
Teaching Microsurgical Breast Reconstruction—A Retrospective Cohort Study

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Training Concept
2.2. Statistical Analysis
2.3. Standard Surgical Technique
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D. Breast Cancer Statistics 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- American Society of Plastic Surgeons. 2018 Plastic Surgery Statistics Report; American Society of Plastic Surgeons: Arlington Heights, IL, USA, 2018. [Google Scholar]
- Erdmann-Sager, J.; Wilkins, E.G.; Pusic, A.L.; Qi, J.; Hamill, J.B.; Kim, H.M.; Guldbrandsen, G.E.; Chun, Y.S. Complications and Patient-Reported Outcomes after Abdominally Based Breast Reconstruction: Results of the Mastectomy Reconstruction Outcomes Consortium Study. Plast. Reconstr. Surg. 2018, 141, 271–281. [Google Scholar] [CrossRef]
- Pien, I.; Caccavale, S.; Cheung, M.C.; Butala, P.; Hughes, D.B.; Ligh, C.; Zenn, M.R.; Hollenbeck, S.T. Evolving Trends in Autologous Breast Reconstruction: Is the Deep Inferior Epigastric Artery Perforator Flap Taking Over? Ann. Plast. Surg. 2016, 76, 489–493. [Google Scholar] [CrossRef]
- Allen, R.J.; Treece, P. Deep inferior epigastric perforator flap for breast reconstruction. Ann. Plast. Surg. 1994, 32, 32–38. [Google Scholar] [CrossRef]
- Blondeel, P.N. One hundred free DIEP flap breast reconstructions: A personal experience. Br. J. Plast. Surg. 1999, 52, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Macadam, S.A.; Bovill, E.S.; Buchel, E.W.; Lennox, P.A. Evidence-Based Medicine: Autologous Breast Reconstruction. Plast. Reconstr. Surg. 2017, 139, 204e–229e. [Google Scholar] [CrossRef]
- Nelson, J.A.; Guo, Y.; Sonnad, S.S.; Low, D.W.; Kovach, S.J., 3rd; Wu, L.C.; Serletti, J.M. A Comparison between DIEP and muscle-sparing free TRAM flaps in breast reconstruction: A single surgeon’s recent experience. Plast. Reconstr. Surg. 2010, 126, 1428–1435. [Google Scholar] [CrossRef]
