
Anxiolytic and Antidepressant Use and Burnout: Optimism as a Mediator in Spanish Nurses

 ,
,  ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
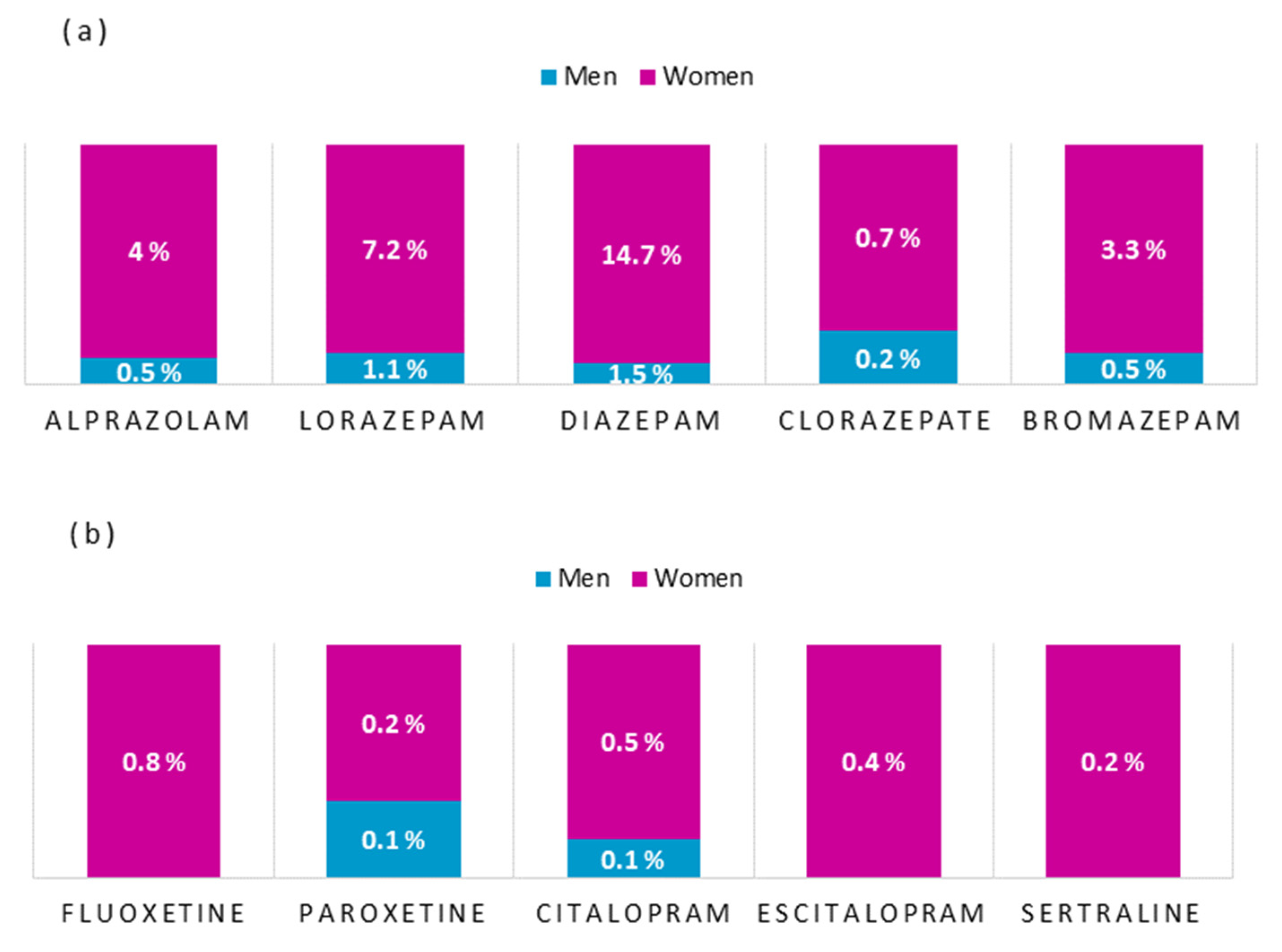
3.1. Drug Use, Burnout and Optimism
