
Complicating Acute Myocardial Infarction. Current Status and Unresolved Targets for Subsequent Research


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
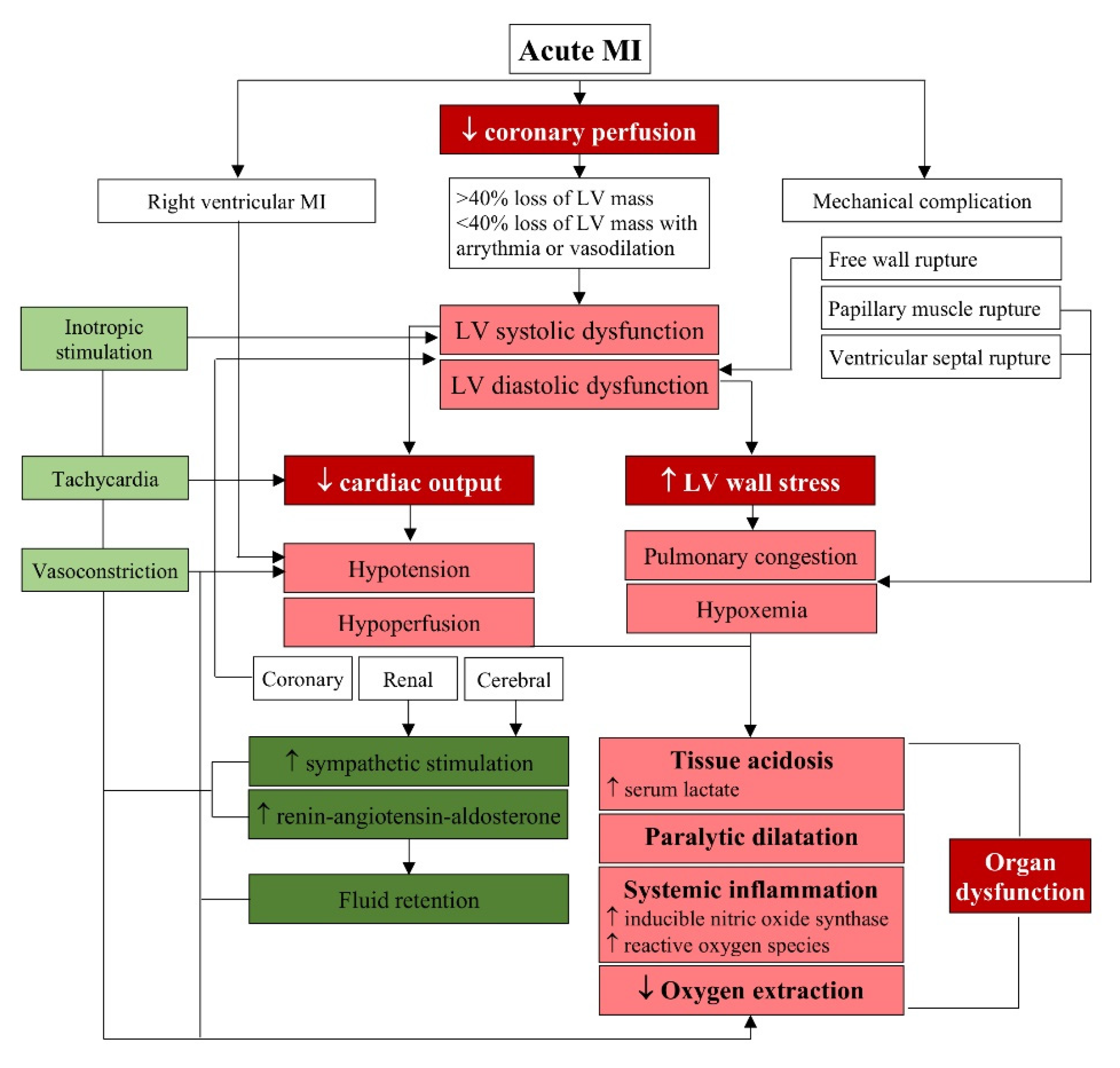
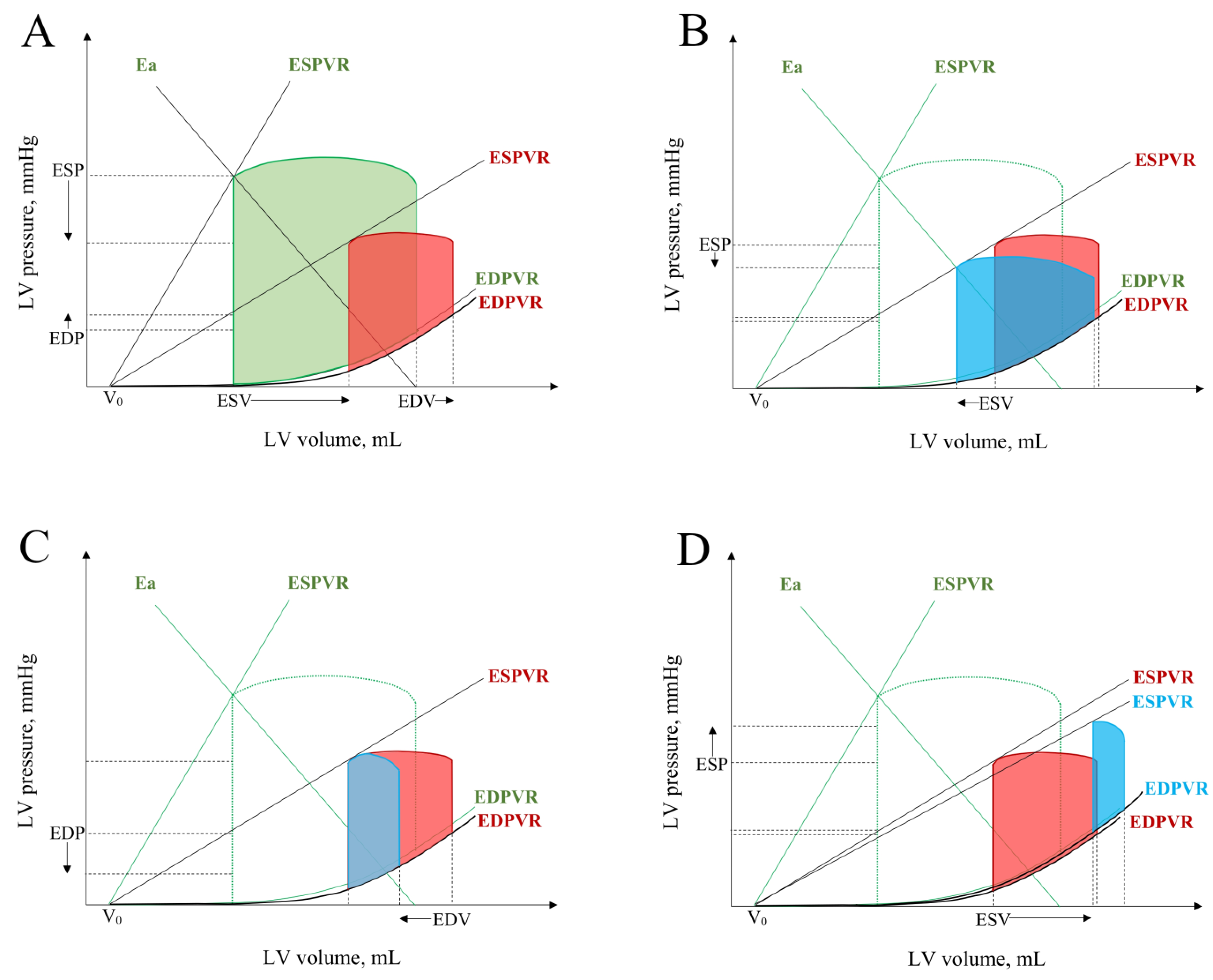
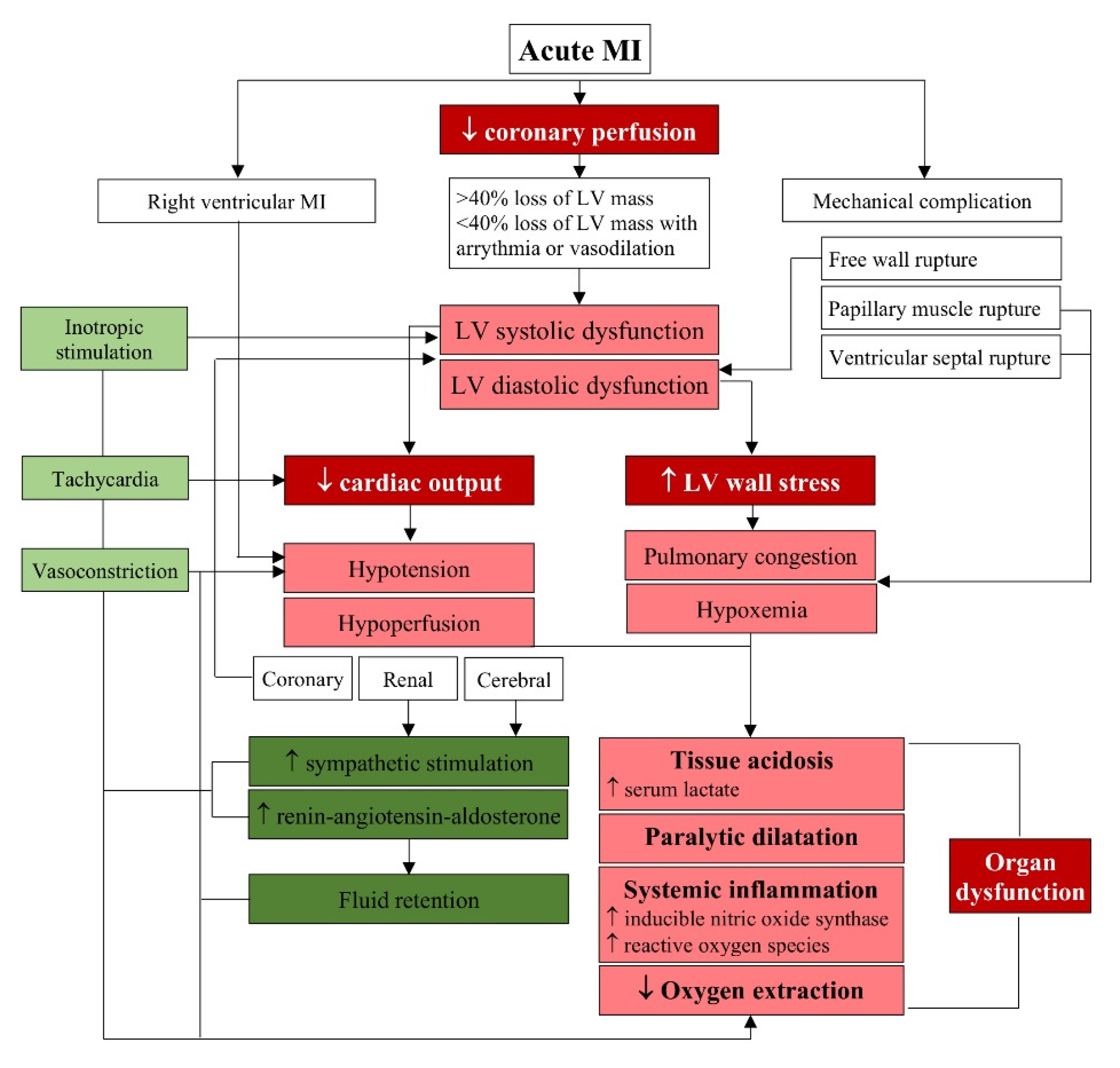
2. Mechanisms of Dysfunction in Complicating MI
3. Pathophysiology of Mechanical Complications of MI
4. Risk Factors of Complicating MI and Predictors of Clinical Outcomes
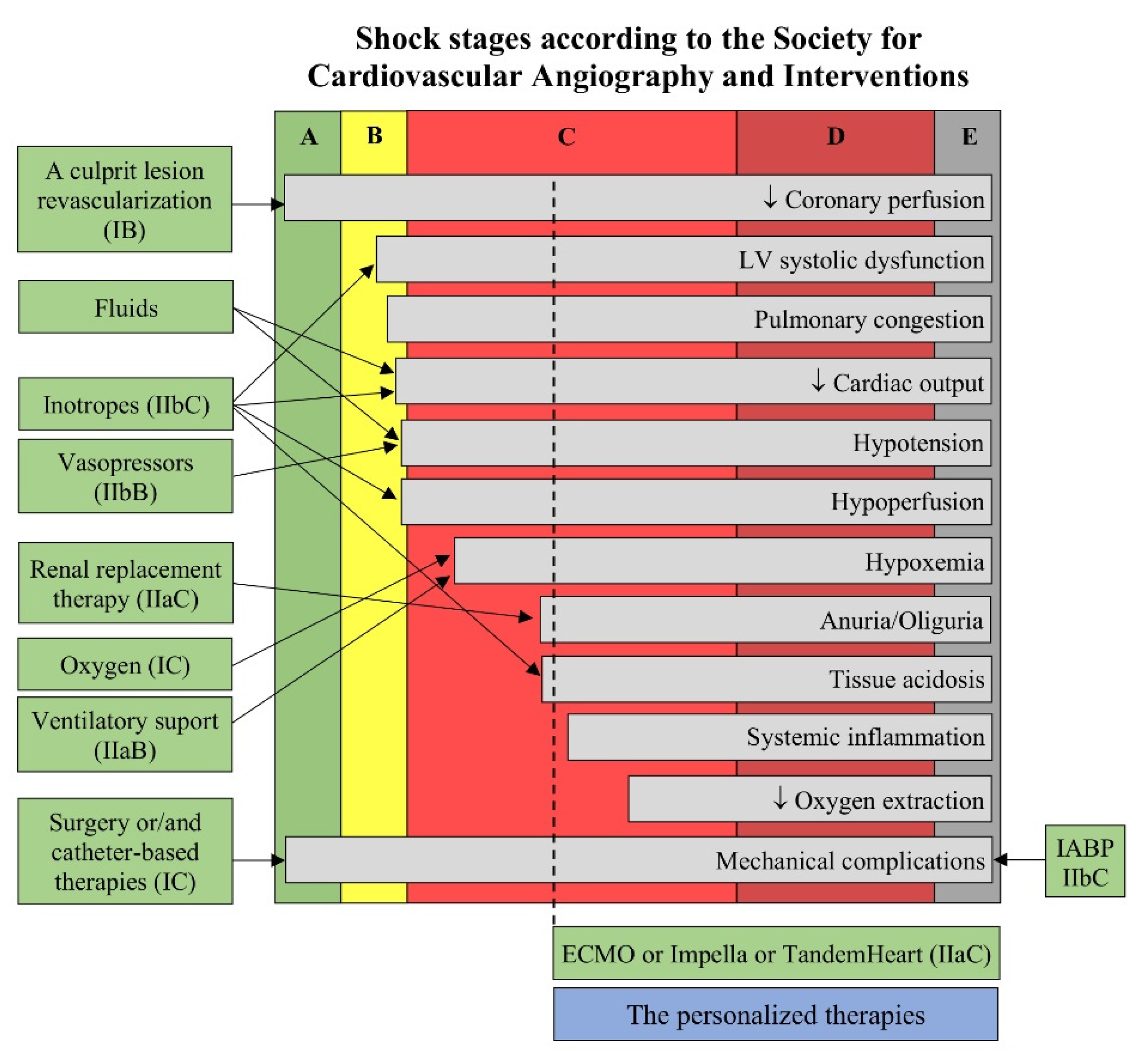
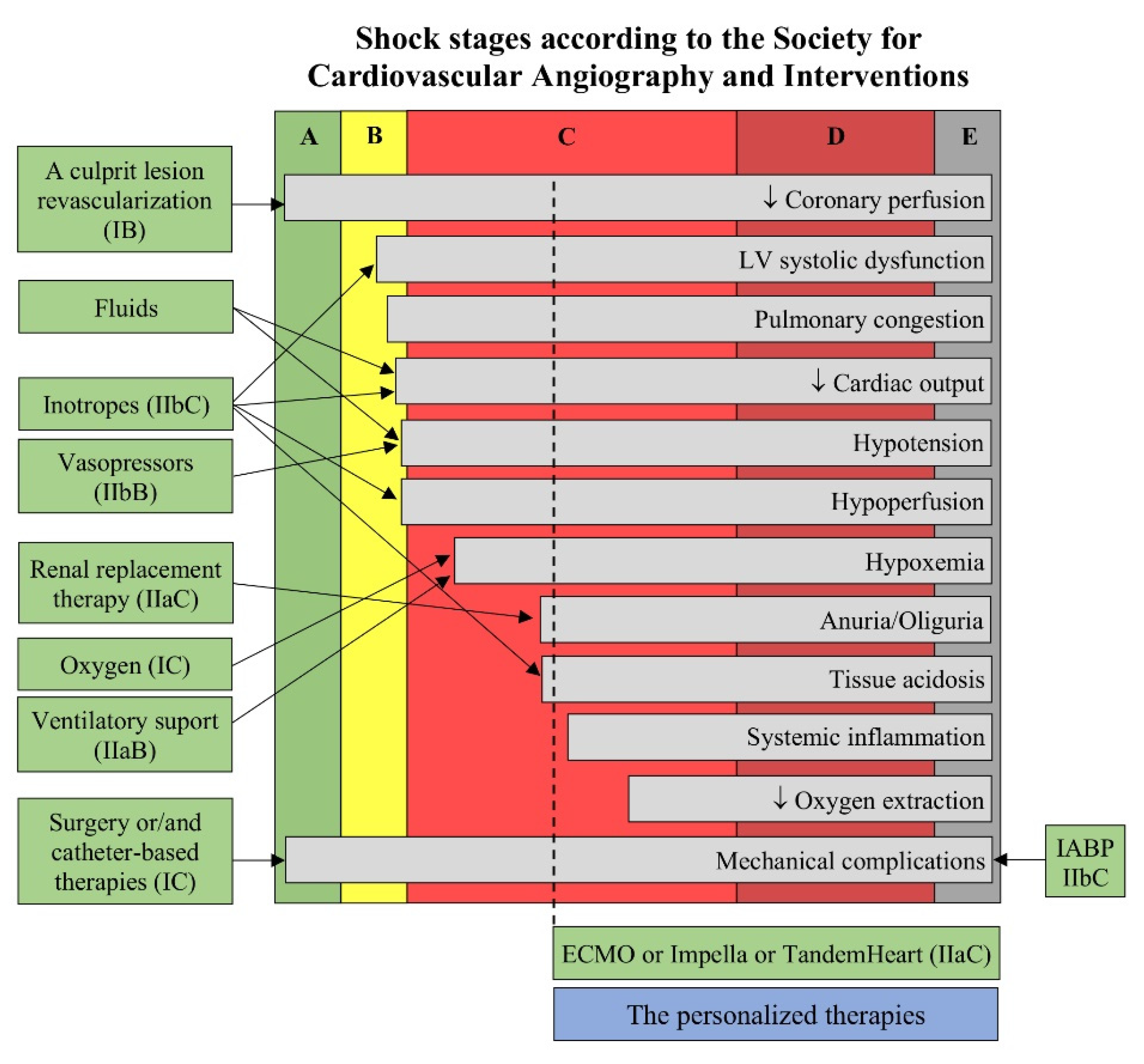
5. Principles for the Management of Patients with Complicating MI
6. Well-Established Therapeutic Approach to Mechanical Complications
7. Mechanical Circulatory Support for Complicating MI
8. Alternative Techniques Dedicated for Mechanical Complications
9. The Concept of Personalized Therapy of Patients with Complicating MI
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Kristensen, S.D.; Laut, K.G.; Fajadet, J.; Kaifoszova, Z.; Kala, P.; Di Mario, C.; Wijns, W.; Clemmensen, P.; Agladze, V.; Antoniades, L.; et al. European Association for Percutaneous Cardiovascular Interventions. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: Current status in 37 ESC countries. Eur. Heart J. 2014, 35, 1957–1970. [Google Scholar] [CrossRef] [Green Version]
- De Luca, L.; Savonitto, S. Composite trends of cardiogenic shock complicating acute myocardial infarction. Eur. J. Heart Fail. 2020, 22, 673–675. [Google Scholar] [CrossRef]
- García-García, C.; Oliveras, T.; El Ouaddi, N.; Rueda, F.; Serra, J.; Labata, C.; Ferrer, M.; Cediel, G.; Montero, S.; Martínez, M.J.; et al. Short- and Long-Term Mortality Trends in STEMI-Cardiogenic Shock over Three Decades (1989–2018): The Ruti-STEMI-Shock Registry. J. Clin. Med. 2020, 9, 2398. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, M.D.; Rørth, R.; Lindholm, M.G.; Kjaergaard, J.; Schmidt, M.; Møller, J.E.; Hassager, C.; Torp-Pedersen, C.; Gislason, G.; Køber, L.; et al. Trends in first-time hospitalization, management, and short-term mortality in acute myocardial infarction–related cardiogenic shock from 2005 to 2017: A nationwide cohort study. Am. Heart J. 2020, 229, 127–137. [Google Scholar] [CrossRef]
- Kolte, D.; Khera, S.; Aronow, W.S.; Mujib, M.; Palaniswamy, C.; Sule, S.; Jain, D.; Gotsis, W.; Ahmed, A.; Frishman, W.H.; et al. Trends in Incidence, Management, and Outcomes of Cardiogenic Shock Complicating ST-Elevation Myocardial Infarction in the United States. J. Am. Heart Assoc. 2014, 3, e000590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbadawi, A.; Elgendy, I.Y.; Mahmoud, K.; Barakat, A.F.; Mentias, A.; Mohamed, A.H.; Ogunbayo, G.O.; Megaly, M.; Saad, M.; Omer, M.; et al. Temporal Trends and Outcomes of Mechanical Complications in Patients With Acute Myocardial Infarction. JACC Cardiovasc. Interv. 2019, 12, 1825–1836. [Google Scholar] [CrossRef]
- Puerto, E.; Viana-Tejedor, A.; Martínez-Sellés, M.; Domínguez-Pérez, L.; Moreno, G.; Martín-Asenjo, R.; Bueno, H. Temporal Trends in Mechanical Complications of Acute Myocardial Infarction in the Elderly. J. Am. Coll. Cardiol. 2018, 72, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Hochman, J.S.; E Buller, C.; A Sleeper, L.; Boland, J.; Dzavik, V.; A Sanborn, T.; Godfrey, E.; White, H.D.; Lim, J.; LeJemtel, T. Cardiogenic shock complicating acute myocardial infarction—etiologies, management and outcome: A report from the SHOCK Trial Registry. Should we emergently revascularize Occluded Coronaries for cardiogenic shock? J. Am. Coll. Cardiol. 2000, 36, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- de la Torre Hernández, J.M. Mechanical Complications in Elderly Patients with Myocardial Infarction: Becoming fewer but just as fatal. J. Am. Coll. Cardiol. 2018, 72, 967–969. [Google Scholar] [CrossRef]