- Selber, J.C.; Nelson, J.; Fosnot, J.; Goldstein, J.; Bergey, M.; Sonnad, S.S.; Serletti, J.M. A prospective study comparing the functional impact of SIEA, DIEP, and muscle-sparing free TRAM flaps on the abdominal wall: Part I. unilateral reconstruction. Plast. Reconstr. Surg. 2010, 126, 1142–1153. [Google Scholar] [CrossRef]
- Atisha, D.; Alderman, A.K. A systematic review of abdominal wall function following abdominal flaps for postmastectomy breast reconstruction. Ann. Plast. Surg. 2009, 63, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Hangge, P.T.; Jogerst, K.; Mohsen, A.; Kosiorek, H.; Cronin, P.A.; Stucky, C.H.; Wasif, N.; Gray, R.J.; Rebecca, A.M.; Casey, W.J., 3rd; et al. Making an informed choice: Which breast reconstruction type has the lowest complication rate? Am. J. Surg. 2019, 218, 1040–1045. [Google Scholar] [CrossRef]
- Kronowitz, S.J.; Robb, G.L. Radiation therapy and breast reconstruction: A critical review of the literature. Plast. Reconstr. Surg. 2009, 124, 395–408. [Google Scholar] [CrossRef]
- Aliu, O.; Zhong, L.; Chetta, M.D.; Sears, E.D.; Ballard, T.; Waljee, J.F.; Chung, K.C.; Momoh, A.O. Comparing Health Care Resource Use between Implant and Autologous Reconstruction of the Irradiated Breast: A National Claims-Based Assessment. Plast. Reconstr. Surg. 2017, 139, 1224e–1231e. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.A.; Voineskos, S.H.; Qi, J.; Kim, H.M.; Hamill, J.B.; Wilkins, E.G.; Pusic, A.L. Elective Revisions after Breast Reconstruction: Results from the Mastectomy Reconstruction Outcomes Consortium. Plast. Reconstr. Surg. 2019, 144, 1280–1290. [Google Scholar] [CrossRef]
