
Multicenter Study of Whole Breast Stiffness Imaging by Ultrasound Tomography (SoftVue) for Characterization of Breast Tissues and Masses


Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects and Masses
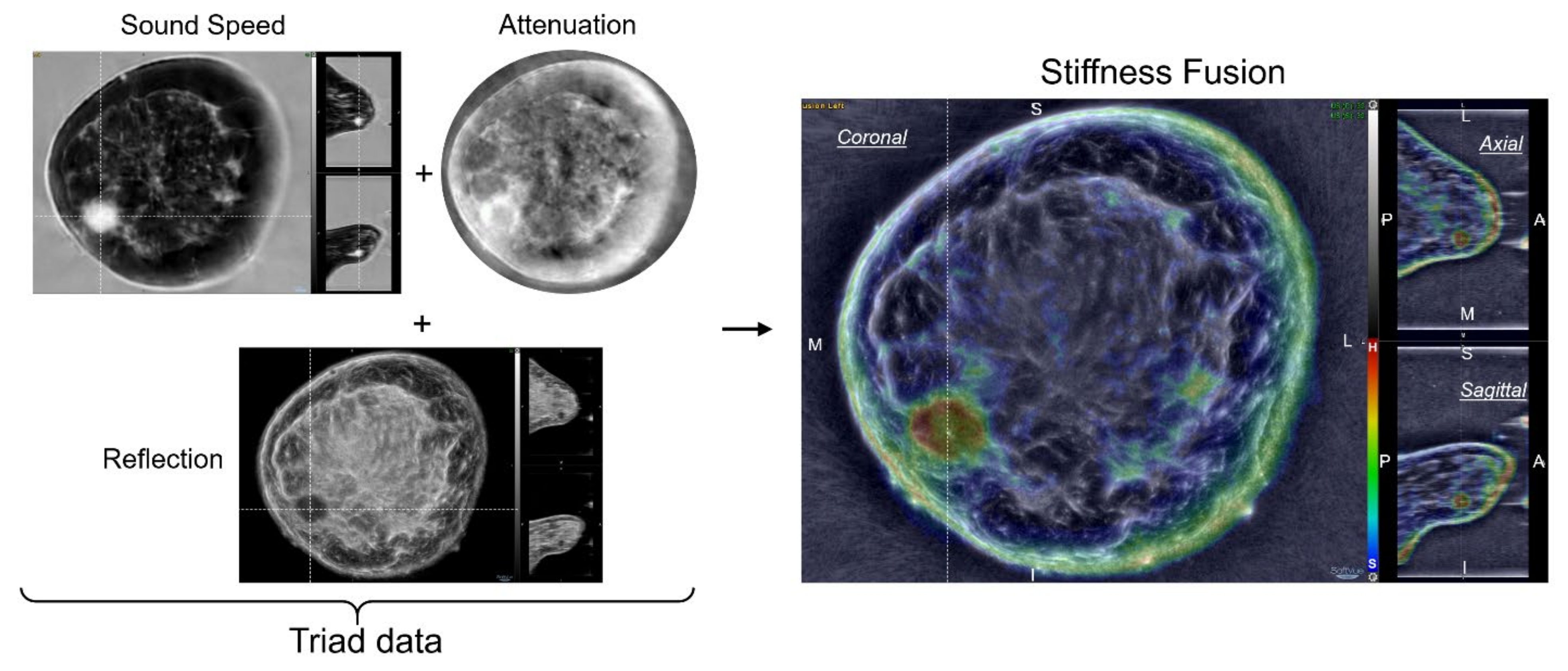
2.2. Equipment–SoftVue Ultrasound Tomography (UST) and Stiffness Imaging
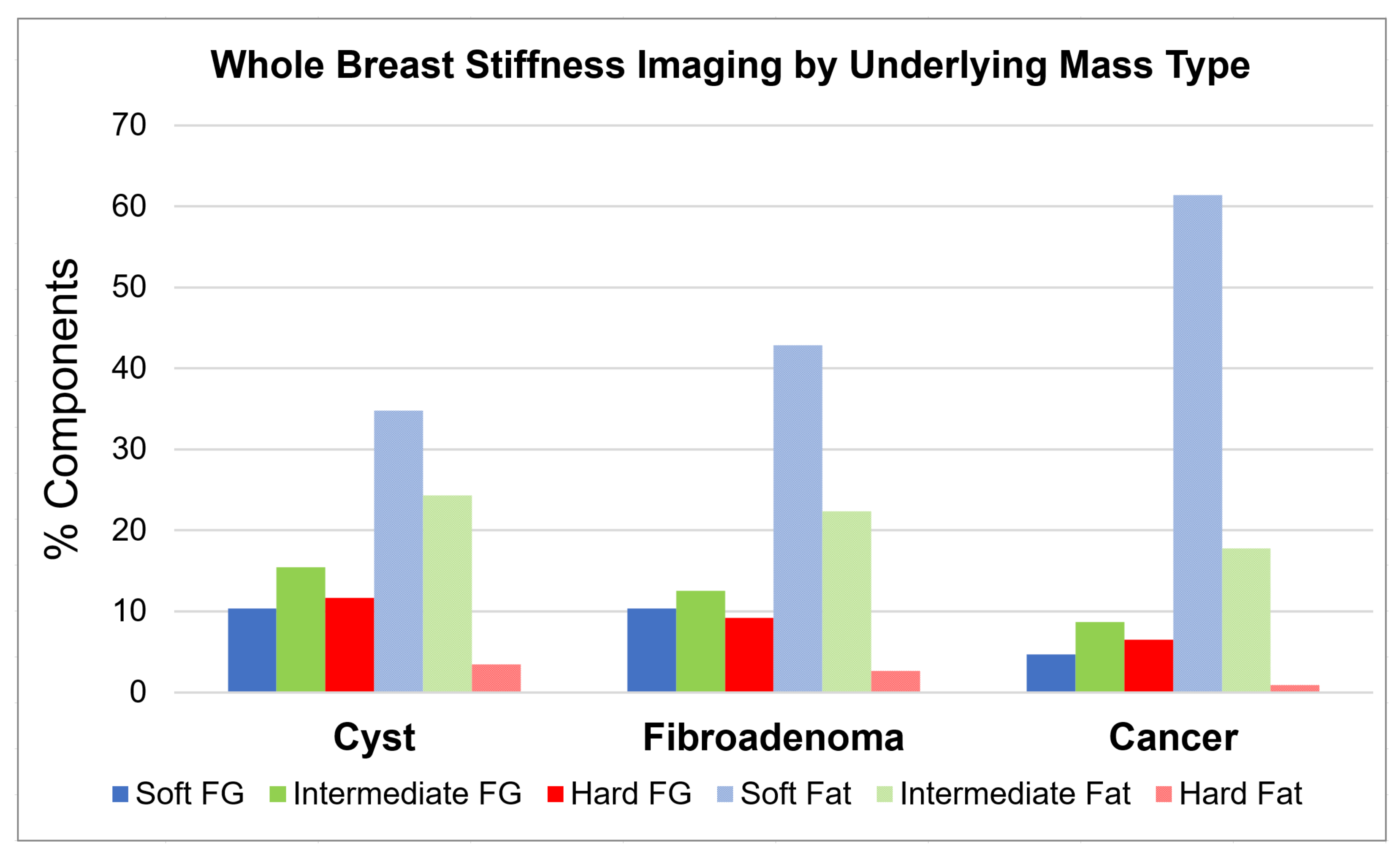
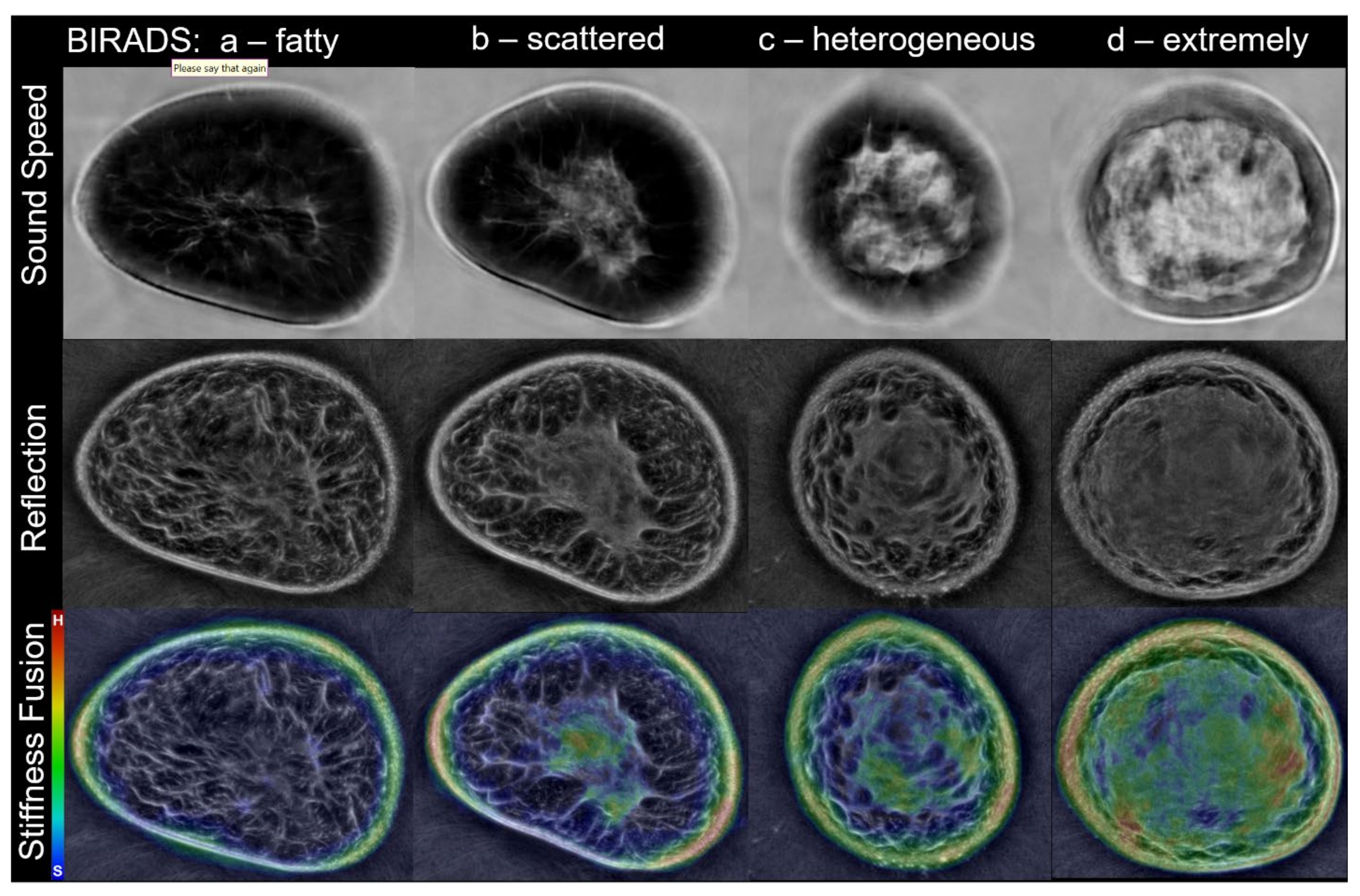
2.3. Whole Breast Tissue Stiffness Distributions
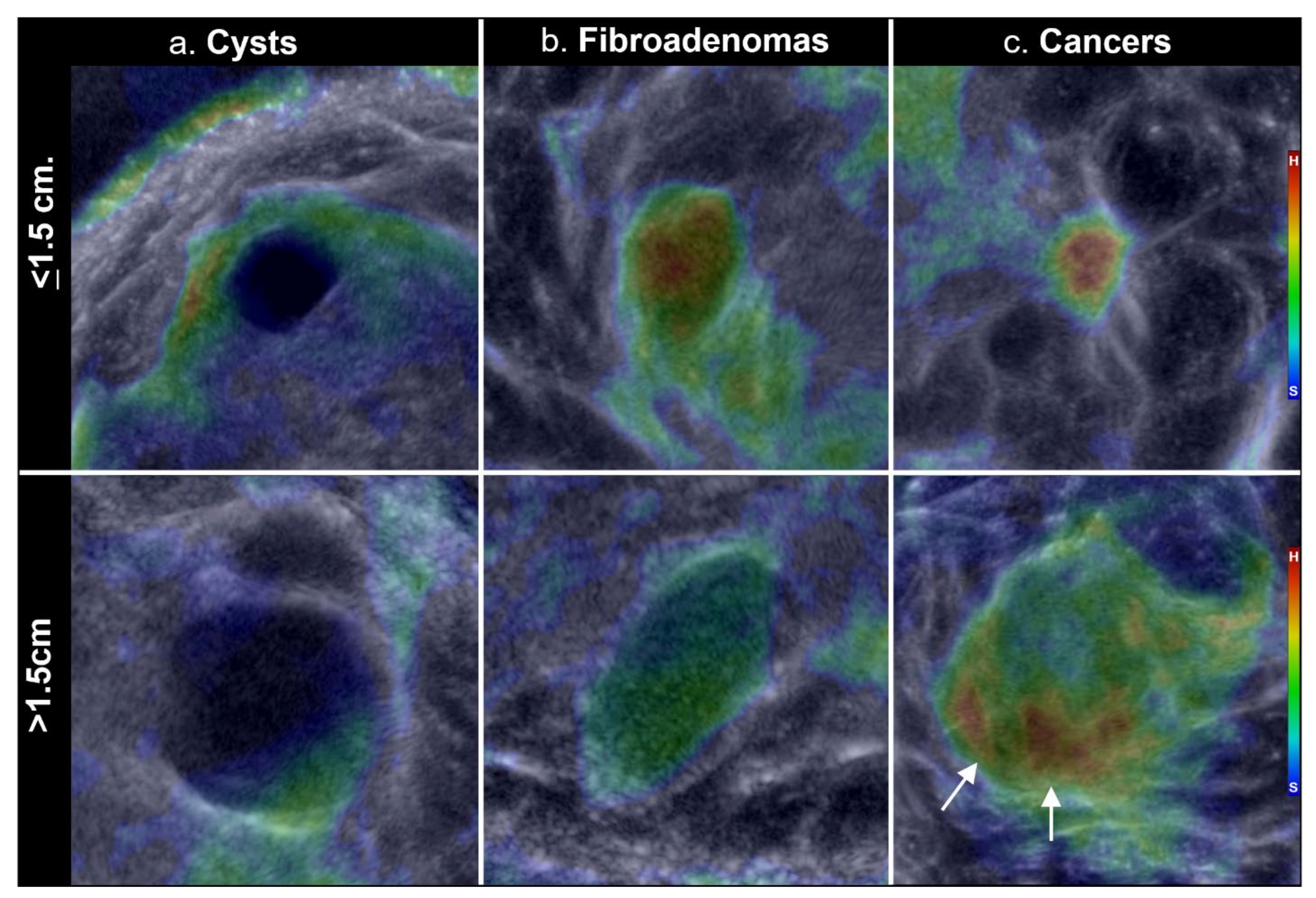
2.4. Mass Stiffness Distributions
2.5. Statistical Analyses
3. Results
3.1. Subjects and Masses
3.2. Whole Breast Stiffness
3.3. Mass Stiffness Distributions
4. Discussion
4.1. Whole Breast Stiffness
4.2. Mass Stiffness Distributions
4.3. Current and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mendelson, E.B.; Bohm-Velez, M.; Berg, W.A.; Whitman, G.J.; Feldman, M.I.; Madjar, H. ACR BI-RADS® Ultrasound. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System, 5th ed.; American College of Radiology: Reston, VA, USA, 2013; pp. 128–130. [Google Scholar]
- Baumgart, F. Stiffness—An unknown world of mechanical science? Injury 2000, 31 (Suppl. 2), 14–23. [Google Scholar]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: Basic principles and technology. Ultraschall Medizin-European J. Ultrasound 2013, 34, 169–184. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.J.; Choi, H.; Park, E.H.; Song, J.S.; Youk, J.H. Evaluation of an automated breast volume scanner according to the fifth edition of BI-RADS for breast ultrasound compared with hand-held ultrasound. Eur. J. Radiol. 2018, 99, 138–145. [Google Scholar] [CrossRef]
