
The Expression of Prolactin Receptors in Benign Breast Tumors Is Not Associated with Serum Prolactin Level

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. The Ethics Committee
2.2. Research Design
2.3. Evaluation of Serum PRL Level
2.4. Histology and Immunohistochemistry
2.5. SDS-PAGE and Western-Blot
2.6. Statistical Analysis
3. Results
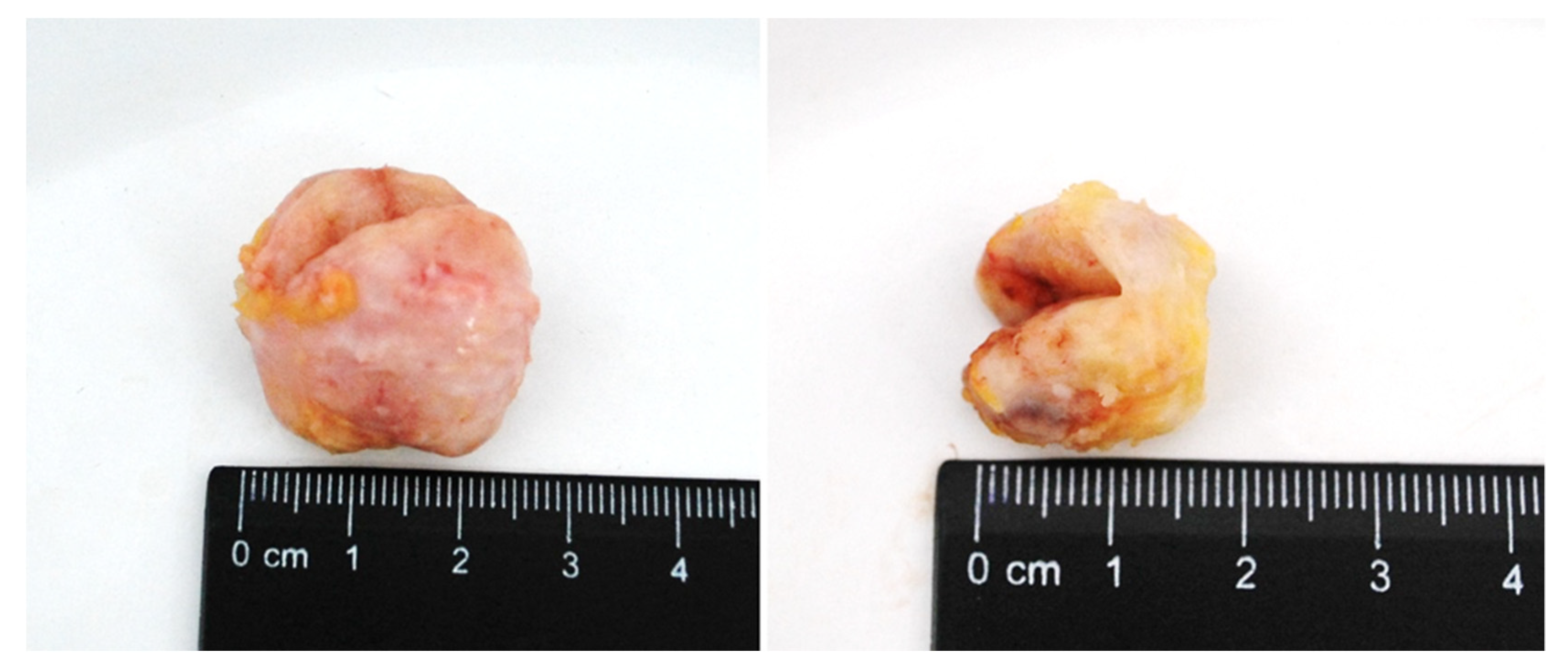
3.1. Macroscopic Study of Breast Tissue
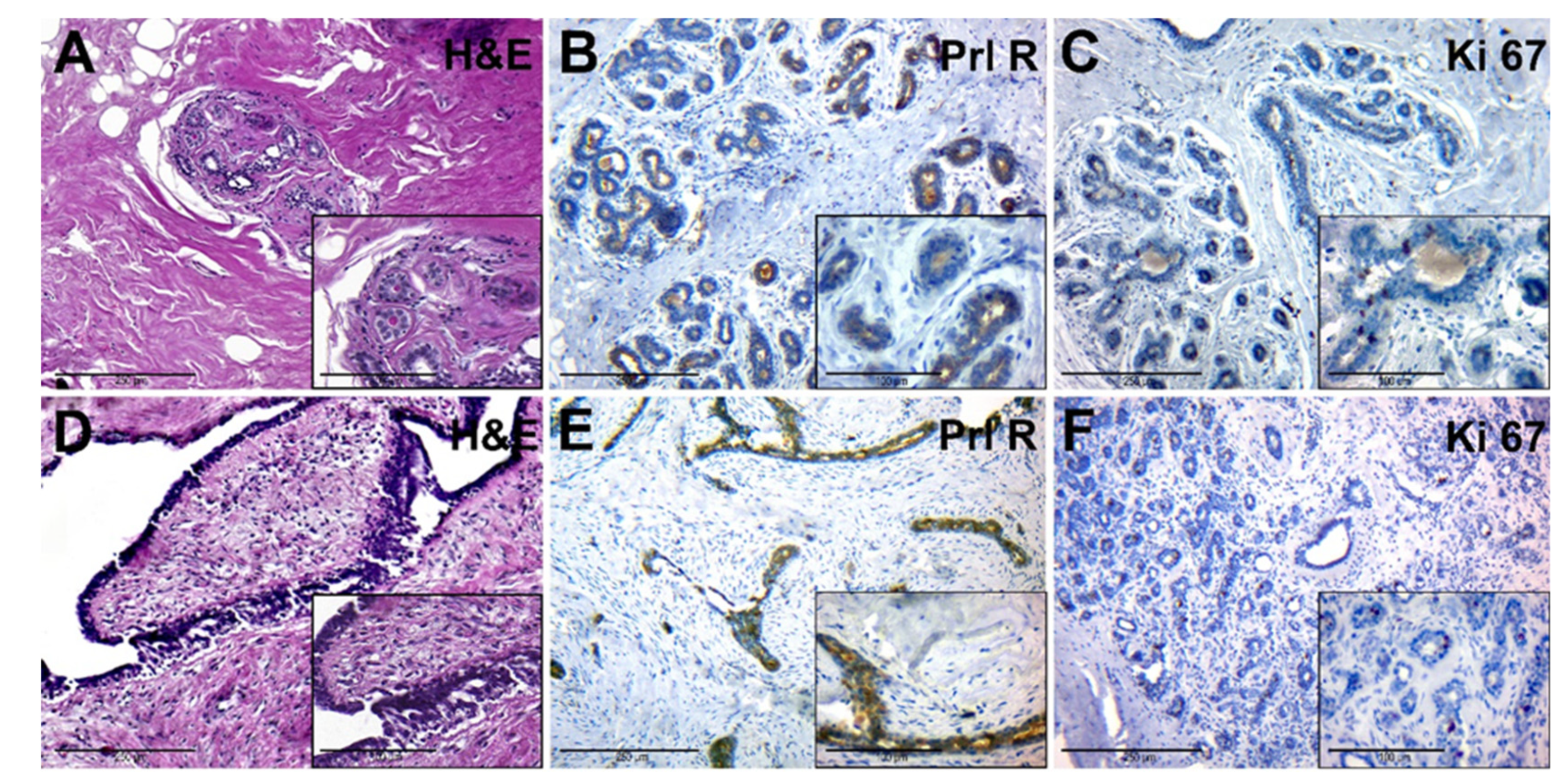
3.2. Histology and Immunohistochemistry
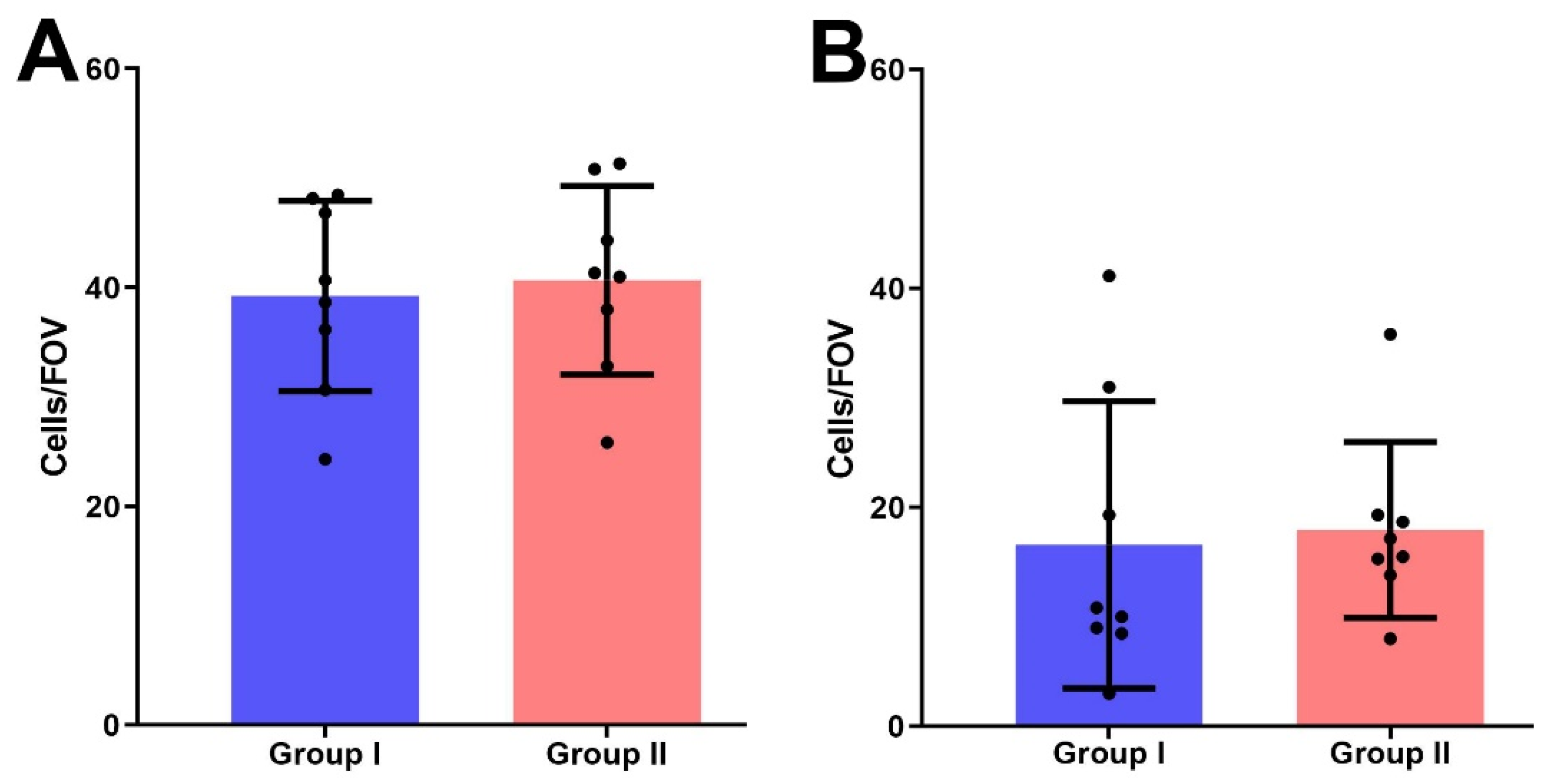
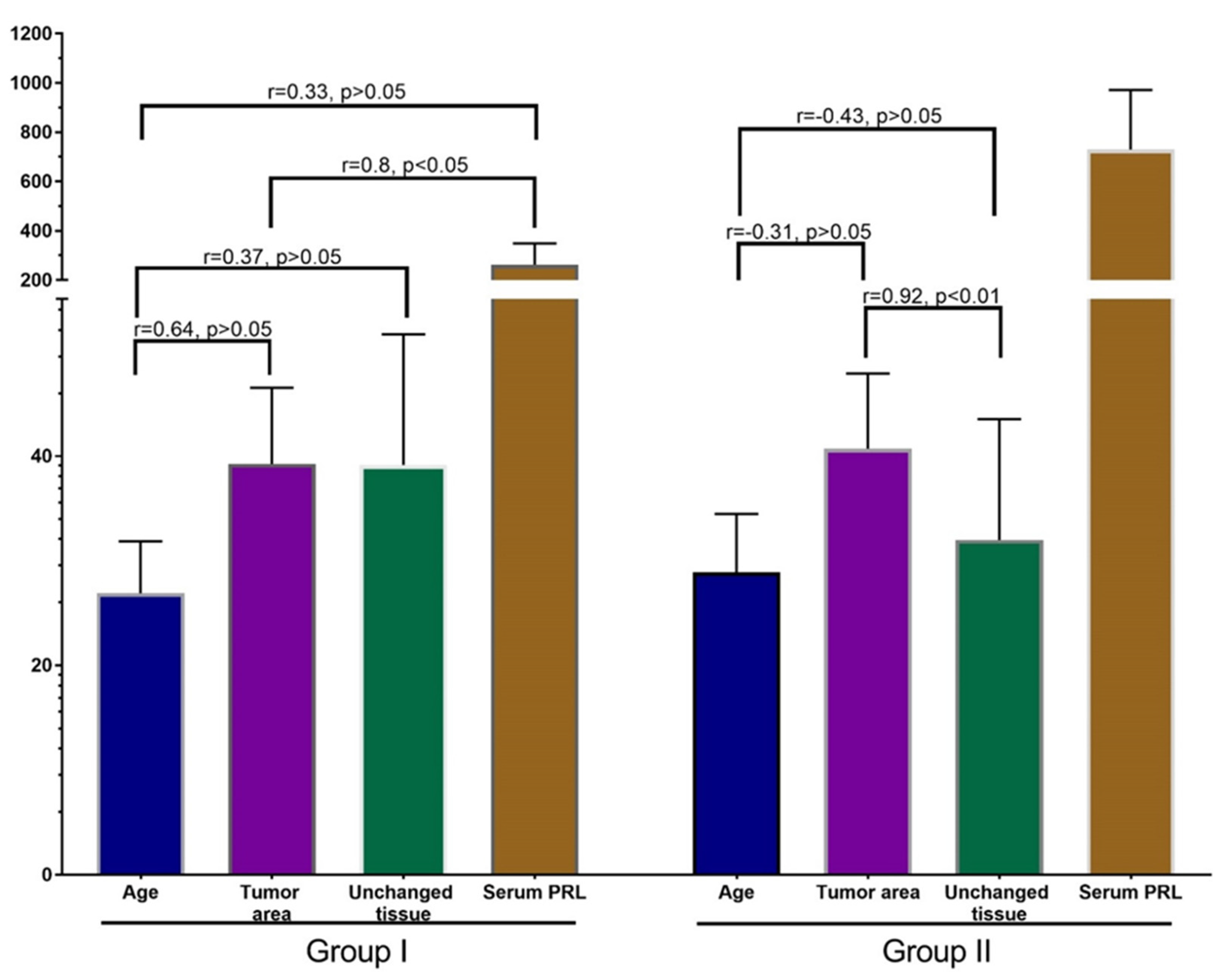
3.3. Statistical Analysis
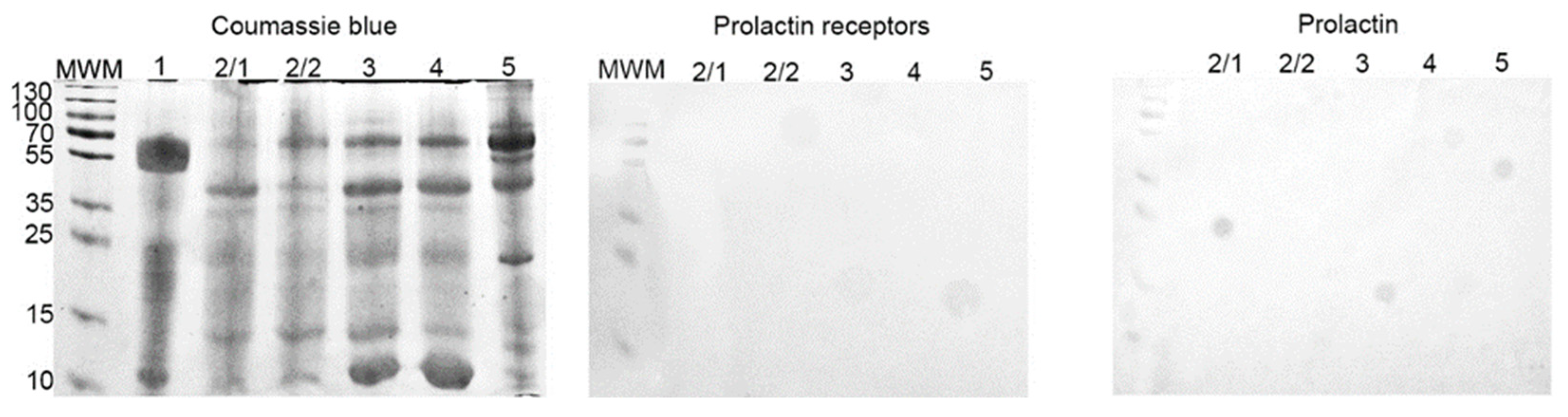
3.4. SDS-PAGE and Western-Blot
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holloran, S.M.; Nosirov, B.; Walter, K.R.; Trinca, G.M.; Lai, Z.; Jin, V.X.; Hagan, C.R. Reciprocal fine-tuning of progesterone and prolactin-regulated gene expression in breast cancer cells. Mol. Cell. Endocrinol. 2020, 511, 110859. [Google Scholar] [CrossRef]
- Zhao, D.; Ma, G.; Zhang, X.; He, Y.; Li, M.; Han, X.; Fu, L.; Dong, X.-Y.; Nagy, T.; Zhao, Q.; et al. Zinc Finger Homeodomain Factor Zfhx3 Is Essential for Mammary Lactogenic Differentiation by Maintaining Prolactin Signaling Activity. J. Biol. Chem. 2016, 291, 12809–12820. [Google Scholar] [CrossRef]
