
Imbalance in the Levels of Angiogenic Factors in Patients with Acute and Chronic Central Serous Chorioretinopathy

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Examination
2.2. Sample Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Rijssen, T.J.; van Dijk, E.H.C.; Yzer, S.; Ohno-Matsui, K.; Keunen, J.E.E.; Schlingemann, R.O.; Sivaprasad, S.; Querques, G.; Downes, S.M.; Fauser, S.; et al. Central serous chorioretinopathy: Towards an evidence-based treatment guideline. Prog. Retin. Eye Res. 2019, 100770. [Google Scholar] [CrossRef]
- Chung, Y.-R.; Seo, E.J.; Lew, H.M.; Lee, K.H. Lack of positive effect of intravitreal bevacizumab in central serous chorioretinopathy: Meta-analysis and review. Eye Lond. Engl. 2013, 27, 1339–1346. [Google Scholar] [CrossRef]
- Sartini, F.; Figus, M.; Nardi, M.; Casini, G.; Posarelli, C. Non-resolving, recurrent and chronic central serous chorioretinopathy: Available treatment options. Eye Lond. Engl. 2019, 33, 1035–1043. [Google Scholar] [CrossRef]
- Vilela, M.; Mengue, C. Central Serous Chorioretinopathy Classification. Pharmaceuticals 2020, 14, 26. [Google Scholar] [CrossRef]
- Daruich, A.; Matet, A.; Dirani, A.; Bousquet, E.; Zhao, M.; Farman, N.; Jaisser, F.; Behar-Cohen, F. Central serous chorioretinopathy: Recent findings and new physiopathology hypothesis. Prog. Retin. Eye Res. 2015, 48, 82–118. [Google Scholar] [CrossRef] [PubMed]
- Gawęcki, M.; Jaszczuk-Maciejewska, A.; Jurska-Jaśko, A.; Kneba, M.; Grzybowski, A. Impairment of visual acuity and retinal morphology following resolved chronic central serous chorioretinopathy. BMC Ophthalmol. 2019, 19, 160. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.M.G.; Lee, W.K.; Koizumi, H.; Dansingani, K.; Lai, T.Y.Y.; Freund, K.B. Pachychoroid disease. Eye Lond. Engl. 2019, 33, 14–33. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Leong, B.C.S.; Parikh, R.; Fragiotta, S.; Freund, K.B. Association between choroidal caverns and choroidal vascular hyperpermeability in eyes with pachychoroid diseases. Retina Phila. Pa 2018, 38, 1977–1983. [Google Scholar] [CrossRef]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrzaszcz, M.; Wilanska, J.; Jager, M.J.; Markiewicz, A.; Romanowska-Dixon, B.; Sanak, M.; Kubicka-Trzaska, A. Differences in anti-endothelial and anti-retinal antibody titers: Implications for the pathohysiology of acute and chronic central serous chorioretinopathy. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2020, 71. [Google Scholar] [CrossRef]
- Cheung, C.M.G.; Lai, T.Y.Y.; Ruamviboonsuk, P.; Chen, S.-J.; Chen, Y.; Freund, K.B.; Gomi, F.; Koh, A.H.; Lee, W.-K.; Wong, T.Y. Polypoidal Choroidal Vasculopathy: Definition, Pathogenesis, Diagnosis, and Management. Ophthalmology 2018, 125, 708–724. [Google Scholar] [CrossRef]
- Kato, Y.; Oguchi, Y.; Omori, T.; Shintake, H.; Tomita, R.; Kasai, A.; Ogasawara, M.; Sugano, Y.; Itagaki, K.; Ojima, A.; et al. Complement Activation Products and Cytokines in Pachychoroid Neovasculopathy and Neovascular Age-Related Macular Degeneration. Invest. Ophthalmol. Vis. Sci. 2020, 61, 39. [Google Scholar] [CrossRef]
- Hosoda, Y.; Yoshikawa, M.; Miyake, M.; Tabara, Y.; Ahn, J.; Woo, S.J.; Honda, S.; Sakurada, Y.; Shiragami, C.; Nakanishi, H.; et al. CFH and VIPR2 as susceptibility loci in choroidal thickness and pachychoroid disease central serous chorioretinopathy. Proc. Natl. Acad. Sci. USA 2018, 115, 6261–6266. [Google Scholar] [CrossRef]
- Sartini, F.; Figus, M.; Casini, G.; Nardi, M.; Posarelli, C. Pachychoroid neovasculopathy: A type-1 choroidal neovascularization belonging to the pachychoroid spectrum-pathogenesis, imaging and available treatment options. Int. Ophthalmol. 2020, 40, 3577–3589. [Google Scholar] [CrossRef]
