
Gender-Based Differences by Age Range in Patients Hospitalized with COVID-19: A Spanish Observational Cohort Study

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
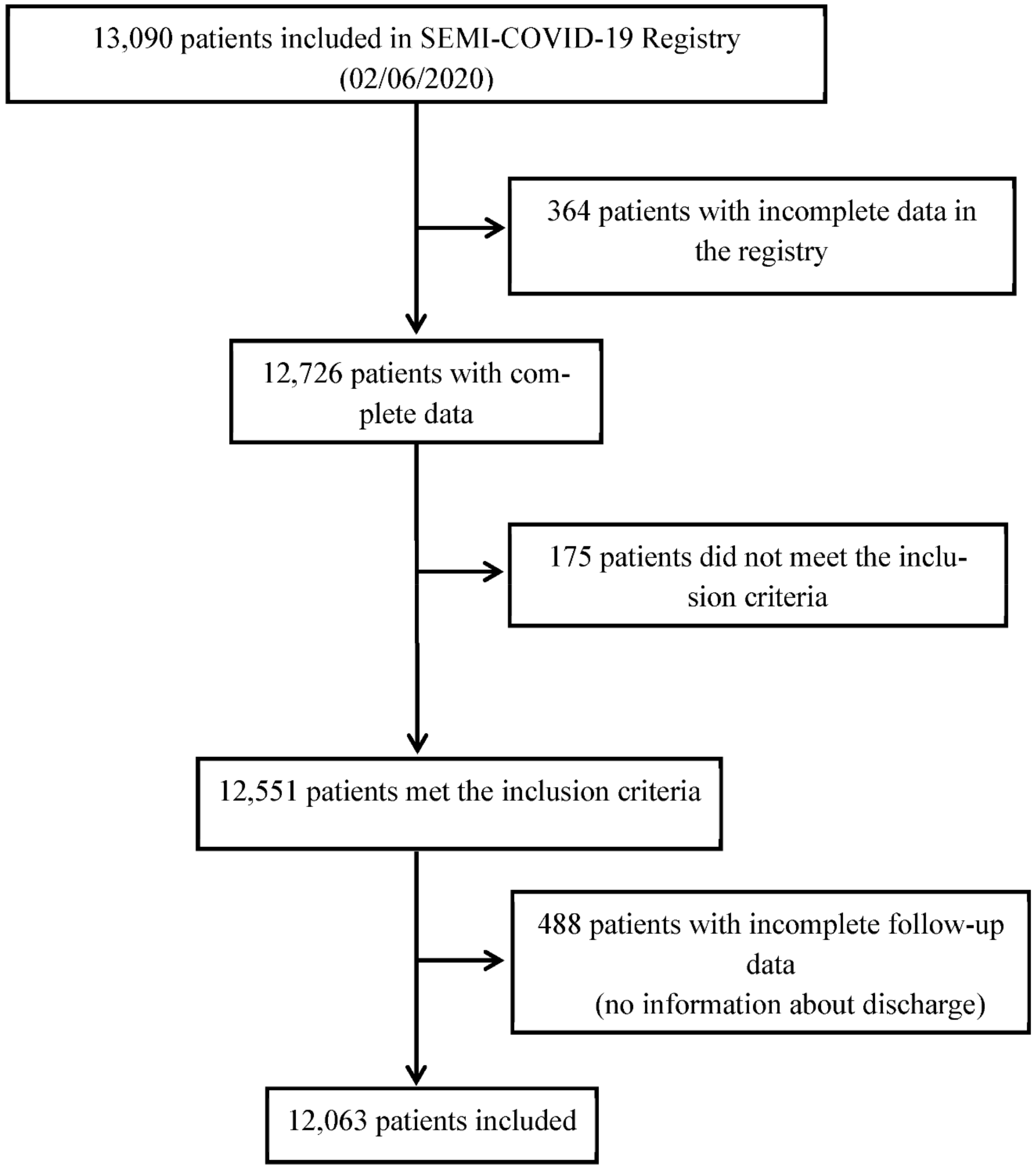
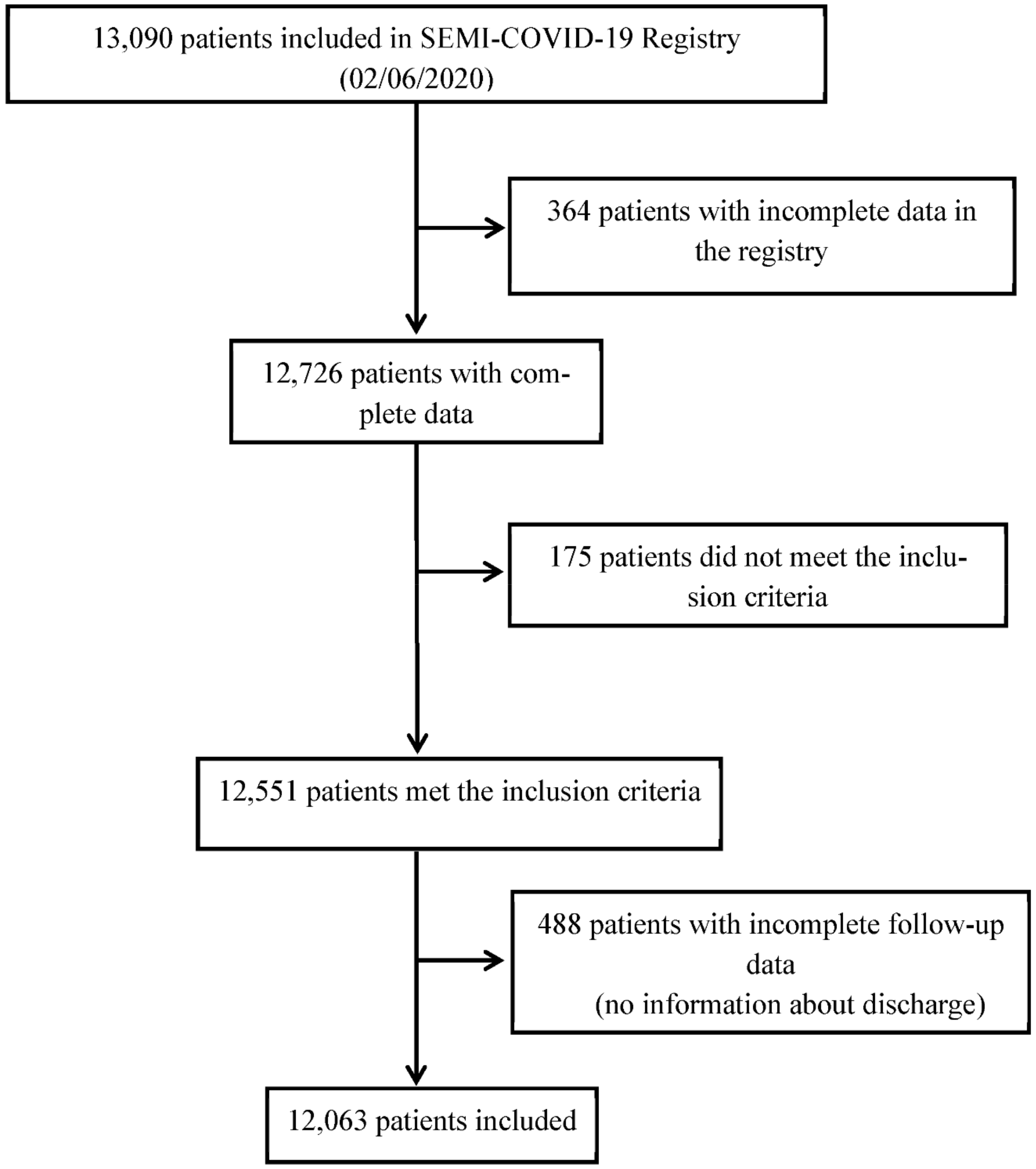
2.2. Population and Inclusion Criteria
2.3. Ethical Aspects
2.4. Data Analysis
3. Results
3.1. General Data at Baseline
3.2. Symptoms upon Admission
3.3. Treatments
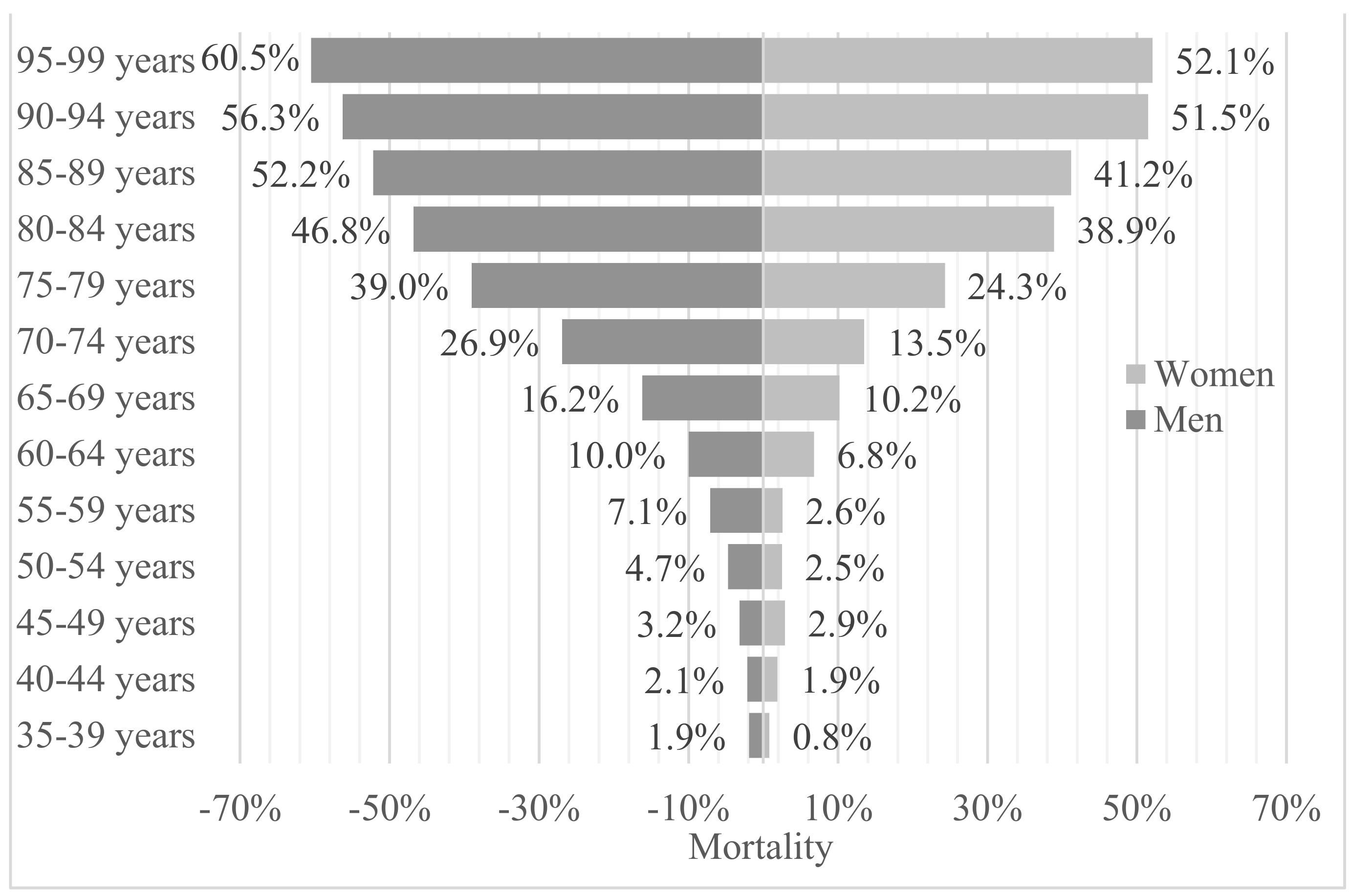
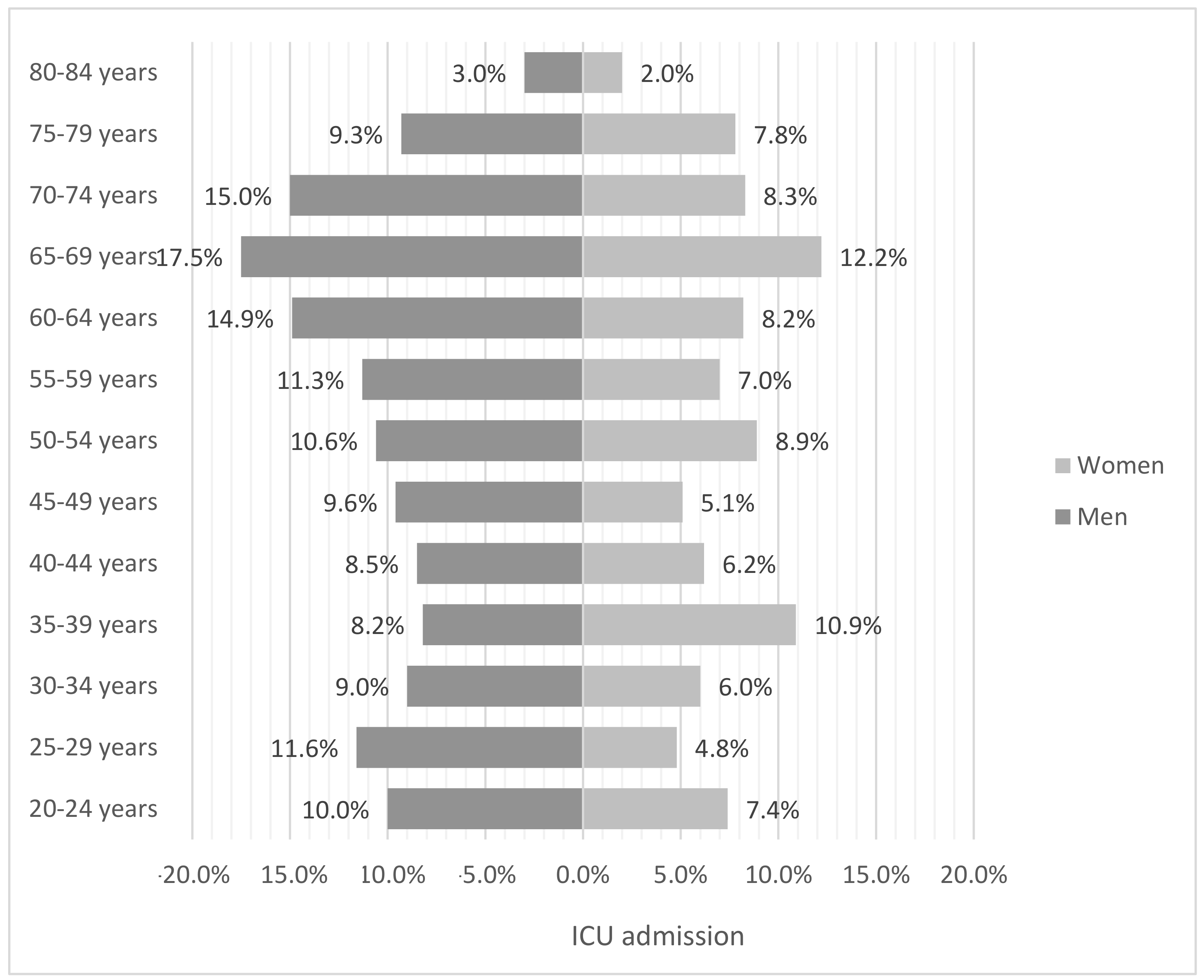
3.4. Outcomes
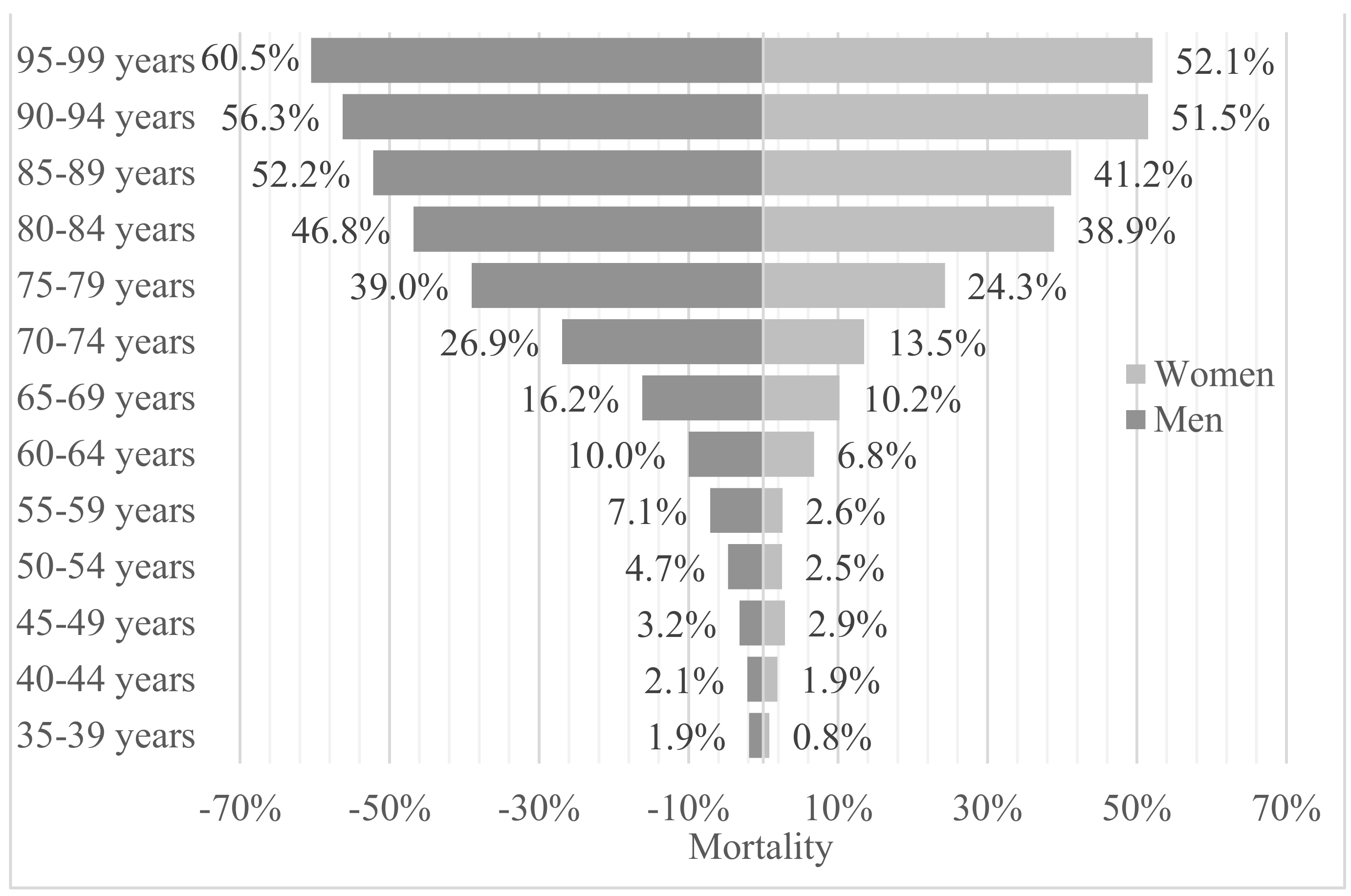
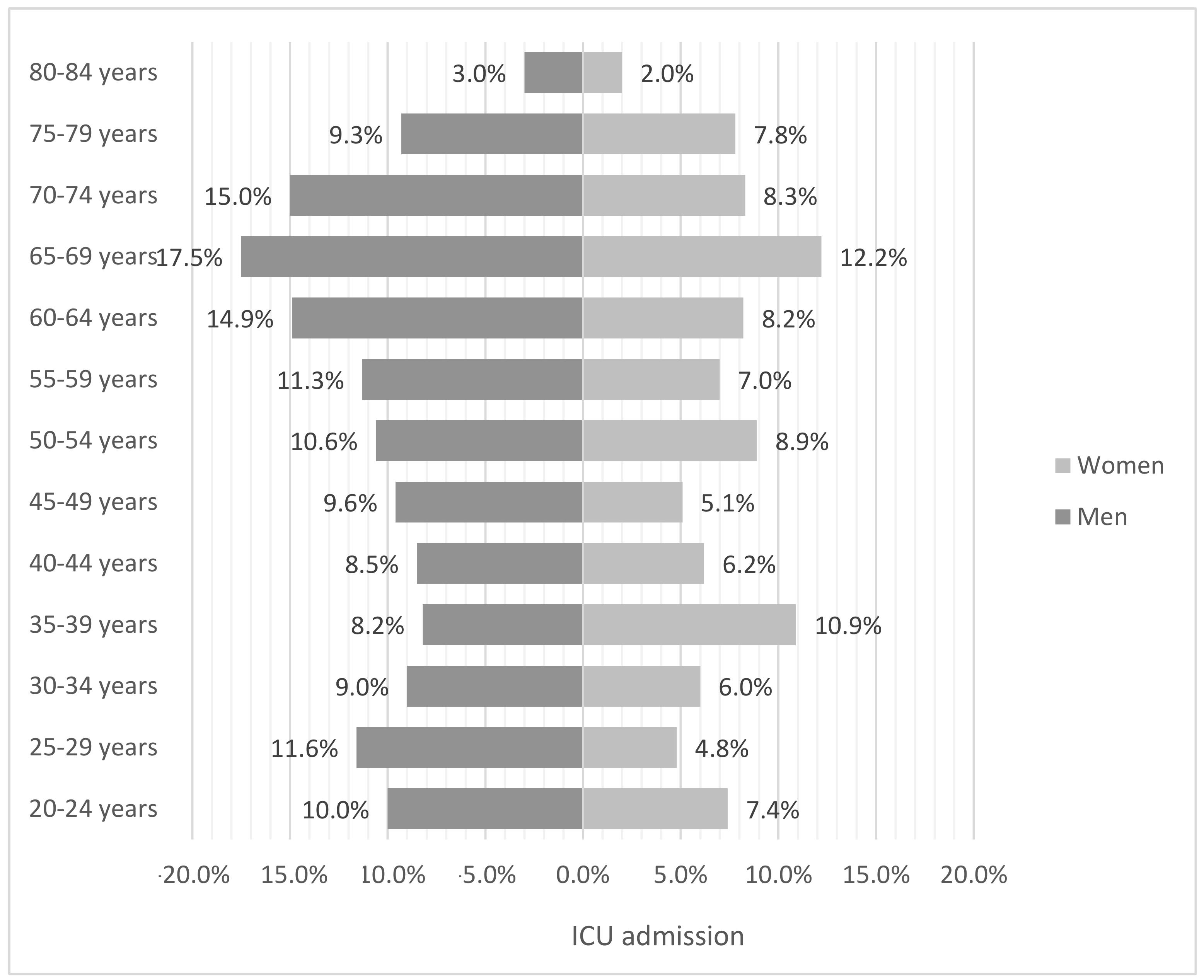