- Duric, N.; Littrup, P.; Poulo, L.; Babkin, A.; Pevzner, R.; Holsapple, E.; Rama, O.; Glide, C. Detection of breast cancer with ultrasound tomography: First results with the Computed Ultrasound Risk Evaluation (CURE) prototype. Med. Phys. 2007, 34, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Duric, N.; Boyd, N.; Littrup, P.; Sak, M.; Myc, L.; Li, C.; West, E.; Minkin, S.; Martin, L.; Yaffe, M.; et al. Breast density measurements with ultrasound tomography: A comparison with film and digital mammography. Med. Phys. 2013, 40, 013501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duric, N.; Littrup, P.; Li, C.; Roy, O.; Schmidt, S.; Seamans, J.; Wallen, A.; Bey-Knight, L. Whole breast tissue characterization with ultrasound tomography. In Proceedings of the SPIE Medical Imaging: Ultrasonic Imaging and Tomography, Orlando, FL, USA, 21–26 February 2015; International Society for Optics and Photonics: Bellingham, WA, USA, 2015; Volume 9419, p. 94190G. [Google Scholar]
- Malik, B.; Klock, J.; Wiskin, J.; Lenox, M. Objective breast tissue image classification using quantitative transmission ultrasound tomography. Sci. Rep. 2016, 6, 38857. [Google Scholar] [CrossRef] [Green Version]
- Iuanow, E.; Smith, K.; Obuchowski, N.A.; Bullen, J.; Klock, J. Accuracy of cyst versus solid diagnosis in the breast using quantitative transmission (QT) ultrasound. Acad. Radiol. 