
Patient Safety in a Box: Implementation and Evaluation of the Emergency Box in Geriatric and Parkinson Patients



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethic Approval and Patient Recruitment
2.2. Assessment
2.2.1. ER Survey (n = 102)
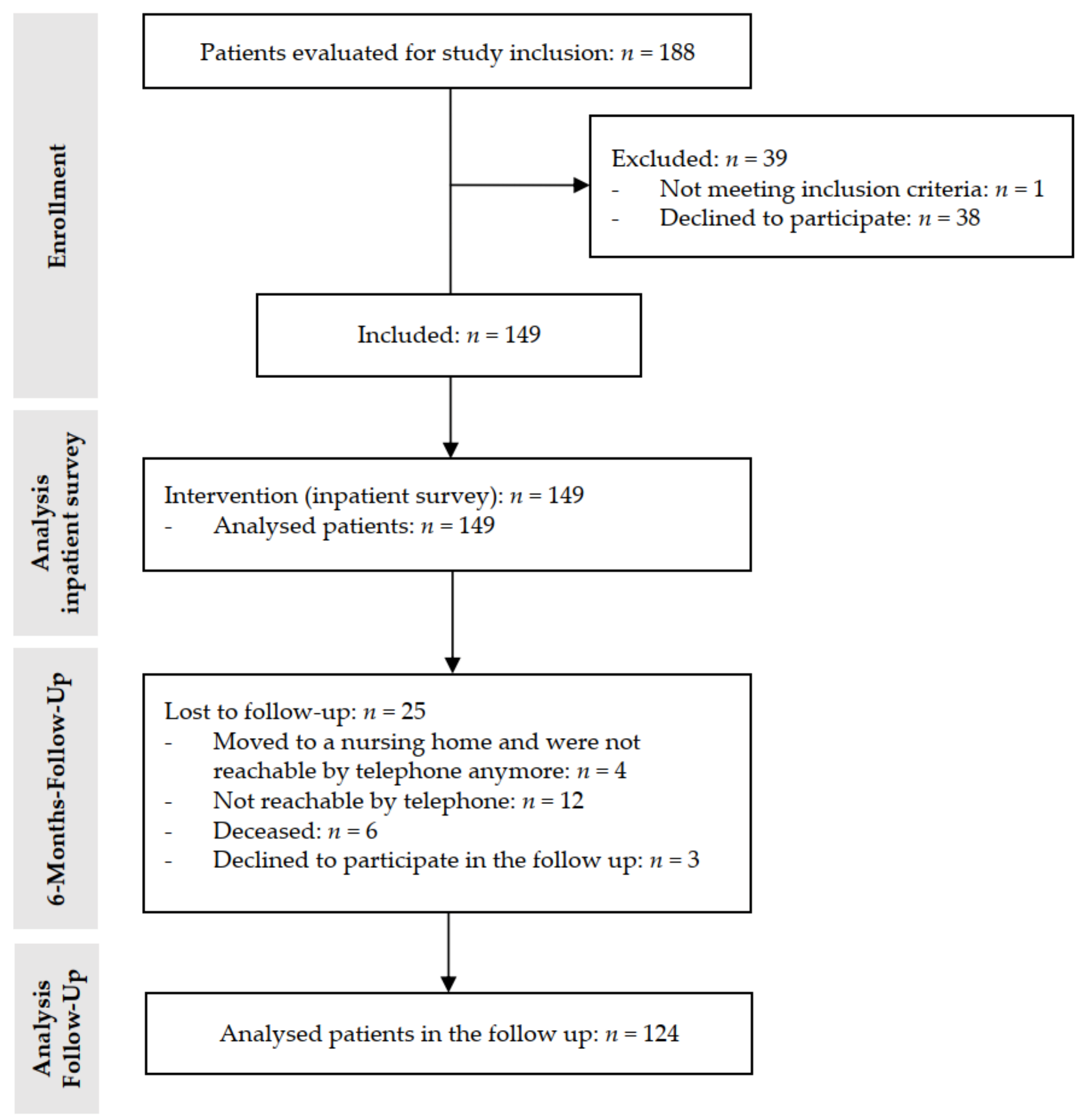
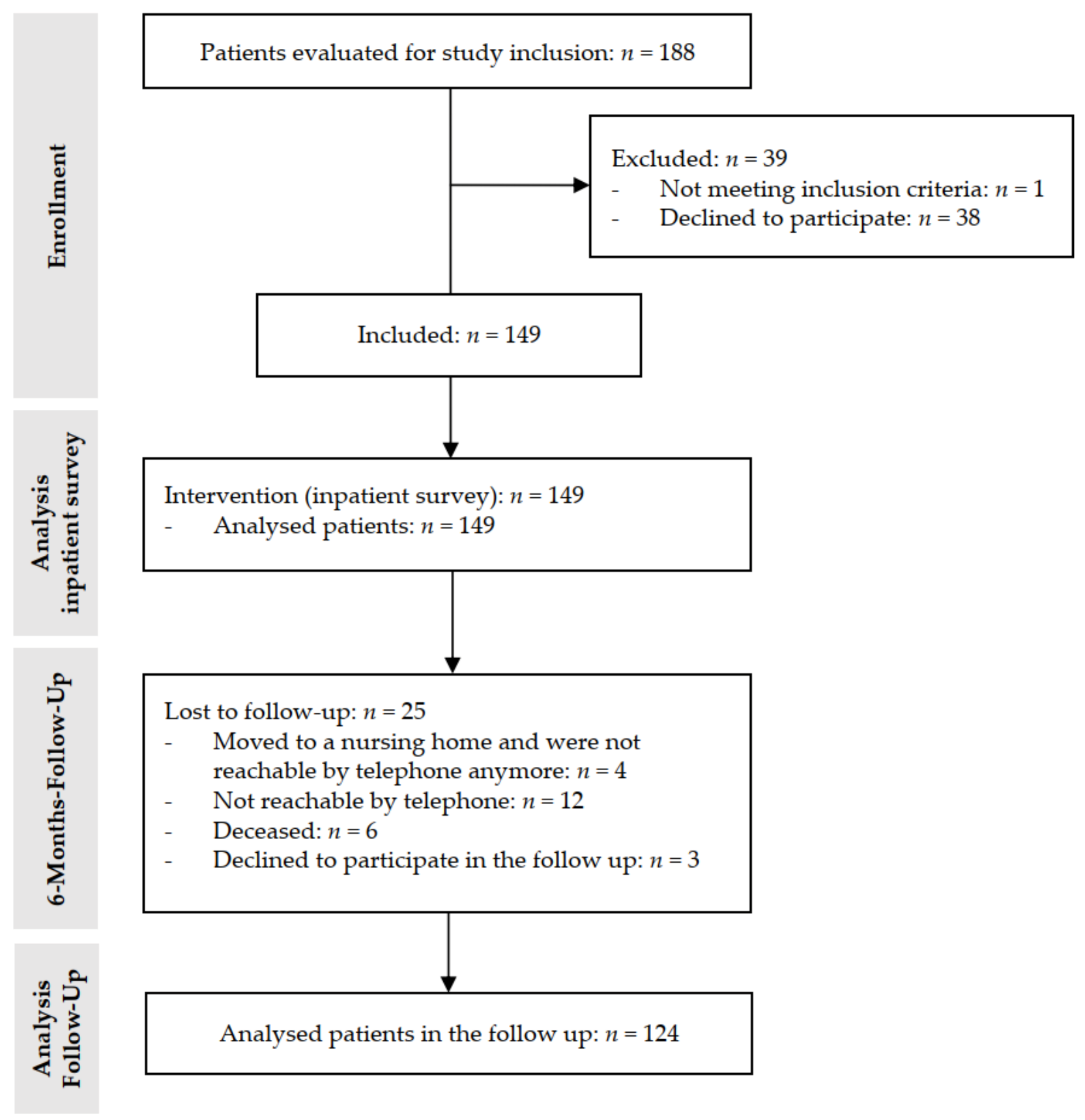
2.2.2. Inpatient Survey (n = 149)
2.2.3. Follow-Up after 6 Months (n = 124)
2.3. Emergency Box
2.4. Statistical Analysis
3. Results
3.1. ER Survey (n = 102)
3.2. Inpatient Survey (n = 149)
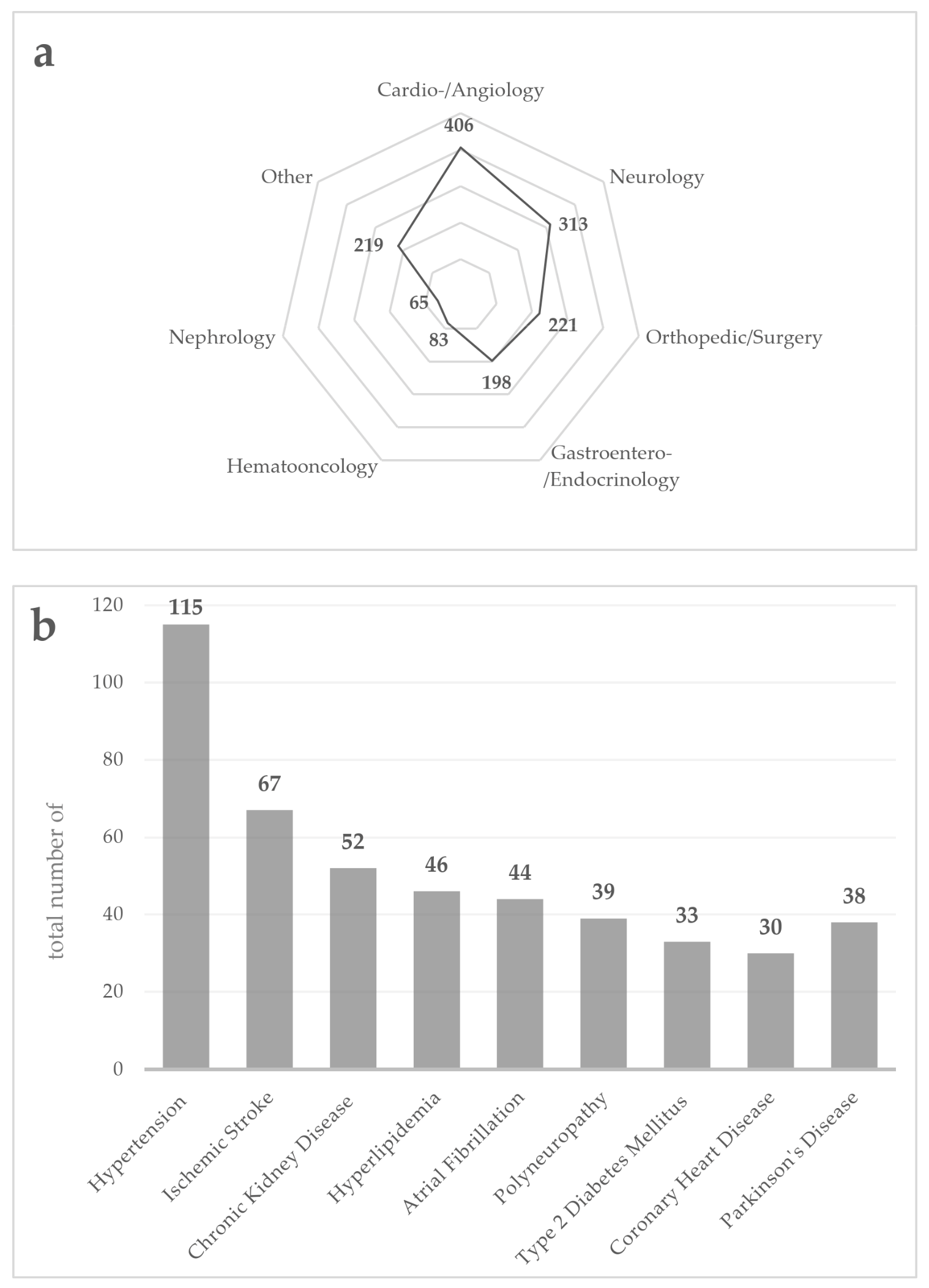
3.2.1. Demographics, Comorbidities, and Medication
3.2.2. Inpatient Assessment