- Atıcı, Ö.K.; Govindrajan, N.; Lopetegui-González, I.; Shemanko, C.S. Prolactin: A hormone with diverse functions from mammary gland development to cancer metastasis. Semin Cell Dev. Biol. 2021, 114, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Aksamitiene, E.; Achanta, S.; Kolch, W.; Kholodenko, B.N.; Hoek, J.B.; Kiyatkin, A. Prolactin-Stimulated Activation of ERK1/2 Mitogen-Activated Protein Kinases is Controlled by PI3-Kinase/Rac/PAK Signaling Pathway in Breast Cancer Cells. Cell Signal 2011, 23, 1794–1805. [Google Scholar] [CrossRef]
- Grible, J.M.; Zot, P.; Olex, A.L.; Hedrick, S.E.; Harrell, J.C.; Woock, A.E.; Idowu, M.O.; Clevenger, C.V. The human intermediate prolactin receptor is a mammary proto-oncogene. NPJ Breast Cancer 2021, 7, 37. [Google Scholar] [CrossRef]
- Pałubska, S.; Adamiak-Godlewska, A.; Winkler, I.; Romanek-Piva, K.; Rechberger, T.; Gogacz, M. Hyperprolactinaemia—A problem in patients from the reproductive period to the menopause. Menopausal Rev. 2017, 16, 1–7. [Google Scholar] [CrossRef]