- Razdan, S.N.; Cordeiro, P.G.; Albornoz, C.R.; Ro, T.; Cohen, W.A.; Mehrara, B.J.; McCarthy, C.M.; Disa, J.J.; Pusic, A.L.; Matros, E. Cost-Effectiveness Analysis of Breast Reconstruction Options in the Setting of Postmastectomy Radiotherapy Using the BREAST-Q. Plast. Reconstr. Surg. 2016, 137, 510e–517e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Disa, J.J.; Cordeiro, P.G.; Hidalgo, D.A. Efficacy of conventional monitoring techniques in free tissue transfer: An 11-year experience in 750 consecutive cases. Plast. Reconstr. Surg. 1999, 104, 97–101. [Google Scholar] [CrossRef]
- Salgarello, M.; Pagliara, D.; Rossi, M.; Visconti, G.; Barone-Adesi, L. Postoperative Monitoring of Free DIEP Flap in Breast Reconstruction with Near-Infrared Spectroscopy: Variables Affecting the Regional Oxygen Saturation. J. Reconstr. Microsurg. 2018, 34, 383–388. [Google Scholar] [CrossRef]
- Salgarello, M.; Pagliara, D.; Rossi, M.; Visconti, G.; Barone-Adesi, L. Tissue Oximetry Monitoring for Free Deep Inferior Epigastric Perforator Flap Viability: Factors to be Considered toward Optimizing Postoperative Outcome. J. Reconstr. Microsurg. 2018, 34, e4. [Google Scholar] [CrossRef]
- Hofer, S.O.; Damen, T.H.; Mureau, M.A.; Rakhorst, H.A.; Roche, N.A. A Critical Review of Perioperative Complications in 175 Free Deep Inferior Epigastric Perforator Flap Breast Reconstructions. Ann. Plast. Surg. 2007, 59, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Hallock, G.G. Is There a “Learning Curve” for Muscle Perforator Flaps? Ann. Plast. Surg. 2008, 60, 146–149. [Google Scholar] [CrossRef]
- Busic, V.; Das-Gupta, R.; Mesic, H.; Begic, A. The deep inferior epigastric perforator flap for breast reconstruction, the learning curve explored. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Grinsell, D.G.; McCoubrey, G.W.; Finkemeyer, J.P. The Deep Inferior Epigastric Perforator Learning Curve in the Current Era. Ann. Plast. Surg. 2016, 76, 72–77. [Google Scholar] [CrossRef]