3.3. Follow-Up after 6 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kahn, J.H.; Magauran, B.G., Jr.; Olshaker, J.S.; Shankar, K.N. Current Trends in Geriatric Emergency Medicine. Emerg. Med. Clin. N. Am. 2016, 34, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.G.; McLeod, A.; McCue, P.; Phelps, K.; Bardsley, M.; Roberts, H.C.; Conroy, S.P. New horizons in comprehensive geriatric assessment. Age Ageing 2017, 46, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGilton, K.S.; Vellani, S.; Yeung, L.; Chishtie, J.; Commisso, E.; Ploeg, J.; Andrew, M.K.; Ayala, A.P.; Gray, M.; Morgan, D.; et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: A scoping review. BMC Geriatr. 2018, 18, 231. [Google Scholar] [CrossRef] [PubMed]
- Klietz, M.; Greten, S.; Wegner, F.; Höglinger, G.U. Safety and Tolerability of Pharmacotherapies for Parkinson’s Disease in Geriatric Patients. Drugs Aging 2019, 36, 511–530. [Google Scholar] [CrossRef]
- Tenison, E.; Henderson, E.J. Multimorbidity and Frailty: Tackling Complexity in Parkinson’s Disease. J. Parkinsons Dis. 2020, 10, S85–S91. [Google Scholar] [CrossRef]
- Bray Lions Club. ‘Message in a Bottle’ is an Emergency Information Scheme. Available online: http://www.braylionsclub.ie/message_in_a_bottle.html (accessed on 19 September 2021).
