
Steroid-Resistant Graves’ Orbitopathy Treated with Tocilizumab in Real-World Clinical Practice: A 9-Year Single-Center Experience

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Outcomes and Assessments
2.3. Statistical Analyses
3. Results
3.1. Patients
3.2. Primary Outcomes
3.2.1. Clinical Activity Score and Thyrotropin Receptor Antibody
3.2.2. Recurrences
3.2.3. Composite Evaluation of Graves’ Orbitopathy
3.3. Secondary Outcomes
3.4. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perros, P.; Hegedüs, L.; Bartalena, L.; Marcocci, C.; Kahaly, G.J.; Baldeschi, L.; Salvi, M.; Lazarus, J.H.; Eckstein, A.; Pitz, S.; et al. Graves’ orbitopathy as a rare disease in Europe: A European Group on Graves’ Orbitopathy (EUGOGO) position statement. Orphanet J. Rare Dis. 2017, 12, 72. [Google Scholar] [CrossRef]
- Hai, Y.P.; Lee, A.C.H.; Frommer, L.; Diana, T.; Kahaly, G.J. Immunohistochemical analysis of human orbital tissue in Graves’ orbitopathy. J. Endocrinol. Investig. 2020, 43, 123–137. [Google Scholar] [CrossRef]
- Kumar, S.; Schiefer, R.; Coenen, M.J.; Bahn, R.S. A stimulatory thyrotropin receptor antibody (M22) and thyrotropin increase interleukin-6 expression and secretion in Graves’ orbital preadipocyte fibroblasts. Thyroid 2010, 20, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Gerding, M.N.; van der Meer, J.W.; Broenink, M.; Bakker, O.; Wiersinga, W.M.; Prummel, M.F. Association of thyrotrophin receptor antibodies with the clinical features of Graves’ ophthalmopathy. Clin. Endocrinol. 2000, 52, 267–271. [Google Scholar] [CrossRef]
- Salvi, M.; Girasole, G.; Pedrazzoni, M.; Passeri, M.; Giuliani, N.; Minelli, R.; Braverman, L.E.; Roti, E. Increased serum concentrations of interleukin-6 (IL-6) and soluble IL-6 receptor in patients with Graves’ disease. J. Clin. Endocrinol. Metab. 1996, 81, 2976–2979. [Google Scholar] [CrossRef]
- Jyonouchi, S.C.; Valyasevi, R.W.; Harteneck, D.A.; Dutton, C.M.; Bahn, R.S. Interleukin-6 stimulates thyrotropin receptor expression in human orbital preadipocyte fibroblasts from patients with Graves’ ophthalmopathy. Thyroid 2001, 11, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Bartalena, L.; Lai, A.; Compri, E.; Marcocci, C.; Tanda, M.L. Novel immunomodulating agents for Graves orbitopathy. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Salvi, M.; Campi, I. Medical Treatment of Graves’ Orbitopathy. Horm. Metab. Res. 2015, 47, 779–788. [Google Scholar] [CrossRef]
- Bartalena, L.; Baldeschi, L.; Boboridis, K.; Eckstein, A.; Kahaly, G.J.; Marcocci, C.; Perros, P.; Salvi, M.; Wiersinga, W.M.; European Group on Graves’ Orbitopathy (EUGOGO). The 2016 European Thyroid Association/European Group on Graves’ Orbitopathy Guidelines for the Management of Graves’ Orbitopathy. Eur. Thyroid. J. 2016, 5, 9–26. [Google Scholar] [CrossRef]
- Stan, M.N.; Garrity, J.A.; Carranza Leon, B.G.; Prabin, T.; Bradley, E.A.; Bahn, R.S. Randomized controlled trial of rituximab in patients with Graves’ orbitopathy. J. Clin. Endocrinol. Metab. 2015, 100, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Salvi, M.; Vannucchi, G.; Currò, N.; Campi, I.; Covelli, D.; Dazzi, D.; Simonetta, S.; Guastella, C.; Pignataro, L.; Avignone, S.; et al. Efficacy of B-cell targeted therapy with rituximab in patients with active moderate to severe Graves’ orbitopathy: A randomized controlled study. J. Clin. Endocrinol. Metab. 2015, 100, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Mourits, M.P.; Prummel, M.F.; Wiersinga, W.M.; Koornneef, L. Clinical activity score as a guide in the management of patients with Graves’ ophthalmopathy. Clin. Endocrinol. 1997, 47, 9–14, Erratum in Clin. Endocrinol. 1997, 47, 632. [Google Scholar] [CrossRef]