- Sartini, F.; Menchini, M.; Posarelli, C.; Casini, G.; Figus, M. Bullous Central Serous Chorioretinopathy: A Rare and Atypical Form of Central Serous Chorioretinopathy. A Systematic Review. Pharmaceuticals 2020, 13, 221. [Google Scholar] [CrossRef] [PubMed]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrząszcz, M.; Kubicka-Trząska, A.; Romanowska-Dixon, B.; Sanak, M. Altered plasma cytokine levels in acute and chronic central serous chorioretinopathy. Acta Ophthalmol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Shiragami, C.; Takasago, Y.; Osaka, R.; Kobayashi, M.; Ono, A.; Yamashita, A.; Hirooka, K. Clinical Features of Central Serous Chorioretinopathy With Type 1 Choroidal Neovascularization. Am. J. Ophthalmol. 2018, 193, 80–86. [Google Scholar] [CrossRef]
- Mrejen, S.; Balaratnasingam, C.; Kaden, T.R.; Bottini, A.; Dansingani, K.; Bhavsar, K.V.; Yannuzzi, N.A.; Patel, S.; Chen, K.C.; Yu, S.; et al. Long-term Visual Outcomes and Causes of Vision Loss in Chronic Central Serous Chorioretinopathy. Ophthalmology 2019, 126, 576–588. [Google Scholar] [CrossRef]
- Van Bergen, T.; Etienne, I.; Cunningham, F.; Moons, L.; Schlingemann, R.O.; Feyen, J.H.M.; Stitt, A.W. The role of placental growth factor (PlGF) and its receptor system in retinal vascular diseases. Prog. Retin. Eye Res. 2019, 69, 116–136. [Google Scholar] [CrossRef]
- Muether, P.S.; Neuhann, I.; Buhl, C.; Hermann, M.M.; Kirchhof, B.; Fauser, S. Intraocular growth factors and cytokines in patients with dry and neovascular age-related macular degeneration. Retina Phila. Pa 2013, 33, 1809–1814. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, J.; Wertheimer, C.; Wolf, A.; Liegl, R.; Priglinger, C.; Priglinger, S.; Eibl-Lindner, K. Combined VEGF and PDGF inhibition for neovascular AMD: Anti-angiogenic properties of axitinib on human endothelial cells and pericytes in vitro. Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 2017, 255, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Gavard, J.; Patel, V.; Gutkind, J.S. Angiopoietin-1 prevents VEGF-induced endothelial permeability by sequestering Src through mDia. Dev. Cell 2008, 14, 25–36. [Google Scholar] [CrossRef]
- Nagy, J.A.; Benjamin, L.; Zeng, H.; Dvorak, A.M.; Dvorak, H.F. Vascular permeability, vascular hyperpermeability and angiogenesis. Angiogenesis 2008, 11, 109–119. [Google Scholar] [CrossRef]
- Farnoodian, M.; Wang, S.; Dietz, J.; Nickells, R.W.; Sorenson, C.M.; Sheibani, N. Negative regulators of angiogenesis: Important targets for treatment of exudative AMD. Clin. Sci. Lond. Engl. 1979 2017, 131, 1763–1780. [Google Scholar] [CrossRef] [PubMed]
- Kuwano, M.; Fukushi, J.; Okamoto, M.; Nishie, A.; Goto, H.; Ishibashi, T.; Ono, M. Angiogenesis factors. Intern. Med. Tokyo Jpn. 2001, 40, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Rizzi, A.; Benagiano, V.; Ribatti, D. Angiogenesis versus arteriogenesis. Rom. J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2017, 58, 15–19. [Google Scholar]
- Branchini, L.A.; Adhi, M.; Regatieri, C.V.; Nandakumar, N.; Liu, J.J.; Laver, N.; Fujimoto, J.G.; Duker, J.S. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology 2013, 120, 1901–1908. [Google Scholar] [CrossRef] [PubMed]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrząszcz, M.; Żuber-Łaskawiec, K.; Sanak, M.; Romanowska-Dixon, B. Quality of life of patients with central serous chorioretinopathy—A major cause of vision threat among middle-aged individuals. Arch. Med. Sci. 2020, 16. [Google Scholar] [CrossRef]
