
Surgical Aortic Valve Replacement—Age-Dependent Choice of Prosthesis Type

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Endpoints
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Patients‘ Characteristics
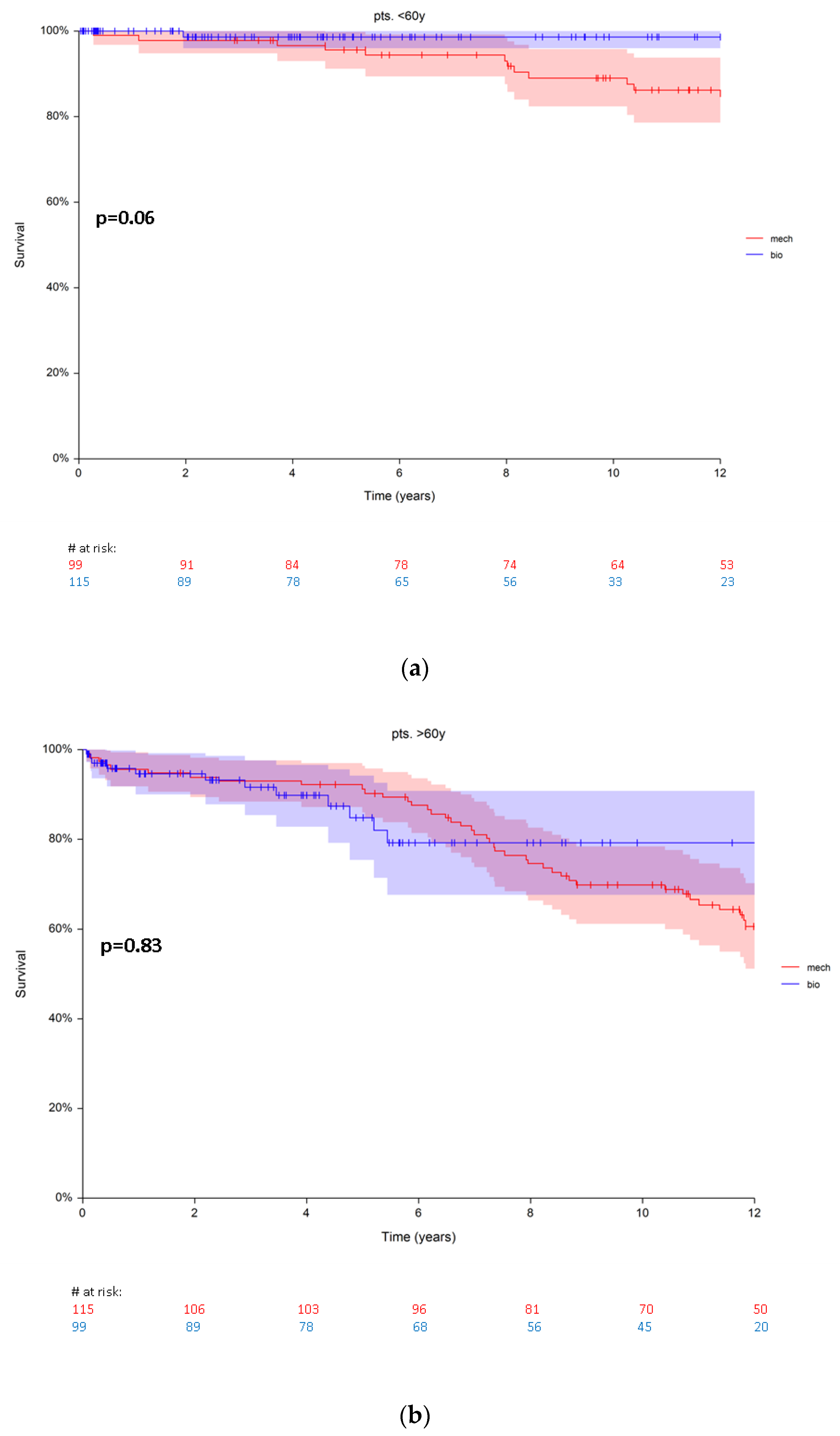
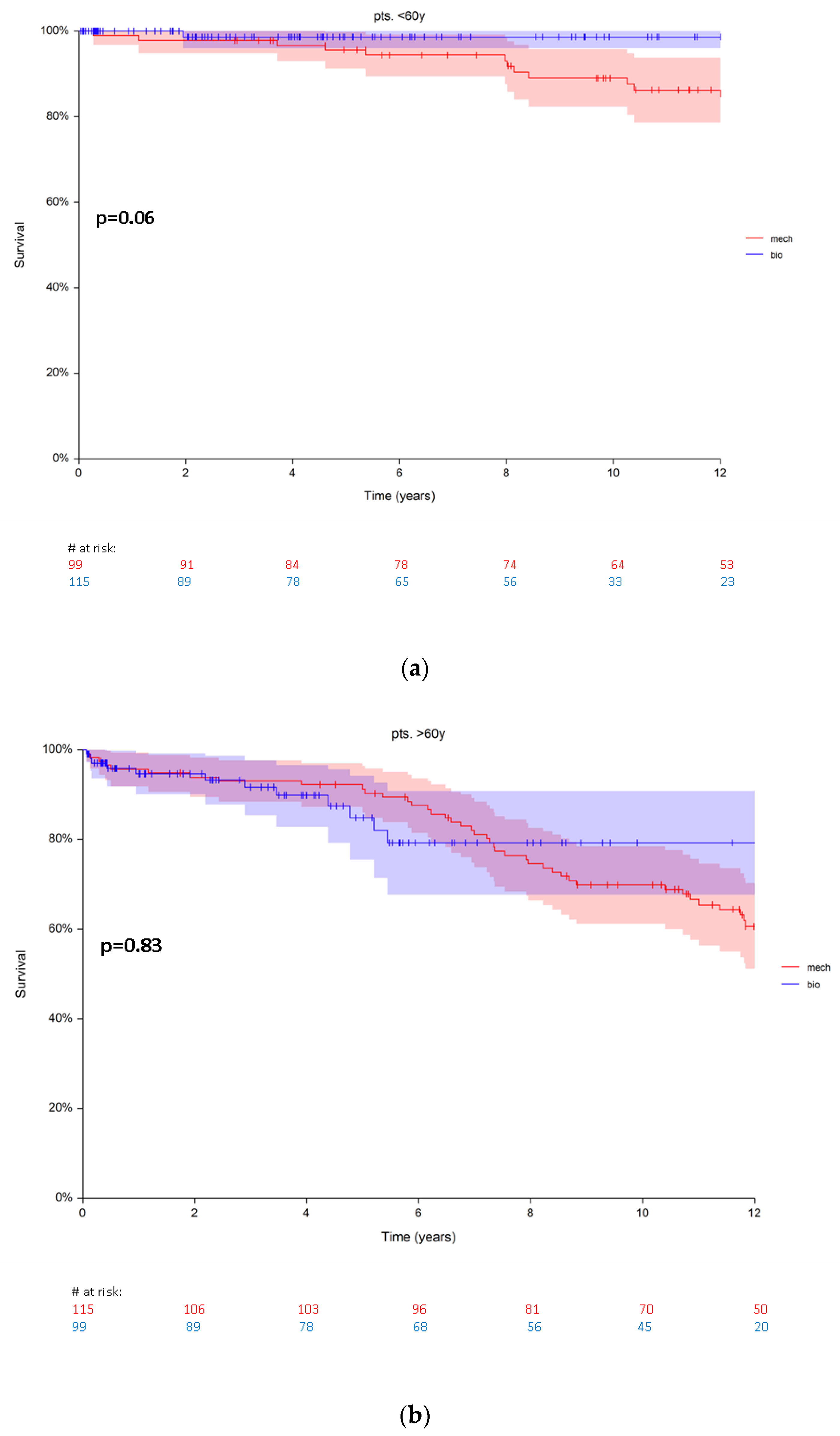
3.2. Mortality
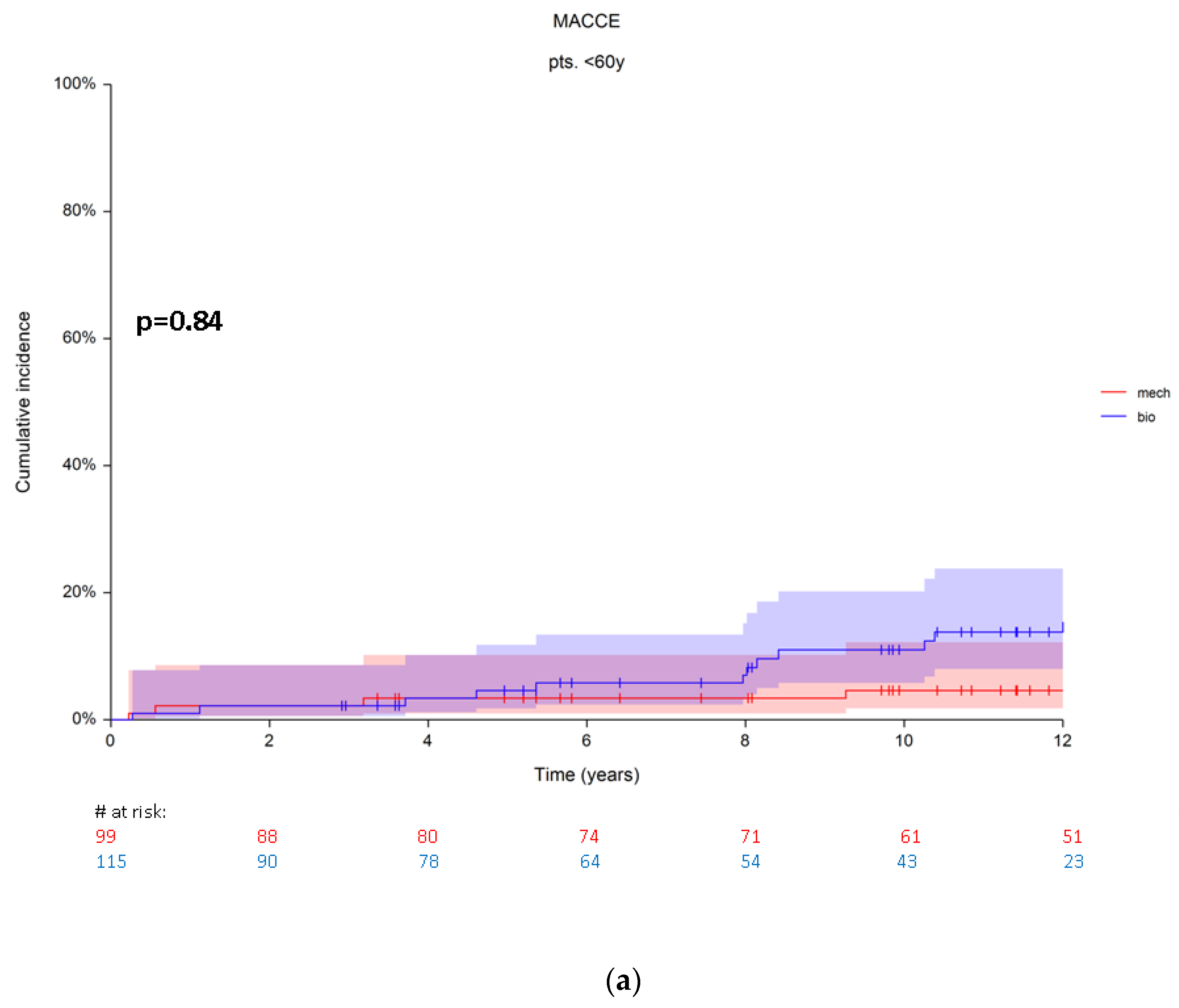
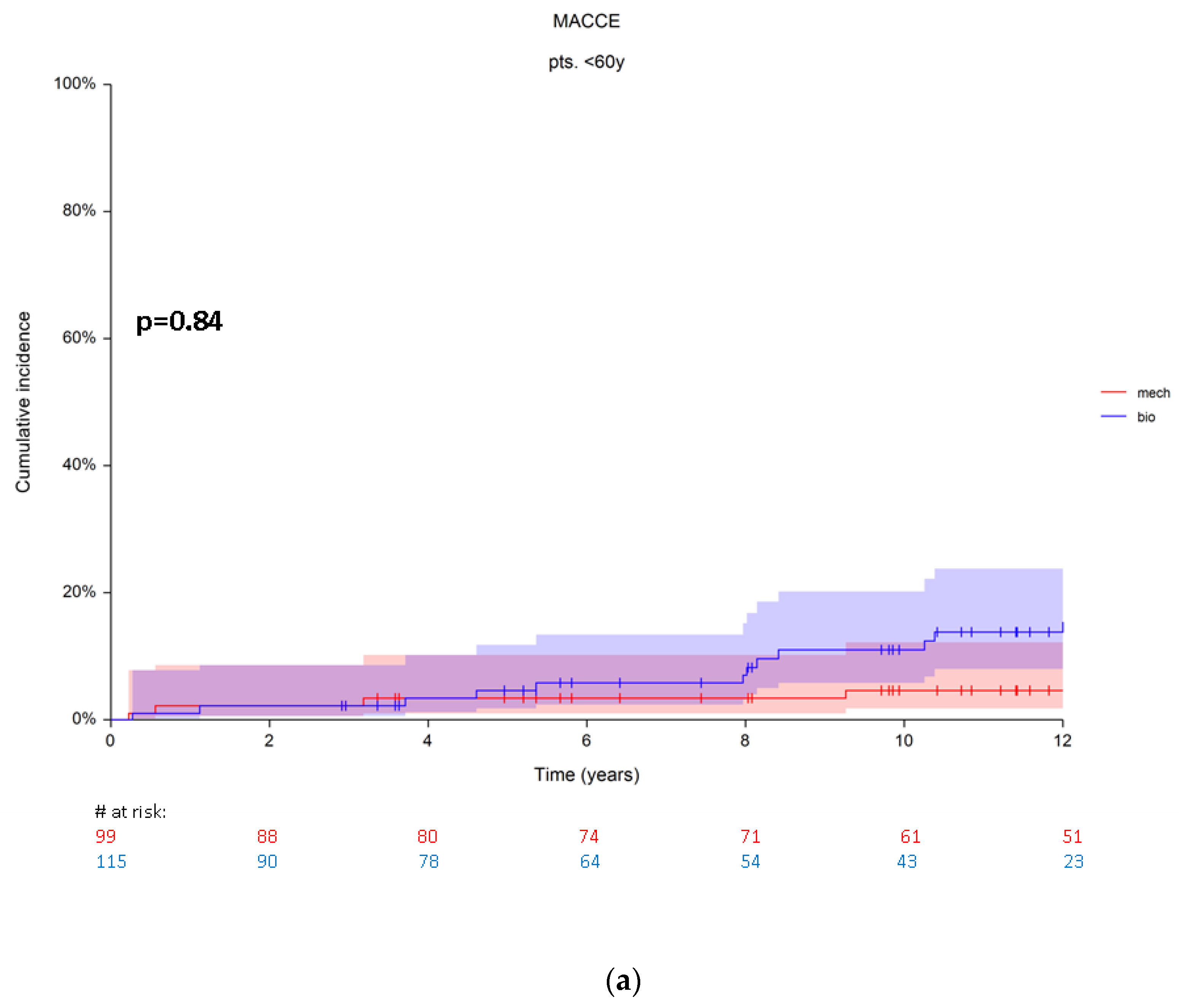
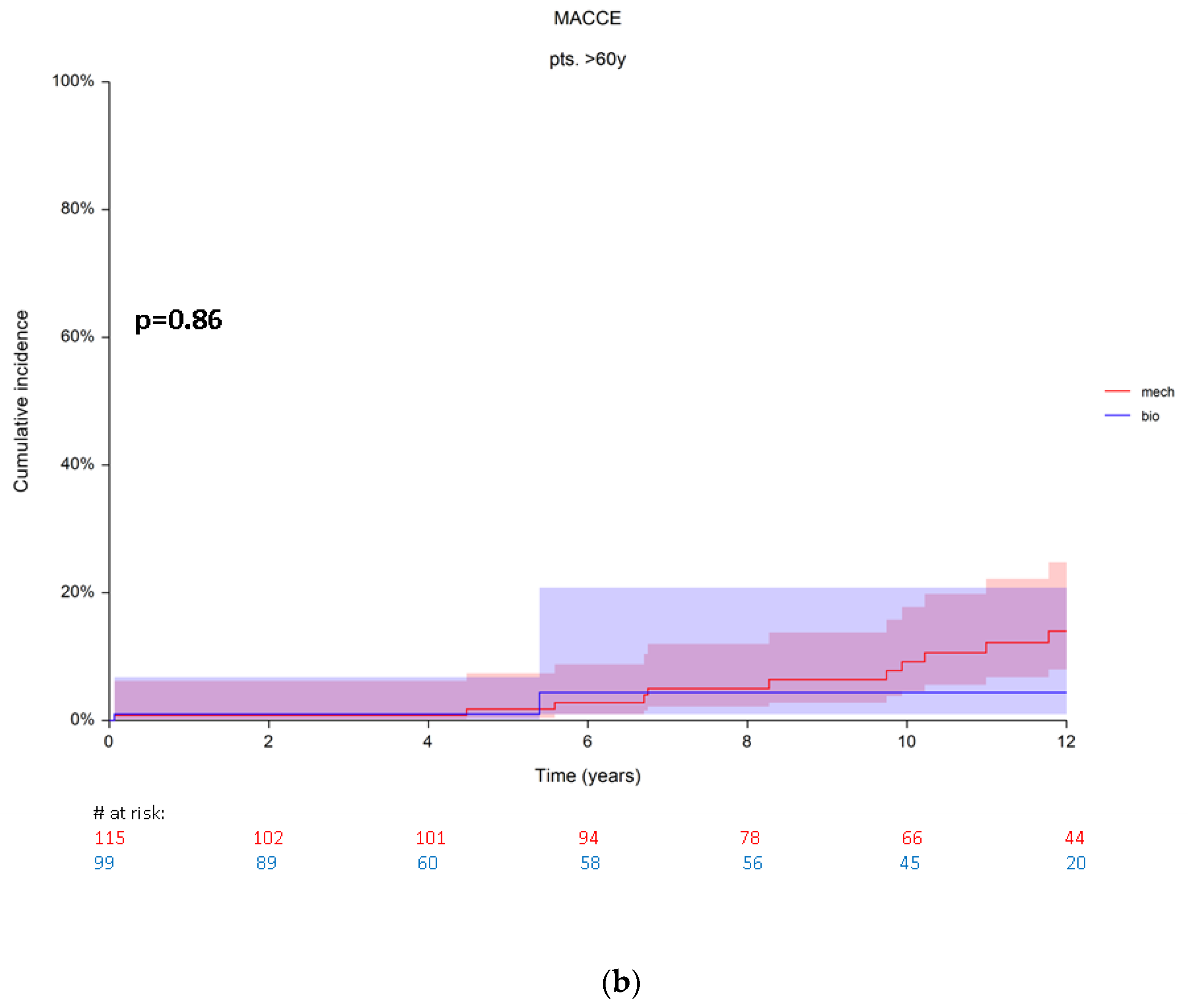
3.3. Major Adverse Cardiovascular and Cerebral Events (MACCE)
4. Discussion
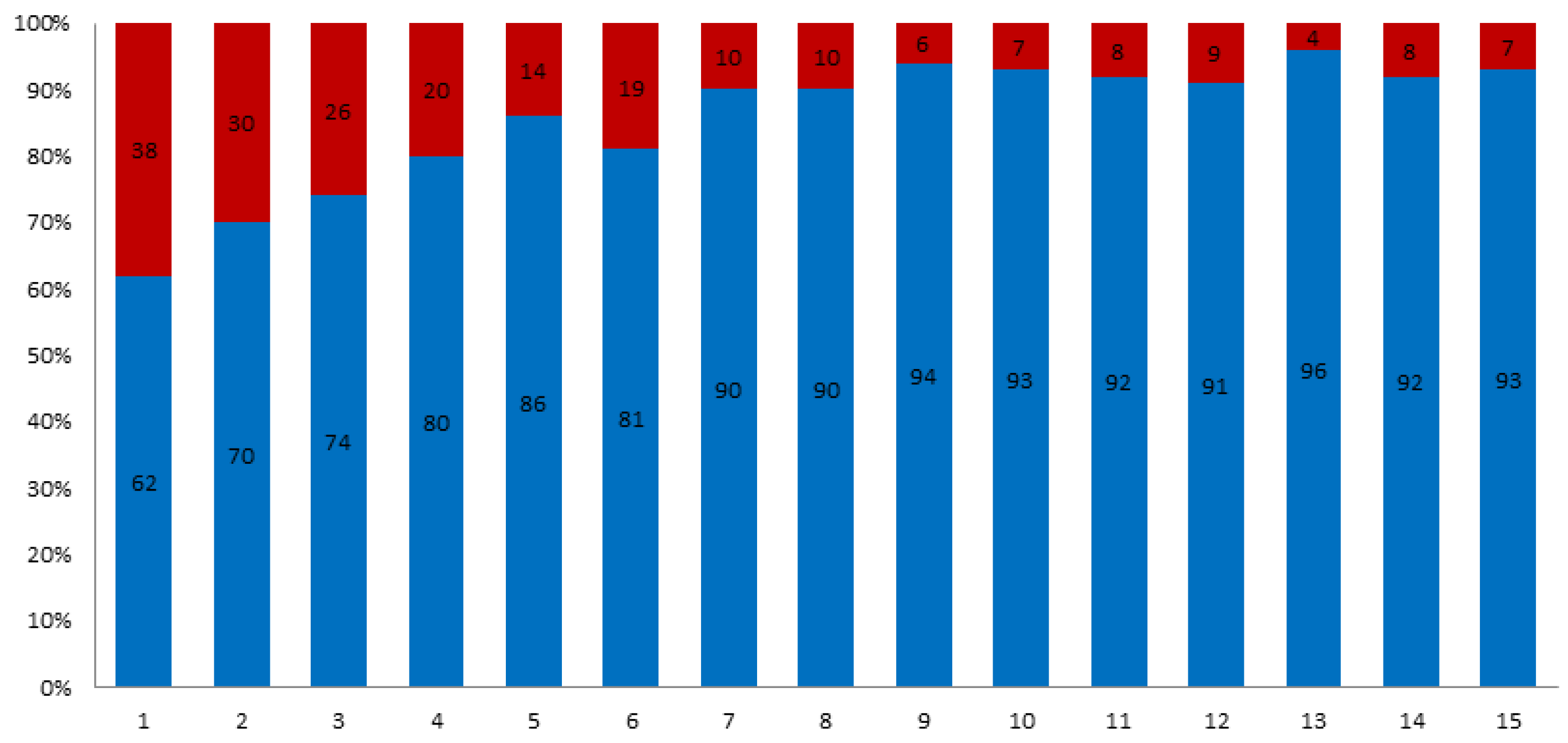
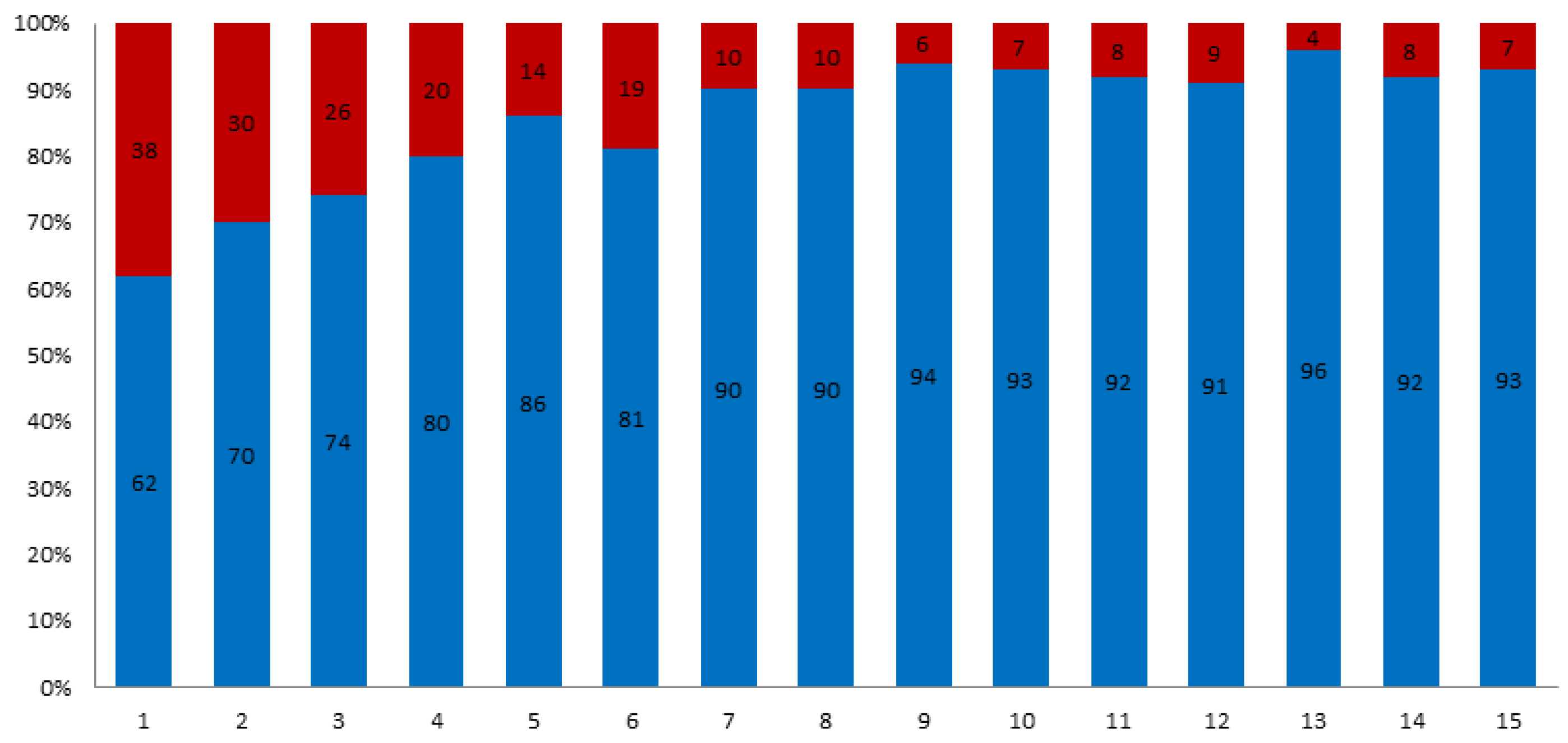
4.1. Growing Trend to Choose Bioprosthetic Replacement
4.2. Pros and Cons of Both Options Regarding MACCE
4.3. Options and Future Prospects
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Russo, A.; Grigioni, F.; Avierinos, J.; Freeman, W.K.; Suri, R.; Michelena, H.; Brown, R.; Sundt, T.M.; Enriquez-Sarano, M. Thromboembolic complications after surgical correction of mitral regurgitation incidence, predictors, and clinical implications. J. Am. Coll. Cardiol. 2008, 51, 1203–1211. [Google Scholar] [CrossRef] [Green Version]
- Chiang, Y.P.; Chikwe, J.; Moskowitz, A.J.; Itagaki, S.; Adams, D.H.; Egorova, N.N. Survival and long-term outcomes following bioprosthetic vs mechanical aortic valve replacement in patients aged 50 to 