- Bajaj, A.; Sethi, A.; Rathor, P.; Suppogu, N.; Sethi, A. Acute Complications of Myocardial Infarction in the Current Era: Diagnosis and management. J. Investig. Med. 2015, 63, 844–855. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Zeymer, U.; Bueno, H.; Granger, C.B.; Hochman, J.; Huber, K.; Lettino, M.; Price, S.; Schiele, F.; Tubaro, M.; Vranckx, P.; et al. Acute Cardiovascular Care Association position statement for the diagnosis and treatment of patients with acute myocardial infarction complicated by cardiogenic shock: A document of the Acute Cardiovascular Care Association of the European Society of Cardiology. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 183–197. [Google Scholar] [CrossRef] [Green Version]
- Aymong, E.D.; Ramanathan, K.; Buller, C.E. Pathophysiology of Cardiogenic Shock Complicating Acute Myocardial Infarction. Med. Clin. N. Am. 2007, 91, 701–712. [Google Scholar] [CrossRef]
- Fincke, R.; Hochman, J.; Lowe, A.M.; Menon, V.; Slater, J.; Webb, J.G.; LeJemtel, T.H.; Cotter, G.; SHOCK Investigators. Cardiac power is the strongest hemodynamic correlate of mortality in cardiogenic shock: A report from the SHOCK trial registry. J. Am. Coll. Cardiol. 2004, 44, 340–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hieda, M.; Goto, Y. Cardiac Mechanoenergetics in Patients with Acute Myocardial Infarction: From pressure-volume loop diagram related to cardiac oxygen consumption. Heart Fail. Clin. 2020, 16, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Lim, S. Cardiogenic Shock: Failure of Oxygen Delivery and Oxygen Utilization. Clin. Cardiol. 2016, 39, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Squara, P.; Hollenberg, S.; Payen, D. Reconsidering Vasopressors for Cardiogenic Shock: Everything should be made as simple as possible, but not simpler. Chest 2019, 156, 392–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jentzer, J.C.; Burstein, B.; Van Diepen, S.; Murphy, J.; Holmes, D.R., Jr.; Bell, M.R.; Barsness, G.W.; Henry, T.D.; Menon, V.; Rihal, C.S.; et al. Defining shock and preshock for mortality risk stratification in cardiac intensive care unit patients. Circ Heart Fail. 2021, 14, e007678. [Google Scholar] [CrossRef]
- Baran, D.A.; Grines, C.L.; Bailey, S.; Burkhoff, D.; Hall, S.A.; Henry, T.D.; Hollenberg, S.M.; Kapur, N.K.; O’Neill, W.; Ornato, J.P.; et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter. Cardiovasc. Interv. 2019, 94, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Chioncel, O.; Parissis, J.; Mebazaa, A.; Thiele, H.; Desch, S.; Bauersachs, J.; Harjola, V.; Antohi, E.; Arrigo, M.; Ben Gal, T.; et al. Epidemiology, pathophysiology and contemporary management of cardiogenic shock—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1315–1341. [Google Scholar] [CrossRef]
- Kirschenbaum, L.A.; Astiz, M.E.; Rackow, E.C.; Saha, D.C.; Lin, R. Microvascular response in patients with cardiogenic shock. Crit. Care Med. 2000, 28, 1290–1294. [Google Scholar] [CrossRef] [PubMed]
- Wijntjens, G.W.M.; Fengler, K.; Fuernau, G.; Jung, C.; Uil, C.D.; Akin, S.; van de Hoef, T.P.; Šerpytis, R.; Diletti, R.; Henriques, J.P.S.; et al. Prognostic implications of microcirculatory perfusion versus macrocirculatory perfusion in cardiogenic shock: A CULPRIT-SHOCK substudy. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 108–119. [Google Scholar] [CrossRef] [Green Version]
- Du, Z.; Jia, Z.; Wang, J.; Xing, Z.; Jiang, C.; Xu, B.; Yang, X.; Yang, F.; Na Miao, N.; Xing, J.; et al. Effect of increasing mean arterial blood pressure on microcirculation in patients with cardiogenic shock supported by extracorporeal membrane oxygenation. Clin. Hemorheol. Microcirc. 2018, 70, 27–37. [Google Scholar] [CrossRef]
- Graf, T.; Desch, S.; Eitel, I.; Thiele, H. Acute myocardial infarction and cardiogenic shock: Pharmacologic and mechanical hemodynamic support pathways. Coron. Artery Dis. 2015, 26, 535–544. [Google Scholar] [CrossRef]
