
Evaluation of the Outcome of Local Surgery for Stomal Prolapse

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Local Repair Procedures for Stomal Prolapse
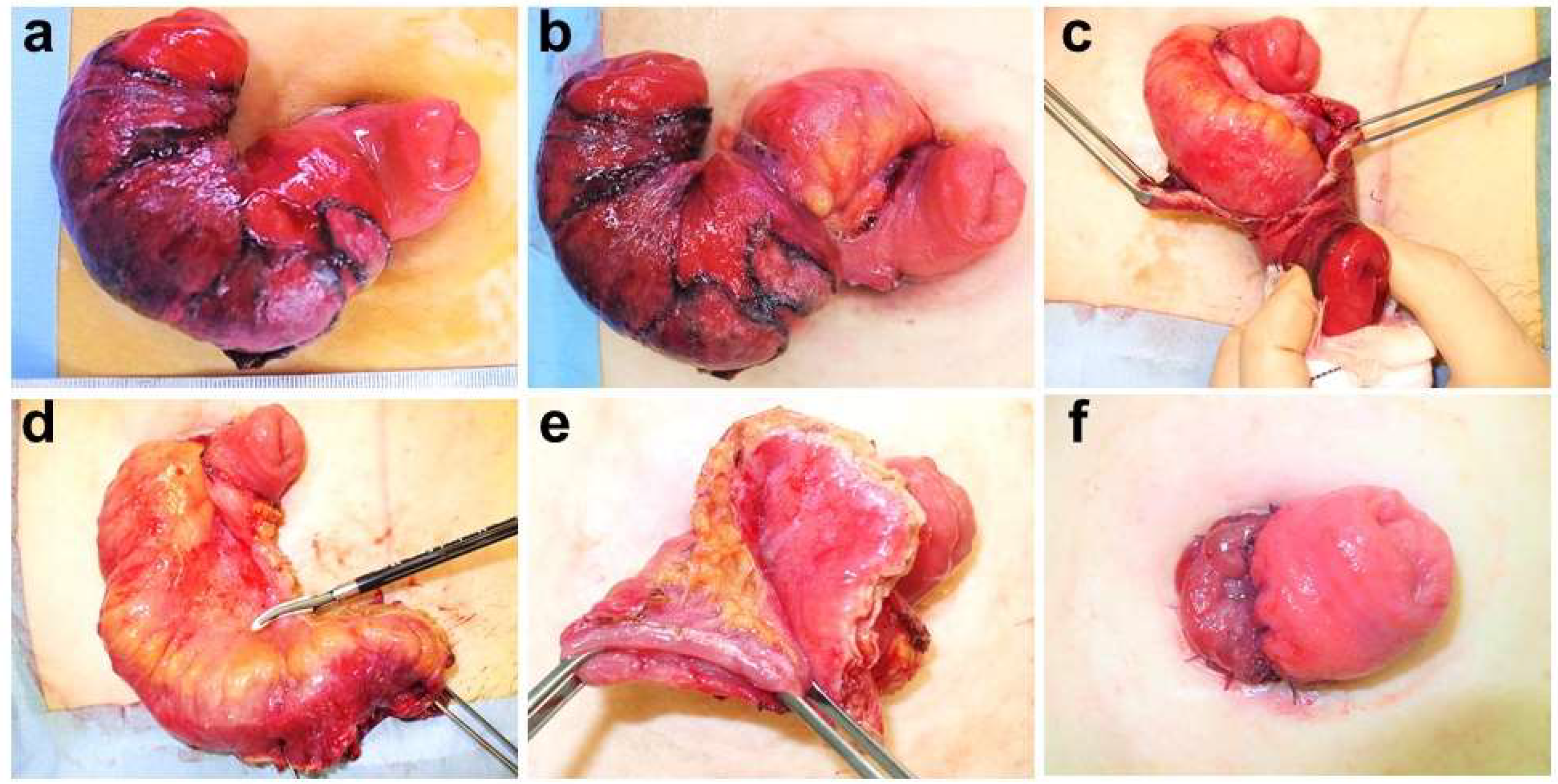
2.3. Local Laparotomic Stomal Reconstruction
2.4. Stapling Repair
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krishnamurty, D.M.; Blatnik, J.; Mutch, M. Stoma Complications. Clin. Colon Rectal Surg. 2017, 30, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Husain, S.G.; Cataldo, T.E. Late Stomal Complications. Clin. Colon Rectal Surg. 2008, 21, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, V.; Bangeas, P.; Xanthopoulou, K.; Paramythiotis, D.; Michalopoulos, A. Stoma prolapse handmade repair under local anesthesia with variation of Altemeier method in severe patients: A case report and review of the literature. J. Surg. Case Rep. 2017, 2, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Murakami, M.; Ozawa, Y.; Uchida, M.; Yamazaki, K.; Fujimori, A.; Otsuka, K.; Aoki, T. The modified Altemeier procedure for a loop colostomy prolapse. Surg. Today 2015, 45, 1463–1466. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Jalouta, T.; Luchtefeld, M.; Ogilvie, J. Surgical management of stomal prolapse—Is there a superior approach to repair? Am. J. Surg. 2020, 220, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Monette, M.M.; Harney, R.T.; Morris, M.S.; Chu, D.I. Local repair of stoma prolapse: Case report of an in vivo application of linear stapler devices. Ann. Med. Surg. 2016, 11, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Maruta, M.; Utsumi, T.; Sato, H.; Aoyama, H.; Katsuno, H.; Hultén, L. Local correction of a transverse loop colostomy prolapse by means of a stapler device. Tech. Coloproctol. 2004, 8, 45–46. [Google Scholar] [CrossRef] [PubMed]
- Hata, F.; Kitagawa, S.; Nishimori, H.; Furuhata, T.; Tsuruma, T.; Ezoe, E.; Ishiyama, G.; Ohno, K.; Fukui, R.; Yanai, Y.; et al. A novel, easy, and safe technique to repair a stoma prolapse using a surgical stapling device. Dig. Surg. 2005, 22, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Tepetes, K.; Spyridakis, M.; Hatzitheofilou, C. Local treatment of a loop colostomy prolapse with a linear stapler. Tech. Coloproctol. 2005, 9, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Masumori, K.; Maeda, K.; Koide, Y.; Hanai, T.; Sato, H.; Matsuoka, H.; Katsuno, H.; Noro, T. Simple excision and closure of a distal limb of loop colostomy prolapse by stapler device. Tech. Coloproctol. 2011, 16, 143–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleres, F.; Saladino, E.; Famulari, C.; Macrì, A. Local repair of a trans-stomal ileocecal prolapse by stapler device. Updat. Surg. 2013, 66, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, H.J.M.; Bhalerao, S. Correction of end colostomy prolapse using a curved surgical stapler, performed under sedation. Tech. Coloproctol. 2010, 14, 165–167. [Google Scholar] [CrossRef] [PubMed]
