
The Operative Time for Unilateral Inguinal Hernia Repair in Children Performed with Percutaneous Internal Ring Suturing (PIRS) or Open Approach Method

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Operative Techniques
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ravi, K.; Hamer, D.B. Surgical treatment of inguinal herniae in children. Hernia 2003, 7, 137–140. [Google Scholar] [CrossRef]
- Rosenberg, J. Pediatric inguinal hernia repair—A critical appraisal. Hernia 2008, 12, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; St Peter, S.D.; Escolino, M.; Juang, D.; Settimi, A.; Holcomb, G.W., 3rd. Laparoscopic Versus Open Inguinal Hernia Repair in Pediatric Patients: A Systematic Review. J. Laparoendosc Adv. Surg. Tech. 2014, 24, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Sözübir, S.; Ekingen, G.; Şenel, U.; Kahraman, H.; Güvenç, B.H. A continuous debate on contralateral processus vaginalis: Evaluation technique and approach to patency. Hernia 2006, 10, 74–78. [Google Scholar] [CrossRef]
- Kalantari, M.; Shirgir, S.; Ahmadi, J.; Zanjani, A.; Soltani, A.E. Inguinal hernia and occurrence on the other side: A prospective analysis in Iran. Hernia 2008, 13, 41. [Google Scholar] [CrossRef] [PubMed]
- Steinau, G.; Böhm, G.; Vaassen, P.; Wenzl, T.; Schumpelick, V. Contralateral inguinal hernia in childhood and youth: Which child will develop a contralateral inguinal hernia? Hernia 2008, 12, 631. [Google Scholar] [CrossRef] [PubMed]
- Jallouli, M.; Yaich, S.; Dhaou, M.B.; Yengui, H.; Trigui, D.; Damak, J.; Mhiri, R. Are there any predictive factors of metachronous inguinal hernias in children with unilateral inguinal hernia? Hernia 2009, 13, 613. [Google Scholar] [CrossRef]