69 years. JAMA 2014, 312, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Glaser, N.; Jackson, V.; Holzmann, M.J.; Franco-Cereceda, A.; Sartipy, U. Aortic valve replacement with mechanical vs. biological prostheses in patients aged 50–69 years. Eur. Heart J. 2016, 37, 2658–2667. [Google Scholar] [PubMed] [Green Version]
- Goldstone, A.B.; Chiu, P.; Baiocchi, M.; Lingala, B.; Patrick, W.L.; Fischbein, M.P.; Woo, Y.J. Mechanical or biologic prostheses for aortic-valve and mitral-valve replacement. N. Engl. J. Med. 2017, 377, 1847–1857. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; de Bonis, M.; de Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 60, 727–800. [Google Scholar]
- Hammermeister, K.; Sethi, G.K.; Henderson, W.G.; Grover, F.L.; Oprian, C.; Rahimtoola, S.H. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: Final report of the Veterans Affairs randomized trial. J. Am. Coll. Cardiol. 2000, 36, 1152–1158. [Google Scholar] [CrossRef] [Green Version]
- Oxenham, H.; Bloomfield, P.; Wheatley, D.; Lee, R.J.; Cunningham, J.; Prescott, R.; Mille, H. Twenty year comparison of a Bjork-Shiley mechanical heart valve with porcine bioprostheses. Heart 2003, 89, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Stassano, P.; di Tommaso, L.; Monaco, M.; Iorio, F.; Pepino, P.; Spampinato, N.; Vosa, C. Aortic valve replacement: A prospective randomized evaluation of mechanical versus biological valves in patients ages 55 to 70 years. J. Am. Coll. Cardiol. 