3.5. Risk Factors for Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Anxela Crestelo Vieitez | anxela90@gmail.com |
| María del Mar García Andreu | mariadelmargarciaandreu@gmail.com |
| Claudia Josa Laorden | claudiajosa@gmail.com |
| Manuel Rubio-Rivas | mrubio@bellvitgehospital.cat |
| Marcos Sánchez | marcossanferab@gmail.com |
| Neera Toledo Samaniego | neera.toledo@salud.madrid.org |
| Francisco Arnalich Fernández | farnalich@salud.madrid.org |
| Rosario Iguaran Bermudez | draiguaran@gmail.com |
| Eva Mª Fonseca Aizpuru | evamfonseca@yahoo.es |
| Juan Antonio Vargas Núñez | juanantonio.vargas@uam.es |
| Paula Maria Pesqueira Fontan | paulapesqueira@hotmail.com |
| Jorge Serrano Ballesteros | jserrano645@gmail.com |
| Santiago Jesús Freire Castro | santiago.freire.castro@sergas.es |
| Melani Pestaña Fernández | Melani.Pestana@sanitatintegral.org |
| Alba Viana García | alvigar83@gmail.com |
| Victoria Nuñez Rodriguez | mijas29@hotmail.com |
| Vicente Giner-Galvañ | ginervicgal@gmail.com |
| Francisco Javier Carrasco Sánchez | fjcarrascos@icloud.com |
| Almudena Hernández Milián | ahernandez4@hsll.es |
| Marta Cobos-Siles | mcoboss@saludcastillayleon.es |
| Jose Javier Napal Lecumberri | josejavier.napal@scsalud.es |
| Virginia Herrero García | virgyherrero@hotmail.com |
| Maria de los Reyes Pascual Pérez | cperezb@coma.es |
| Jesús Millán Núñez-Cortés | jesus.millan@salud.madrid.org |
| José Manuel Casas Rojo | jm.casas@gmail.com |
References
- Ambrosino, I.; Barbagelata, E.; Ortona, E.; Ruggieri, A.; Massiah, G.; Giannico, O.V.; Politi, C.; Moretti, A.M. Gender differences in patients with COVID-19: A narrative review. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 15 January 2021).