- Prondzinsky, R.; Unverzagt, S.; Lemm, H.; Wegener, N.-A.; Schlitt, A.; Heinroth, K.M.; Dietz, S.; Buerke, U.; Kellner, P.; Loppnow, H.; et al. Interleukin-6, -7, -8 and -10 predict outcome in acute myocardial infarction complicated by cardiogenic shock. Clin. Res. Cardiol. 2012, 101, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Harjola, V.-P.; Mullens, W.; Banaszewski, M.; Bauersachs, J.; Brunner-La Rocca, H.P.; Chioncel, O.; Collins, S.P.; Doehner, W.; Filippatos, G.S.; Flammer, A.J.; et al. Organ dysfunction, injury and failure in acute heart failure: From pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2017, 19, 821–836. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Menon, V.; Lowe, A.M.; Lange, M.; Dzavik, V.; Sleeper, L.A.; Hochman, J.; SHOCK Investigators. Systemic Inflammatory Response Syndrome After Acute Myocardial Infarction Complicated by Cardiogenic Shock. Arch. Intern. Med. 2005, 165, 1643–1650. [Google Scholar] [CrossRef]
- Parenica, J.; Jarkovsky, J.; Malaska, J.; Mebazaa, A.; Gottwaldova, J.; Helanova, K.; Litzman, J.; Dastych, M.; Tomandl, J.; Spinar, J.; et al. Infectious Complications and Immune/Inflammatory Response in Cardiogenic Shock Patients: A prospective observational study. Shock 2017, 47, 165–174. [Google Scholar] [CrossRef]
- Nagatomo, Y.; Tang, W.H.W. Intersections Between Microbiome and Heart Failure: Revisiting the Gut Hypothesis. J. Card. Fail. 2015, 21, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Topaz, O.; Taylor, A.L. Interventricular septal rupture complicating acute myocardial infarction: From pathophysiologic features to the role of invasive and noninvasive diagnostic modalities in current management. Am. J. Med. 1992, 93, 683–688. [Google Scholar] [CrossRef]
- Slater, J.; Brown, R.J.; A Antonelli, T.; Menon, V.; Boland, J.; Col, J.; Dzavik, V.; Greenberg, M.; Menegus, M.; Connery, C.; et al. Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: A report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock? J. Am. Coll. Cardiol. 2000, 36, 1117–1122. [Google Scholar] [CrossRef] [Green Version]
- Birnbaum, Y.; Fishbein, M.C.; Blanche, C.; Siegel, R.J. Ventricular Septal Rupture after Acute Myocardial Infarction. N. Engl. J. Med. 2002, 347, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, B.S.; Granger, C.B.; Birnbaum, Y.; Pieper, K.S.; Morris, D.C.; Kleiman, N.S.; Vahanian, A.; Califf, R.M.; Topol, E. Risk Factors, Angiographic Patterns, and Outcomes in Patients with Ventricular Septal Defect Complicating Acute Myocardial Infarction. GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. Circulation 2000, 101, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Yip, H.-K.; Fang, C.-Y.; Tsai, K.-T.; Chang, H.-W.; Yeh, K.-H.; Fu, M.; Wu, C.-J. The Potential Impact of Primary Percutaneous Coronary Intervention on Ventricular Septal Rupture Complicating Acute Myocardial Infarction. Chest 2004, 125, 1622–1628. [Google Scholar] [CrossRef] [Green Version]
- Hasdai, D.; Behar, S.; Wallentin, L.; Danchin, N.; Gitt, A.; Boersma, H.; Fioretti, P.; Simoons, M.; Battler, A. A prospective survey of the characteristics, treatments and outcomes of patients with acute coronary syndromes in Europe and the Mediterranean basin. The Euro Heart Survey of Acute Coronary Syndromes (Euro Heart Survey ACS). Eur. Heart J. 2002, 23, 1190–1201. [Google Scholar] [CrossRef] [Green Version]
- López-Sendón, J.; Gurfinkel, E.P.; Lopez de Sa, E.; Agnelli, G.; Gore, J.M.; Steg, P.G.; Eagle, K.A.; Cantador, J.R.; Fitzgerald, G.; Granger, C.B.; et al. Factors related to heart rupture in acute coronary syndromes in the Global Registry of Acute Coronary Events. Eur. Heart J. 2010, 31, 1449–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, J.M.; Roberts, W.C. Acquired ventricular septal defect during acute myocardial infarction: Analysis of 38 unoperated necropsy patients and comparison with 50 unoperated necropsy patients without rupture. Am. J. Cardiol. 1988, 62, 8–19. [Google Scholar] [CrossRef]