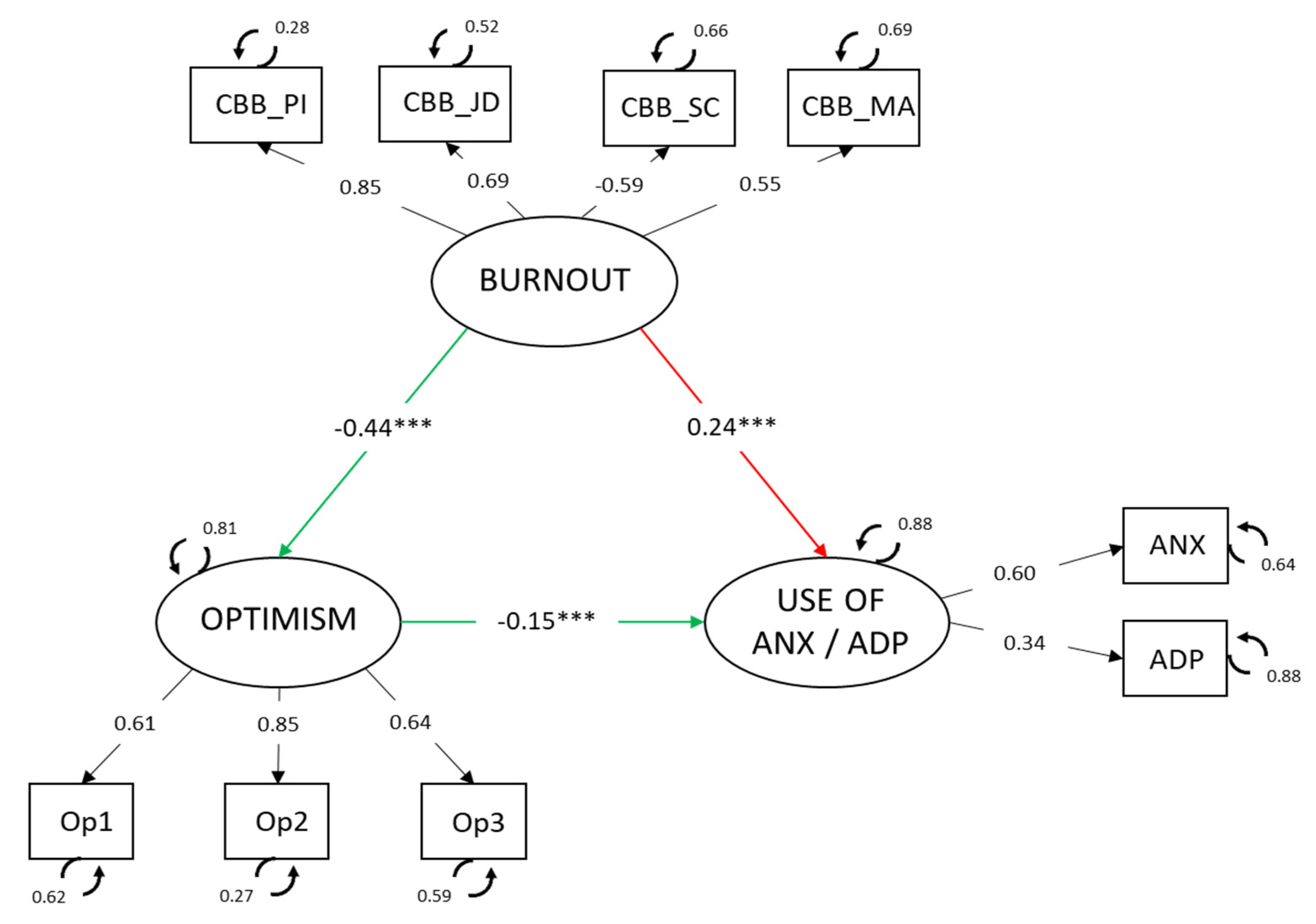
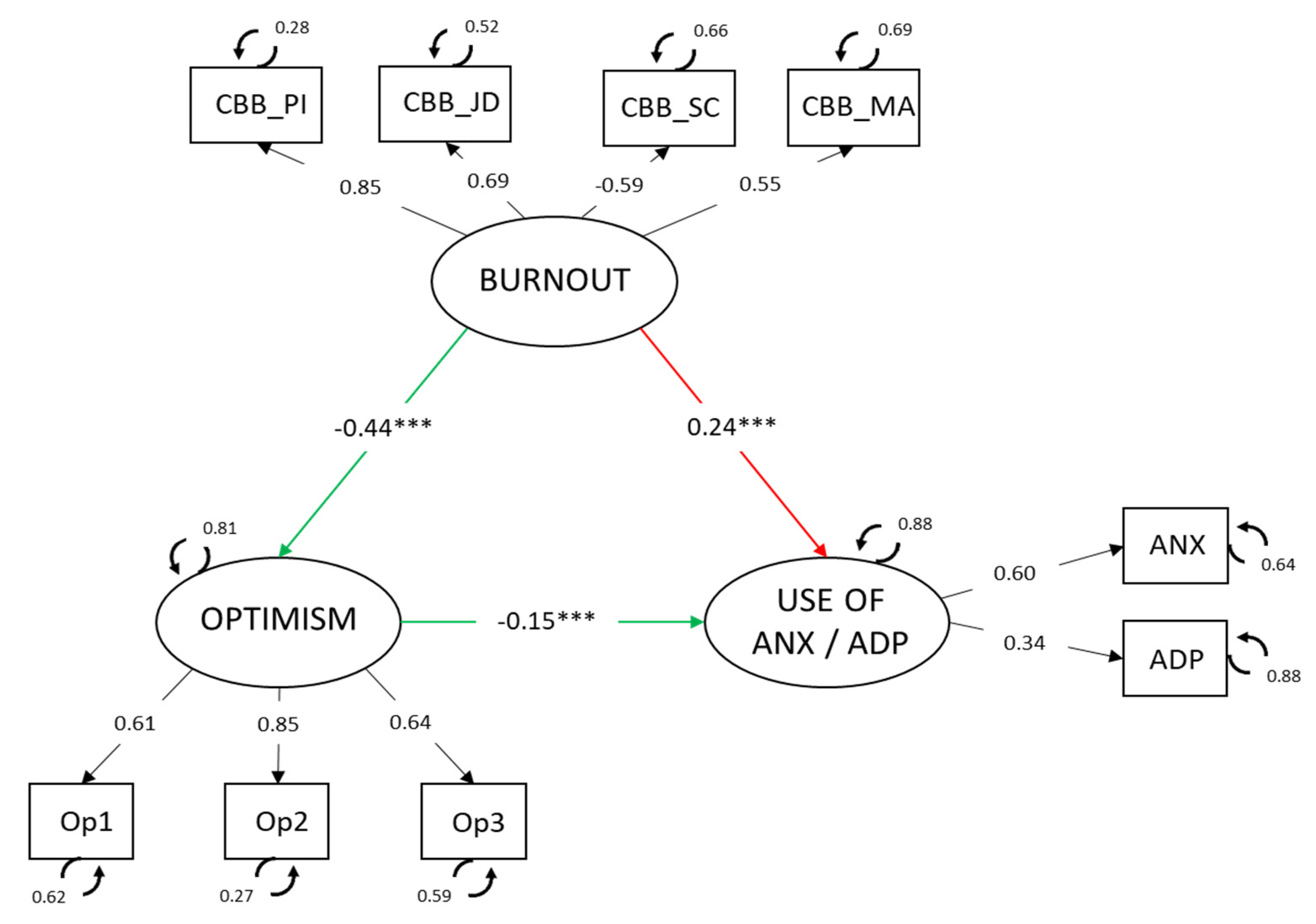
3.2. Involvement of Optimism in the Relationship between Burnout and Use of Anxiolytics and Antidepressants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). ICD-11 International Classification of Diseases-Mortality and Morbidity Statistics; 11th Revision; OMS, 2018; Available online: https://icd.who.int/browse11/l-m/en (accessed on 2 November 2021).