- Pérez-Moreiras, J.V.; Rodríguez Álvarez, F.; Prada-Sánchez, M.C.; Varela-Agra, M.; Gómez Carnero, J.; Toledano, N.; Cabral, J. Thyroid orbitopathy. Protocol of activity, treatment, and rehabilitation surgery. In Orbit: Examination, Diagnosis, Microsurgery and Pathology, 2nd ed.; Pérez-Moreiras, J.V., Prada-Sánchez, M.C., Antúnez-López, J., Eds.; Jaypee Highlights Medical Publisers, Inc.: Panama City, Panama, 2018; Volume 2, pp. 477–601. [Google Scholar]
- Smith, T.J.; Janssen, J.A.M.J.L. Insulin-like Growth Factor-I Receptor and Thyroid-Associated Ophthalmopathy. Endocr. Rev. 2019, 40, 236–267. [Google Scholar] [CrossRef] [PubMed]
- Douglas, R.S.; Kahaly, G.J.; Patel, A.; Sile, S.; Thompson, E.H.; Perdok, R.; Fleming, J.C.; Fowler, B.T.; Marcocci, C.; Marinò, M.; et al. Teprotumumab for the Treatment of Active Thyroid Eye Disease. N. Engl. J. Med. 2020, 382, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Kahaly, G.J.; Ezra, D.G.; Fleming, J.C.; Dailey, R.A.; Tang, R.A.; Harris, G.J.; Antonelli, A.; Salvi, M.; Goldberg, R.A.; et al. Teprotumumab for Thyroid-Associated Ophthalmopathy. N. Engl. J. Med. 2017, 376, 1748–1761. [Google Scholar] [CrossRef]
- Strianese, D.; Rossi, F. Interruption of autoimmunity for thyroid eye disease: B-cell and T-cell strategy. Eye 2019, 33, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Moreiras, J.V.; Álvarez-López, A.; Gómez, E.C. Treatment of active corticosteroid-resistant graves’ orbitopathy. Ophthalmic Plast. Reconstr. Surg. 2014, 30, 162–167. [Google Scholar] [CrossRef]
- Perez-Moreiras, J.V.; Gomez-Reino, J.J.; Maneiro, J.R.; Perez-Pampin, E.; Romo Lopez, A.; Rodríguez Alvarez, F.M.; Castillo Laguarta, J.M.; Del Estad Cabello, A.; Gessa Sorroche, M.; España Gregori, E.; et al. Efficacy of Tocilizumab in Patients With Moderate-to-Severe Corticosteroid-Resistant Graves Orbitopathy: A Randomized Clinical Trial. Am. J. Ophthalmol. 2018, 195, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.J.; Wagner, L.H.; Seiff, S.R. Tocilizumab as a steroid sparing agent for the treatment of Graves’ orbitopathy. Am. J. Ophthalmol. Case Rep. 2017, 7, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Sy, A.; Eliasieh, K.; Silkiss, R.Z. Clinical Response to Tocilizumab in Severe Thyroid Eye Disease. Ophthalmic Plast. Reconstr. Surg. 2017, 33, e55–e57. [Google Scholar] [CrossRef]
- de-Pablo-Gómez-de-Liaño, L.; Fernández-Vigo, J.I.; Troyano-Rivas, J.; Niño-Rueda, C.; Romo-López, Á.; Gómez-de-Liaño, R. Response to tocilizumab treatment in Graves’ ophthalmopathy by measuring rectus muscle thickness and chemosis using optical coherence tomography. Arch. Soc. Esp. Oftalmol. 2018, 93, 386–391, English, Spanish. [Google Scholar] [CrossRef]