- Hirche, C.; Kneser, U.; Xiong, L.; Wurzer, P.; Ringwald, F.; Obitz, F.; Fischer, S.; Harhaus, L.; Gazyakan, E.; Kremer, T. Microvascular free flaps are a safe and suitable training procedure during structured plastic surgery residency: A comparative cohort study with 391 patients. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 715–721. [Google Scholar] [CrossRef]
- Kotsougiani, D.; Ringwald, F.; Hundepool, C.A.; Neubrech, F.; Kremer, T.; Bickert, B.; Kneser, U.; Hirche, C. Safety and Suitability of Finger Replantations as a Residency Training Procedure: A Retrospective Cohort Study with Analysis of the Initial Postoperative Outcomes. Ann. Plast. Surg. 2017, 78, 431–435. [Google Scholar] [CrossRef]
- Craggs, B.; Vanmierlo, B.; Zeltzer, A.; Buyl, R.; Haentjens, P.; Hamdi, M. Donor-Site Morbidity following Harvest of the Transverse Myocutaneous Gracilis Flap for Breast Reconstruction. Plast. Reconstr. Surg. 2014, 134, 682e–691e. [Google Scholar] [CrossRef]
- Bodin, F.; Dissaux, C.; Dupret-Bories, A.; Schohn, T.; Fiquet, C.; Bruant-Rodier, C. The transverse musculo-cutaneous gracilis flap for breast reconstruction: How to avoid complications. Microsurgery 2016, 36, 42–48. [Google Scholar] [CrossRef]
- Enajat, M.; Smit, J.M.; Rozen, W.M.; Hartman, E.H.; Liss, A.; Kildal, M.; Audolfsson, T.; Acosta, R. Aesthetic refinements and reoperative procedures following 370 consecutive DIEP and SIEA flap breast reconstructions: Important considerations for patient consent. Aesthetic Plast. Surg. 2010, 34, 306–312. [Google Scholar] [CrossRef]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Klok, J.A.; Cordeiro, P.G.; Cano, S.J. Development of a new patient-reported outcome measure for breast surgery: The BREAST-Q. Plast. Reconstr. Surg. 2009, 124, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Cohen, W.A.; Mundy, L.R.; Ballard, T.N.; Klassen, A.; Cano, S.J.; Browne, J.; Pusic, A.L. The BREAST-Q in surgical research: A review of the literature 2009–2015. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 149–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagliara, D.; Albanese, R.; Storti, G.; Barone-Adesi, L.; Salgarello, M. Patient-reported Outcomes in Immediate and Delayed Breast Reconstruction with Deep Inferior Epigastric Perforator Flap. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1666. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Passive Training | Active Training | After Training | No-Training |
|---|---|---|---|---|
| Total (n) | 34 | 51 | 59 | 45 |
| DIEP (n) | 17 | 24 | 37 | 18 |
| Per trainee | 2.8 | 4 | ||
| Range | 2–4 | 2–7 | ||
| Age (years) | 48.3 | 51.8 | 49.9 | 48.9 |
| p-value | 0.84 | 0.33 | 0.74 | |
| DIEP (%) (vs. MS-TRAM) | 82 | 58 | 89 | 83 |
| p-value | 0.94 | 0.09 | 0.55 | |
| BMI | 29.8 | 30.9 | 30.8 | 31.6 |
| p-value | 0.90 | 0.95 | 0.89 | |
| Smoking (n) | 0 | 3 | 0 | 1 |
| p-value | 0.92 | 0.49 | 0.81 | |
| Hypertension (n) | 2 | 2 | 1 | 3 |
| p-value | 0.91 | 0.82 | 0.70 | |
| Diabetes (n) | 0 | 1 | 0 | 3 |
| p-value | 0.66 | 0.79 | 0.40 | |
| Radiotherapy (%) | 41 | 92 | 65 | 72 |
| p-value | 0.07 | 0.10 | 0.59 | |
| Chemotherapy (%) | 41 | 75 | 51 | 56 |
| p-value | 0.41 | 0.19 | 0.77 | |
| Immediate (%) | 12 | 12 | 11 | 6 |
| p-value | 0.2 | 0.2 | 0.15 | |
| NSM (%) | 0.72 | 0.65 | 0.7 | |
| p-value | 0.2 | 0.2 | 0.15 | |
| TUG (n) | 17 | 27 | 22 | 27 |
| per trainee | 2.8 | 4.5 | ||
| Range | 2–7 | 2–9 | ||
| Age (years) | 48.2 | 45.8 | 40.5 | 41.7 |
| p-value | 0.06 | 0.15 | 0.68 | |
| BMI | 24.9 | 24.0 | 23.0 | 24.3 |
| p-value | 0.90 | 0.99 | 0.81 | |
| Smoking (n) | 2 | 2 | 2 | 0 |
| p-value | 0.70 | 0.78 | 0.55 | |
| Hypertension (n) | 0 | 1 | 3 | 3 |
| p-value | 0.45 | 0.56 | 0.89 | |
| Diabetes (n) | 0 | 0 | 0 | 1 |
| p-value | 0.89 | 0.89 | 0.70 | |
| Radiotherapy (%) | 53 | 33 | 45 | 52 |
| p-value | 0.95 | 0.18 | 0.66 | |
| Chemotherapy (%) | 59 | 43 | 50 | 56 |