- Maslach, C.; Leiter, M.P. Burnout. In Encyclopedia of Mental Health; Friedman, H.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 222–227. [Google Scholar] [CrossRef]
- Zhao, X.; Ding, S. Phenomenology of Burnout Syndrome and Connection Thereof with Coping Strategies and Defense Mechanisms among University Professors. Eur. J. Investig. Health. Psychol. Educ. 2020, 10, 82–93. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, B.; Maharaj, S.; Simpson, A.; Nassif, N.; Lal, S. The Metabolic Role of Depression and Burnout in Nurses. Transl. Metac. Syndrom Res. 2020, 3, 9–11. [Google Scholar] [CrossRef]
- Stelnicki, A.M.; Jamshidi, L.; Angehrn, A.; Hadjistavropoulos, H.D.; Carleton, R.N. Associations between Burnout and Mental Disorder Symptoms Among Nurses in Canada. Can. J. Nurs. Res. 2021, 53, 254–263. [Google Scholar] [CrossRef]
- Woo, T.; Ho, R.; Tang, A.; Tam, W. Global Prevalence of Burnout Symptoms Among Nurses: A Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2020, 123, 9–20. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Martos, Á.; Gázquez, J.J. New Burnout Evaluation Model Based on the Brief Burnout Questionnaire: Psychometric Properties for Nursing. Int. J. Environ. Res. Public Health 2018, 15, 2718. [Google Scholar] [CrossRef] [Green Version]
- Kelly, L.A.; Gee, P.M.; Butler, R.J. Impact of Nurse Burnout on Organizational and Position Turnover. Nurs. Outlook 2021, 69, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Bakhamis, L.; Paul, D.; Smith, H.; Coustasse, A. Still an Epidemic. The Burnout Syndrome in Hospital Registered Nurses. Health Care Manag. 2019, 38, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Jaworek, M.; Marek, T.; Karwowski, W.; Andrzajczak, C.; Fenaidy, A.M. Burnout Syndrome as a Mediator for the Effect of Work-Related Factors on Musculoskeletal Complaints among Hospital Nurses. Int. J. Ind. Ergon. 2010, 40, 368–375. [Google Scholar] [CrossRef]
- Saavedra, F.J.; Murvartian, L.; Vallecillo, N. Health and Burnout of Home Health Care Assistants: Impact of a Training Intervention. Ann. Psicol. 2020, 36, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Granados, L.; Aparisi, D.; Inglés, C.J.; Aparicio López, M.D.; Fernández Sogorb, A.; García Fernández, J.M. Do the Depression, Anxiety and Stress Factors Predict the Dimension of Depersonalization and Low Personal Accomplishment in Professorate? Eur. J. Dev. Edu. Psychop. 2019, 7, 83–92. [Google Scholar] [CrossRef]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The Relationship between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 284. [Google Scholar] [CrossRef] [Green Version]
- Soriano, J.G.; Pérez-Fuentes, M.C.; Molero, M.M.; Tortosa, B.M.; González, A. Benefits of Psychological Intervention Related to Stress and Anxiety: Systematic Review and Meta-Analysis. Eur. J. Educ. Psychol. 2019, 12, 191–206. [Google Scholar] [CrossRef]