- Canas, C.A.; Bonilla-Abadia, F.; Vallejo, K.; Rengifo, H.M.; Gallon, M.A.; Tobon, G.J. Successful Treatment for Severe Thyroid-associated Ophthalmopathy with Tocilizumab. Endocr. Metab. Immune. Disord. Drug Targets 2018, 18, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Camps, I.; Molina-Pallete, R.; Bort-Martí, M.A.; Todolí, J.; España-Gregori, E. Tocilizumab as first treatment option in optic neuropathy secondary to Graves’ orbitopathy. Orbit 2018, 37, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Copperman, T.; Idowu, O.O.; Kersten, R.C.; Vagefi, M.R. Subcutaneous Tocilizumab for Thyroid Eye Disease: Simplified Dosing and Delivery. Ophthalmic Plast. Reconstr. Surg. 2019, 35, e64–e66. [Google Scholar] [CrossRef]
- Maldiney, T.; Deschasse, C.; Bielefeld, P. Tocilizumab for the Management of Corticosteroid-Resistant Mild to Severe Graves’ Ophthalmopathy, a Report of Three Cases. Ocul. Immunol. Inflamm. 2020, 28, 281–284. [Google Scholar] [CrossRef]
- Ceballos-Macías, J.J.; Rivera-Moscoso, R.; Flores-Real, J.A.; Vargas-Sánchez, J.; Ortega-Gutiérrez, G.; Madriz-Prado, R.; Velasco-Ramos, P.C.; Muñoz-Monroy, O.E.; Meneses-Pérez, A.C.; Fernández-Morales, I.N.; et al. Tocilizumab in glucocorticoid-resistant graves orbitopathy. A case series report of a mexican population. Ann. Endocrinol. 2020, 81, 78–82. [Google Scholar] [CrossRef]
- Bennedjaï, A.; Bouheraoua, N.; Gatfossé, M.; Dupasquier-Fediaevsky, L.; Errera, M.H.; Tazartes, M.; Borderie, V.; Hennocq, Q.; Dellal, A.; Riviere, S.; et al. Tocilizumab versus Rituximab in Patients with Moderate to Severe Steroid-resistant Graves’ Orbitopathy. Ocul. Immunol. Inflamm. 2020, 1–6. [Google Scholar] [CrossRef]
- Sánchez-Bilbao, L.; Martínez-López, D.; Revenga, M.; López-Vázquez, Á.; Valls-Pascual, E.; Atienza-Mateo, B.; Valls-Espinosa, B.; Maiz-Alonso, O.; Blanco, A.; Torre-Salaberri, I.; et al. Anti-IL-6 Receptor Tocilizumab in Refractory Graves’ Orbitopathy: National Multicenter Observational Study of 48 Patients. J. Clin. Med. 2020, 9, 2816. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Dragan, L.R.; Seiff, S.R.; Lee, D.C. Longitudinal correlation of thyroid-stimulating immunoglobulin with clinical activity of disease in thyroid-associated orbitopathy. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, A.K.; Plicht, M.; Lax, H.; Neuhäuser, M.; Mann, K.; Lederbogen, S.; Heckmann, C.; Esser, J.; Morgenthaler, N.G. Thyrotropin receptor autoantibodies are independent risk factors for Graves’ ophthalmopathy and help to predict severity and outcome of the disease. J. Clin. Endocrinol. Metab. 2006, 91, 3464–3470. [Google Scholar] [CrossRef]
- Lantz, M.; Planck, T.; Asman, P.; Hallengren, B. Increased TRAb and/or low anti-TPO titers at diagnosis of graves’ disease are associated with an increased risk of developing ophthalmopathy after onset. Exp. Clin. Endocrinol. Diabetes 2014, 122, 113–117. [Google Scholar] [CrossRef]
- Nicolì, F.; Lanzolla, G.; Mantuano, M.; Ionni, I.; Mazzi, B.; Leo, M.; Sframeli, A.; Posarelli, C.; Maglionico, M.N.; Figus, M.; et al. Correlation between serum anti-TSH receptor autoantibodies (TRAbs) and the clinical feature of Graves’ orbitopathy. J. Endocrinol. Investig. 2020. [Google Scholar] [CrossRef]
- Glinoer, D.; de Nayer, P.; Bex, M. Belgian Collaborative Study Group on Graves’ Disease. Effects of l-thyroxine administration, TSH-receptor antibodies and smoking on the risk of recurrence in Graves’ hyperthyroidism treated with antithyroid drugs: A double-blind prospective randomized study. Eur. J. Endocrinol. 2001, 144, 475–483. [Google Scholar] [CrossRef]