2009, 54, 1862–1868. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; Falk, V.; Bax, J.J.; de Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. J. Thorac. Cardiovasc. Surg. 2013, 145, 6–23. [Google Scholar] [CrossRef] [Green Version]
- Une, D.; Ruel, M.; David, T.E. Twenty-year durability of the aortic Hancock II bioprosthesis in young patients: Is it durable enough? Eur. J. Cardiothorac. Surg. 2014, 46, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Potter, D.D.; Sundt, T.M., 3rd; Zehr, K.J.; Dearani, J.A.; Daly, R.C.; Mullany, C.J.; McGregor, C.G.A.; Puga, F.J.; Schaff, H.V.; Orszulak, T.A. Operative risk of reoperative aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2005, 129, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Head, S.J.; Celik, M.; Kappetein, A.P. Mechanical versus bioprosthetic aortic valve replacement. Eur. Heart J. 2017, 38, 2183–2191. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.L.; Schaff, H.V.; Lahr, B.D.; Mullany, C.J.; Sundt, T.M.; Dearani, J.A.; McGregor, C.G.; Orszulak, T.A. Aortic valve replacement in patients aged 50 to 70 years: Improved outcome with mechanical versus biologic prostheses. J. Thorac. Cardiovasc. Surg. 2008, 135, 878–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, D.F.; Seco, M.; Wu, J.J.; Edelman, J.B.; Wilson, M.K.; Vallely, M.P.; Byrom, M.J.; Bannon, P.G. Mechanical Versus Bioprosthetic Aortic Valve Replacement in Middle-Aged Adults: A Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2016, 102, 315–327. [Google Scholar] [CrossRef] [Green Version]
- Chikwe, J.; Chiang, Y.P.; Egorova, N.N.; Itagaki, S.; Adams, D.H. Survival and outcomes following bioprosthetic vs mechanical mitral valve replacement in patients aged 50 to 69 years. JAMA 2015, 313, 1435–1442. [Google Scholar] [CrossRef]
- Isaacs, A.J.; Shuhaiber, J.; Salemi, A.; Isom, O.W.; Sedrakyan, A. National trends in utilization and in-hospital outcomes of mechanical versus bioprosthetic aortic valve replacements. J. Thorac. Cardiovasc. Surg. 2015, 149, 1262–1269 e3. [Google Scholar] [CrossRef] [Green Version]
- Diaz, R.; Hernandez-Vaquero, D.; Alvarez-Cabo, R.; Avanzas, P.; Silva, J.; Moris, C.; Pascual, I. Long-term outcomes of mechanical versus biological aortic valve prosthesis: Systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2019, 158, 706–714 e18. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; Noureddine, H.; Englberger, L.; Dick, F.; Gahl, B.; Aymard, T.; Czerny, M.; Tevaearai, H.; Mario Stalder, T.P.C. Ten-year comparison of pericardial tissue valves versus mechanical prostheses for aortic valve replacement in patients younger than 60 years of age. J. Thorac. Cardiovasc. Surg. 2012, 144, 1075–1083. [Google Scholar] [CrossRef] [Green Version]
- Kaneko, T.; Aranki, S.; Javed, Q.; McGurk, S.; Shekar, P.; Davidson, M.; Cohn, L. Mechanical versus bioprosthetic mitral valve replacement in patients < 65 years old. J. Thorac. Cardiovasc. Surg. 2014, 147, 117–126. [Google Scholar]
- Korteland, N.M.; Etnel, J.R.G.; Arabkhani, B.; Mokhles, M.M.; Mohamad, A.; Roos-Hesselink, J.W.; Bogers, A.J.J.C.; Takkenberg, J.J.M. Mechanical aortic valve replacement in non-elderly adults: Meta-analysis and microsimulation. Eur. Heart J. 2017, 38, 3370–3377. [Google Scholar] [CrossRef] [PubMed]
- McClure, R.S.; McGurk, S.; Cevasco, M.; Maloney, A.; Gosev, I.; Wiegerinck, E.M.; Salvio, G.; Tokmaji, G.; Borstlap, W.; Nauta, F.; et al. Late outcomes comparison of nonelderly patients with stented bioprosthetic and mechanical valves in the aortic position: A propensity-matched analysis. J. Thorac. Cardiovasc. Surg. 2014, 148, 1931–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krane, M.; Boehm, J.; Prinzing, A.; Ziegelmueller, J.; Holfeld, J.; Lange, R. Excellent Hemodynamic Performance After Aortic Valve Neocuspidization