- Cybulski, M.; Cybulski, L.; Krajewska-Kulak, E.; Orzechowska, M.; Cwalina, U. Preferences and attitudes of older adults of Bialystok, Poland toward the use of over-the-counter drugs. Clin. Interv. Aging 2018, 13, 623–632. [Google Scholar] [CrossRef] [Green Version]
- Sieber, C.C. The elderly patient—Who is that? Internist 2007, 48, 1190–1194. [Google Scholar] [CrossRef]
- Freyer, J.; Greißing, C.; Buchal, P.; Kabitz, H.J.; Kasprick, L.; Schuchmann, M.; Sultzer, R.; Schiek, S.; Bertsche, T. Discharge medication—What do patients know about their medication on discharge? Dtsch. Med. Wochenschr. 2016, 141, e150–e156. [Google Scholar] [CrossRef]
- Feldmann, F.; Zipprich, H.M.; Witte, O.W.; Prell, T. Self-Reported Nonadherence Predicts Changes of Medication after Discharge from Hospital in People with Parkinson’s Disease. Parkinsons Dis. 2020, 2020, 4315489. [Google Scholar] [CrossRef]
- Krause, O.; Glaubitz, S.; Hager, K.; Schleef, T.; Wiese, B.; Junius-Walker, U. Post-discharge adjustment of medication in geriatric patients: A prospective cohort study. Z. Gerontol. Geriatr. 2020, 53, 663–670. [Google Scholar] [CrossRef]
- Dormann, H.; Sonst, A.; Müller, F.; Vogler, R.; Patapovas, A.; Pfistermeister, B.; Plank-Kiegele, B.; Kirchner, M.; Hartmann, N.; Bürkle, T.; et al. Adverse drug events in older patients admitted as an emergency: The role of potentially inappropriate medication in elderly people (PRISCUS). Dtsch. Arztebl. Int. 2013, 110, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Greten, S.; Müller-Funogea, J.I.; Wegner, F.; Höglinger, G.U.; Simon, N.; Junius-Walker, U.; Gerbel, S.; Krause, O.; Klietz, M. Drug safety profiles in geriatric patients with Parkinson’s disease using the FORTA (Fit fOR The Aged) classification: Results from a mono-centric retrospective analysis. J. Neural Transm. 2021, 128, 49–60. [Google Scholar] [CrossRef]
- Schyve, P.M. Language differences as a barrier to quality and safety in health care: The Joint Commission perspective. J. Gen. Intern. Med. 2007, 22 (Suppl. S2), 360–361. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.F.; Hussey, P.S. Population aging: A comparison among industrialized countries. Health Aff. 2000, 19, 191–203. [Google Scholar] [CrossRef]
- Roberts, D.C.; McKay, M.P.; Shaffer, A. Increasing rates of emergency department visits for elderly patients in the United States, 1993 to 2003. Ann. Emerg. Med. 2008, 51, 769–774. [Google Scholar] [CrossRef]
- Shah, M.N.; Bazarian, J.J.; Lerner, E.B.; Fairbanks, R.J.; Barker, W.H.; Auinger, P.; Friedman, B. The epidemiology of emergency medical services use by older adults: An analysis of the National Hospital Ambulatory Medical Care Survey. Acad. Emerg. Med. 2007, 14, 441–447. [Google Scholar] [CrossRef]