- Prasad, A.; Prasad, M. SARS-CoV-2: The emergence of a viral pathogen causing havoc on human existence. J. Genet. 2020, 99, 1–4. [Google Scholar] [CrossRef]
- Klein, S.L.; Morgan, R. The impact of sex and gender on immunotherapy outcomes. Biol. Sex Differ. 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Global Health 50/50: The Sex, Gender and COVID-19 Project. University College of London: c2017–2020. Available online: https://globalhealth5050.org/covid19/ (accessed on 15 January 2021).
- Casas Rojo, J.M.; Antón Santos, J.M.; Nuñez-Cortés, J.M.; Lumbreras, C.; Ramos Rincón, J.M.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.M.; Vargas-Núñez, J.A.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Network. Rev. Clin. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Huang, T.; Wang, Y.; Wang, Z.; Liang, Y.; Huang, T.; Zhang, H.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Ciminelli, G.; Garcia-Mandicó, S. COVID-19 in Italy: An Analysis of Death Registry Data. J. Public Health 2020, 42, 723–730. [Google Scholar] [CrossRef]
- European Union Agency. European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/covid-19-pandemic (accessed on 15 January 2021).
- United Kingdom. Intensive Care National Audit & Researcg Centre. Available online: https://www.icnarc.org (accessed on 15 January 2021).
- Meng, Y.; Wu, P.; Lu, W.; Liu, K.; Ma, K.; Huang, L.; Cai, J.; Zhang, H.; Qin, Y.; Sun, H.; et al. Sex-specific clinical characteristics and prognosis of coronavirus disease-19 infection in Wuhan, China: A retrospective study of 168 severe patients. PLoS Pathog. 2020, 16, e1008520. [Google Scholar] [CrossRef]
- Nasiri, M.J.; Haddadi, S.; Tahvildari, A.; Farsi, Y.; Arbabi, M.; Hasanzadeh, S.; Jamshidi, P.; Murthi, M.; Mirsaeidi, M. COVID-19 Clinical Characteristics, and Sex-Specific Risk of Mortality: Systematic Review and Meta-Analysis. Front. Med. 2020, 7, 459. [Google Scholar] [CrossRef]
- Yang, T.; Barnett, R.; Jiang, S.; Yu, L.; Xian, H.; Ying, J.; Zheng, W. Gender balance and its impact on male and female smoking rates in Chinese cities. Soc. Sci. Med. 2016, 154, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020, 108, 154262. [Google Scholar] [CrossRef]
- Borghesi, A.; Zigliani, A.; Masciullo, R.; Golemi, S.; Maculotti, P.; Farina, D.; Maroldi, R. Radiographic severity index in COVID-19 pneumonia: Relationship to age and sex in 783 Italian patients. Radiol. Med. 2020, 125, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Mesas, A.E.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Cabrera, M.A.S.; De Andrade, S.M.; Sequí-Dominguez, I.; Martínez-Vizcaíno, V. Predictors of in-hospital COVID-19 mortality: A comprehensive systematic review and meta-analysis exploring differences by age, sex and health conditions. PLoS ONE 2020, 15, e0241742. [Google Scholar] [CrossRef]
- O’Brien, J.; Du, K.Y.; Peng, C. Incidence, clinical features, and outcomes of COVID-19 in Canada: Impact of sex and age. J. Ovarian Res. 2020, 13, 1–12. [Google Scholar] [CrossRef]
- Qian, J.; Zhao, L.; Ye, R.-Z.; Li, X.-J.; Liu, Y.-L. Age-dependent Gender Differences in COVID-19 in Mainland China: Comparative Study. Clin. Infect. Dis. 2020, 71, 2488–2494. [Google Scholar] [CrossRef]
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.R.; Franssen, G.H.L.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic risk factors for COVID-19 infection, severity, ICU admission and death: A meta-analysis of 59 studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef]
- Słomka, A.; Kowalewski, M.; Żekanowska, E. Coronavirus Disease 2019 (COVID–19): A Short Review on Hematological Manifestations. Pathogens 2020, 9, 493. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, Z.; Tian, J.; Xiong, S. Risk factors associated with disease progression in a cohort of patients infected with the 2019 novel coronavirus. Ann. Palliat. Med. 2020, 9, 428–436. [Google Scholar] [CrossRef]
- Fei, Z.; Ting, Y.; Ronghui, D.; Guohui, F.; Ying, L.; Zibo, L.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar]