- Patkowski, D.; Chrzan, R.; Jaworski, W.; Apoznański, W.; Czernik, J. Percutaneous internal ring suturing for inguinal hernia repair in children under three months of age. Adv. Clin. Exp. Med. 2006, 15, 851–856. [Google Scholar]
- Patkowski, D.; Czernik, J.; Chrzan, R.; Jaworski, W.; Apoznański, W. Percutaneous Internal Ring Suturing: A Simple Minimally Invasive Technique for Inguinal Hernia Repair in Children. J. Laparoendosc. Adv. Surg. Tech. 2006, 16, 513–517. [Google Scholar] [CrossRef]
- Wolak, P.K.; Patkowski, D. Laparoscopic inguinal hernia repair in children using the percutaneous internal ring suturing technique-own experience. Wideochir. Inne Tech. Maloinwazyjne 2014, 9, 53–58. [Google Scholar] [CrossRef]
- Wenk, K.; Sick, B.; Sasse, T.; Moehrlen, U.; Meuli, M.; Vuille-dit-Bille, R. Incidence of metachronous contralateral inguinal hernias in children following unilateral repair–A meta-analysis of prospective studies. J. Pediatr. Surg. 2015, 50, 2147–2154. [Google Scholar] [CrossRef] [PubMed]
- Erginel, B.; Akin, M.; Yildiz, A.; Karadag, C.A.; Sever, N.; Dokucu, A.I. Percutaneous internal ring suturing a first choice laparoscopic inguinal hernia repair method in girls: A single-center study in 148 patients. Pediatr. Surg. Int. 2016, 32, 697–700. [Google Scholar] [CrossRef] [PubMed]
- Schier, F. Laparoscopic inguinal hernia repair—A prospective personal series of 542 children. J. Pediatr. Surg. 2006, 41, 1081–1084. [Google Scholar] [CrossRef] [PubMed]