Using Autologous Pericardium. Ann. Thorac. Surg. 2020, 111, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Etnel, J.R.G.; Grashuis, P.; Huygens, S.A.; Pekbay, B.; Papageorgiou, G.; Helbing, W.A.; Roos-Hesselink, J.W.; Bogers, A.J.J.C.; Mokhles, M.M.; Takkenberg, J.J.M. The Ross procedure: A systematic review and meta-analysis. Circulation 2009, 119, 222–228. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Propensity Score Matching | ||||
|---|---|---|---|---|
| Bioprosthesis n = 1845 | Mechnical Prosthesis n = 327 | p | Standardised Mean Difference | |
| Age, years | 69 ± 10 | 54 ± 13 | <0.01 | −2.04 |
| Sex, men | 1064 (57) | 229 (70) | <0.01 | −4.18 |
| Weight, kg | 79 ± 15 | 78 ± 10 | 0.06 | −1.34 |
| Height, cm | 179 ± 16 | 177 ± 14 | 0.15 | −1.40 |
| Chronic obstructive pulmonary disease, n (%) | 188 (10) | 25 (7.6) | 0.19 | −1.43 |
| Peripheral vascular disease, n (%) | 66 (3.5) | 8 (2.4) | 0.29 | −1.04 |
| Hyperlipoproteinemia, n (%) | 702 (38) | 88 (2.7) | <0.01 | −3.86 |
| Arterial hypertension, n (%) | 1403 (76) | 185 (56) | <0.01 | −7.33 |
| Pulmonary hypertension, n (%) | 249 (13.5) | 42 (12.8) | 0.74 | −3.21 |
| Diabetes mellitus, n (%) | 336 (18) | 33 (10) | <0.01 | −3.60 |
| Stroke, n (%) | 66 (3.5) | 8 (2.4) | 0.40 | −1.04 |
| Cancer, n (%) | 151 (8) | 9 (2.7) | 0.001 | −3.46 |