- Newey, P.J.; Gorvin, C.; Cleland, S.J.; Willberg, C.; Bridge, M.; Azharuddin, M.; Drummond, R.S.; Van Der Merwe, P.A.; Klenerman, P.; Bountra, C.; et al. Mutant Prolactin Receptor and Familial Hyperprolactinemia. N. Engl. J. Med. 2013, 369, 2012–2020. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.A.; Medler, T.R.; Feeney, Y.B.; Wetz, S.M.; Tommerdahl, K.L.; Clevenger, C.V. The Prolactin Receptor Transactivation Domain Is Associated with Steroid Hormone Receptor Expression and Malignant Progression of Breast Cancer. Am. J. Pathol. 2013, 182, 217–233. [Google Scholar] [CrossRef]
- Sutherland, A.; Forsyth, A.; Cong, Y.; Grant, L.; Juan, T.H.; Lee, J.K.; Klimowicz, A.; Petrillo, S.K.; Hu, J.; Chan, A.; et al. The Role of Prolactin in Bone Metastasis and Breast Cancer Cell–Mediated Osteoclast Differentiation. Natl. Cancer Inst. 2016, 108, 338. [Google Scholar] [CrossRef]
- Howell, S.J.; Anderson, E.; Hunter, T.; Farnie, G.; Clarke, R.B. Prolactin receptor antagonism reduces the clonogenic capacity of breast cancer cells and potentiates doxorubicin and paclitaxel cytotoxicity. Breast Cancer Res. 2008, 10, R68. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Peston, D.; Vonderhaar, B.K.; Shousha, S. Expression of prolactin receptors in normal, benign, and malignant breast tissue: An immunohistological study. J. Clin. Pathol. 2001, 54, 956–960. [Google Scholar] [CrossRef]
- Nicol, M.; Willis, C.; Yiangou, C.; Sinnett, D.; Shousha, S. Relationship Between Serum Prolactin Levels and Histology of Benign and Malignant Breast Lesions: A Detailed Study of 153 Consecutive Cases. Breast J. 2002, 8, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Manhès, C.; Kayser, C.; Bertheau, P.; Kelder, B.; Kopchick, J.J.; Kelly, P.A.; Touraine, P.; Goffin, V. Local over-expression of prolactin in differentiating mouse mammary gland induces functional defects and benign lesions, but no carcinoma. J. Endocrinol. 2006, 190, 271–285. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, K.A.; Rugowski, D.E.; Shea, M.P.; Sullivan, R.; Moser, A.R.; Schuler, L.A. Prolactin synergizes with canonical Wnt signals to drive development of ER+ mammary tumors via activation of the Notch pathway. Cancer Lett. 2021, 503, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Hachim, I.Y.; López-Ozuna, V.M.; Hachim, M.Y.; Lebrun, J.-J.; Ali, S. Prolactin hormone exerts anti-tumorigenic effects in HER-2 overexpressing breast cancer cells through regulation of stemness. Stem Cell Res. 2019, 40, 101538. [Google Scholar] [CrossRef] [PubMed]
- Hyznyak, O.; Mykytiuk, M.; Gogitidze, T. Age norms of the serum prolactin level in blood of healthy volunteers. Probl. Endocr. Pathol. 2015, 2, 76–84. [Google Scholar]
- Romaniuk, A.; Lyndin, M.; Moskalenko, R.; Kuzenko, Y.; Gladchenko, O.; Lyndina, Y. Pathogenetic mechanisms of heavy metals eff ect on proapoptotic and proliferative potential of breast cancer. Interv. Med. Appl. Sci. 2015, 7, 63–68. [Google Scholar] [CrossRef][Green Version]
- López-Ozuna, V.M.; Hachim, I.Y.; Hachim, M.; Lebrun, J.-J.; Ali, S. Prolactin modulates TNBC aggressive phenotype limiting tumorigenesis. Endocr. Relat. Cancer 2019, 26, 321–337. [Google Scholar] [CrossRef]
- Shams, A.; Binothman, N.; Boudreault, J.; Wang, N.; Shams, F.; Hamam, D.; Tian, J.; Moamer, A.; Dai, M.; Lebrun, J.-J.; et al. Prolactin receptor-driven combined luminal and epithelial differentiation in breast cancer restricts plasticity, stemness, tumorigenesis and metastasis. Oncogenesis 2021, 10, 10. [Google Scholar] [CrossRef]