- Glasson, J.R.; Komeda, M.; Daughters, G.T.; Bolger, A.F.; Karlsson, M.O.; Foppiano, L.E.; Hayase, M.; Oesterle, S.N.; Ingels, N.B.; Miller, D. Early systolic mitral leaflet “loitering” during acute ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 1998, 116, 193–205. [Google Scholar] [CrossRef] [Green Version]
- Lamas, G.A.; Mitchell, G.F.; Flaker, G.C.; Smith, S.C.; Gersh, B.J.; Basta, L.; Moyé, L.; Braunwald, E.; Pfeffer, M.A. Clinical Significance of Mitral Regurgitation After Acute Myocardial Infarction. Circulation 1997, 96, 827–833. [Google Scholar] [CrossRef]
- Barbour, D.J.; Roberts, W.C. Rupture of a left ventricular papillary muscle during acute myocardial infarction: Analysis of 22 necropsy patients. J. Am. Coll. Cardiol. 1986, 8, 558–565. [Google Scholar] [CrossRef] [Green Version]
- Estes, E.H., Jr.; Dalton, F.M.; Entman, M.L.; Dixon, H.B.; Hackel, D.B. The anatomy and blood supply of the papillary muscles of the left ventricle. Am. Heart J. 1966, 71, 356–362. [Google Scholar] [CrossRef]
- Bouma, W.; Wijdh-den Hamer, I.J.; Klinkenberg, T.J.; Kuijpers, M.; Bijleveld, A.; Van Der Horst, I.C.; Erasmus, M.E.; Gorman, I.J.H.; Gorman, R.C.; Mariani, M.A. Mitral valve repair for post-myocardial infarction papillary muscle rupture. Eur. J. Cardio-Thorac. Surg. 2013, 44, 1063–1069. [Google Scholar] [CrossRef] [Green Version]
- Bouma, W.; Wijdh-den Hamer, I.J.; Koene, B.M.; Kuijpers, M.; Natour, E.; E Erasmus, M.; Van Der Horst, I.C.C.; Iii, J.H.G.; Gorman, R.C.; A Mariani, M. Predictors of in-hospital mortality after mitral valve surgery for post-myocardial infarction papillary muscle rupture. J. Cardiothorac. Surg. 2014, 9, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matteucci, M.; Formica, F.; Kowalewski, M.; Massimi, G.; Ronco, D.; Beghi, C.; Lorusso, R. Meta-analysis of surgical treatment for postinfarction left ventricular free-wall rupture. J. Card. Surg. 2021, 36, 3326–3333. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, N.; Puymirat, E.; Delmas, C.; Ortuno, S.; Durand, E.; Bataille, V.; Drouet, E.; Bonello, L.; Bonnefoy-Cudraz, E.; Lesmeles, G.; et al. Trends in cardiogenic shock complicating acute myocardial infarction. Eur. J. Heart Fail. 2020, 22, 664–672. [Google Scholar] [CrossRef]
- Acharya, D. Predictors of Outcomes in Myocardial Infarction and Cardiogenic Shock. Cardiol. Rev. 2018, 26, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Valuckiene, Z.; Budrys, P.; Jurkevicius, R. Predicting ischemic mitral regurgitation in patients with acute ST-elevation myocardial infarction: Does time to reperfusion really matter and what is the role of collateral circulation? Int. J. Cardiol. 2016, 203, 667–671. [Google Scholar] [CrossRef] [Green Version]
- Schroeter, T.; Lehmann, S.; Misfeld, M.; Borger, M.; Subramanian, S.; Mohr, F.W.; Bakthiary, F. Clinical Outcome After Mitral Valve Surgery Due to Ischemic Papillary Muscle Rupture. Ann. Thorac. Surg. 2013, 95, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Morillon-Lutun, S.; Maucort-Boulch, D.; Mewton, N.; Farhat, F.; Bresson, D.; Girerd, N.; Desebbe, O.; Henaine, R.; Kirkorian, G.; Bonnefoy-Cudraz, E. Therapeutic Management Changes and Mortality Rates over 30 Years in Ventricular Septal Rupture Complicating Acute Myocardial Infarction. Am. J. Cardiol. 2013, 112, 1273–1278. [Google Scholar] [CrossRef]
- Moreyra, A.E.; Huang, M.S.; Wilson, A.C.; Deng, Y.; Cosgrove, N.M.; Kostis, J.B.; MIDAS Study Group (MIDAS 13). Trends in Incidence and Mortality Rates of Ventricular Septal Rupture During Acute Myocardial Infarction. Am. J. Cardiol. 2010, 106, 1095–1100. [Google Scholar] [CrossRef]