2017, 24, 1148–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiskin, J.; Malik, B.; Natesan, R.; Lenox, M. Quantitative assessment of breast density using transmission ultrasound tomography. Med. Phys. 2019, 46, 2610–2620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, B.; Klock, J. Breast cyst fluid analysis correlations with speed of sound using transmission ultrasound. Acad. Radiol. 2019, 26, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Duric, N.; Sak, M.; Fan, S.; Pfeiffer, R.M.; Littrup, P.J.; Simon, M.S.; Gorski, D.H.; Ali, H.; Purrington, K.S.; Brem, R.F.; et al. Using whole breast ultrasound tomography to improve breast cancer risk assessment: A novel risk factor based on the quantitative tissue property of sound speed. J. Clin. Med. 2020, 9, 367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duric, N.; Littrup, P.; Sak, M.; Li, C.; Chen, D.; Roy, O.; Brem, R. A novel marker, based on ultrasound tomography, for monitoring early response to neoadjuvant chemotherapy. J. Breast Imaging 2020, 2, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Ranger, B.; Littrup, P.J.; Duric, N.; Chandiwala-Mody, P.; Li, C.; Schmidt, S.; Lupinacci, J. Breast ultrasound tomography versus MRI for clinical display of anatomy and tumor rendering: Preliminary results. AJR Am. J. Roentgenol. 2012, 198, 233–239. [Google Scholar] [CrossRef] [Green Version]
- O’Flynn, E.A.M.; Fromageau, J.; Ledger, A.E.; Messa, A.; D’Aquino, A.; Schoemaker, M.J.; Schmidt, M.; Duric, N.; Swerdlow, A.J.; Bamber, J.C. Ultrasound tomography evaluation of breast density: A comparison with non-contrast magnetic resonance imaging. Investig. Radiol. 