- Kelly, B.; Blake, C.; Lennon, O. Acute Hospital Admissions of Individuals with a Known Parkinson’s Disease Diagnosis in Ireland 2009–2012: A Short Report. J. Parkinsons Dis. 2016, 6, 709–716. [Google Scholar] [CrossRef]
- Okunoye, O.; Kojima, G.; Marston, L.; Walters, K.; Schrag, A. Factors associated with hospitalisation among people with Parkinson’s disease—A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2020, 71, 66–72. [Google Scholar] [CrossRef]
- Shahgholi, L.; De Jesus, S.; Wu, S.S.; Pei, Q.; Hassan, A.; Armstrong, M.J.; Martinez-Ramirez, D.; Schmidt, P.; Okun, M.S. Hospitalization and rehospitalization in Parkinson disease patients: Data from the National Parkinson Foundation Centers of Excellence. PLoS ONE 2017, 12, e0180425. [Google Scholar] [CrossRef] [Green Version]
- King, L.A.; Priest, K.C.; Nutt, J.; Chen, Y.; Chen, Z.; Melnick, M.; Horak, F. Comorbidity and functional mobility in persons with Parkinson disease. Arch. Phys. Med. Rehabil. 2014, 95, 2152–2157. [Google Scholar] [CrossRef]
- Lee, J.W.; Mah, G.; Kalia, S.; Miyasaki, J. Emergency Room Visit Prevention for Older Patients with Parkinsonism in a Geriatric Clinic. Can. J. Neurol. Sci. 2021, 48, 666–675. [Google Scholar] [CrossRef]
- de Heer, G.; Saugel, B.; Sensen, B.; Rübsteck, C.; Pinnschmidt, H.O.; Kluge, S. Advance Directives and Powers of Attorney in Intensive Care Patients. Dtsch. Arztebl. Int. 2017, 114, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Klietz, M.; Berndt, J.M.; Wegner, F.; Schneider, N.; Höglinger, G.U.; Eggers, C.; Stiel, S. Consensus-Based Recommendations for Advance Directives of People with Parkinson’s Disease in Regard to Typical Complications by German Movement Disorder Specialists. J. Clin. Med. 2020, 9, 449. [Google Scholar] [CrossRef] [Green Version]
- Klietz, M.; Öcalan, Ö.; Schneider, N.; Dressler, D.; Stiel, S.; Wegner, F. Advance Directives of German People with Parkinson’s Disease Are Unspecific in regard to Typical Complications. Parkinsons Dis. 2019, 2019, 2107821. [Google Scholar] [CrossRef] [Green Version]
- Bertram, N.; Püschner, F.; Gonçalves, A.S.O.; Binder, S.; Amelung, V.E. Einführung einer elektronischen Patientenakte in Deutschland vor dem Hintergrund der internationalen Erfahrungen. In Krankenhaus-Report 2019: Das Digitale Krankenhaus; Klauber, J., Geraedts, M., Friedrich, J., Wasem, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–16. [Google Scholar]
- Kassenärztliche Bundesvereinigung (KBV). Anwendungen in der TI: Elektronischer Medikationsplan (eMP). Available online: https://www.kbv.de/html/emp.php (accessed on 19 September 2021).