- El-Asrar, M.A.; Elbarbary, N.S.; Ismail, E.A.R.; Bakr, A.A. Circulating angiopoietin-2 levels in children and adolescents with type 1 diabetes mellitus: Relation to carotid and aortic intima-media thickness. Angiogenesis 2016, 19, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, D.-Y.; Park, D.Y.; Park, I.; Chang, W.; Nakaoka, Y.; Komuro, I.; Yoo, O.-J.; Koh, G.Y. Angiopoietin-1 suppresses choroidal neovascularization and vascular leakage. Invest. Ophthalmol. Vis. Sci. 2014, 55, 2191–2199. [Google Scholar] [CrossRef]
- Terao, N.; Koizumi, H.; Kojima, K.; Yamagishi, T.; Nagata, K.; Kitazawa, K.; Yamamoto, Y.; Yoshii, K.; Hiraga, A.; Toda, M.; et al. Association of Upregulated Angiogenic Cytokines With Choroidal Abnormalities in Chronic Central Serous Chorioretinopathy. Invest. Ophthalmol. Vis. Sci. 2018, 59, 5924–5931. [Google Scholar] [CrossRef]
- Ngok, S.P.; Geyer, R.; Liu, M.; Kourtidis, A.; Agrawal, S.; Wu, C.; Seerapu, H.R.; Lewis-Tuffin, L.J.; Moodie, K.L.; Huveldt, D.; et al. VEGF and Angiopoietin-1 exert opposing effects on cell junctions by regulating the Rho GEF Syx. J. Cell Biol. 2012, 199, 1103–1115. [Google Scholar] [CrossRef]
- Peters, S.; Cree, I.A.; Alexander, R.; Turowski, P.; Ockrim, Z.; Patel, J.; Boyd, S.R.; Joussen, A.M.; Ziemssen, F.; Hykin, P.G.; et al. Angiopoietin modulation of vascular endothelial growth factor: Effects on retinal endothelial cell permeability. Cytokine 2007, 40, 144–150. [Google Scholar] [CrossRef]
- Schubert, C.; Pryds, A.; Zeng, S.; Xie, Y.; Freund, K.B.; Spaide, R.F.; Merriam, J.C.; Barbazetto, I.; Slakter, J.S.; Chang, S.; et al. Cadherin 5 is regulated by corticosteroids and associated with central serous chorioretinopathy. Hum. Mutat. 2014, 35, 859–867. [Google Scholar] [CrossRef]
- Dewerchin, M.; Carmeliet, P. PlGF: A multitasking cytokine with disease-restricted activity. Cold Spring Harb. Perspect. Med. 2012, 2. [Google Scholar] [CrossRef]
- van Royen, N.; Piek, J.J.; Buschmann, I.; Hoefer, I.; Voskuil, M.; Schaper, W. Stimulation of arteriogenesis; a new concept for the treatment of arterial occlusive disease. Cardiovasc. Res. 2001, 49, 543–553. [Google Scholar] [CrossRef]
- Spaide, R.F. Optical Coherence Tomography Angiography Signs of Vascular Abnormalization With Antiangiogenic Therapy for Choroidal Neovascularization. Am. J. Ophthalmol. 2015, 160, 6–16. [Google Scholar] [CrossRef]
- Saito, M.; Saito, W.; Hirooka, K.; Hashimoto, Y.; Mori, S.; Noda, K.; Ishida, S. Pulse Waveform Changes in Macular Choroidal Hemodynamics With Regression of Acute Central Serous Chorioretinopathy. Invest. Ophthalmol. Vis. Sci. 2015, 56, 6515–6522. [Google Scholar] [CrossRef]
- Lim, J.W.; Kim, M.U.; Shin, M.-C. Aqueous humor and plasma levels of vascular endothelial growth factor and interleukin-8 in patients with central serous chorioretinopathy. Retina Phila. Pa 2010, 30, 1465–1471. [Google Scholar] [CrossRef]
- Shin, M.C.; Lim, J.W. Concentration of cytokines in the aqueous humor of patients with central serous chorioretinopathy. Retina Phila. Pa 2011, 31, 1937–1943. [Google Scholar] [CrossRef]
- Ji, S.; Wei, Y.; Chen, J.; Tang, S. Clinical efficacy of anti-VEGF medications for central serous chorioretinopathy: A meta-analysis. Int. J. Clin. Pharm. 2017, 39, 514–521. [Google Scholar] [CrossRef]
- Spaide, R.F.; Koizumi, H.; Pozzoni, M.C.; Pozonni, M.C. Enhanced depth imaging spectral-domain optical coherence tomography. Am. J. Ophthalmol. 2008, 146, 496–500. [Google Scholar] [CrossRef]
- Żuber-Łaskawiec, K.; Kubicka-Trząska, A.; Karska-Basta, I.; Pociej-Marciak, W.; Romanowska-Dixon, B. Non-Responsiveness and Tachyphylaxis to Anti-Vascular Endothelial Growth Factor Treatment in Naive Patients with Exudative Age-Related Macular Degeneration. Available online: https://pubmed.ncbi.nlm.nih.gov/32009630/ (accessed on 2 December 2020).