- Kara, Ö.; Yıldız, A.; Toydemir, H.E.; Gökyiğit, F.M.; Akın, M.; Karadağ, Ç.A.; Sever, N.; Dokucu, A.İ. Does percutaneous internal ring suturing contain risk of ilioinguinal nerve entrapment? Pediatr. Surg. Int. 2015, 31, 485–491. [Google Scholar] [CrossRef]
- Zhang, Y.; Chao, M.; Zhang, X.; Wang, Z.; Fan, D.; Zhang, K.; Cai, Y.; Liang, C. Does the laparoscopic treatment of paediatric hydroceles represent a better alternative to the traditional open repair technique? A retrospective study of 1332 surgeries performed at two centres in China. Hernia 2018, 22, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, M.; Magrini, E.; Appignani, A. Preliminary experience with laparoscopic repair of associated inguinal and umbilical hernias in children. Hernia 2015, 19, 617–621. [Google Scholar] [CrossRef]
- Thomas, D.T.; Göcmen, K.B.; Tulgar, S.; Boga, I. Percutaneous internal ring suturing is a safe and effective method for the minimal invasive treatment of pediatric inguinal hernia: Experience with 250 cases. J. Pediatr. Surg. 2016, 51, 1330–1335. [Google Scholar] [CrossRef] [PubMed]
- Shehata, S.M.K.; El Attar, A.A.; Attia, M.A.; Hassan, A.M. Laparoscopic herniotomy in children: Prospective assessment of tertiary center experience in a developing country. Hernia 2013, 17, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhang, H.; Pu, J.; Mei, H.; Zheng, L.; Tong, Q. Laparoscopic vs. open herniorrhaphy in the management of pediatric inguinal hernia: A systemic review and meta-analysis. J. Pediatr. Surg. 2011, 46, 1824–1834. [Google Scholar] [CrossRef]