- Rudman, A.; Arborelius, L.; Dahlgren, A.; Finnes, A.; Gustavsson, P. Consequences of Early Career Nurse Burnout: A Prospective Long-Term Follow-Up on Cognitive Functions, Depressive Symptoms, and Insomnia. EClinicalMedicine 2020, 27, 100565. [Google Scholar] [CrossRef]
- Sang, E.; Liao, Y.M.; Miao, N.F.; Chou, K.R.; Chung, M.H. Patterns and Correlates of Benzodiazepine Use in Nurses: A Nationwide, Population-Based Study. Int. J. Ment. Health Nurs. 2018, 27, 400–407. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M. Analysis of Burnout Predictors in Nursing: Risk and Protective Psychological Factors. Eur. J. Psychol. Appl. Leg. Context 2019, 11, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Bamonti, P.; Conti, E.; Cavanagh, C.; Gerolimatos, L.; Gregg, J.; Goulet, C.; Pifer, M.; Edelstein, B. Coping, Cognitive Emotion Regulation, and Burnout in Long-Term Care Nursing Staff: A Preliminary Study. J. Appl. Gerontol. 2017, 38, 92–111. [Google Scholar] [CrossRef]
- Cooper, C.; Katona, C.; Orrell, M.; Livingston, G. Coping Strategies and Anxiety in Caregivers of People with Alzheimer’s Disease: The LASER-AD Study. J. Affect. Disord. 2006, 9, 15–20. [Google Scholar] [CrossRef]
- Limiña-Gras, R.M.; Sánchez-López, P.; Saavedra-San Román, A.I.; Corbalán-Bernal, F.J. Health and Gender in Female-Dominated Occupations: The Case of Male Nurses. J. Mens. Stud. 2013, 21, 135–148. [Google Scholar] [CrossRef]
- Madsen, I.E.H.; Lange, T.; Borritz, M.; Rugulies, R. Burnout as a Risk Factor for Antidepressant Treatment—A Repeated Measures Time-to-Event Analysis of 2936 Danish Human Service Workers. J. Psychiatr. Res. 2015, 65, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.L.C.; Wu, M.P.; Ho, C.H.; Wang, J.J. Risks of Treated Anxiety, Depression, and Insomnia among Nurses: A Nationwide Longitudinal Cohort Study. PLoS ONE 2018, 13, e0204224. [Google Scholar] [CrossRef] [Green Version]
- Souto-Gestal, A.; Cabanach, R.G.; Franco, V. Depressive Symptomatology and Perception of Academic Stressors in Physiotherapy Students. Eur. J. Educ. Psychol. 2019, 12, 165–174. [Google Scholar] [CrossRef]
- Cares, A.; Pace, E.; Denious, J.; Crane, L.A. Substance Use and Mental Illness among Nurses: Workplace Warning Signs and Barriers to Seeking Assistance. Subst. Abus. 2015, 36, 59–66. [Google Scholar] [CrossRef]
- Marques, M.M.; Alves, E.; Queirós, C.; Norton, P.; Henriques, A. The Effect of Profession on Burnout in Hospital Staff. Occup. Med. 2018, 68, 207–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saridi, M.; Kordosi, A.; Toska, A.; Peppou, L.E.; Economou, M.; Souliotis, K. Attitudes of Health Professionals towards the Stigma Surrounding Depression in Times of Economic Crisis. Int. J. Soc. Psychiatry 2017, 63, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Subdirección General de Información Sanitaria. Salud Mental en Datos: Prevalencia de los Problemas de Salud y Consumo de Psicofármacos y Fármacos Relacionados a Partir de los Registros Clínicos de Atención Primaria. Ministerio de Sanidad. 2020. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/Salud_mental_datos.pdf (accessed on 2 November 2021).