- Sacconi, R.; Tomasso, L.; Corbelli, E.; Carnevali, A.; Querques, L.; Casati, S.; Bandello, F.; Querques, G. Early response to the treatment of choroidal neovascularization complicating central serous chorioretinopathy: A OCT-angiography study. Eye Lond. Engl. 2019, 33, 1809–1817. [Google Scholar] [CrossRef] [PubMed]
- Schierling, W.; Troidl, K.; Troidl, C.; Schmitz-Rixen, T.; Schaper, W.; Eitenmüller, I.K. The role of angiogenic growth factors in arteriogenesis. J. Vasc. Res. 2009, 46, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Behzadian, M.A.; Windsor, L.J.; Ghaly, N.; Liou, G.; Tsai, N.-T.; Caldwell, R.B. VEGF-induced paracellular permeability in cultured endothelial cells involves urokinase and its receptor. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2003, 17, 752–754. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Dreffs, A.; Díaz-Coránguez, M.; Runkle, E.A.; Gardner, T.W.; Chiodo, V.A.; Hauswirth, W.W.; Antonetti, D.A. Occludin S490 Phosphorylation Regulates Vascular Endothelial Growth Factor-Induced Retinal Neovascularization. Am. J. Pathol. 2016, 186, 2486–2499. [Google Scholar] [CrossRef] [PubMed]
- Murakami, T.; Frey, T.; Lin, C.; Antonetti, D.A. Protein kinase cβ phosphorylates occludin regulating tight junction trafficking in vascular endothelial growth factor-induced permeability in vivo. Diabetes 2012, 61, 1573–1583. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.-H.; Park, S.W.; Kim, K.