- Kopel, J.; Perisetti, A.; Roghani, A.; Aziz, M.; Gajendran, M.; Goyal, H. Racial and Gender-Based Differences in COVID-19. Front. Public Health 2020, 8, 418. [Google Scholar] [CrossRef]
- Pradhan, A.; Olsson, P.E. Sex differences in severity and mortality from COVID-19: Are males more vulnerable? Biol. Sex Differ. 2020, 11, 53. [Google Scholar] [CrossRef] [PubMed]
- Sama, I.; Ravera, A.; Santema, B.; Van Goor, H.; Ter Maaten, J.; Cleland, J.; Rienstra, M.; Friedrich, A.; Samani, N.; Ng, L.; et al. Circulating plasma concentrations of angiotenis-converting enzyme 2 in men and women with heart failure and effects of renin-angiotensin-aldosterone inhibitors. Eur. Heart J. 2020, 41, 1810–1817. [Google Scholar] [CrossRef]
- Haitao, T.; Vermunt, J.; Abeykoon, J.; Ghamrawi, R.; Gunaratne, M.; Jayachandran, M.; Narang, K.; Parashuram, S.; Suvakov, S.; Garovic, V. COVID-19 and Sex Differences: Mechanisms and Biomarkers. Mayo Clin. Proc. 2020, 95, 2089–2203. [Google Scholar] [CrossRef] [PubMed]
- Sriram, K.; Insel, P.A. A hypothesis for pathobiology and treatment of COVID-19: The centrality of ACE1/ACE2 imbalance. BJP 2020, 24, 177. [Google Scholar]
| Male n = 6853 (56.8%) | Female n = 5210 (43.2%) | Total n = 12063 | p-Value | |
|---|---|---|---|---|
| Age, mean (SD) | 65.7 (15.8) | 67.9 (16.9) | 66.7 (16.3) | <0.001 |
| Smoker, n (%) | 445 (6.9) | 167 (3.3) | 612 (5.3) | <0.001 |
| Obesity, n (%) | 1265 (20.5) | 1052 (22.3) | 2317 (21.2) | 0.022 |
| Arterial hypertension, n (%) | 3422 (50.0) | 2636 (50.7) | 6058 (50.3) | 0.453 |
| Dyslipidemia, n (%) | 2699 (39.5) | 2052 (39.5) | 4751 (39.5) | 0.997 |
| Atrial fibrillation, n (%) | 786 (11.5) | 554 (10.7) | 1340 (11.1) | 0.145 |
| Severe dependency, n (%) | 346 (5.1) | 516 (10.1) | 862 (7.3) | <0.001 |
| Charlson Comorbidity Index, mean (SD) | 3.57 (2.76) | 3.59 (2.60) | 3.58 (2.69) | 0.729 |
| Anxiety, n (%) | 323 (4.7) | 636 (12.3) | 959 (8.0) | <0.001 |
| Depression, n (%) | 418 (6.1) | 844 (16.3) | 1262 (10.5) | <0.001 |
| Neurodegenerative disease, n (%) | 524 (7.7) | 606 (11.7) | 1130 (9.4) | <0.001 |
| Rare disease, n (%) | 111 (1.6) | 90 (1.7) | 201 (1.7) | <0.001 |
| Dialysis, n (%) | 79 (1.2) | 43 (0.8) | 122 (1.0) | 0.109 |
| Male n = 6853 (56.8) | Female n = 5210 (43.2) | Total n = 12,063 | p-Value | |
|---|---|---|---|---|
| Symptoms | ||||
| Dry cough, n (%) | 3996 (58.5) | 3011 (58.1) | 7007 (58.3) | <0.001 |
| Productive cough, n (%) | 1152 (16.9) | 723 (13.9) | 1875 (15.6) | |
| Fever > 38°, n (%) | 4650 (68.1) | 2976 (57.4) | 7626 (63.5) | <0.001 |
| Ageusia, n (%) | 414 (6.2) | 381 (7.6) | 795 (6.8) | 0.005 |
| Anorexia, n (%) | 1267 (18.9) | 1063 (20.9) | 2330 (19.8) | 0.008 |
| Headache, n (%) | 729 (10.8) | 635 (12.4) | 1364 (11.5) | 0.007 |
| Diarrhea, n (%) | 1473 (21.7) | 1285 (24.9) | 2758 (23.1) | <0.001 |
| General malaise, n (%) | 663 (9.9) | 805 (15.9) | 1468 (12.5) | <0.001 |
| Vomiting, n (%) | 377 (5.6) | 506 (9.9) | 883 (7.4) | <0.001 |
| Abdominal pain, n (%) | 376 (5.6) | 402 (7.8) | 778 (6.5) | <0.001 |
| Arthralgia, n (%) | 2043 (30.2) | 1610 (31.5) | 3653 (30.8) | 0.158 |
| Anosmia, n (%) | 385 (5.8) | 331 (6.6) | 716 (6.1) | 0.089 |
| Asthenia, n (%) | 2878 (42.7) | 2266 (44.4) | 5144 (43.4) | 0.072 |
| Odynophagia, n (%) | 631 (9.4) | 531 (10.4) | 1162 (9.8) | 0.062 |
| Dyspnea, n (%) | 3971 (58.2) | 2960 (57.2) | 6931 (57.8) | 0.265 |
| Physical Examination | ||||
| Confusion, n (%) | 713 (10.6) | 702 (13.7) | 1415 (11.9) | <0.001 |
| Tachypnea, n (%) | 2173 (32.6) | 1505 (29.8) | 3678 (31.4) | 0.002 |
| Hypotension (SBP < 100 mmHg), n (%) | 358 (5.5) | 331 (6.7) | 689 (6.0) | 0.006 |
| Tachycardia (>100 bpm), n (%) | 1502 (22.8) | 1075 (21.5) | 2577 (22.2) | 0.103 |
| Oxygen saturation < 92%, n (%) | 2363 (35.6) | 1569 (31.1) | 3932 (33.6) | <0.001 |
| Wheezing, n (%) | 355 (5.3) | 359 (7.1) | 714 (6.1) | <0.001 |
| Rales, n (%) | 757 (11.4) | 517 (10.2) | 1274 (10.9) | 0.045 |
| Crackles, n (%) | 3504 (52.8) | 2648 (52.4) | 6157 (52.7) | 0.666 |