- Roos, J.C.P.; Paulpandian, V.; Murthy, R. Serial TSH-receptor antibody levels to guide the management of thyroid eye disease: The impact of smoking, immunosuppression, radio-iodine, and thyroidectomy. Eye 2019, 33, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, P. Smoking and thyroid disorders--a meta-analysis. Eur J Endocrinol 2002, 146, 153–161. [Google Scholar] [CrossRef]
- Prummel, M.F.; Wiersinga, W.M. Smoking and risk of Graves’ disease. JAMA 1993, 269, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Pfeilschifter, J.; Ziegler, R. Smoking and endocrine ophthalmopathy: Impact of smoking severity and current vs lifetime cigarette consumption. Clin. Endocrinol. 1996, 45, 477–481. [Google Scholar] [CrossRef]
- Bartalena, L.; Marcocci, C.; Tanda, M.L.; Manetti, L.; Dell’Unto, E.; Bartolomei, M.P.; Nardi, M.; Martino, E.; Pinchera, A. Cigarette smoking and treatment outcomes in Graves ophthalmopathy. Ann. Intern. Med. 1998, 129, 632–635. [Google Scholar] [CrossRef]
- Eckstein, A.; Quadbeck, B.; Mueller, G.; Rettenmeier, A.W.; Hoermann, R.; Mann, K.; Steuhl, P.; Esser, J. Impact of smoking on the response to treatment of thyroid associated ophthalmopathy. Br. J. Ophthalmol. 2003, 87, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Perricone, C.; Versini, M.; Ben-Ami, D.; Gertel, S.; Watad, A.; Segel, M.J.; Ceccarelli, F.; Conti, F.; Cantarini, L.; Bogdanos, D.P.; et al. Smoke and autoimmunity: The fire behind the disease. Autoimmun. Rev. 2016, 15, 354–374. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.P.; Watad, A.; Shoenfeld, Y. Nicotine and autoimmunity: The lotus’ flower in tobacco. Pharmacol. Res. 2018, 128, 101–109. [Google Scholar] [CrossRef]
- Bartalena, L.; Marcocci, C.; Bogazzi, F.; Manetti, L.; Tanda, M.L.; Dell’Unto, E.; Bruno-Bossio, G.; Nardi, M.; Bartolomei, M.P.; Lepri, A.; et al. Relation between therapy for hyperthyroidism and the course of Graves’ ophthalmopathy. N. Engl. J. Med. 1998, 338, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Menconi, F.; Profilo, M.A.; Leo, M.; Sisti, E.; Altea, M.A.; Rocchi, R.; Latrofa, F.; Nardi, M.; Vitti, P.; Marcocci, C.; et al. Spontaneous improvement of untreated mild Graves’ ophthalmopathy: Rundle’s curve revisited. Thyroid 2014, 24, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Khandji, J.; Kazim, M. Recurrent Thyroid Eye Disease. Ophthalmic Plast. Reconstr. Surg. 2015, 31, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Kahaly, G.J.; Pitz, S.; Hommel, G.; Dittmar, M. Randomized, single blind trial of intravenous versus oral steroid monotherapy in Graves’ orbitopathy. J. Clin. Endocrinol. Metab. 2005, 90, 5234–5240. [Google Scholar] [CrossRef]
- Tanda, M.L.; Piantanida, E.; Liparulo, L.; Veronesi, G.; Lai, A.; Sassi, L.; Pariani, N.; Gallo, D.; Azzolini, C.; Ferrario, M.; et al. Prevalence and natural history of Graves’ orbitopathy in a large series of patients with newly diagnosed graves’ hyperthyroidism seen at a single center. J. Clin. Endocrinol. Metab. 2013, 98, 1443–1449. [Google Scholar] [CrossRef]
- Rare Diseases: Natural History Studies for Drug Development Guidance for Industry—Draft. March 2019. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/rare-diseases-natural-history-studies-drug-development (accessed on 16 January 2021).