-J.; Bae, J.-S.; Lee, E.H.; Paek, S.H.; Kim, S.U.; Ye, S.; Kim, J.-H.; Cho, C.-H. Endothelial STAT3 Activation Increases Vascular Leakage Through Downregulating Tight Junction Proteins: Implications for Diabetic Retinopathy. J. Cell. Physiol. 2017, 232, 1123–1134. [Google Scholar] [CrossRef]
- Mesquida, M.; Leszczynska, A.; Llorenç, V.; Adán, A. Interleukin-6 blockade in ocular inflammatory diseases. Clin. Exp. Immunol. 2014, 176, 301–309. [Google Scholar] [CrossRef]
- Chen, Z.; Rubin, J.; Tzima, E. Role of PECAM-1 in arteriogenesis and specification of preexisting collaterals. Circ. Res. 2010, 107, 1355–1363. [Google Scholar] [CrossRef]
- Takeda, Y.; Costa, S.; Delamarre, E.; Roncal, C.; Leite de Oliveira, R.; Squadrito, M.L.; Finisguerra, V.; Deschoemaeker, S.; Bruyère, F.; Wenes, M.; et al. Macrophage skewing by Phd2 haplodeficiency prevents ischaemia by inducing arteriogenesis. Nature 2011, 479, 122–126. [Google Scholar] [CrossRef]
- Galis, Z.S.; Sukhova, G.K.; Libby, P. Microscopic localization of active proteases by in situ zymography: Detection of matrix metalloproteinase activity in vascular tissue. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 1995, 9, 974–980. [Google Scholar] [CrossRef]
- Humar, R.; Zimmerli, L.; Battegay, E. Angiogenesis and hypertension: An update. J. Hum. Hypertens. 2009, 23, 773–782. [Google Scholar] [CrossRef]