- Rothe, N.; Steffen, J.; Penz, M.; Kirschbaum, C.; Walther, A. Examination of Peripheral Basal and Reactive Cortisol Levels in Major Depressive Disorder and the Burnout Syndrome: A Systematic Review. Neurosci. Biobehav. Rev. 2020, 114, 232–270. [Google Scholar] [CrossRef] [PubMed]
- Travella, G.; Parker, G. Distinguishing Burnout from Depression: An Exploratory Qualitative Study. Psychiatry Res. 2020, 291, 113212. [Google Scholar] [CrossRef]
- Barragán, A.B.; Molero, M.M.; Pérez-Fuentes, M.C.; Simón Márquez, M.D.M.; Sisto, M.; Gázquez Linares, J.J. Published Research on Burnout in Nursing in Spain in the Last Decade: Bibliometric Analysis. Healthcare 2020, 8, 478. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Martos, Á.; Gázquez, J.J. Burnout and Engagement: Personality Profiles in Nursing Professionals. J. Clin. Med. 2019, 8, 286. [Google Scholar] [CrossRef] [Green Version]
- Santirso, F.A.; Lila, M.; Gracia, E. Motivational Strategies, Working Alliance, and Protherapeutic Behaviors in Batterer Intervention Programs: A Randomized Controlled Trial. Eur. J. Psychol. Appl. Leg. Context 2020, 12, 77–84. [Google Scholar] [CrossRef]
- Rees, C.S.; Eley, R.; Osseiran-Moisson, K.F.; Francis, K.; Cusack, L.; Heritage, B.; Hegney, D. Individual and Environmental Determinants of Burnout among Nurses. J. Health Serv. Res. Policy 2019, 24, 191–200. [Google Scholar] [CrossRef]
- Stefanova, E.; Dubljevic, O.; Herbert, C.; Fairfield, B.; Schroeter, M.L.; Stern, E.R.; Urben, S.; Derntl, B.; Wiebking, C.; Brown, C.; et al. Anticipatory Feelings: Neural Correlates and Linguistic Markers. Neurosci. Biobehav. Rev. 2020, 113, 308–324. [Google Scholar] [CrossRef]
- Luthans, F.; Youssef, C.M. Human, Social, and Now Positive Psychological Capital Management. Organ. Dyn. 2004, 33, 143–160. [Google Scholar] [CrossRef]
- McAllister, M.; McKinnon, J. The Importance of Teaching and Learning Resilience in the Health Disciplines: A Critical Review of the Literature. Nurse Educ. Today 2009, 29, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Terry, D.; Peck, B.; Smith, A.; Nguyen, H. Occupational Self-Efficacy and Psychological Capital Amongst Nursing Students: A Cross Sectional Study Understanding the Malleable Attributes for Success. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menéndez-Aller, Á.; Postigo, Á.; Montes-Álvarez, P.; González-Primo, F.J.; García-Cueto, E. Humor as a Protective Factor against Anxiety and Depression. Int. J. Clin. Health Psychol. 2020, 20, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ercolani, G.; Varani, S.; Peghetti, B.; Franchini, L.; Malerba, M.B.; Messana, R.; Sichi, V.; Pannuti, R.; Pannuti, F. Burnout in Home Palliative Care: What Is the Role of Coping Strategies? J. Palliat. Care 2020, 35, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Kubzansky, L.D.; Kubzansky, P.E.; Maselko, J. Optimism and Pessimism in the Context of Health: Bipolar Opposites or Separate Constructs? Pers. Soc. Psychol. Bull. 2004, 30, 943–956. [Google Scholar] [CrossRef] [PubMed]
- Serrano, C.; Andreu, Y.; Murgui, S. The Big Five and Subjective Wellbeing: The Mediating Role of Optimism. Psicothema 2020, 32, 352–358. [Google Scholar] [CrossRef]
- Hirata, M.; Villar, M.A.; Mendoça, C.; Trevisan, J.; Gonçalvez, A. Psychological Concept of Optimism and Drug Use among Nursing Students. Acta Paul. Enferm. 2011, 24, 393–399. [Google Scholar] [CrossRef]