- Rueda, F.; Borràs, E.; García-García, C.; Iborra-Egea, O.; Revuelta-López, E.; Harjola, V.-P.; Cediel, G.; Lassus, J.; Tarvasmäki, T.; Mebazaa, A.; et al. Protein-based cardiogenic shock patient classifier. Eur. Heart J. 2019, 40, 2684–2694. [Google Scholar] [CrossRef] [Green Version]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Christopher, E.B.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early Revascularization in Acute Myocardial Infarction Complicated by Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef] [Green Version]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Dzavik, V.; Buller, C.E.; Aylward, P.; Col, J.; White, H.D.; SHOCK Investigators. Early Revascularization and Long-term Survival in Cardiogenic Shock Complicating Acute Myocardial Infarction. JAMA 2006, 295, 2511–2515. [Google Scholar] [CrossRef] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Giménez, M.R.; Miller, P.E.; Alviar, C.L.; Van Diepen, S.; Granger, C.B.; Montalescot, G.; Windecker, S.; Maier, L.; Serpytis, P.; Serpytis, R.; et al. Outcomes Associated with Respiratory Failure for Patients with Cardiogenic Shock and Acute Myocardial Infarction: A Substudy of the CULPRIT-SHOCK Trial. J. Clin. Med. 2020, 9, 860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feistritzer, H.-J.; Desch, S.; Freund, A.; Poess, J.; Zeymer, U.; Ouarrak, T.; Schneider, S.; De Waha-Thiele, S.; Fuernau, G.; Eitel, I.; et al. Prognostic Impact of Active Mechanical Circulatory Support in Cardiogenic Shock Complicating Acute Myocardial Infarction, Results from the Culprit-Shock Trial. J. Clin. Med. 2020, 9, 1976. [Google Scholar] [CrossRef]
- Thiele, H.; Akin, I.; Sandri, M.; Fuernau, G.; De Waha, S.; Meyer-Saraei, R.; Nordbeck, P.; Geisler, T.; Landmesser, U.; Skurk, C.; et al. PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock. N. Engl. J. Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunwald, E.; A Kloner, R. Myocardial reperfusion: A double-edged sword? J. Clin. Investig. 1985, 76, 1713–1719. [Google Scholar] [CrossRef]
- Kloner, R.A. Current State of Clinical Translation of Cardioprotective Agents for Acute Myocardial Infarction. Circ. Res. 2013, 113, 451–463. [Google Scholar] [CrossRef] [Green Version]
- Zalewski, J.; Claus, P.; Bogaert, J.; Driessche, N.V.; Driesen, R.B.; Galan, D.T.; Sipido, K.R.; Buszman, P.; Milewski, K.; Van De Werf, F. Cyclosporine A reduces microvascular obstruction and preserves left ventricular function deterioration following myocardial ischemia and reperfusion. Basic Res. Cardiol. 2015, 110, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zalewski, J.; Durak, M.; Lech, P.; Gajos, G.; Undas, A.; Nessler, J.; Rosławiecka, A.; Zmudka, K. Platelet activation and microvascular injury in patients with ST-segment elevation myocardial infarction. Kardiol. Pol. 2012, 70, 677–684. [Google Scholar]
- Hamirani, Y.S.; Wong, A.; Kramer, C.M.; Salerno, M. Effect of Microvascular Obstruction and Intramyocardial Hemorrhage by CMR on LV Remodeling and Outcomes After Myocardial Infarction: A systematic review and meta-analysis. JACC Cardiovasc. Imaging 2014, 7, 940–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinstadler, S.J.; Fuernau, G.; Eitel, C.; De Waha, S.; Desch, S.; Metzler, B.; Schuler, G.; Thiele, H.; Eitel, I. Shock Index as a Predictor of Myocardial Damage and Clinical Outcome in ST-Elevation Myocardial Infarction. Circ. J. 2016, 80, 924–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnaoutakis, G.J.; Zhao, Y.; George, T.J.; Sciortino, C.M.; McCarthy, P.M.; Conte, J.V. Surgical Repair of Ventricular Septal Defect After Myocardial Infarction: Outcomes From The Society of Thoracic Surgeons National Database. Ann. Thorac. Surg. 2012, 94, 436–444. [Google Scholar] [CrossRef] [Green Version]
- Thiele, H.; Lauer, B.; Hambrecht, R.; Boudriot, E.; Sick, P.; Niebauer, J.; Falk, V.; Schuler, G. Short- and long-term hemodynamic effects of intra-aortic balloon support in ventricular septal defect complicating acute myocardial infarction. Am. J. Cardiol. 2003, 92, 450–454. [Google Scholar] [CrossRef]