- Gall, W.; Aly, A.F.; Sojer, R.; Spahni, S.; Ammenwerth, E. The national e-medication approaches in Germany, Switzerland and Austria: A structured comparison. Int. J. Med. Inform. 2016, 93, 14–25. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Information | |
|---|---|
| 1. | Address and personal data |
| 2. | Allergies |
| 3. | Important diagnoses |
| 4. | Vaccinations |
| 5. | Preexisting disabilities (e.g., blindness, deafness) |
| 6. | Important past operative procedures |
| 7. | Medication |
| 8. | Information on the general practitioner |
| 9. | Information about the patient will and where it can be found |
| 10. | Information on an organ donation statement and where it can be found |
| 11. | Information about a nursing care service |
| 12. | Photograph of the patient |
| 13. | Emergency contact data |
| 14. | Information on the existence of a pet and contact data of an emergency pet caregiver |
| n | % | |
|---|---|---|
| Medication scheme was brought to the ER | ||
| Yes | 74 | 72.6 |
| No | 28 | 27.4 |
| Medication was remembered correctly | ||
| Yes | 5 | 4.9 |
| No | 97 | 95.1 |
| Calling relatives/general practitioners was necessary | ||
| Yes | 25 | 24.5 |
| No | 76 | 74.5 |
| Not specified | 1 | 0.98 |
| Delay of diagnostics/treatment | ||
| Yes | 12 | 11.8 |
| No | 90 | 88.2 |
| Further explanation of the delay | ||
| Misjudgment due to lack of information | 5 | 35.7 |
| Additional unnecessary diagnostics | 4 | 28.6 |
| Relevant delay in treatment | 3 | 21.4 |
| Contraindicated therapy | 1 | 7.1 |
| Relevant delay in general | 1 | 7.1 |
| n | % | |
|---|---|---|
| Admission to the ER in the follow-up period | ||
| Yes | 29 | 23.4 |
| No | 95 | 76.6 |
| Transportation to the ER | ||
| From home, through rescue services | 20 | 69 |
| From home, brought by relatives | 4 | 13.8 |
| Admission from a medical practice | 5 | 17.2 |
| The emergency box was used by rescue services | ||
| Yes | 4 | 20 |
| No | 16 | 80 |
| Facilitated admission due to the emergency box | ||
| Yes | 4 | 100 |
| No | 0 | 0 |
| Correct application at the patients’ home | ||
| Storage in the fridge | ||
| Yes | 88 | 71 |
| No | 36 | 29 |
| Stickers were used correctly | ||
| Yes | 79 | 63.7 |
| No | 44 | 35.5 |
| Not specified | 1 | 0.8 |
| Inlet was filled out correctly | ||
| Yes | 109 | 87.9 |
| Partially | 8 | 6.5 |
| No | 3 | 2.4 |
| Not specified | 4 | 3.2 |
| Inlet was updated | ||
| Yes | 29 | 23.4 |
| Not necessary | 43 | 34.7 |
| No | 49 | 39.5 |
| Not specified | 3 | 2.4 |
| Further documents, e.g., medication list, were added | ||
| Yes | 51 | 41.1 |
| No | 70 | 56.5 |
| Not specified | 3 | 2.4 |
| Increased feeling of safety | ||
| Yes | 39 | 31.5 |
| No | 77 | 62.1 |
| Not specified | 8 | 6.5 |
| Further use in the future | ||
| Yes | 109 | 87.9 |
| No | 10 | 8.1 |
| Perhaps | 2 | 1.6 |
| Not specified | 3 | 2.4 |
| Satisfied with the handling | ||
| Yes | 103 | 83.1 |
| No | 6 | 4.8 |
| Not specified | 15 | 12.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krey, L.; Lange, P.; Tran, A.T.; Greten, S.; Höglinger, G.U.; Wegner, F.; Krause, O.; Klietz, M. Patient Safety in a Box: Implementation and Evaluation of the Emergency Box in Geriatric and Parkinson Patients. J. Clin. Med. 2021, 10, 5618. https://doi.org/10.3390/jcm10235618
Krey L, Lange P, Tran AT, Greten S, Höglinger GU, Wegner F, Krause O, Klietz M. Patient Safety in a Box: Implementation and Evaluation of the Emergency Box in Geriatric and Parkinson Patients. Journal of Clinical Medicine. 2021; 10(23):5618. https://doi.org/10.3390/jcm10235618
Chicago/Turabian StyleKrey, Lea, Pia Lange, Anh Thu Tran, Stephan Greten, Günter U. Höglinger, Florian Wegner, Olaf Krause, and Martin Klietz. 2021. "Patient Safety in a Box: Implementation and Evaluation of the Emergency Box in Geriatric and Parkinson Patients" Journal of Clinical Medicine 10, no. 23: 5618. https://doi.org/10.3390/jcm10235618
APA StyleKrey, L., Lange, P., Tran, A. T., Greten, S., Höglinger, G. U., Wegner, F., Krause, O., & Klietz, M. (2021). Patient Safety in a Box: Implementation and Evaluation of the Emergency Box in Geriatric and Parkinson Patients. Journal of Clinical Medicine, 10(23), 5618. https://doi.org/10.3390/jcm10235618