- Romswinkel, E.V.; Konig, H.H.; Hajek, A. The Role of Optimism in the Relationship between Job Stress and Depressive Symptoms. Longitudinal Findings from the German Ageing Survey. J. Affect. Disord. 2018, 241, 249–255. [Google Scholar] [CrossRef]
- Yaldiz, L.M.; Truxillo, D.M.; Cadiz, D.M. Who Benefits More? The Moderating Role of Age on the Relationship between Work and Person Characteristics and Employee Attitudes and Wellbeing. Occup. Med. 2020, 4, 139–160. [Google Scholar] [CrossRef]
- Zborowska, A.; Gurowiec, P.J.; Mlynarska, A.; Uchmanowicz, I. Factors Affecting Occupational Burnout among Nurses Including Job Satisfaction, Life Satisfaction, and Life Orientation: A Cross-Sectional Study. Psychol. Res. Behav. Manag. 2021, 14, 1761–1777. [Google Scholar] [CrossRef]
- Malagón-Aguilera, M.C.; Suner-Soler, R.; Bonmati-Tomas, A.; Bosch-Ferre, C.; Gelabert-Viella, S.; Fontova-Almato, A.; Grau-Martín, A.; Juvinya-Canal, D. Dispositional Optimism, Burnout and Their Relationship with Self-Reported Health Status among Nurses Working in Long-Term Healthcare Centers. Int. J. Environ. Res. Public Health 2020, 17, 4918. [Google Scholar] [CrossRef]
- Molero, M.M.; Pérez-Fuentes, M.C.; Gázquez, J.J. Analysis of the Mediating Role of Self-Efficacy and Self-Esteem on the Effect of Workload on Burnout’s Influence on Nurses’ Plans to Work Longer. Front. Psychol. 2020, 9, 2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.S.; Han, J.W.; Kim, Y.H. Effect of Nurses’ Emotional Labor on Customer Orientation and Service Delivery: The Mediating Effects of Work Engagement and Burnout. Saf. Health Work 2018, 9, 441–446. [Google Scholar] [CrossRef]
- Macaya, M.C.; Lanciego, Y.; Pacheco, I. Nurse Intervention for the Study of the Health Perceived by Caregivers: Workshops Aimed at Training the Caregiver. Eur. J. Health Res. 2020, 6, 145–156. [Google Scholar] [CrossRef]
- Abram, M.D.; Jacobowitz, W. Resilience and Burnout in Healthcare Students and Inpatient Psychiatric Nurses: A Between-Groups Study of Two Populations. Arch. Psychiatr. Nurs. 2021, 35, 1–8. [Google Scholar] [CrossRef]
- Brailovskaia, J.; Margraf, J. Predicting Adaptive and Maladaptive Responses to the Coronavirus (COVID-19) Outbreak: A Prospective Longitudinal Study. Int. J. Clin. Health Psychol. 2020, 20, 183–191. [Google Scholar] [CrossRef] [PubMed]
- da Silva, C.J.; da Conceição Silva, R.M.; de Souza, F.R.; dos Santos Lopes, S.S.; da Silva, T.M.; Silva, R.P. Prevalence in the Use of Anxiolytics among Nursing Professionals: An Integrative Review. Int. J. Psychol. Res. Rev. 2020, 3, 34. [Google Scholar]
- Otero, J.M.; Luengo, A.; Romero, E.; Gómez, J.A.; Castro, C. Psicología de la Personalidad. Manual de Prácticas; Ariel Practicum: Barcelona, Spain, 1998. [Google Scholar]
- Scheier, M.F.; Carver, C.; Bridges, M.W. Distinguishing Optimism from Neuroticism (and Trait Anxiety, Self-Mastery, and Self-Esteem): A Reevaluation of the Life Orientation Test. J. Pers. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef]