- Koh, A.S.; Loh, Y.J.; Lim, Y.P.; Le Tan, J. Ventricular septal rupture following acute myocardial infarction. Acta Cardiol. 2011, 66, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Harmon, L.; Boccalandro, F. Cardiogenic shock secondary to severe acute ischemic mitral regurgitation managed with an impella 2.5 percutaneous left ventricular assist device. Catheter. Cardiovasc. Interv. 2011, 79, 1129–1134. [Google Scholar] [CrossRef]
- Scherer, C.; Lüsebrink, E.; Kupka, D.; Stocker, T.J.; Stark, K.; Stremmel, C.; Orban, M.; Petzold, T.; Germayer, A.; Mauthe, K.; et al. Long-Term Clinical Outcome of Cardiogenic Shock Patients Undergoing Impella CP Treatment vs. Standard of Care. J. Clin. Med. 2020, 9, 3803. [Google Scholar] [CrossRef]
- Schrage, B.; Becher, P.M.; Goßling, A.; Savarese, G.; Dabboura, S.; Yan, I.; Beer, B.; Söffker, G.; Seiffert, M.; Kluge, S.; et al. Temporal trends in incidence, causes, use of mechanical circulatory support and mortality in cardiogenic shock. ESC Heart Fail. 2021, 8, 1295–1303. [Google Scholar] [CrossRef]
- Asleh, R.; Resar, J.R. Utilization of Percutaneous Mechanical Circulatory Support Devices in Cardiogenic Shock Complicating Acute Myocardial Infarction and High-Risk Percutaneous Coronary Interventions. J. Clin. Med. 2019, 8, 1209. [Google Scholar] [CrossRef] [Green Version]
- Ouweneel, D.M.; Eriksen, E.; Sjauw, K.D.; van Dongen, I.M.; Hirsch, A.; Packer, E.J.; Vis, M.M.; Wykrzykowska, J.; Koch, K.T.; Baan, J.; et al. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2017, 69, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Kutty, R.S.; Jones, N.; Moorjani, N. Mechanical Complications of Acute Myocardial Infarction. Cardiol. Clin. 2013, 31, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, P.; Burri, H.; Fahrat, F.; Cucherat, M.; Jegaden, O.; Obadia, J.-F.; Kirkorian, G.; Touboul, P. Perioperative outcome and long-term survival of surgery for acute post-infarction mitral regurgitation. Eur. J. Cardio-Thorac. Surg. 2004, 26, 330–335. [Google Scholar] [CrossRef] [Green Version]
- Lorusso, R.; Gelsomino, S.; De Cicco, G.; Beghi, C.; Russo, C.; De Bonis, M.; Colli, A.; Sala, A. Mitral valve surgery in emergency for severe acute regurgitation: Analysis of postoperative results from a multicentre study. Eur. J. Cardio-Thorac. Surg. 2008, 33, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Kishon, Y.; Oh, J.K.; Schaff, H.V.; Mullany, C.J.; Tajik, A.J.; Gersh, B.J. Mitral Valve Operation in Postinfarction Rupture of a Papillary Muscle: Immediate Results and Long-Term Follow-Up of 22 Patients. Mayo Clin. Proc. 1992, 67, 1023–1030. [Google Scholar] [CrossRef]
- Russo, A.; Suri, R.M.; Grigioni, F.; Roger, V.L.; Oh, J.K.; Mahoney, D.W.; Schaff, H.; Enriquez-Sarano, M. Clinical Outcome After Surgical Correction of Mitral Regurgitation Due to Papillary Muscle Rupture. Circulation 2008, 118, 1528–1534. [Google Scholar] [CrossRef] [Green Version]
- Molek, P.; Wlodarczyk, A.; Gajos, G.; Nessler, J.; Zalewski, J. Simultaneous cardiac free wall rupture and ventricular septal rupture following acute myocardial infarction treated with emergency balloon closure. Pol. Arch. Intern. Med. 2019, 129, 830–832. [Google Scholar] [CrossRef]
- Bartlett, R.H.; Chapman, R.A. Economics of ECLS. In Extracorporeal Cardiopulmonary Support in Critical Care, 3rd ed.; Van Meurs, K., Lally, K.P., Peek, G., Eds.; ESLO: Ann Arbor, MI, USA, 2005; pp. 203–215. [Google Scholar]
- Sjauw, K.D.; Engström, A.E.; Vis, M.M.; Van Der Schaaf, R.J.; Baan, J.; Koch, K.T.; De Winter, R.J.; Piek, J.J.; Tijssen, J.G.; Henriques, J.P. A systematic review and meta-analysis of intra-aortic balloon pump therapy in ST-elevation myocardial infarction: Should we change the guidelines? Eur. Heart J. 2008, 30, 459–468. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Lim, S.-H.; Hong, J.; Hong, Y.-S.; Lee, C.J.; Jung, J.-H.; Yu, S. Efficacy of veno-arterial extracorporeal membrane oxygenation in acute myocardial infarction with cardiogenic shock. Resuscitation 2012, 83, 971–975. [Google Scholar] [CrossRef]