2017, 52, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Sak, M.; Duric, N.; Littrup, P.; Bey-Knight, L.; Ali, H.; Vallieres, P.; Sherman, M.E.; Gierach, G.L. Using speed of sound imaging to characterize breast density. Ultrasound Med. Biol. 2017, 43, 91–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sak, M.; Duric, N.; Littrup, P.; Sherman, M.; Gierach, G. Ultrasound Tomography Imaging with Waveform Sound Speed: Parenchymal Changes in Women Undergoing Tamoxifen Therapy. In Medical Imaging 2017: Ultrasonic Imaging and Tomography; International Society for Optics and Photonics: Bellingham, DC, USA, 2017; Volume 10139, p. 101390W. [Google Scholar]
- Sandhu, G.Y.; Li, C.; Roy, O.; Schmidt, S.; Duric, N. Frequency domain ultrasound waveform tomography: Breast imaging using a ring transducer. Phys. Med. Biol. 2015, 60, 5381. [Google Scholar] [CrossRef]
- Duck, F.A. Physical Properties of Tissue; Academic Press: London, UK, 1990. [Google Scholar]
- Mast, T.D. Empirical relationships between acoustic parameters in human soft tissues. Acoust. Res. Lett. Online 2000, 1, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Wells, P.N.T.; Liang, H.D. Medical ultrasound: Imaging of soft tissue strain and elasticity. J. R. Soc. Interface 2011, 8, 1521–1549. [Google Scholar] [CrossRef] [Green Version]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound elastography: Review of techniques and clinical applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Glozman, T.; Azhari, H. A method for characterization of tissue elastic properties combining ultrasonic computed tomography with elastography. Ultrasound Med. 2010, 29, 387–398. [Google Scholar] [CrossRef] [Green Version]