- Jewell, N.P. Natural history of diseases: Statistical designs and issues. Clin. Pharmacol. Ther. 2016, 100, 353–361. [Google Scholar] [CrossRef]
- Prada-Ramallal, G.; Takkouche, B.; Figueiras, A. Bias in pharmacoepidemiologic studies using secondary health care databases: A scoping review. BMC Med. Res. Methodol. 2019, 19, 53. [Google Scholar] [CrossRef]
- Bartalena, L.; Piantanida, E.; Gallo, D.; Lai, A.; Tanda, M.L. Epidemiology, Natural History, Risk Factors, and Prevention of Graves’ Orbitopathy. Front. Endocrinol. 2020, 11, 615993. [Google Scholar] [CrossRef]
- Selva, D.; Chen, C.; King, G. Late reactivation of thyroid orbitopathy. Clin. Exp. Ophthalmol. 2004, 32, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Schulte, P.J.; Mascha, E.J. Propensity Score Methods: Theory and Practice for Anesthesia Research. Anesth. Analg. 2018, 127, 1074–1084. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Baseline |
|---|---|
| Age—mean yr (SD) | 53.8 (10.5) |
| Female sex—% (No. of patients) | 75.9 (41) |
| Smoker—% (No. of patients) | 38.9 (21) |
| Diabetes—% (No. of patients) 1 | 9.4 (5) |
| Thyroid status—% (No. of patients) Hyperthyroidism Hypothyroidism | 87.0 (47) 13.0 (7) |
| FT3—mean pg/mL (SD) (No. of patients) 2 | 3.4 (1.0) (16) |
| FT4—mean ng/dL (SD) (No. of patients) 2 | 1.3 (0.7) (52) |
| TSH—mean mU/L (SD) (No. of patients) 2 | 3.0 (4.0) (53) |
| Thyrotropin receptor antibody—mean U/L (SD) (No. of patients) Normal TRAb (≤10 U/L)—% (No. of patients) | 69.0 (87.5) (54) 9.3 (5) |
| Previous treatment—% (No. of patients) Radioactive iodine 1 Thyroidectomy | 18.9 (10) 24.1 (13) |
| Time between GO and GD diagnoses—median mo (range) (No. of patients) 3 | 4.5 (2.0–11.0) (6) |
| Time between GD and GO diagnoses—median mo (range) (No. of patients) 3 | 5.9 (0.9–200.2) (38) |
| Time between GO diagnosis and tocilizumab onset—median mo (range) (No. of patients) | 10.5 (3.5–22.9) (54) |
| Clinical Activity Score 4—mean pt (SD) (No. of patients) | 6.7 (1.5) (54) |
| Exophthalmos—mean mm (SD) (No. of eyes) | 21.8 (3.2) (107) |
| Eyelid retraction—mean mm 5 (SD) (No. of eyes) Upper Lower | 2.5 (1.3) (88) 1.7 (0.7) (46) |
| Diplopia—% (No. of patients) 6 Primary gaze Extreme gaze | 25.5 (12) 59.6 (28) |