- Tsao, N.-W.; Shih, C.-M.; Yeh, J.-S.; Kao, Y.-T.; Hsieh, M.-H.; Ou, K.-L.; Chen, J.-W.; Shyu, K.-G.; Weng, Z.-C.; Chang, N.-C.; et al. Extracorporeal membrane oxygenation–assisted primary percutaneous coronary intervention may improve survival of patients with acute myocardial infarction complicated by profound cardiogenic shock. J. Crit. Care 2012, 27, 530.e1–530.e11. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Freund, A.; Gimenez, M.R.; de Waha-Thiele, S.; Akin, I.; Pöss, J.; Feistritzer, H.-J.; Fuernau, G.; Graf, T.; Nef, H.; et al. Extracorporeal life support in patients with acute myocardial infarction complicated by cardiogenic shock—Design and rationale of the ECLS-SHOCK trial. Am. Heart J. 2021, 234, 1–11. [Google Scholar] [CrossRef]
- Burkhoff, D.; Cohen, H.; Brunckhorst, C.; O’Neill, W.W.; TandemHeart Investigators Group. A randomized multicenter clinical study to evaluate the safety and efficacy of the TandemHeart percutaneous ventricular assist device versus conventional therapy with intraaortic balloon pumping for treatment of cardiogenic shock. Am. Heart J. 2006, 152, 469.e1–469.e8. [Google Scholar] [CrossRef]
- Thiele, H.; Sick, P.; Boudriot, E.; Diederich, K.-W.; Hambrecht, R.; Niebauer, J.; Schuler, G. Randomized comparison of intra-aortic balloon support with a percutaneous left ventricular assist device in patients with revascularized acute myocardial infarction complicated by cardiogenic shock. Eur. Heart J. 2005, 26, 1276–1283. [Google Scholar] [CrossRef] [Green Version]
- Seyfarth, M.; Sibbing, D.; Bauer, I.; Fröhlich, G.; Bott-Flügel, L.; Byrne, R.; Dirschinger, J.; Kastrati, A.; Schömig, A. A Randomized Clinical Trial to Evaluate the Safety and Efficacy of a Percutaneous Left Ventricular Assist Device Versus Intra-Aortic Balloon Pumping for Treatment of Cardiogenic Shock Caused by Myocardial Infarction. J. Am. Coll. Cardiol. 2008, 52, 1584–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engström, A.E.; Cocchieri, R.; Driessen, A.H.; Sjauw, K.D.; Vis, M.M.; Baan, J.; de Jong, M.; Lagrand, W.K.; van der Sloot, J.A.P.; Tijssen, J.G.; et al. The Impella 2.5 and 5.0 devices for ST-elevation myocardial infarction patients presenting with severe and profound cardiogenic shock: The Academic Medical Center intensive care unit experience*. Crit. Care Med. 2011, 39, 2072–2079. [Google Scholar] [CrossRef] [Green Version]
- Lauten, A.; Engström, A.E.; Jung, C.; Empen, K.; Erne, P.; Cook, S.; Windecker, S.; Bergmann, M.W.; Klingenberg, R.; Lüscher, T.F.; et al. Percutaneous Left-Ventricular Support With the Impella-2.5–Assist Device in Acute Cardiogenic Shock: Results of the Impella-EUROSHOCK-registry. Circ. Heart Fail. 2013, 6, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assenza, G.E.; McElhinney, D.B.; Valente, A.M.; Pearson, D.D.; Volpe, M.; Martucci, G.; Landzberg, M.J.; Lock, J.E. Transcatheter Closure of Post-myocardial Infarction Ventricular Septal Rupture. Circ. Cardiovasc. Interv. 2013, 6, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Thiele, H.; Kaulfersch, C.; Daehnert, I.; Schoenauer, M.; Eitel, I.; Borger, M.; Schuler, G. Immediate primary transcatheter closure of postinfarction ventricular septal defects. Eur. Heart J. 2008, 30, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Calvert, P.A.; Cockburn, J.; Wynne, D.; Ludman, P.; Rana, B.S.; Northridge, D.; Mullen, M.J.; Malik, I.; Turner, M.; Khogali, S.; et al. Percutaneous Closure of Postinfarction Ventricular Septal Defect: In-hospital outcomes and long-term follow-up of UK experience. Circulation 2014, 129, 2395–2402. [Google Scholar] [CrossRef] [PubMed]
- Bilge, M.; Alemdar, R.; Yasar, A.S. Successful percutaneous mitral valve repair with the mitraclip system of acute mitral regurgitation due to papillary muscle rupture as complication of acute myocardial infarction. Catheter. Cardiovasc. Interv. 2014, 83, E137–E140. [Google Scholar] [CrossRef] [PubMed]