| After Propensity Score Matching | ||||
| Bioprosthesis n = 214 | Mechnical prosthesis n = 214 | p | Standardised Mean Difference | |
| Age, years | 60 ± 10 | 60 ± 9 | 0.14 | −3.45 |
| Sex, men | 149 (69.6) | 140 (65) | 0.40 | 1.92 |
| Weight, kg | 81 ± 16 | 80 ± 14 | 0.86 | −2.90 |
| Height, cm | 180 ± 15 | 179 ± 16 | 0.98 | −1.94 |
| Chronic obstructive pulmonary disease, n (%) | 8 (3.7) | 16 (7.4) | 0.14 | 1.67 |
| Peripheral vascular disease, n (%) | 1 (0.5) | 5 (2.3) | 0.21 | 1.64 |
| Hyperlipoproteinemia, n (%) | 87 (40) | 66 (30) | 0.04 | −2.11 |
| Arterial hypertension, n (%) | 164 (76) | 138 (64) | 0.006 | −2.75 |
| Pulmonary hypertension, n (%) | 54 (25) | 29 (13.5) | 0.005 | −3.08 |
| Diabetes mellitus, n (%) | 44 (20) | 29 (13.5) | 0.07 | −1.92 |
| Stroke, n (%) | 13 (6) | 8 (3.7) | 0.26 | −1.11 |
| Cancer, n (%) | 13 (6) | 9 (4.2) | 0.42 | −4.36 |
| Pts. < 60 y n = 214 | Pts. > 60 y n = 214 | p | Standardised Mean Difference | |
|---|---|---|---|---|
| Sex, men | 139 (64.9) | 150 (70) | 0.40 | −3.51 |
| Weight, kg | 80 ± 14 | 82 ± 6 | 0.80 | 1.92 |
| Height, cm | 180 ± 16 | 179 ± 16 | 0.98 | −2.90 |
| Chronic obstructive pulmonary disease, n (%) | 11 (5.1) | 13 (6) | 0.90 | −2.96 |
| Peripheral vascular disease, n (%) | 1 (0.46) | 5 (2.3) | 0.21 | 1.49 |
| Hyperlipoproteinemia, n (%) | 66 (30.8) | 87 (40.6) | 0.04 | −3.40 |