- Littrup, P.J.; Duric, N.; Sak, M.; Li, C.; Roy, O.; Brem, R.F.; Yamashita, M. The fat-glandular interface and breast tumor locations: Appearances on ultrasound tomography are supported by quantitative peritumoral analysis. J. Breast Imaging 2021, 3, 455–464. [Google Scholar] [CrossRef]
- Kompaniez-Dunigan, E.; Abbey, C.K.; Boone, J.M.; Webster, M.A. Visual adaptation and the amplitude spectra of radiological images. Cogn. Res. Princ. Implic. 2018, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haralick, R.M.; Sternberg, S.R.; Zhuang, X. Image analysis using mathematical morphology. IEEE Trans. Pattern Anal. Mach. Intell. 1987, 9, 532–550. [Google Scholar] [CrossRef] [PubMed]
- Gubarkova, E.V.; Sovetsky, A.A.; Zaitsev, V.Y.; Matveyev, A.L.; Vorontsov, D.A.; Sirotkina, M.A.; Matveev, L.A.; Plekhanov, A.A.; Pavlova, N.P.; Kuznetsov, S.S.; et al. OCT-elastography-based optical biopsy for breast cancer delineation and express assessment of morphological/molecular subtypes. Biomed. Opt. Express 2019, 10, 2244–2263. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.H.; Li, M.; Han, W.S.; Ryu, H.S.; Moon, W.K. The spatial relationship of malignant and benign breast lesions with respect to the fat-gland interface on magnetic resonance imaging. Nat. Sci. Rep. 2016, 6, 39085. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SoftVue UST Operating Parameters | |
|---|---|
| Number of transducer elements | 2048 |
| Maximum breast diameter | 22 cm |
| Anatomic coverage (visualized) | Pectoralis muscle to nipple |
| Operating frequency | 3 MHz |
| Imaging resolution (Superior-inferior × Transverse × Anterior-posterior) | 0.75 × 0.75 × 2.5 mm |