- Ferrando, P.J.; Chico, E.; Tous, J.M. Propiedades Psicométricas del Test de Optimismo Life Orientation Test [Psychometric Properties of Optimism Test Life Orientation Test]. Psicothema 2002, 14, 673–680. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp. Released; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Ventura-León, J.L.; Caycho, T. El Coeficiente Omega: Un Método Alternativo para la Estimación de la Confiabilidad [The Omega Coefficient: An Alternative Method for Estimating Reliability]. Rev. Latinoam. Cienc. Soc. Niñez Juv. 2017, 15, 625–627. [Google Scholar]
- McDonald, R.P. Test Theory: A Unified Approach; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1999. [Google Scholar]
- Welch, B.L. The Generalization of “Student’s” Problem When Several Different Population Variances are Involved. Biometrika 1947, 34, 28–35. [Google Scholar] [CrossRef]
- Derrick, B.; Toher, D.; White, P. Why Welch’s Test is Type I Error Robust. Quant. Meth. Psych. 2016, 12, 30–38. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling and More. Version 0.5–12 (BETA). J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- JASP Team. JASP; Version 0.14; Computer Software; JASP Team: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Method. 2008, 6, 53–60. [Google Scholar]
- Iacobucci, D. Structural Equations Modeling: Fit Indices, Sample Size, and Advanced Topics. J. Consum. Psychol. 2010, 20, 90–98. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford: New York, NY, USA, 2005. [Google Scholar]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Personal Impact | Job Dissatisfaction | Social Climate | Motivational Abandonment | Optimism | ||
|---|---|---|---|---|---|---|
| Anxiolytics | Pearson’s r | 0.190 *** | 0.103 *** | −0.102 *** | 0.094 *** | −0.138 *** |
| 95% CI Upper | 0.239 | 0.154 | −0.051 | 0.145 | −0.086 | |
| 95% CI Lower | 0.139 | 0.052 | −0.153 | 0.042 | −0.188 | |
| Antidepressant | Pearson’s r | 0.110 *** | 0.067 * | −0.074 ** | 0.084 ** | −0.078 ** |
| 95% CI Upper | 0.161 | 0.118 | −0.022 | 0.135 | −0.026 | |
| 95% CI Lower | 0.058 | 0.015 | −0.125 | 0.032 | −0.129 | |
| M (SD) | 7.47 (2.50) | 8.43 (2.63) | 12.2 (1.80) | 9.12 (2.44) | 8.25 (2.10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martos Martínez, Á.; Barragán Martín, A.B.; Gázquez Linares, J.J.; Molero Jurado, M.d.M.; Simón Márquez, M.d.M.; Pérez-Fuentes, M.d.C. Anxiolytic and Antidepressant Use and Burnout: Optimism as a Mediator in Spanish Nurses. J. Clin. Med. 2021, 10, 5741. https://doi.org/10.3390/jcm10245741
Martos Martínez Á, Barragán Martín AB, Gázquez Linares JJ, Molero Jurado MdM, Simón Márquez MdM, Pérez-Fuentes MdC. Anxiolytic and Antidepressant Use and Burnout: Optimism as a Mediator in Spanish Nurses. Journal of Clinical Medicine. 2021; 10(24):5741. https://doi.org/10.3390/jcm10245741
Chicago/Turabian StyleMartos Martínez, África, Ana Belén Barragán Martín, José Jesús Gázquez Linares, María del Mar Molero Jurado, María del Mar Simón Márquez, and María del Carmen Pérez-Fuentes. 2021. "Anxiolytic and Antidepressant Use and Burnout: Optimism as a Mediator in Spanish Nurses" Journal of Clinical Medicine 10, no. 24: 5741. https://doi.org/10.3390/jcm10245741
APA StyleMartos Martínez, Á., Barragán Martín, A. B., Gázquez Linares, J. J., Molero Jurado, M. d. M., Simón Márquez, M. d. M., & Pérez-Fuentes, M. d. C. (2021). Anxiolytic and Antidepressant Use and Burnout: Optimism as a Mediator in Spanish Nurses. Journal of Clinical Medicine, 10(24), 5741. https://doi.org/10.3390/jcm10245741