- Kavarthapu, R.; Dufau, M.L. Essential role of endogenous prolactin and CDK7 in estrogen-induced upregulation of the prolactin receptor in breast cancer cells. Oncotarget 2017, 8, 27353–27363. [Google Scholar] [CrossRef][Green Version]
- Hachim, I.Y.; Hachim, M.Y.; Lopez, V.M.; Lebrun, J.-J.; Ali, S. Prolactin Receptor Expression is an Independent Favorable Prognostic Marker in Human Breast Cancer. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Chakhtoura, Z.; Laki, F.; Bernadet, M.; Cherifi, I.; Chiche, A.; Pigat, N.; Bernichtein, S.; Courtillot, C.; Boutillon, F.; Bièche, I.; et al. Gain-of-function Prolactin Receptor Variants Are Not Associated With Breast Cancer and Multiple Fibroadenoma Risk. Clin. Endocrinol. Metab. 2016, 101, 4449–4460. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y. The many faces of prolactin in breast cancer. Adv. Exp. Med. Biol. 2015, 846, 61–81. [Google Scholar] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolomiiets, O.; Yazykov, O.; Piddubnyi, A.; Lyndin, M.; Lukavenko, I.; Andryushchenko, V.; Romaniuk, A.; Moskalenko, R. The Expression of Prolactin Receptors in Benign Breast Tumors Is Not Associated with Serum Prolactin Level. J. Clin. Med. 2021, 10, 5866. https://doi.org/10.3390/jcm10245866