| Data acquisition time per breast | ~2 min |
| Reconstruction time per slice | 4 s |
| Patient throughput (projected) | 4 h |
| Radiologists review time (~complexity) | 2–4 min |
| #Slices per stack (~breast size) | ~30–60 |
| Mass Histology | Count (N) | <1.5 cm | >1.5 cm |
|---|---|---|---|
| Cancer | 78 | 52 | 26 |
| Subtypes: IDC | 57 | 37 | 20 |
| DCIS alone | 6 | 5 | 1 |
| ILC | 10 | 5 | 5 |
| Other | 3 | 3 | 0 |
| DCIS + IDC | 2 | 2 | 0 |
| Fibroadenoma | 105 | 88 | 17 |
| Cyst | 91 | 80 | 11 |
| Other benign | 24 | 21 | 3 |
| Subtypes: Containing fibrosis | 21 | ||
| Fibrocystic change | 2 | ||
| Granulomatous Mastitis | 1 | ||
| Totals | 298 | 241 | 57 |
| Fibroglandular | Fatty | Total | ||||
|---|---|---|---|---|---|---|
| (cc) | % Total | (cc) | % Total | (cc) | % Total | |
| Hard | 66 | 9.0% | 16 | 2.2% | 82 | 11.2% |
| Intermediate | 87 | 11.8% | 160 | 21.7% | 247 | 33.4% |
| Soft | 61 | 8.3% | 347 | 47.1% | 408 | 55.4% |
| Total | 214 | 29.1% | 523 | 71.0% | 737 | 100.0% |
| Total Mass Comparisons | Stiffness (5–95% C.I) | p Values | |||
|---|---|---|---|---|---|
| Small | Unfiltered | Cancer (CA) | 0.1256–0.8585 | CA vs. Cyst: | 0.000000001 |
| (≤1.5 cm) | Fibroadenoma (FA) | 0.0021–0.8634 | CA vs. FA: | 0.08 | |
| Cyst | 0.00012–0.6499 | Cyst vs. FA: | 0.0000017 | ||
| Filtered | Cancer (CA) | 0.1247–0.6967 | CA vs. Cyst: | 6 × 10−11 | |
| Fibroadenoma (FA) | 0.1704–0.5303 | CA vs. FA: | 0.000036 | ||
| Cyst | 0.001–0.3618 | Cyst vs. FA: | 0.00028 | ||
| Large | Unfiltered | Cancer (CA) | 0.1916–0.8288 | CA vs. Cyst: | 2 × 10−10 |
| (>1.5 cm) | Fibroadenoma (FA) | 0.036–0.7005 | CA vs. FA: | 0.037 | |