- Koide, Y.; Maeda, K.; Katsuno, H.; Hanai, T.; Masumori, K.; Matsuoka, H.; Endo, T.; Cheong, Y.C.; Uyama, I. Outcomes of stapler repair with anastomosis for stoma prolapse. Surg. Today 2021, 51, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Masumori, K.; Maeda, K.; Hanai, T.; Sato, H.; Koide, Y.; Matsuoka, H.; Katsuno, H.; Shiota, M. Short-term outcomes of local correction of stoma prolapse with a stapler device. Tech. Coloproctol. 2013, 17, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Abulafi, A.M.; Sherman, I.W.; Fiddian, R.V. Délorme operation for prolapsed colostomy. BJS 2005, 76, 1321–1322. [Google Scholar] [CrossRef] [PubMed]
- Marrosu, A.; Paliogiannis, P.; Sassu, M.A.; Attene, F.; Trignano, M. Correction of an end colostomy prolapse with the Delorme technique. A case report. Ann. Ital. Chir. 2012, 83, 567–569. [Google Scholar] [PubMed]
- Kim, J.T.; Kumar, R.R. Reoperation for Stoma-Related Complications. Clin. Colon Rectal Surg. 2006, 19, 207–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osborne, W.; North, J.; Williams, J. Using a risk assessment tool for parastomal hernia prevention. Br. J. Nurs. 2018, 27, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | All Patients (n = 15) |
|---|---|
| Age (years) | 79 (51–92) |
| Sex | |
| Male | 9 (60%) |
| Female | 6 (40%) |
| Body mass index | 22.3 (14–27.8) |
| Urgency of previous operation for stoma construction | |
| Elective | 9 (60%) |
| Emergency | 6 (40%) |
| Type of stoma | |
| Loop ileostomy | 3 (20%) |
| Loop colostomy | 8 (53.3%) |
| End colostomy | 3 (20%) |
| Double-barreled stoma of ileum and colon | 1 (6.7%) |
| Prolapse side of loop or double-barreled stoma | |
| Oral | 6 (50%) |
| Anal | 5 (41.7%) |
| Both | 1 (8.3%) |
| Prolapse intestine (including a both-side case) | |
| Colon | 13 (81.3%) |
| Ileum | 3 (8.7%) |
| Length of stoma prolapse (cm) | 14.5 (5–20) |
| Duration until prolapse (days) | 103 (7–1854) |
| Anesthesia used | |
| General | 14 (93.3%) |
| Epidural + spinal | 1 (6.7%) |
| Observation period after reconstruction (days) | 193 (11–2069) |
| No. | Length of Stoma Prolapse (cm) | Prolapse Intestine | Anesthesia | Surgical Methods | Operation Time (min) | Blood Loss | Length of Hospital Stay (Days) | Postoperative Complications |
|---|---|---|---|---|---|---|---|---|