- Pociej-Marciak, W.; Karska-Basta, I.; Kuźniewski, M.; Kubicka-Trząska, A.; Romanowska-Dixon, B. Sudden visual deterioration as a first symptom of chronic kidney failure. Case Rep Ophtalmol. 2015, 28, 394–400. [Google Scholar] [CrossRef]
- Kniggendorf, V.F.; Novais, E.A.; Kniggendorf, S.L.; Xavier, C.; Cole, E.D.; Regatieri, C.V. Effect of intravitreal anti-VEGF on choroidal thickness in patients with diabetic macular edema using spectral domain OCT. Arq. Bras. Oftalmol. 2016, 79, 155–158. [Google Scholar] [CrossRef]
- Kim, D.Y.; Joe, S.G.; Yang, H.S.; Lee, J.Y.; Kim, J.-G.; Yoon, Y.H. Subfoveal choroidal thickness changes in treated idiopathic central serous chorioretinopathy and their association with recurrence. Retina Phila. Pa 2015, 35, 1867–1874. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Chronic CSC (n = 30) | Acute CSC (n = 30) | Controls (n = 20) | p Value |
|---|---|---|---|---|
| Male sex, n (%) | 24 (80.0) | 25 (83.3) | 11 (55.0) | 0.056 1 |
| Age, y | 44.5 (6.1) | 42.7 (9.9) | 39.2 (7.4) | 0.078 2 |
| Smoking (current, former), n (%) | 8 (26.7) | 7 (23.3) | 7 (35.0) | 0.658 3 |
| Hypertension, n (%) | 6 (20.0) | 11 (36.7) | 4 (20.0) | 0.26 4 |
| Hashimoto thyroiditis, n (%) | 2 (6) | 1 (3) | 0 (0) | 0.781 |
| Helicobacter pylori infection, n (%) | 6 (20) | 0 (0) | 0 (0) | 0.007 |
| Gout, n (%) | 2 (6) | 1 (3) | 0 (0) | 0.781 |
| Ischemic heart disease, n (%) | 1 (3) | 1 (3) | 0 (0) | 1.000 |
| Variable | Chronic CSC (n = 30) | Acute CSC (n = 30) | Controls (n = 20) | p Value | |
|---|---|---|---|---|---|