| Variable | No. of Patients | Pre-Treatment Mean U/L (SD) 1,5 | Post-Treatment Mean U/L (SD) 2,5 | Reduction U/L (%) 3 | p-Value 4 |
|---|---|---|---|---|---|
| Thyroid status 6 | |||||
| Hyperthyroidism | 46 | 58.3 (63.0) | 11.4 (10.9) | 46.9 (80.4) | <0.001 |
| Hypothyroidism | 7 | 146.4 (172.1) | 56.1 (106.1) | 90.3 (61.7) | 0.018 |
| Radioiodine 7 | |||||
| No | 42 | 71.2 (83.7) | 11.7 (11.2) | 59.5 (83.6) | <0.001 |
| Yes | 10 | 68.5 (112.9) | 41.9 (89.7) | 26.6 (38.6) | 0.005 |
| Thyroidectomy 6,8 | |||||
| No | 40 | 58.1 (74.0) | 17.4 (45.8) | 40.7 (70.0) | <0.001 |
| Yes | 13 | 106.3 (117.9) | 17.2 (16.2) | 89.1 (83.8) | 0.002 |
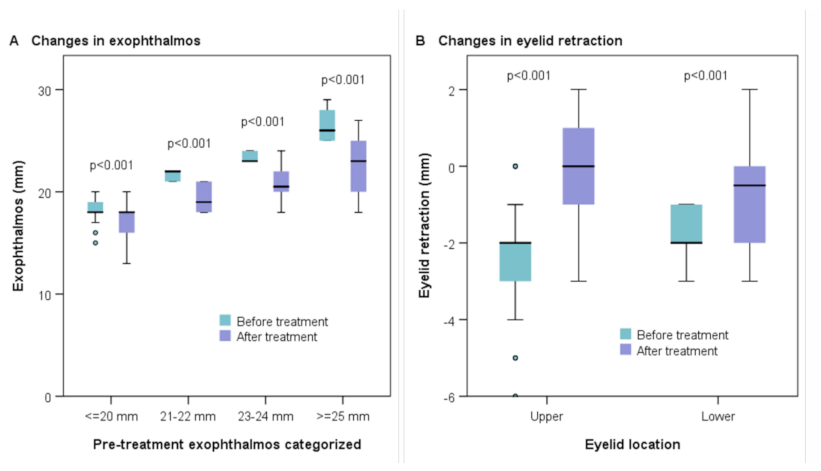
| Variable | No. of Eyes | Pre-Treatment Mean mm (range) | Post-Treatment Mean mm (range) | Reduction mm (%) 1 | p-Value 2 |
|---|---|---|---|---|---|
| Exophthalmos | |||||
| ≤20 mm | 40 | 18.4 (15–20) | 17.2 (13–20) | 1.2 (6.5) | <0.001 |
| 21–22 mm | 18 | 21.6 (21–22) | 19.2 (18–21) | 2.4 (11.1) | <0.001 |
| 23–24 mm | 28 | 23.5 (23–24) | 20.8 (18–24) | 2.7 (11.5) | <0.001 |
| ≥25 mm | 21 | 26.5 (25–29) | 22.7 (18–27) | 3.8 (14.3) | <0.001 |
| Eyelid retraction | |||||
| Upper 3 | 88 | −2.5 (−6 to 0) | −0.2 (−3 to +2) | 2.3 (92.0) | <0.001 |
| Lower 4 | 46 | −1.7 (−3 to −1) | −0.7 (−3 to +2) | 1.0 (58.8) | <0.001 |
| Characteristic | Stan et al. (2015) [10] | Smith et al. (2017) [16] | Pérez-Moreiras et al. (2018) [19] | Douglas et al. (2020) [15] | Pérez-Moreiras et al. (2021) |
|---|---|---|---|---|---|
| Design (study drug) | RCT (rituximab) | RCT (teprotumumab) | RCT (tocilizumab) | RCT (teprotumumab) | Retrospective (tocilizumab) |
| Control group—No. of patients (type of control) | 12 (placebo) | 44 (placebo) | 17 (placebo) | 42 (placebo) | 54 (pre–post) |
| Main outcomes | CAS | Composite outcome (exophthalmos, CAS) | CAS | Exophthalmos, CAS | CAS, TRAb, exophthalmos, eyelid retraction, diplopia |
| Definition of response | Decrease in CAS of ≥2 pt (24 wk) + decrease in exophthalmos of ≥2 mm, decrease in eyelid fissure width of ≥3 mm, improvement in diplopia score, among others (24, 52 wk) (secondary outcomes) + no need for additional therapy (success) |