- Bahlmann, E.; Frerker, C.; Kreidel, F.; Thielsen, T.; Ghanem, A.; van der Schalk, H.; Grahn, H.; Kuck, K.-H. MitraClip Implantation After Acute Ischemic Papillary Muscle Rupture in a Patient With Prolonged Cardiogenic Shock. Ann. Thorac. Surg. 2015, 99, e41–e42. [Google Scholar] [CrossRef]
- Canovas, S.J.; Lim, E.; Dalmau, M.J.; Bueno, M.; Buendía, J.; Hornero, F.; Gil, O.; Garcia, R.; Paya, R.; Perez, J.; et al. Midterm Clinical and Echocardiographic Results With Patch Glue Repair of Left Ventricular Free Wall Rupture. Circulation 2003, 108, II-237–II-240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, H.; Masuo, M.; Yoshimoto, H.; Toyama, J.; Shimada, M.; Shimamura, Y.; Hojo, H.; Kondo, K.; Kitamura, S.; Miura, Y. Oozing Type Cardiac Rupture Repaired With Percutaneous Injection of Fibrin-Glue Into the Pericardial Space: Case report. Jpn. Circ. J. 2000, 64, 312–315. [Google Scholar] [CrossRef] [Green Version]
- Zalewski, J.; Lewicki, L.; Krawczyk, K.; Zabczyk, M.; Targonski, R.; Molek, P.; Nessler, J.; Undas, A. Polyhedral erythrocytes in intracoronary thrombus and their association with reperfusion in myocardial infarction. Clin. Res. Cardiol. 2019, 108, 950–962. [Google Scholar] [CrossRef]
- Zalewski, J.; Zmudka, K.; Musialek, P.; Zajdel, W.; Pieniążek, P.; Kadzielski, A.; Przewlocki, T. Detection of microvascular injury by evaluating epicardial blood flow in early reperfusion following primary angioplasty. Int. J. Cardiol. 2004, 96, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Gajos, G.; Zalewski, J.; Mostowik, M.; Konduracka, E.; Nessler, J.; Undas, A. Polyunsaturated omega-3 fatty acids reduce lipoprotein-associated phospholipase A2 in patients with stable angina. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 434–439. [Google Scholar] [CrossRef]
- Zalewski, J.; Bogaerts, K.; Desmet, W.; Sinnaeve, P.; Berger, P.; Grines, C.; Danays, T.; Armstrong, P.; Van De Werf, F. Intraluminal Thrombus in Facilitated Versus Primary Percutaneous Coronary Intervention: An Angiographic Substudy of the ASSENT-4 PCI (Assessment of the Safety and Efficacy of a New Treatment Strategy with Percutaneous Coronary Intervention) Trial. J. Am. Coll. Cardiol. 2011, 57, 1867–1873. [Google Scholar] [CrossRef] [PubMed]
- Zalewski, J.; Nycz, K.; Przewlocki, T.; Durak, M.; Cul, M.; Zajdel, W.; Zmudka, K. Evolution of myocardial perfusion during primary angioplasty in spontaneously reperfused infarct-related artery. Int. J. Cardiol. 2011, 147, 25–31. [Google Scholar] [CrossRef]
- Iborra-Egea, O.; Rueda, F.; García-García, C.; Borràs, E.; Sabidó, E.; Bayes-Genis, A. Molecular signature of cardiogenic shock Impact on long-term clinical outcomes and left ventricular function recovery. Eur. Heart J. 2020, 41, 3839–3848. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zalewski, J.; Nowak, K.; Furczynska, P.; Zalewska, M. Complicating Acute Myocardial Infarction. Current Status and Unresolved Targets for Subsequent Research. J. Clin. Med. 2021, 10, 5904. https://doi.org/10.3390/jcm10245904
Zalewski J, Nowak K, Furczynska P, Zalewska M. Complicating Acute Myocardial Infarction. Current Status and Unresolved Targets for Subsequent Research. Journal of Clinical Medicine. 2021; 10(24):5904. https://doi.org/10.3390/jcm10245904
Chicago/Turabian StyleZalewski, Jaroslaw, Karol Nowak, Patrycja Furczynska, and Magdalena Zalewska. 2021. "Complicating Acute Myocardial Infarction. Current Status and Unresolved Targets for Subsequent Research" Journal of Clinical Medicine 10, no. 24: 5904. https://doi.org/10.3390/jcm10245904
APA StyleZalewski, J., Nowak, K., Furczynska, P., & Zalewska, M. (2021). Complicating Acute Myocardial Infarction. Current Status and Unresolved Targets for Subsequent Research. Journal of Clinical Medicine, 10(24), 5904. https://doi.org/10.3390/jcm10245904