| CT, µm | 406.1 (88.1) | 421.5 (85.3) | 317.4 (61.4) | <0.001 1 | |
| Affected eye, n (%) | Right | 10 (33.3) | 14 (46.7) | - | 0.225 2 |
| Left | 12 (40) | 13 (43.3) | - | ||
| Both | 8 (26.7) | 3 (10.0) | - | ||
| BCVA(logMAR), n (%) | 0.3< * ≤0.0 | 23 (76.7) | 20 (66.7) | 20 (100.0) | 0.017 3 |
| 1.0≤ * ≤0.3 | 7 (23.3) | 10 (33.3) | 0 | ||
| Angiogenic Factor, pg/mL | Acute CSC (n = 30) | Chronic CSC (n = 30) | Controls (n = 20) | p Value |
|---|---|---|---|---|
| PEDF | 94.99 (47.91–200.92) | 82.89 (45.73–155.99) | 74.12 (54.45–159.35) | 0.80 1 |
| FGF-basic | 48.97 (2.74) | 48.97 (4.71) | 50.49 (3.11) | 0.28 2 |
| Endostatin | 18,009.97 (4466.25) | 18,241.17 (4524.54) | 16,854.20 (3182.28) | 0.49 3 |
| FGF-acid | 127.40 (7.92) | 125.20 (8.11) | 126.08 (8.20) | 0.58 4 |
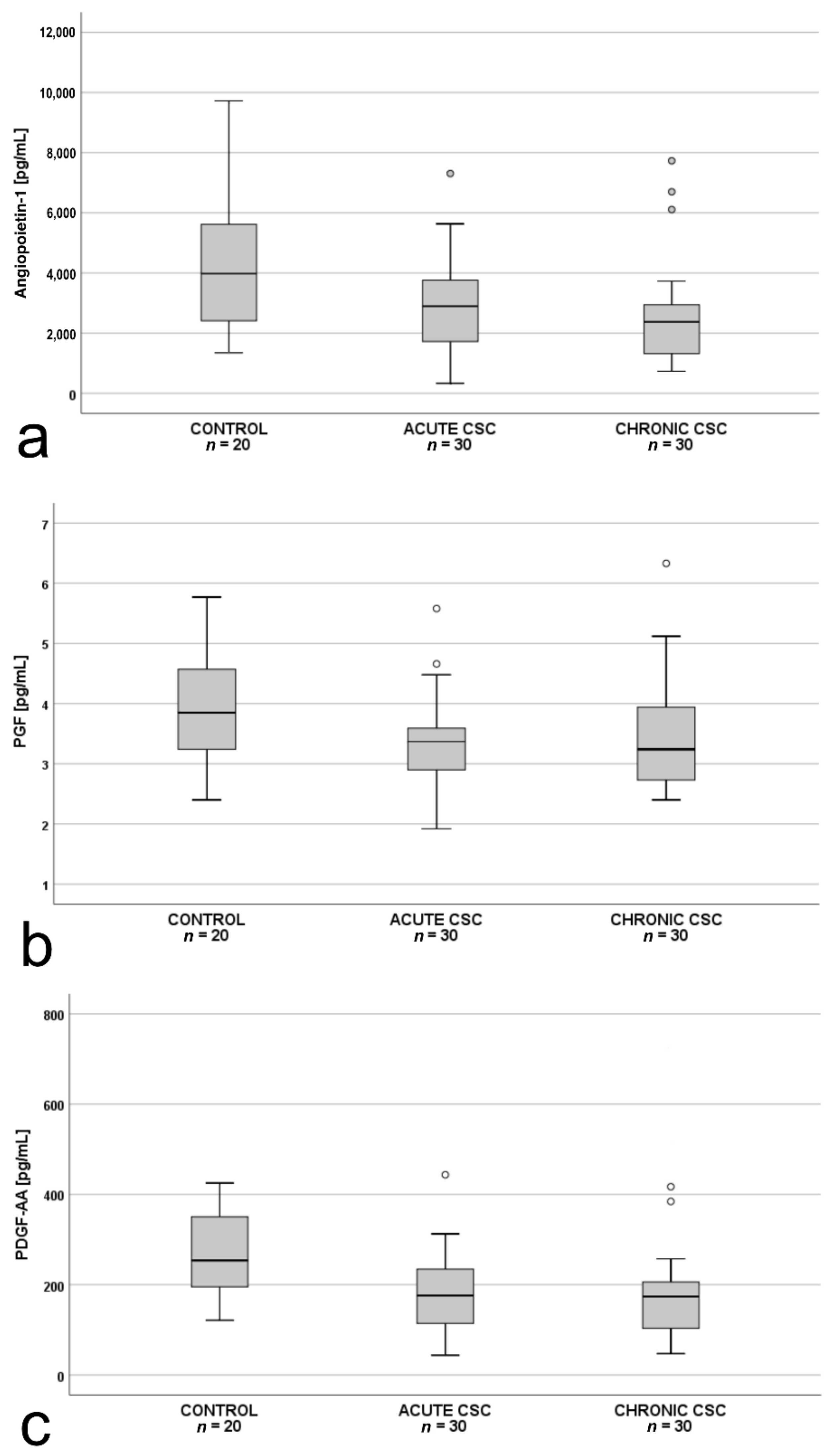
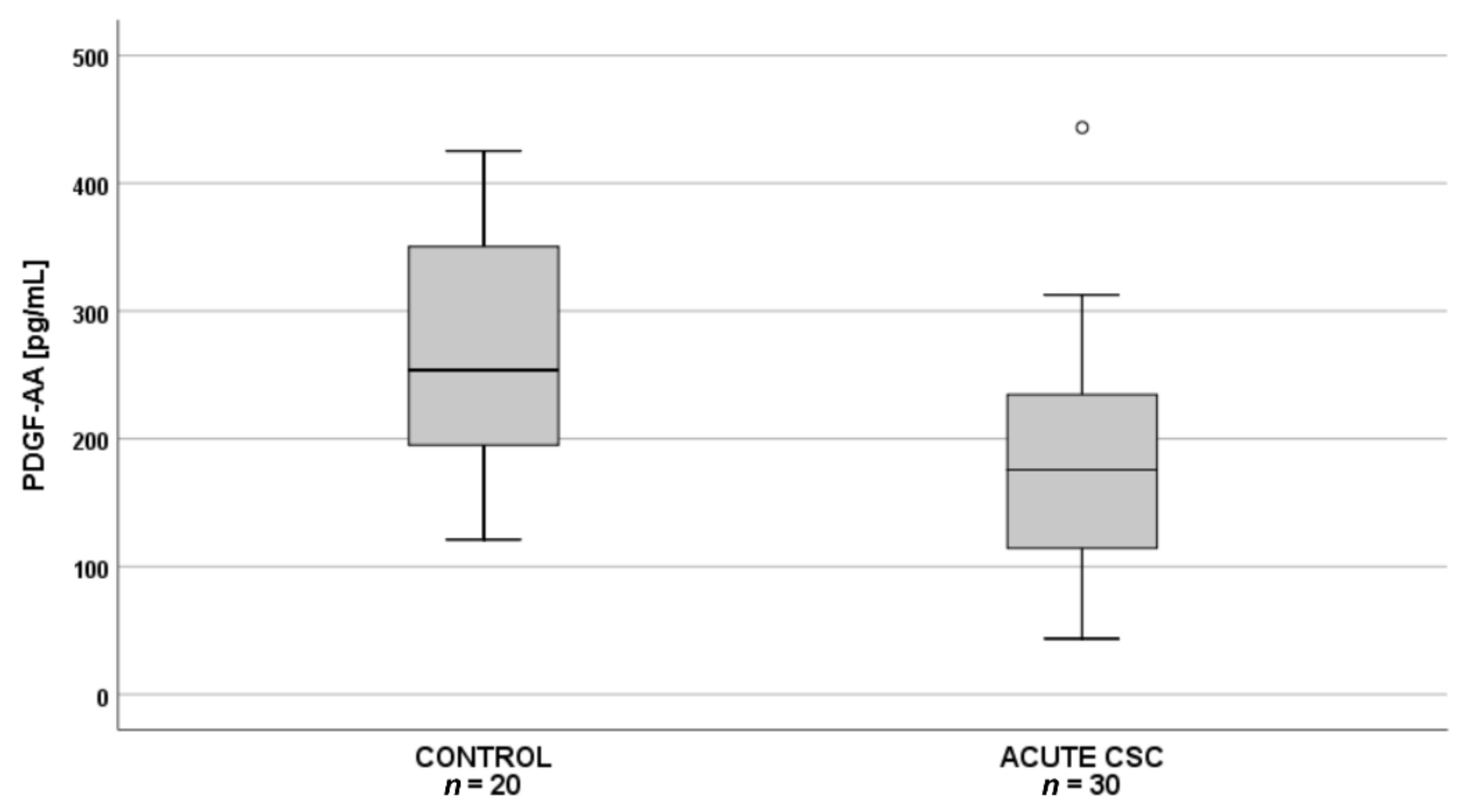
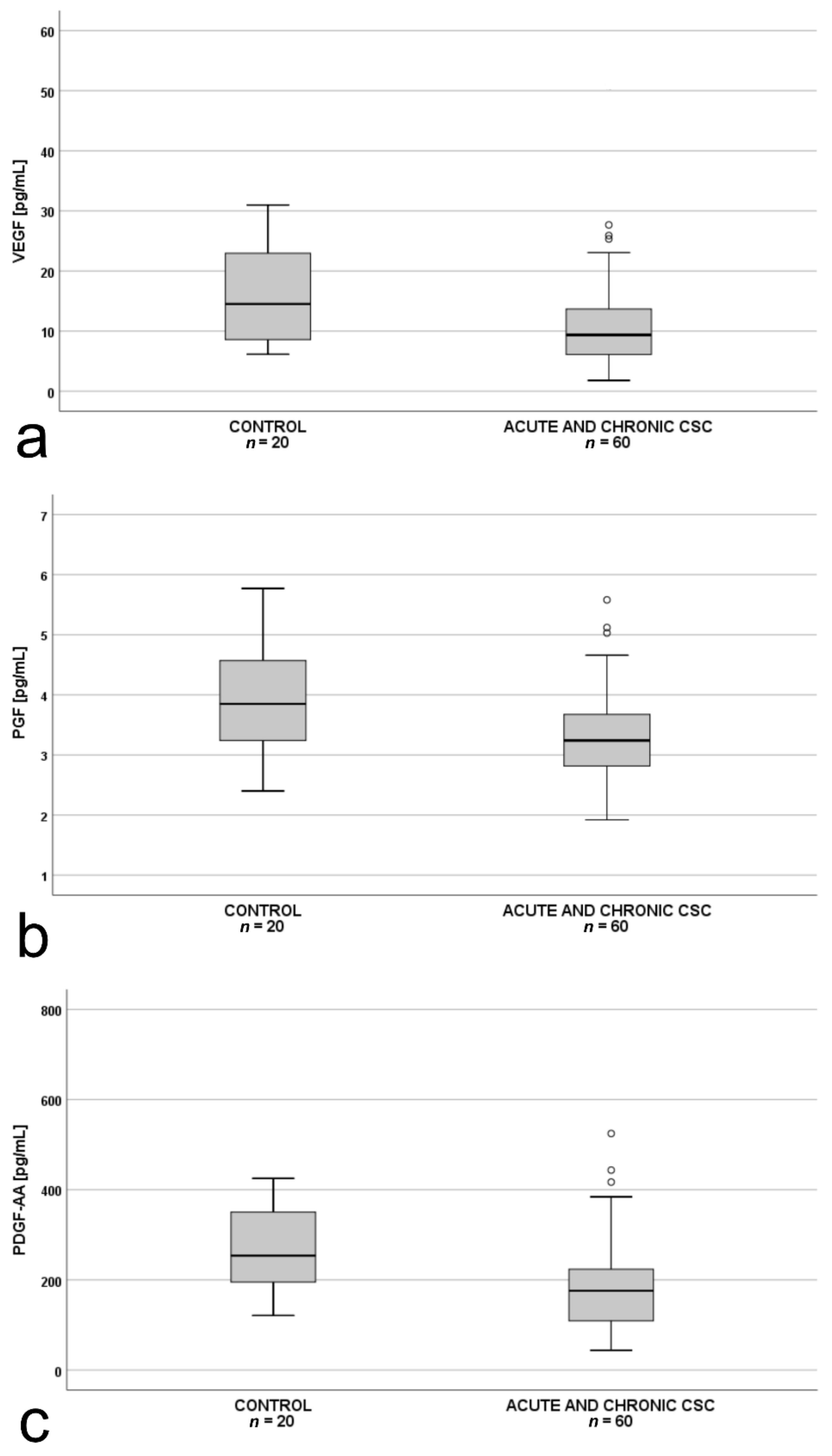
| PDGF-AA | 179.04 (87.66) | 200.23 (143.25) | 265.19 (97.72) | 0.03 5 |
| PlGF | 3.40 (0.76) | 3.44 (0.91) | 3.99 (0.96) | 0.045 6 |
| VEGF-D | 78.62 (5.88) | 76.93 (9.66) | 77.94 (6.99) | 0.70 7 |
| Trombospondin-2 | 4661.00 (4070.00–6002.00) | 5478.00 (5420.00–6933.00) | 5898.00 (4750.00–6857.00) | 0.07 8 |
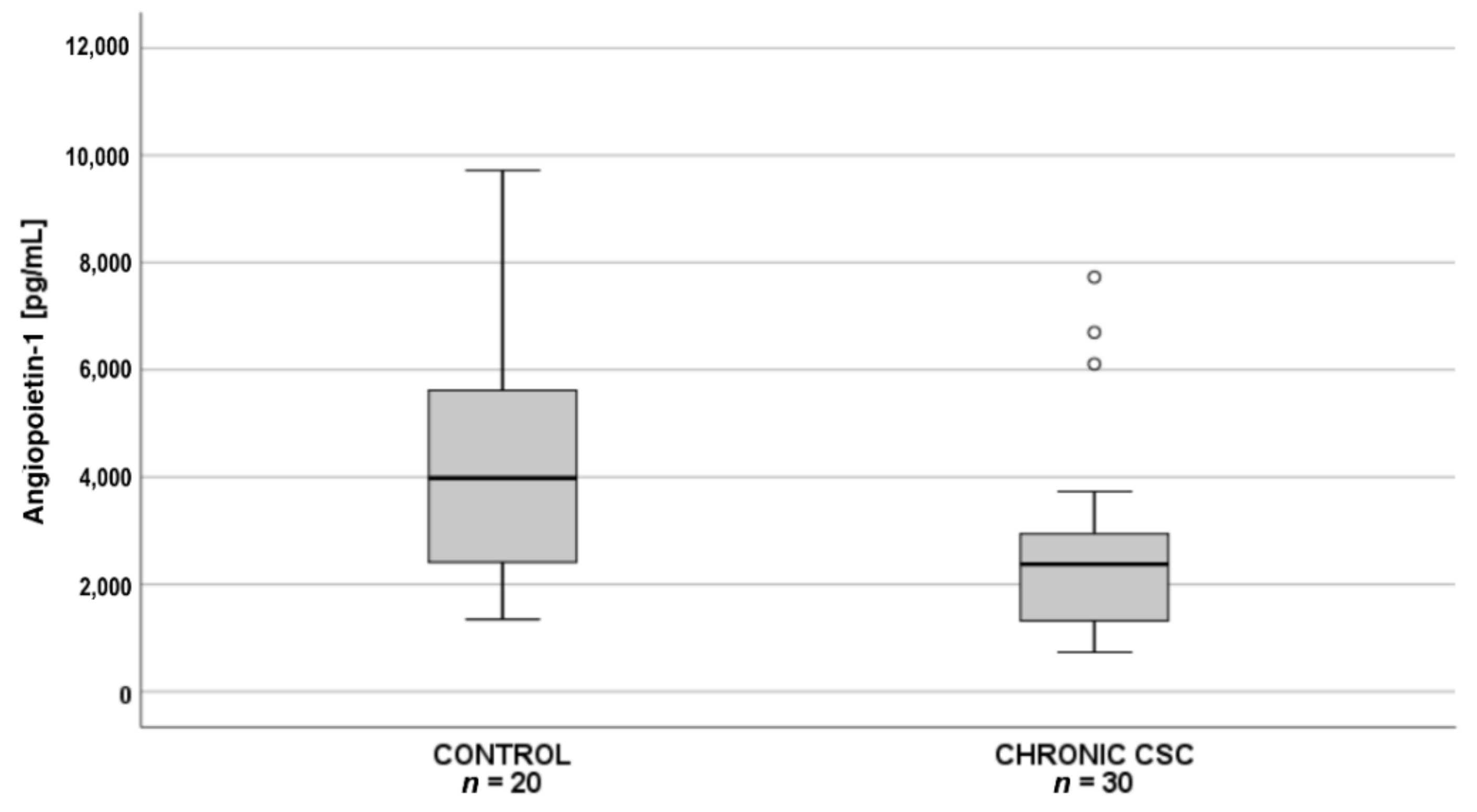
| Angiopoietin-1 | 2894.00 (1722.00–3760.00) | 2373.00 (1321.00–2943.00) | 3982.00 (2411.00–5617.00) | 0.01 9 |