CAS ≤ 1 (6, 12, 18, 24 wk) | Decrease in CAS of ≥2 pt (16 wk) + decrease in exophthalmos ≥2 mm, decrease in eyelid aperture ≥3 mm, improvement in diplopia score or in signs of soft tissue involvement (16, 40 wk) (secondary composite outcome—at least 2 criteria) CAS ≤ 2 (16, 40 wk) |
CAS ≤ 1 (6, 12, 18, 24 wk) | CAS ≤ 1 (also ≤2); TRAb ≤ 10 U/L (4, 8, 12, 16, >16 1 wk) At least 2 (also 3) of the following criteria (≥16 wk): (a) decrease in CAS of ≥2 pt; (b) decrease in exophthalmos of ≥2 mm; (c) decrease in eyelid retraction of ≥2 mm; (d) improvement in diplopia |
| ∆ CAS—mean (SD) (% reduction) | −1.5 (28%) at wk 24 −1.0 (19%) at wk 16 (extrapolated) | −2.4 (46%) (extrapolated) at wk 24 −2.1 (40%) (extrapolated) at wk 18 | −3.0 (1.9) (55%) 2 at wk 16 | n/a | −5.8 (1.5) (87%) at wk 16 |
| Response—No. of patients (%) | Improvement of ≥2 pt in 3/12 (25%) at wk 24 | CAS ≤ 1 in 21% at wk 24 CAS ≤ 1 in 15% at wk 18 (extrapolated) | CAS ≤ 2 in 6/17 (35%) at wk 16 Improvement of ≥2 pt in (10/17) 59% at wk 16 | CAS ≤ 1 in 21% at wk 24 CAS ≤ 1 in 19% at wk 18 | CAS ≤ 1 in 37/50 (74%) at wk 16 CAS ≤ 2 in 43/50 (86%) Improvement of ≥2 pt in 50/50 (100%) |
| ∆ TRAb—median U/L (IQR) (% reduction 3) | −9.5 IU/L (49%) at wk 24 (extrapolated) 4 −6.5 IU/L (33%) at wk 16 (extrapolated) | n/a | n/a | n/a | −26.0 (−70.4 to 10.4) (81%) at wk 16 |
| Response—No. of patients (%) | n/a | n/a | n/a | n/a | TRAb ≤ 10 in 23/42 (55%) at wk 16 |
| ∆ Proptosis—mean mm (SD) (% 3) | Left: 0.0 (1.9) (<1%) 5 at wk 52 Right: 0.0 (1.8) (<1%) 5 | −0.5 (2%) 6 at wk 24 −0.1 (<1%) 6 at wk 18 (extrapolated) | Left: +0.1 (1.7) (<1%) 2,6 at wk 16 Right: +0.1 (1.3) (<1%) 2,6 | −0.5 (2%) 6 at wk 24 −0.6 (3%) 6 at wk 18 | Left: −2.4 (2.1) 6 (11%) at wk ≥16 Right: −2.2 (1.8) 6 (10%) |
| Response—No. patients (%) | Improvement of ≥2 mm in 4/12 (33%) at wk 24 | n/a | Improvement of ≥2 mm in 2/14 (14%) 2 at wk 16 | Improvement of ≥2 mm in 4/42 (10%) ITT at wk 24 (4/34, 12%, PP); 14% ITT at wk 18 | Improvement of ≥2 mm in 42/54 (78%) at wk ≥16 |
| ∆ Eyelid retraction—median mm (IQR) / mean (SD) (% 3) | Left: 0.5 (−1.0 to 1.8) at wk 24 7,8 Right: −0.5 (−1.0 to 1.8) 7,8 | n/a | Left: −0.4 (1.1) (3%) at wk 16 2,7 Right: −0.5 (2.0) (4%) 2,7 | n/a | Left: 2.0 (1.0-3.0) / 2.3 (1.4) (92%) 9 at wk ≥16 Right: 2.0 (1.0–3.0) / 2.4 (1.3) (96%) 9 |