- Jessula, S.; Davies, D.A. Evidence supporting laparoscopic hernia repair in children. Curr. Opin. Pediatr. 2018, 30. [Google Scholar] [CrossRef]
- Raveenthiran, V.; Agarwal, P. Choice of Repairing Inguinal Hernia in Children: Open Versus Laparoscopy. Indian J. Pediatr. 2017, 84, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.L.; Xu, W.J.; Liu, J.B.; Huang, X.; Lv, Z.B. Comparison of laparoscopic hernia repair and open herniotomy in children: A retrospective cohort study. Hernia 2017, 21, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Li, C.; Han, Z.; Nie, X.; Lin, W. Modified single-port vs. two-port laparoscopic herniorrhaphy for children with concealed deferent duct: A retrospective study from a single institution. Hernia 2017, 21, 435–441. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
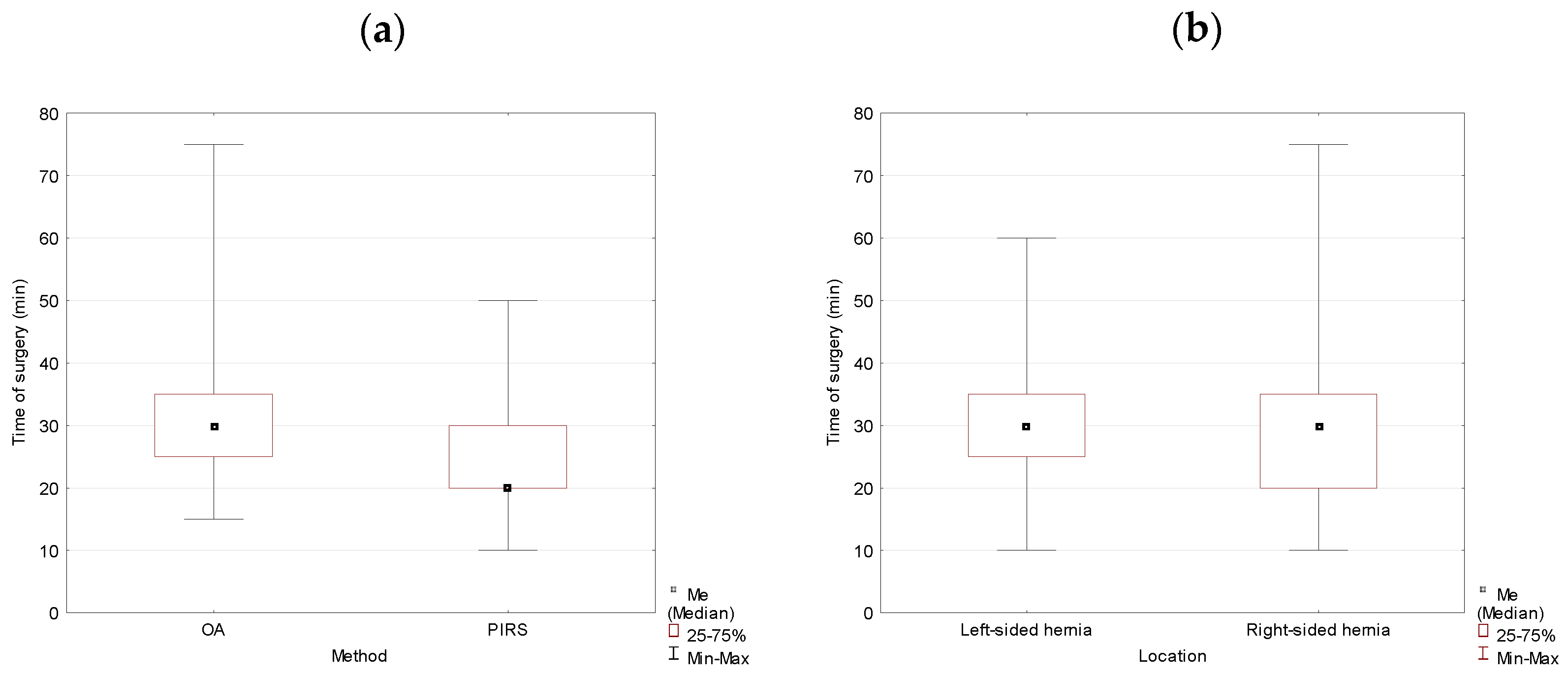
| Variable | n (%) | M (SD) Minutes | Me (IQR) Minutes | p-Value |
|---|---|---|---|---|
| Total | 878 (100.00) | 33.70 (10.52) | 30 (15) | |
| OA | 701 (79.84) | 35.13 (09.75) | 35 (10) | 0.000 * |
| PIRS | 177 (20.16) | 28.02 (11.51) | 25 (15) | |
| Left-sided hernia | 335 (38.15) | 34.57 (10.07) | 35 (10) | 0.024 * |
| Right-sided hernia | 543 (61.85) | 33.17 (10.76) | 30 (15) |
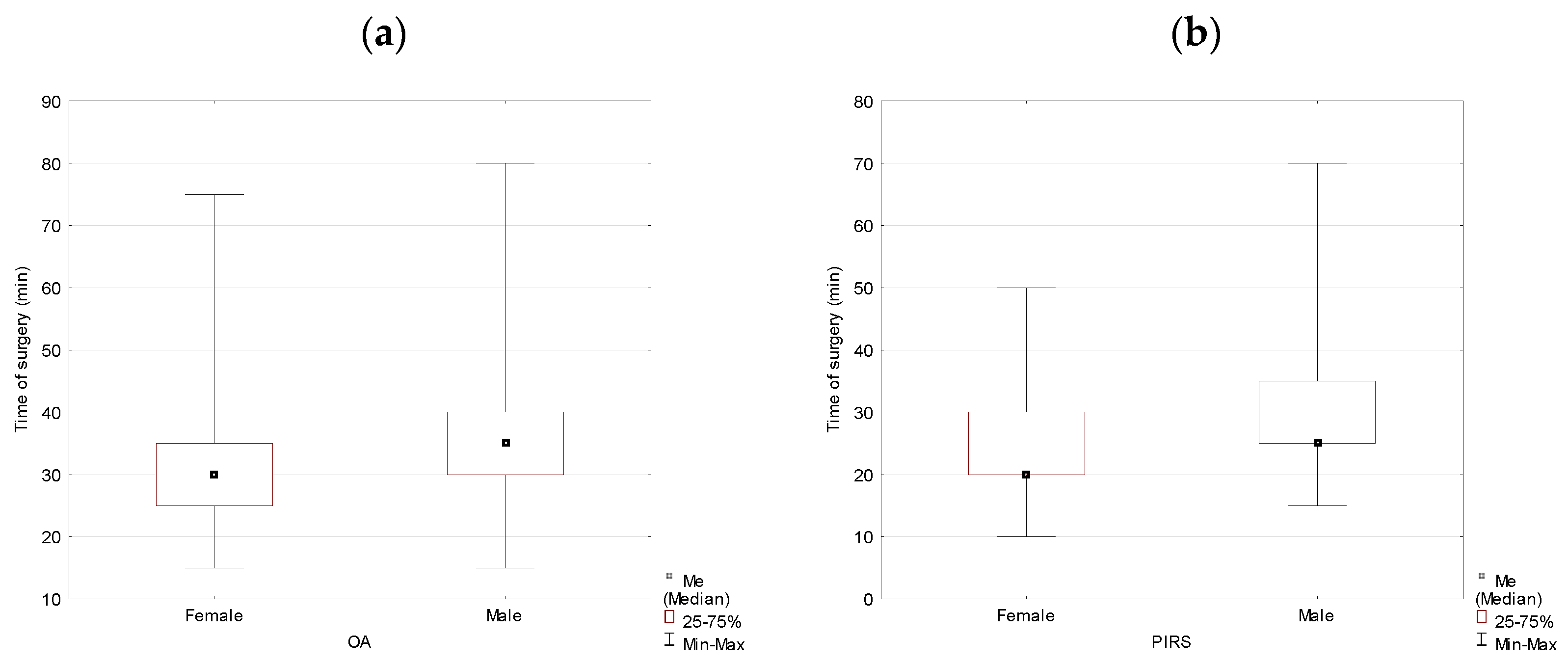
| Variable | n (%) | M(SD) Minutes | Me(IQR) Minutes | p-Value |
|---|---|---|---|---|
| OA | 701 (79.84) | 35.13 (09.75) | 35 (10) | |
| Female | 115(16.41) | 32.96 (9.99) | 30 (10) | 0.005 * |
| Male | 586 (83.59) | 35.56 (9.65) | 35 (10) | |
| PIRS | 177 (20.16) | 28.02 (11.51) | 25 (15) | |
| Female | 74 (41.81) | 24.53 (9.66) | 20 (10) | 0.000 * |