| 1 | 20 | Ileum | General | LLSR | 55 | 850 mL | 33 | None |
| 2 | 14 | Colon | General | SR | 20 | A little | 6 | Parastomal hernia |
| 3 | 12 | Colon | General | SR | 67 | 10 mL | 5 | None |
| 4 | 20 | Ileum | General | LLSR | 35 | A little | 8 | Parastomal hernia |
| 5 | 10 | Colon | General | LLSR | 61 | A little | 14 | None |
| 6 | 10 | Colon | General | LLSR | 60 | A little | 10 | None |
| 7 | 18 | Colon | General | LLSR | 46 | A little | 8 | None |
| 8 | 8 | Colon | General | LLSR | 70 | A little | 7 | None |
| 9 | 15 | Ileum | General | LLSR | 58 | A little | 6 | None |
| 10 | 15 | Colon | General | SR | 20 | A little | 8 | None |
| 11 | 16 | Colon | General | SR | 15 | A little | 5 | None |
| 12 | 5 | Colon | General | SR | 15 | A little | 2 | None |
| 13 | Unknown | Colon | Epidural + spinal | SR→LLSR | 50 | 5 mL | 10 | None |
| 14 | Unknown | Colon | General | SR | 31 | 5 mL | 18 | None |
| 15 | Unknown | Colon | General | LLSR | 30 | A little | 8 | None |
| LLSR (n = 9) | SR (n = 6) | p-Value | |
|---|---|---|---|
| Operation time (min) | 53 (30–70) | 20 (15–67) | 0.036 |
| Blood loss (mL) | A little (A little-850 mL) | A little (A little-10 mL) | 0.776 |
| Length of hospital stay (days) | 8 (6–33) | 5.5 (2–18) | 0.088 |
| Number of staplers used | - | 4 (2–9) | |
| Complications | |||
| Early | None | None | |
| Late | Parastomal hernia 1 | Parastomal hernia 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosuge, M.; Ohkuma, M.; Koyama, M.; Kobayashi, Y.; Nakano, T.; Takano, Y.; Shimoyama, Y.; Takada, N.; Kumamoto, T.; Imaizumi, Y.; et al. Evaluation of the Outcome of Local Surgery for Stomal Prolapse. J. Clin. Med. 2021, 10, 5438. https://doi.org/10.3390/jcm10225438
Kosuge M, Ohkuma M, Koyama M, Kobayashi Y, Nakano T, Takano Y, Shimoyama Y, Takada N, Kumamoto T, Imaizumi Y, et al. Evaluation of the Outcome of Local Surgery for Stomal Prolapse. Journal of Clinical Medicine. 2021; 10(22):5438. https://doi.org/10.3390/jcm10225438
Chicago/Turabian StyleKosuge, Makoto, Masahisa Ohkuma, Muneyuki Koyama, Yasunobu Kobayashi, Takafumi Nakano, Yasuhiro Takano, Yuya Shimoyama, Naoki Takada, Tomotaka Kumamoto, Yuta Imaizumi, and et al. 2021. "Evaluation of the Outcome of Local Surgery for Stomal Prolapse" Journal of Clinical Medicine 10, no. 22: 5438. https://doi.org/10.3390/jcm10225438
APA StyleKosuge, M., Ohkuma, M., Koyama, M., Kobayashi, Y., Nakano, T., Takano, Y., Shimoyama, Y., Takada, N., Kumamoto, T., Imaizumi, Y., Sugano, H., Eto, S., Takeda, Y., Yatabe, S., & Eto, K. (2021). Evaluation of the Outcome of Local Surgery for Stomal Prolapse. Journal of Clinical Medicine, 10(22), 5438. https://doi.org/10.3390/jcm10225438