| Response—No. of patients (%) | Improvement of ≥3 mm in 0% at wk 24 (extrapolated) | n/a | Improvement of ≥3 in 1/14 (7%) 2 at wk 16 | n/a | Improvement of ≥2 mm in 33/44 (75%) at wk ≥16 |
| ∆ Diplopia—median score (IQR) or % difference 10 | 0.0 (−0.8 to 0.0) 11 | −2% in extreme gaze at wk 24 4% in primary gaze (increase) | 0.0 (−1.0 to 0. 0) 2,11 | n/a | −36% in extreme gaze at wk ≥16 −15% in primary gaze |
| Response—No. of patients (%) | Improvement in 8% at wk 24 (extrapolated) 12 | Improvement in 10/39 (26%) at wk 24 13 | Improvement in 0/17 (0%) at wk 16 14 | Improvement in 8/28 (29%) at wk 24; 21% at wk 18 13 | Improvement in 19/28 (68%) at wk ≥16 15 |
| Overall response (composite outcome) | Success rate of 25% at wk 24 | 9/45 (20%) ITT; 8/36 (22%) PP at wk 24 | 5/17 (29%), if ≥2 criteria required (of 5) at wk 16 | 3/42 (7%) at wk 24 12% at wk 18 | 53/54 (98%), if ≥2 criteria required (of 4) at wk ≥16 (37/50, 74%, if ≥3 criteria) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Moreiras, J.V.; Varela-Agra, M.; Prada-Sánchez, M.C.; Prada-Ramallal, G. Steroid-Resistant Graves’ Orbitopathy Treated with Tocilizumab in Real-World Clinical Practice: A 9-Year Single-Center Experience. J. Clin. Med. 2021, 10, 706. https://doi.org/10.3390/jcm10040706
Pérez-Moreiras JV, Varela-Agra M, Prada-Sánchez MC, Prada-Ramallal G. Steroid-Resistant Graves’ Orbitopathy Treated with Tocilizumab in Real-World Clinical Practice: A 9-Year Single-Center Experience. Journal of Clinical Medicine. 2021; 10(4):706. https://doi.org/10.3390/jcm10040706
Chicago/Turabian StylePérez-Moreiras, José V., María Varela-Agra, M. Consuelo Prada-Sánchez, and Guillermo Prada-Ramallal. 2021. "Steroid-Resistant Graves’ Orbitopathy Treated with Tocilizumab in Real-World Clinical Practice: A 9-Year Single-Center Experience" Journal of Clinical Medicine 10, no. 4: 706. https://doi.org/10.3390/jcm10040706
APA StylePérez-Moreiras, J. V., Varela-Agra, M., Prada-Sánchez, M. C., & Prada-Ramallal, G. (2021). Steroid-Resistant Graves’ Orbitopathy Treated with Tocilizumab in Real-World Clinical Practice: A 9-Year Single-Center Experience. Journal of Clinical Medicine, 10(4), 706. https://doi.org/10.3390/jcm10040706