| Cyst | 0.00034–0.2364 | Cyst vs. FA: | 0.00013 | ||
| Filtered | Cancer (CA) | 0.0826–0.8104 | CA vs. Cyst: | 0.00000021 | |
| Fibroadenoma (FA) | 0.0197–0.4830 | CA vs. FA: | 0.127 | ||
| Cyst | 0.00005–0.0691 | Cyst vs. FA: | 0.000025 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Littrup, P.J.; Duric, N.; Sak, M.; Li, C.; Roy, O.; Brem, R.F.; Larsen, L.H.; Yamashita, M. Multicenter Study of Whole Breast Stiffness Imaging by Ultrasound Tomography (SoftVue) for Characterization of Breast Tissues and Masses. J. Clin. Med. 2021, 10, 5528. https://doi.org/10.3390/jcm10235528
Littrup PJ, Duric N, Sak M, Li C, Roy O, Brem RF, Larsen LH, Yamashita M. Multicenter Study of Whole Breast Stiffness Imaging by Ultrasound Tomography (SoftVue) for Characterization of Breast Tissues and Masses. Journal of Clinical Medicine. 2021; 10(23):5528. https://doi.org/10.3390/jcm10235528
Chicago/Turabian StyleLittrup, Peter J., Nebojsa Duric, Mark Sak, Cuiping Li, Olivier Roy, Rachel F. Brem, Linda H. Larsen, and Mary Yamashita. 2021. "Multicenter Study of Whole Breast Stiffness Imaging by Ultrasound Tomography (SoftVue) for Characterization of Breast Tissues and Masses" Journal of Clinical Medicine 10, no. 23: 5528. https://doi.org/10.3390/jcm10235528
APA StyleLittrup, P. J., Duric, N., Sak, M., Li, C., Roy, O., Brem, R. F., Larsen, L. H., & Yamashita, M. (2021). Multicenter Study of Whole Breast Stiffness Imaging by Ultrasound Tomography (SoftVue) for Characterization of Breast Tissues and Masses. Journal of Clinical Medicine, 10(23), 5528. https://doi.org/10.3390/jcm10235528