| Male | 103 (58.19) | 30.53 (12.10) | 25 (10) |
| Variable | n (%) | M(SD) Minutes | Me(IQR) Minutes | p-Value |
|---|---|---|---|---|
| Total | 189 (100.00) | 29.66 (10.67) | 30 (15) | |
| Method | ||||
| OA | 115 (60.85) | 32.96 (9.99) | 30 (10) | 0.000 * |
| PIRS | 74 (39.15) | 24.53 (9.66) | 20 (10) | |
| Location | ||||
| Left-sided hernia | 65 (34.39) | 30.69 (10.38) | 30 (10) | 0.260 nss |
| Right-sided hernia | 124 (65.61) | 29.11 (10.82) | 30 (15) |
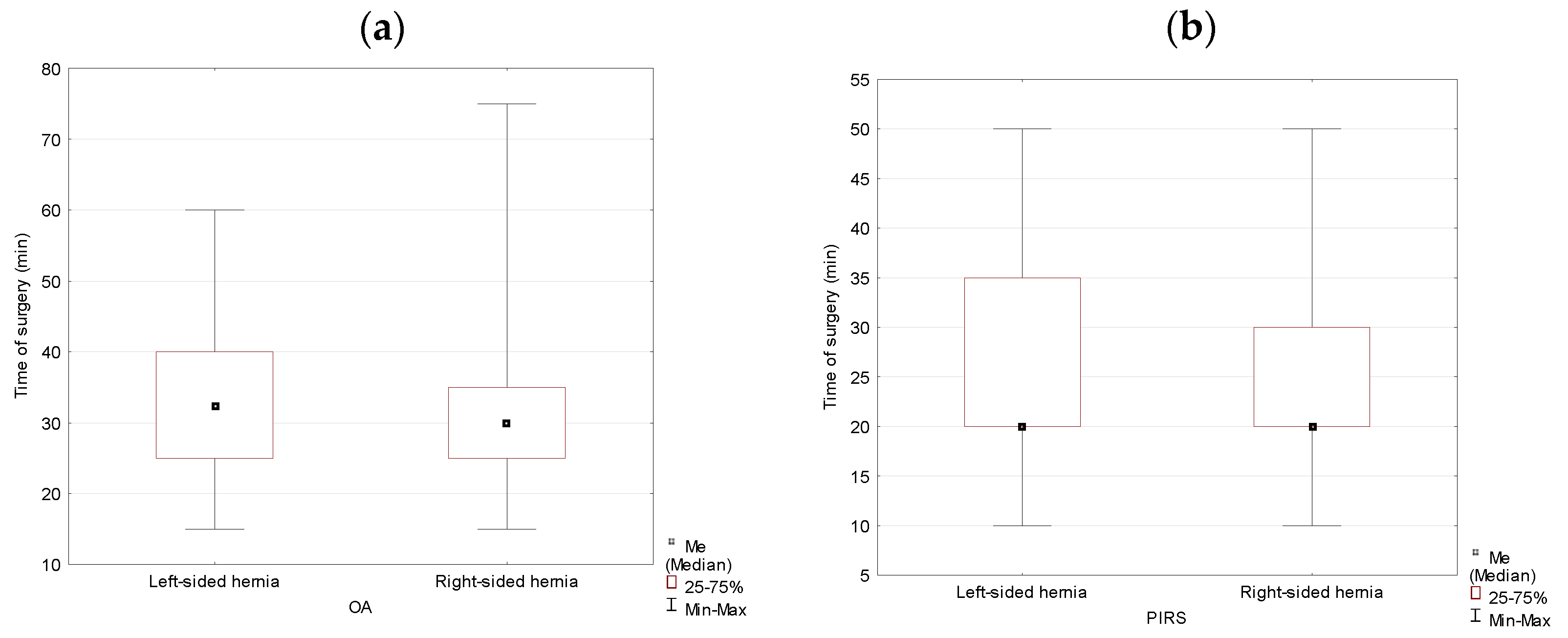
| Variable | n (%) | M (SD) Minutes | Me (IQR) Minutes | p-Value |
|---|---|---|---|---|
| OA | ||||
| Left-sided hernia | 42 (22.22) | 33.57 (9.52) | 32.5 (15) | 0.496 nss |
| Right-sided hernia | 73 (38.62) | 24.53 (9.66) | 30 (10) | |
| PIRS | ||||
| Left-sided hernia | 23 (12.17) | 25.43 (9.99) | 20 (15) | 0.538 nss |
| Right-sided hernia | 51 (26.98) | 24.12 (9.58) | 20 (10) |
| Variable | n (%) | M (SD) Minutes | Me (IQR) Minutes | p-Value |
|---|---|---|---|---|
| Total Male | 689 (100) | 34.81 (10.21) | 35 (10) | |
| Method | ||||
| OA | 586 (85.05) | 35.56 (9.65) | 35 (10) | 0.000 * |
| PIRS | 103 (14.95) | 30.53 (12.10) | 25 (10) | |
| Location | ||||
| Left-sided hernia | 270 (39.19) | 35.50 (9.78) | 35 (10) | 0.085 nss |
| Right-sided hernia | 419 (60.81) | 34.37 (10.46) | 35 (10) |
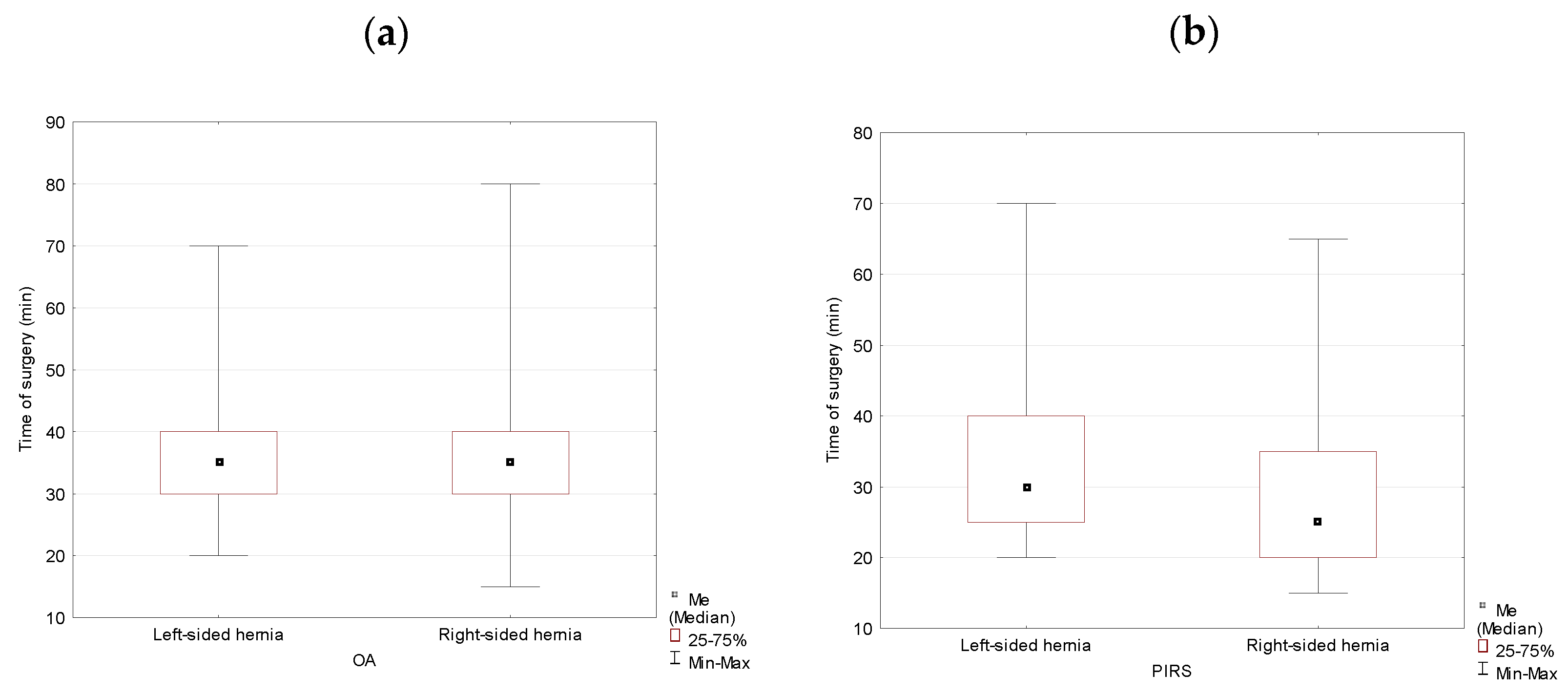
| Variable | n (%) | M (SD) Minutes | Me (IQR) Minutes | p-Value |
|---|---|---|---|---|
| OA | ||||
| Left-sided hernia | 236 (34.25) | 35.78 (9.27) | 35 (10) | 0.428 nss |
| Right-sided hernia | 350 (50.80) | 35.41 (9.91) | 35 (10) | |
| PIRS | ||||
