0.016 |
| ASA status | ||||||
| ASA status 1 | 1.00 | – | – | 1.00 | – | – |
| ASA status 2 | 1.25 | 0.94–1.66 | 0.124 | 0.89 | 0.64–1.24 | 0.476 |
| ASA status 3 | 2.56 | 1.36–4.79 | 0.003 | 1.37 | 0.68–2.75 | 0.379 |
| Operation time; min | 1.01 | 0.99–1.02 | 0.321 | 1.01 | 0.99–1.04 | 0.248 |
| Lowest MBP; mm/Hg | 1.00 | 0.88–1.14 | 0.997 | 1.11 | 0.96–1.27 | 0.15 |
| Total fluids; mL/kg | 1.03 | 0.96–1.10 | 0.423 | 0.90 | 0.58–1.42 | 0.666 |
| Crystalloid; mL/kg | 1.04 | 0.96–1.13 | 0.316 | 1.09 | 0.67–1.80 | 0.722 |
| Synthetic colloid use | 0.95 | 0.74–1.23 | 0.707 | 1.03 | 0.63–1.67 | 0.918 |
| RBC transfusion | 1.23 | 0.68–2.21 | 0.488 | 0.96 | 0.48–1.91 | 0.906 |
| Albumin; g·dL−1 | 0.52 | 0.42–0.66 | <0.001 | 0.57 | 0.44–0.74 | <0.001 |
| Urine output; mL/kg/h | 1.04 | 0.98–1.11 | 0.218 | 1.05 | 0.98–1.12 | 0.184 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, J.H.; Kang, S.-J.; Bang, J.-Y.; Song, J.-G. Comparison of the Effects of Laparoscopic and Open Surgery on Postoperative Acute Kidney Injury in Patients with Colorectal Cancer: Propensity Score Analysis. J. Clin. Med. 2021, 10, 1438. https://doi.org/10.3390/jcm10071438
Sim JH, Kang S-J, Bang J-Y, Song J-G. Comparison of the Effects of Laparoscopic and Open Surgery on Postoperative Acute Kidney Injury in Patients with Colorectal Cancer: Propensity Score Analysis. Journal of Clinical Medicine. 2021; 10(7):1438. https://doi.org/10.3390/jcm10071438
Chicago/Turabian StyleSim, Ji Hoon, Sa-Jin Kang, Ji-Yeon Bang, and Jun-Gol Song. 2021. "Comparison of the Effects of Laparoscopic and Open Surgery on Postoperative Acute Kidney Injury in Patients with Colorectal Cancer: Propensity Score Analysis" Journal of Clinical Medicine 10, no. 7: 1438. https://doi.org/10.3390/jcm10071438
APA StyleSim, J. H., Kang, S.-J., Bang, J.-Y., & Song, J.-G. (2021). Comparison of the Effects of Laparoscopic and Open Surgery on Postoperative Acute Kidney Injury in Patients with Colorectal Cancer: Propensity Score Analysis. Journal of Clinical Medicine, 10(7), 1438. https://doi.org/10.3390/jcm10071438