| Radiological Data | ||||
| Unilateral condensation, n (%) Bilateral condensation, n (%) | 1224 (18.0) 2158 (31.8) | 885 (17.3) 1526 (29.9) | 2109 (17.7) 3684 (31.0) | 0.071 0.007 |
| Unilateral interstitial infiltrates, n (%) Bilateral interstitial infiltrates, n (%) | 700 (10.3) 3647 (53.7) | 547 (10.7) 2481 (48.6) | 1247 (10.5) 6128 (51.5) | 0.194 <0.001 |
| Unilateral pleural effusion, n (%) Bilateral pleural effusion, n (%) | 192 (2.8) 89 (1.3) | 152 (3.0) 96 (1.9) | 344 (2.9) 185 (1.6) | 0.587 0.012 |
| Radiological worsening *, n (%) | 2255 (43.6) | 1343 (35.9) | 3598 (40.4) | <0.001 |
| Laboratory Data | ||||
| Lymphocytes < 1500/mm3, n (%) | 5771 (84.8) | 4101 (79.9) | 9872 (82.7) | <0.001 |
| LDH > 300 IU/L, n (%) | 3377 (56.9) | 2255 (51.1) | 5632 (54.4) | <0.001 |
| D-Dimer > 500 ng/mL, n (%) | 3148 (59.7) | 2417 (61.5) | 5565 (60.4) | 0.084 |
| Male n = 6853 (56.8) | Female n = 5210 (43.2) | Total n = 12,063 | p-Value | |
|---|---|---|---|---|
| Most Used Treatments | ||||
| Hydroxychloroquine, n (%) | 5931 (86.9) | 4353 (84.1) | 10,284 (85.7) | <0.001 |
| Lopinavir/ritonavir, n (%) | 4438 (65.1) | 2954 (57.1) | 7392 (61.7) | <0.001 |
| Remdesivir, n (%) | 42 (0.6) | 16 (0.3) | 58 (0.5) | 0.016 |
| Interferon beta-1B, n (%) | 943 (13.9) | 481 (9.4) | 1424 (11.9) | <0.001 |
| Tocilizumab, n (%) | 738 (10.9) | 324 (6.3) | 1062 (8.9) | <0.001 |
| Systemic steroids, n (%) | 2632 (38.7) | 1571 (30.5) | 4203 (35.2) | <0.001 |
| Chloroquine, n (%) | 313 (4.6) | 215 (4.2) | 528 (4.4) | 0.243 |
| Colchicine, n (%) | 60 (0.9) | 45 (0.9) | 105 (0.9) | 0.959 |
| Immunoglobulins, n (%) | 35 (0.5) | 15 (0.3) | 50 (0.4) | 0.061 |
| Anakinra, n (%) | 45 (0.7) | 15 (0.3) | 60 (0.5) | 0.005 |
| Baricitinib, n (%) | 29 (0.6) | 11 (0.1) | 40 (0.3) | 0.043 |
| Oseltamivir, n (%) | 66 (1.0) | 36 (0.7) | 102 (0.9) | 0.109 |
| Inhaled beclomethasone, n (%) | 390 (5.8) | 284 (5.6) | 674 (5.7) | 0.593 |
| Antibiotics | ||||
| Beta-lactams, n (%) | 5188 (76.2) | 3642 (70.4) | 8830 (73.7) | <0.001 |
| Macrolides, n (%) | 4223 (62.1) | 3013 (58.4) | 7236 (60.0) | <0.001 |
| Quinolones, n (%) | 894 (13.3) | 645 (12.6) | 1539 (13.0) | 0.268 |
| Respiratory Therapies | ||||
| NIMV, n (%) | 384 (5.6) | 187 (3.6) | 571 (4.8) | <0.001 |
| IMV, n (%) | 541 (7.9) | 249 (4.8) | 790 (6.6) | <0.001 |
| High flow nasal cannula, n (%) | 640 (9.4) | 368 (7.2) | 1008 (8.5) | <0.001 |
| Prone positioning, n (%) | 851 (12.5) | 370 (7.2) | 1221 (10.2) | <0.001 |
| Other Treatments During Admission | ||||
| ACEI, n (%) | 672 (9.9) | 421 (8.2) | 1093 (9.2) | 0.001 |
| ARB, n (%) | 703 (10.4) | 535 (10.4) | 1238 (10.4) | 0.965 |
| ASA, n (%) | 962 (14.3) | 581 (11.4) | 1543 (13.1) | <0.001 |
| Statins, n (%) | 967 (14.4) | 642 (12.6) | 1609 (13.6) | 0.005 |
| Vitamin K antagonists, n (%) DOAC, n (%) | 109 (1.6) 127 (1.9) | 91 (1.8) 80 (1.6) | 200 (1.7) 207 (1.7) | 0.516 0.190 |
| LMWH: Prophylactic doses, n (%) LMWH: Full anticoagulant doses, n (%) LMWH: Intermediate doses, n (%) | 4354 (64.2) 797 (11.8) 500 (7.4) | 3435 (66.7) 464 (9.0) 294 (5.7) | 7789 (65.3) 1261 (10.6) 794 (6.7) | 0.139 <0.001 <0.001 |
| Ibuprofen, n (%) Other NSAIDs, n (%) | 65 (1.0) 285 (4.2) | 46 (0.9) 215 (4.2) | 111 (0.9) 500 (4.2) | 0.771 0.934 |
| Male n = 6853 (56.8%) | Female n = 5210 (43.2%) | Total n = 12,063 | p-Value | |
|---|---|---|---|---|
| Complications | ||||
| ARDS mild, n (%) ARDS moderate, n (%) ARDS severe, n (%) | 602 (8.9) 570 (8.4) 1352 (19.9) | 380 (7.4) 311 (6.0) 722 (14.0) | 982 (8.2) 881 (7.4) 2074 (17.4) | <0.001 <0.001 <0.001 |
| Acute kidney injury, n (%) | 1082 (15.9) | 609 (11.8) | 1691 (14.1) | <0.001 |
| Bacterial pneumonia, n (%) | 806 (11.9) | 480 (9.3) | 1286 (10.8) | <0.001 |
| Multi-organic failure, n (%) | 505 (7.4) | 252 (4.9) | 757 (6.3) | <0.001 |
| Sepsis, n (%) | 481 (7.1) | 267 (5.2) | 748 (6.3) | <0.001 |
| Shock, n (%) | 366 (5.4) | 173 (3.4) | 539 (4.5) | <0.001 |
| DIC, n (%) | 89 (1.3) | 41 (0.8) | 130 (1.1) | 0.007 |