| p-value | 0.84 | 0.06 | 0.71 | |
| Immediate (%) | 47 | 32 | 45 | 50 |
| p-value | 0.72 | 0.65 | 0.7 | |
| NSM (%) | 0.72 | 0.65 | 0.7 | |
| p-value | 0.72 | 0.65 | 0.7 |
| Group | Passive Training | Active Training | After Training | No-Training |
|---|---|---|---|---|
| DIEP (n) | 17 | 24 | 37 | 18 |
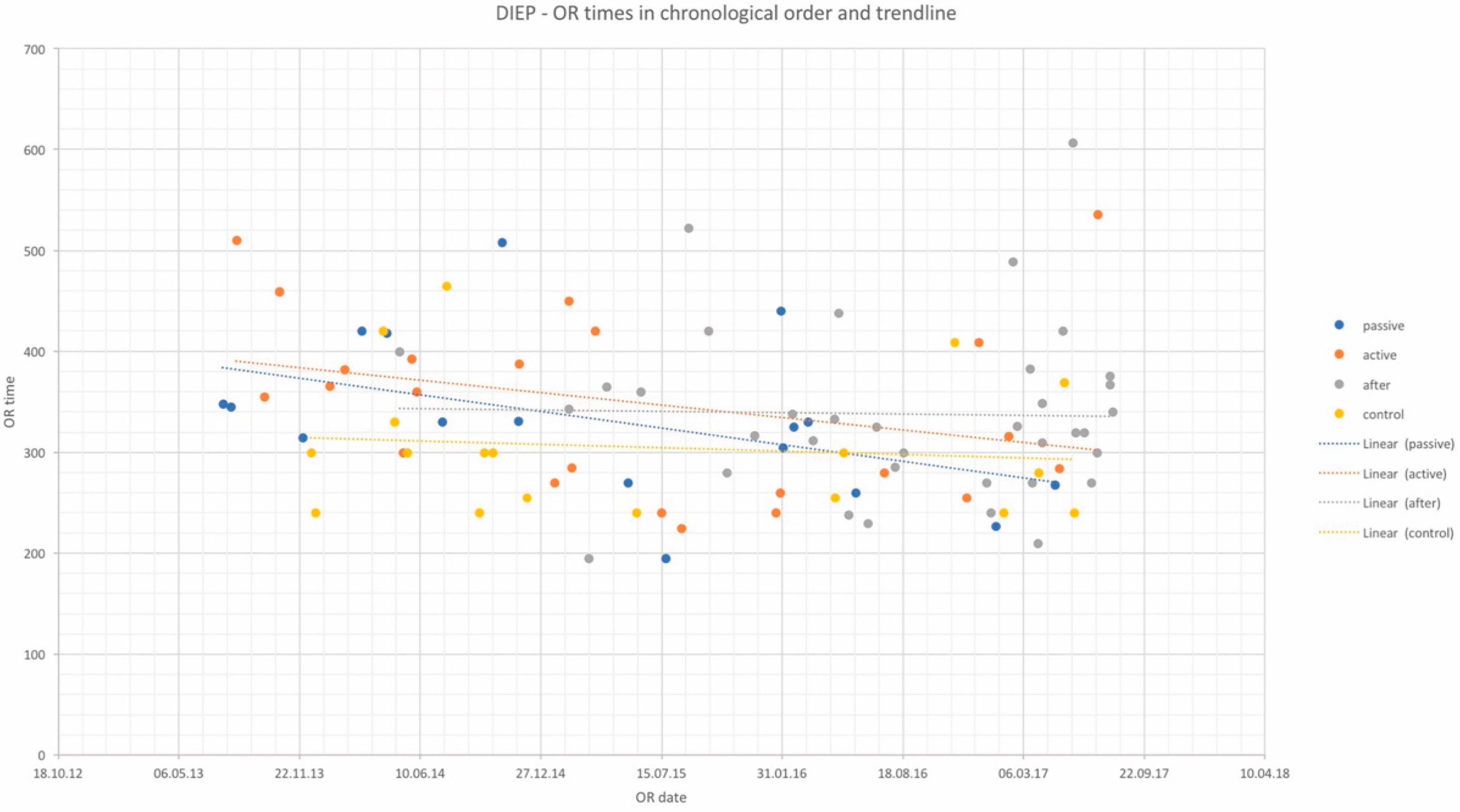
| OR time (min) | 331 | 351 | 338 | 304 |
| p-value | 0.29 | 0.07 | 0.15 | |
| Complications total (%) | 6 | 13 | 16 | 11 |
| p-value | 0.59 | 0.89 | 0.26 | |
| Revisions (%) | 6 | 8 | 5 | 0 |
| p-value | 0.31 | 0.22 | 0.22 | |
| Partial flap loss (%) | 6 | 0 | 3 | 0 |
| p-value | 0.31 | - | 0.49 | |
| Complete flap loss (%) | 0 | 0 | 3 | 0 |
| p-value | - | - | 0.49 | |
| Fat necrosis (%) | 6 | 4 | 5 | 0 |
| p-value | 0.31 | 0.39 | 0.15 | |
| Wound dehiscence recipient site (%) | 6 | 0 | 0 | 0 |
| p-value | 0.49 | - | - | |
| Wound dehiscence donor site (%) | 0 | 0 | 0 | 0 |
| p-value | - | - | - | |
| Infection recipient site (%) | 0 | 0 | 5 | 0 |
| p-value | - | - | 0.6 | |
| Infection donor site (%) | 0 | 0 | 0 | 6 |
| p-value | 0.4 | 0.4 | 0.4 | |
| Hematoma recipient site (%) | 0 | 4 | 3 | 0 |
| p-value | - | 0.11 | 0.26 | |
| Hematoma donor site (%) | 0 | 4 | 3 | 5 |
| p-value | 0.1 | 0.34 | 0.6 | |
| Hernia donor site (%) | 0 | 0 | 3 | 0 |
| p-value | - | - | 0.36 | |
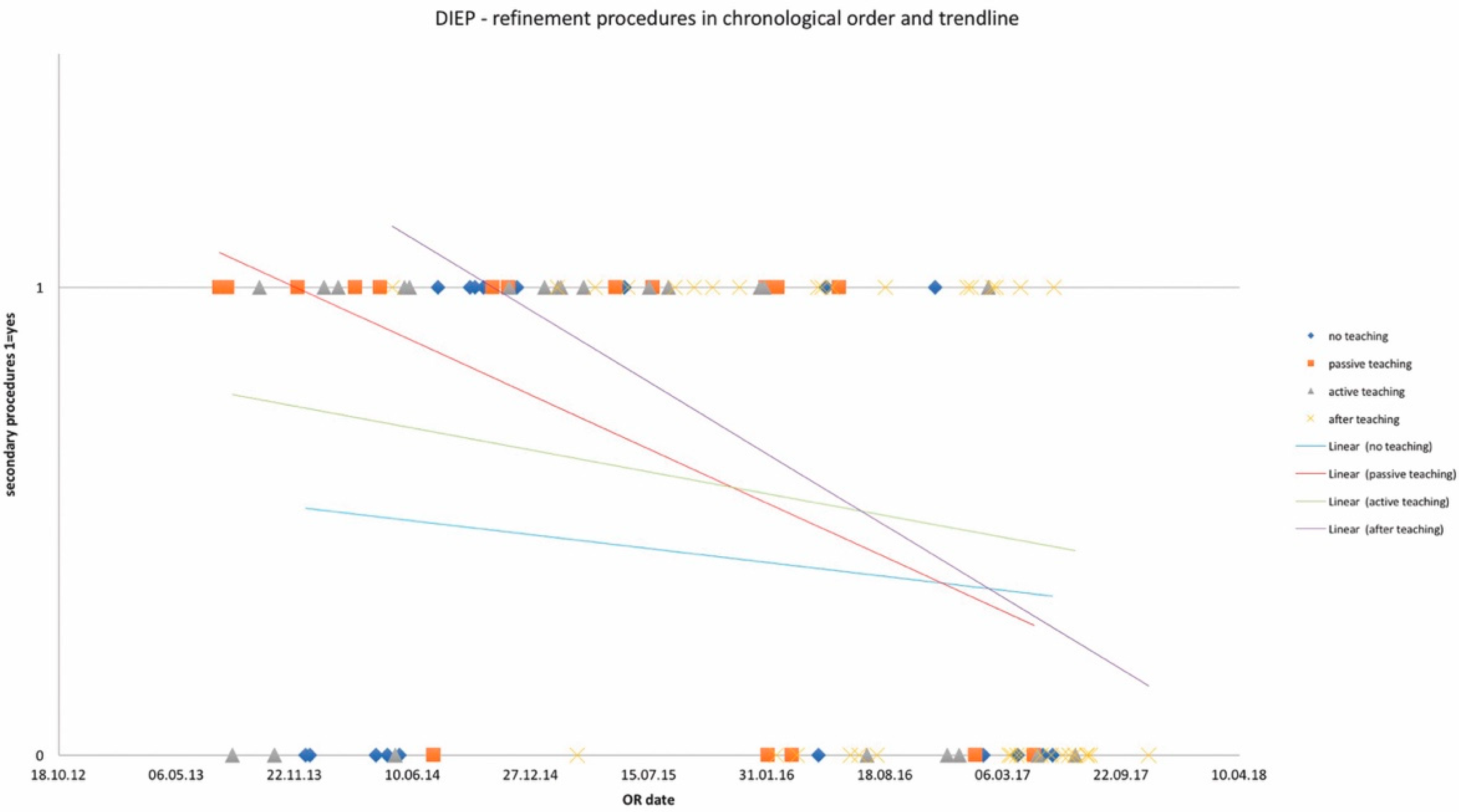
| Refinement procedures (%) | 71 | 63 | 49 | 44 |
| p-value | 0.13 | 0.26 | 0.77 |
| Group | Passive Training | Active Training | After Training | No-Training |
|---|---|---|---|---|
| TUG (n) | 17 | 27 | 22 | 27 |
| OR time (min) | 229 | 214 | 239 | 237 |
| p-value | 0.61 | 0.17 | 0.90 | |
| Complications total (%) | 6 | 19 | 23 | 11 |
| p-value | 0.57 | 0.45 | 0.08 | |
| Revisions (%) | 0 | 4 | 9 | 0 |
| p-value | - | 0.32 | 0.11 | |
| Partial flap loss (%) | 6 | 0 | 0 | 0 |
| p-value | 0.21 | - | - | - |