Kolomiiets O, Yazykov O, Piddubnyi A, Lyndin M, Lukavenko I, Andryushchenko V, Romaniuk A, Moskalenko R. The Expression of Prolactin Receptors in Benign Breast Tumors Is Not Associated with Serum Prolactin Level. Journal of Clinical Medicine. 2021; 10(24):5866. https://doi.org/10.3390/jcm10245866
Chicago/Turabian StyleKolomiiets, Olena, Oleksandr Yazykov, Artem Piddubnyi, Mykola Lyndin, Ivan Lukavenko, Volodymyr Andryushchenko, Anatolii Romaniuk, and Roman Moskalenko. 2021. "The Expression of Prolactin Receptors in Benign Breast Tumors Is Not Associated with Serum Prolactin Level" Journal of Clinical Medicine 10, no. 24: 5866. https://doi.org/10.3390/jcm10245866
APA StyleKolomiiets, O., Yazykov, O., Piddubnyi, A., Lyndin, M., Lukavenko, I., Andryushchenko, V., Romaniuk, A., & Moskalenko, R. (2021). The Expression of Prolactin Receptors in Benign Breast Tumors Is Not Associated with Serum Prolactin Level. Journal of Clinical Medicine, 10(24), 5866. https://doi.org/10.3390/jcm10245866