| Acute myocardial infarction, n (%) | 67 (1.0) | 28 (0.5) | 95 (0.8) | 0.007 |
| Peripheral arterial disease, n (%) | 43 (0.6) | 13 (0.3) | 56 (0.5) | 0.003 |
| Heart failure, n (%) | 398 (5.9) | 333 (6.5) | 731 (6.1) | 0.176 |
| Atrial arrhythmia, n (%) Ventricular arrhythmia, n (%) | 251 (3.7) 27 (0.4) | 179 (3.5) 9 (0.2) | 429 (3.6) 36 (0.3) | 0.462 0.031 |
| Myocarditis, n (%) | 74 (1.1) | 43 (0.8) | 117 (1.0) | 0.159 |
| Seizures, n (%) | 38 (0.3) | 34 (0.3) | 72 (0.6) | 0.484 |
| Ischemic stroke, n (%) Hemorrhagic stroke, n (%) | 36 (0.5) 7 (0.1) | 30 (0.6) 1 (0) | 66 (0.6) 8 (0.1) | 0.712 0.149 |
| VTE: DVT, n (%) VTE: PE, n (%) VTE: DVT + PE, n (%) | 29 (0.4) 103 (1.5) 9 (0.1) | 23 (0.4) 66 (1.3) 7 (0.1) | 52 (0.4) 169 (1.4) 16 (0.1) | 0.892 0.281 0.964 |
| ICU Admission Rate and in-Hospital Mortality | ||||
| ICU admission, n (%) | 684 (10.0) | 318 (6.1) | 1002 (8.3) | <0.001 |
| In-hospital mortality, n (%) | 1547 (23.1) | 962 (18.9) | 2509 (21.3) | <0.001 |
| Mortality | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (CI 95%) | p-Value | HR (CI 95%) | p-Value | |
| Gender (female) | 0.777 (0.710–0.851) | <0.001 | 0.771 (0.642–0.925) | 0.005 |
| Age | 0.920 (0.916–0.924) | <0.001 | 0.945 (0.936–0.954) | <0.001 |
| Moderate dependency Severe dependency | 5.749 (4.970–6.650) 1.203 (1.005–1.439) | <0.001 0.044 | 2.808 (2.049–3.847) 1.405 (1.004–1.967) | <0.001 0.047 |
| Charlson Comorbidity Index < 3 points | 9.759 (8.668–10.988) | <0.001 | 3.431 (2.673–4.403) | <0.001 |
| Fever > 38 °C | 0.812 (0.727–0.907) | <0.001 | 0.907 (0.724–1.135) | 0.393 |
| Dyspnea | 2.097 (1.095–2.308) | <0.001 | 1.173 (0.968–1.422) | 0.104 |
| Confusion | 6.321 (5.619–7.111) | <0.001 | 2.264 (1.781–2.877) | <0.001 |
| Tachypnea > 20 bpm | 4.049 (3.687–4.446) | <0.001 | 1.321 (1.096–1.592) | 0.003 |
| Severe ARDS | 4.757 (4.015–5.638) | <0.001 | 7.942 (6.084–10.366) | <0.001 |
| Bilateral pneumonia | 1.386 (1.216–1.579) | <0.001 | 1.168 (0.898–1.519) | 0.247 |
| Radiological worsening at 7 days of hospitalization | 5.003 (4.424–5.658) | <0.001 | 2.352 (1.956–2.828) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Josa-Laorden, C.; Crestelo-Vieitez, A.; García Andreu, M.d.M.; Rubio-Rivas, M.; Sánchez, M.; Toledo Samaniego, N.; Arnalich Fernández, F.; Iguaran Bermudez, R.; Fonseca Aizpuru, E.M.; Vargas Núñez, J.A.; et al. Gender-Based Differences by Age Range in Patients Hospitalized with COVID-19: A Spanish Observational Cohort Study. J. Clin. Med. 2021, 10, 899. https://doi.org/10.3390/jcm10050899
Josa-Laorden C, Crestelo-Vieitez A, García Andreu MdM, Rubio-Rivas M, Sánchez M, Toledo Samaniego N, Arnalich Fernández F, Iguaran Bermudez R, Fonseca Aizpuru EM, Vargas Núñez JA, et al. Gender-Based Differences by Age Range in Patients Hospitalized with COVID-19: A Spanish Observational Cohort Study. Journal of Clinical Medicine. 2021; 10(5):899. https://doi.org/10.3390/jcm10050899
Chicago/Turabian StyleJosa-Laorden, Claudia, Anxela Crestelo-Vieitez, María del Mar García Andreu, Manuel Rubio-Rivas, Marcos Sánchez, Neera Toledo Samaniego, Francisco Arnalich Fernández, Rosario Iguaran Bermudez, Eva Ma Fonseca Aizpuru, Juan Antonio Vargas Núñez, and et al. 2021. "Gender-Based Differences by Age Range in Patients Hospitalized with COVID-19: A Spanish Observational Cohort Study" Journal of Clinical Medicine 10, no. 5: 899. https://doi.org/10.3390/jcm10050899
APA StyleJosa-Laorden, C., Crestelo-Vieitez, A., García Andreu, M. d. M., Rubio-Rivas, M., Sánchez, M., Toledo Samaniego, N., Arnalich Fernández, F., Iguaran Bermudez, R., Fonseca Aizpuru, E. M., Vargas Núñez, J. A., Pesqueira Fontan, P. M., Serrano Ballesteros, J., Freire Castro, S. J., Pestaña Fernández, M., Viana García, A., Nuñez Rodriguez, V., Giner-Galvañ, V., Carrasco Sánchez, F. J., Hernández Milián, A., ... on behalf of the SEMI-COVID-19 Network. (2021). Gender-Based Differences by Age Range in Patients Hospitalized with COVID-19: A Spanish Observational Cohort Study. Journal of Clinical Medicine, 10(5), 899. https://doi.org/10.3390/jcm10050899