| Left-sided hernia | 34 (4.93) | 33.53 (12.82) | 30 (15) | 0.033 * |
| Right-sided hernia | 69 (10.01) | 29.05 (11.54) | 25 (15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolak, P.K.; Strzelecka, A.; Piotrowska, A.; Dąbrowska, K.; Wolak, P.P.; Piotrowska, I.; Nowak-Starz, G. The Operative Time for Unilateral Inguinal Hernia Repair in Children Performed with Percutaneous Internal Ring Suturing (PIRS) or Open Approach Method. J. Clin. Med. 2021, 10, 1293. https://doi.org/10.3390/jcm10061293
Wolak PK, Strzelecka A, Piotrowska A, Dąbrowska K, Wolak PP, Piotrowska I, Nowak-Starz G. The Operative Time for Unilateral Inguinal Hernia Repair in Children Performed with Percutaneous Internal Ring Suturing (PIRS) or Open Approach Method. Journal of Clinical Medicine. 2021; 10(6):1293. https://doi.org/10.3390/jcm10061293
Chicago/Turabian StyleWolak, Przemyslaw Karol, Agnieszka Strzelecka, Aneta Piotrowska, Katarzyna Dąbrowska, Piotr Przemysław Wolak, Ilona Piotrowska, and Grażyna Nowak-Starz. 2021. "The Operative Time for Unilateral Inguinal Hernia Repair in Children Performed with Percutaneous Internal Ring Suturing (PIRS) or Open Approach Method" Journal of Clinical Medicine 10, no. 6: 1293. https://doi.org/10.3390/jcm10061293
APA StyleWolak, P. K., Strzelecka, A., Piotrowska, A., Dąbrowska, K., Wolak, P. P., Piotrowska, I., & Nowak-Starz, G. (2021). The Operative Time for Unilateral Inguinal Hernia Repair in Children Performed with Percutaneous Internal Ring Suturing (PIRS) or Open Approach Method. Journal of Clinical Medicine, 10(6), 1293. https://doi.org/10.3390/jcm10061293