| Complete flap loss (%) | 0 | 4 | 0 | 0 |
| p-value | - | 0.32 | - | |
| Fat necrosis (%) | 6 | 0 | 0 | 4 |
| p-value | 0.74 | - | - | |
| Wound dehiscence recipient site (%) | 0 | 0 | 0 | 0 |
| p-value | - | - | - | |
| Wound dehiscence donor site (%) | 6 | 11 | 9 | 7 |
| p-value | 0.85 | 0.40 | 0.26 | |
| Infection recipient site (%) | 0 | 0 | 0 | 4 |
| p-value | 0.12 | - | - | |
| Infection donor site (%) | 6 | 4 | 0 | 0 |
| p-value | 0.09 | 0.1 | - | |
| Hematoma recipient site (%) | 6 | 4 | 9 | 0 |
| p-value | 0.09 | 0.1 | 0.07 | |
| Hematoma donor site (%) | 0 | 7 | 9 | 4 |
| p-value | ||||
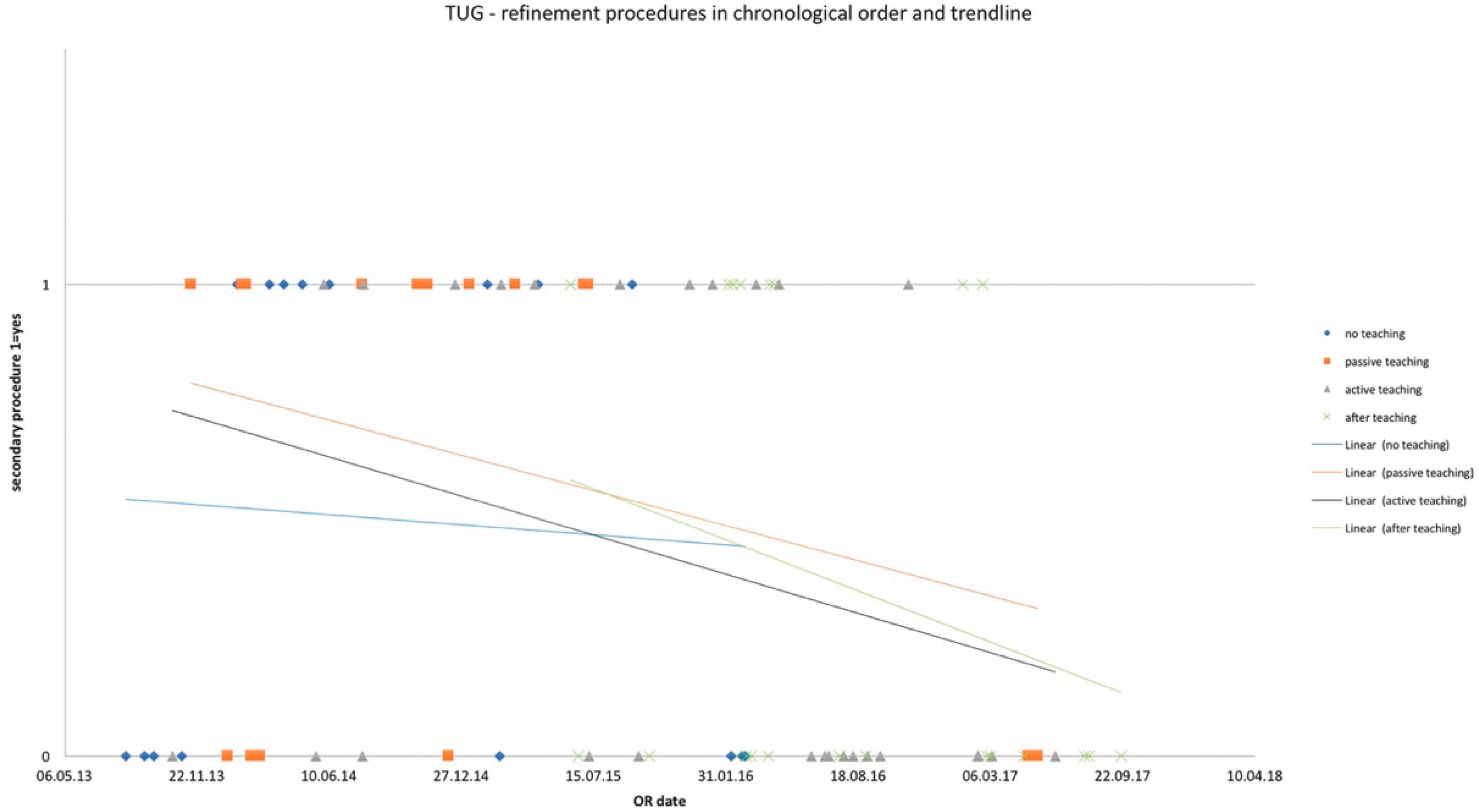
| Refinement procedures (%) | 65 | 41 | 36 | 56 |
| p-value | 0.56 | 0.28 | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fischer, S.; Diehm, Y.F.; Kotsougiani-Fischer, D.; Gazyakan, E.; Radu, C.A.; Kremer, T.; Hirche, C.; Kneser, U. Teaching Microsurgical Breast Reconstruction—A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 5875. https://doi.org/10.3390/jcm10245875
Fischer S, Diehm YF, Kotsougiani-Fischer D, Gazyakan E, Radu CA, Kremer T, Hirche C, Kneser U. Teaching Microsurgical Breast Reconstruction—A Retrospective Cohort Study. Journal of Clinical Medicine. 2021; 10(24):5875. https://doi.org/10.3390/jcm10245875
Chicago/Turabian StyleFischer, Sebastian, Yannick F. Diehm, Dimitra Kotsougiani-Fischer, Emre Gazyakan, Christian A. Radu, Thomas Kremer, Christoph Hirche, and Ulrich Kneser. 2021. "Teaching Microsurgical Breast Reconstruction—A Retrospective Cohort Study" Journal of Clinical Medicine 10, no. 24: 5875. https://doi.org/10.3390/jcm10245875
APA StyleFischer, S., Diehm, Y. F., Kotsougiani-Fischer, D., Gazyakan, E., Radu, C. A., Kremer, T., Hirche, C., & Kneser, U. (2021). Teaching Microsurgical Breast Reconstruction—A Retrospective Cohort Study. Journal of Clinical Medicine, 10(24), 5875. https://doi.org/10.3390/jcm10245875