| Arterial hypertension, n (%) | 145 (67.7) | 157 (73) | 0.07 | −2.02 |
| Pulmonary hypertension, n (%) | 43 (20) | 40 (18.6) | 0.89 | −2.56 |
| Diabetes mellitus, n (%) | 31 (14.4) | 42 (19.6) | 0.08 | −3.81 |
| Stroke, n (%) | 8 (3.7) | 13 (6) | 0.26 | −1.92 |
| Cancer, n (%) | 8 (3.7) | 14 (6.5) | 0.40 | −1.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitanova, K.; Wirth, F.; Boehm, J.; Burri, M.; Lange, R.; Krane, M. Surgical Aortic Valve Replacement—Age-Dependent Choice of Prosthesis Type. J. Clin. Med. 2021, 10, 5554. https://doi.org/10.3390/jcm10235554
Vitanova K, Wirth F, Boehm J, Burri M, Lange R, Krane M. Surgical Aortic Valve Replacement—Age-Dependent Choice of Prosthesis Type. Journal of Clinical Medicine. 2021; 10(23):5554. https://doi.org/10.3390/jcm10235554
Chicago/Turabian StyleVitanova, Keti, Felix Wirth, Johannes Boehm, Melchior Burri, Rüdiger Lange, and Markus Krane. 2021. "Surgical Aortic Valve Replacement—Age-Dependent Choice of Prosthesis Type" Journal of Clinical Medicine 10, no. 23: 5554. https://doi.org/10.3390/jcm10235554
APA StyleVitanova, K., Wirth, F., Boehm, J., Burri, M., Lange, R., & Krane, M. (2021). Surgical Aortic Valve Replacement—Age-Dependent Choice of Prosthesis Type. Journal of Clinical Medicine, 10(23), 5554. https://doi.org/10.3390/jcm10235554