| VEGF | 8.80 (6.00-14.40) | 9.40 (6.60-13.10) | 14.50 (8.60-23.00) | 0.07 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karska-Basta, I.; Pociej-Marciak, W.; Chrząszcz, M.; Kubicka-Trząska, A.; Dębicka-Kumela, M.; Gawęcki, M.; Romanowska-Dixon, B.; Sanak, M. Imbalance in the Levels of Angiogenic Factors in Patients with Acute and Chronic Central Serous Chorioretinopathy. J. Clin. Med. 2021, 10, 1087. https://doi.org/10.3390/jcm10051087
Karska-Basta I, Pociej-Marciak W, Chrząszcz M, Kubicka-Trząska A, Dębicka-Kumela M, Gawęcki M, Romanowska-Dixon B, Sanak M. Imbalance in the Levels of Angiogenic Factors in Patients with Acute and Chronic Central Serous Chorioretinopathy. Journal of Clinical Medicine. 2021; 10(5):1087. https://doi.org/10.3390/jcm10051087
Chicago/Turabian StyleKarska-Basta, Izabella, Weronika Pociej-Marciak, Michał Chrząszcz, Agnieszka Kubicka-Trząska, Magdalena Dębicka-Kumela, Maciej Gawęcki, Bożena Romanowska-Dixon, and Marek Sanak. 2021. "Imbalance in the Levels of Angiogenic Factors in Patients with Acute and Chronic Central Serous Chorioretinopathy" Journal of Clinical Medicine 10, no. 5: 1087. https://doi.org/10.3390/jcm10051087
APA StyleKarska-Basta, I., Pociej-Marciak, W., Chrząszcz, M., Kubicka-Trząska, A., Dębicka-Kumela, M., Gawęcki, M., Romanowska-Dixon, B., & Sanak, M. (2021). Imbalance in the Levels of Angiogenic Factors in Patients with Acute and Chronic Central Serous Chorioretinopathy. Journal of Clinical Medicine, 10(5), 1087. https://doi.org/10.3390/jcm10051087