
Rapid Ventricular Pacing as a Safe Procedure for Clipping of Complex Ruptured and Unruptured Intracranial Aneurysms

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
Anesthesia Management
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, R.D.; Broderick, J.P. Unruptured intracranial aneurysms: Epidemiology, natural history, management options, and familial screening. Lancet Neurol. 2014, 13, 393–404. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.; Yu, L.-M.; Clarke, M.; Sneade, M.; A Yarnold, J.; Sandercock, P. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Spetzler, R.F.; McDougall, C.G.; Zabramski, J.M.; Albuquerque, F.C.; Hills, N.K.; Russin, J.J.; Partovi, S.; Nakaji, P.; Wallace, R.C. The Barrow Ruptured Aneurysm Trial: 6-year results. J. Neurosurg. 2015, 123, 609–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darsaut, T.E.; Darsaut, N.M.; Chang, S.D.; Silverberg, G.D.; Shuer, L.M.; Tian, L.; Dodd, R.L.; Do, H.M.; Marks, M.P.; Steinberg, G.K. Predictors of Clinical and Angiographic Outcome After Surgical or Endovascular Therapy of Very Large and Giant Intracranial Aneurysms. Neurosurgery 2011, 68, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.C.; Wilson, C.B.; Halbach, V.V.; Higashida, R.T.; Dowd, C.F.; McDermott, M.W.; Applebury, C.B.; Farley, T.L.; Gress, D.R. Endovascular and surgical treatment of unruptured cerebral aneurysms: Comparison of risks. Ann Neurol. 2000, 48, 11–19. [Google Scholar] [CrossRef]
- Bendok, B.R.; Gupta, D.K.; Rahme, R.J.; Eddleman, C.S.; Adel, J.G.; Sherma, A.K.; Surdell, D.L.; Bebawy, J.F.; Koht, A.; Batjer, H.H. Adenosine for Temporary Flow Arrest During Intracranial Aneurysm Surgery: A Single-Center Retrospective Review. Neurosurgery 2011, 69, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Kalani, M.Y.S.; Ramey, W.; Albuquerque, F.C.; McDougall, C.G.; Nakaji, P.; Zabramski, J.M.; Spetzler, R.F. Revascularization and aneurysm surgery: Techniques, indications, and outcomes in the endovascular era. Neurosurgery 2014, 74, 482–498. [Google Scholar] [CrossRef] [PubMed]
- Waqas, M.; Dossani, R.H.; Vakharia, K.; Rai, H.H.; Chin, F.; Tso, M.K.; Rajah, G.B.; Snyder, K.V.; Davies, J.M.; Levy, E.I.; et al. Complete flow control using transient concurrent rapid ventricular pacing or intravenous adenosine and afferent arterial balloon occlusion during transvenous embolization of cerebral arteriovenous malformations: Case series. J. Neuroint. Surg. 2021, 13, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Berger, M.; Agrawal, A.; Huang, M.; Karikari, I.; Nimjee, S.; Zomorodi, A.R.; McDonagh, D.L. Rapid ventricular pacing assisted hypotension in the management of sudden intraoperative hemorrhage during cerebral aneurysm clipping. Asian J. Neurosurg. 2014, 9, 33–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nimjee, S.; Smith, T.P.; Kanter, R.J.; Ames, W.; Machovec, K.A.; Grant, G.A.; Zomorodi, A.R. Rapid ventricular pacing for a basilar artery pseudoaneurysm in a pediatric patient: Case report. J. Neurosurgery: Pediatry 2015, 15, 625–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saldien, V.; Menovsky, T.; Rommens, M.; Van Der Steen, G.; Van Loock, K.; Vermeersch, G.; Mott, C.; Bosmans, J.; De Ridder, D.; Maas, A.I. Rapid Ventricular Pacing for Flow Arrest During Cerebrovascular Surgery: Revival of an Old Concept. Oper. Neurosurg. 2011, 70, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, J.R.; Payne, R.; Rodriguez-Diaz, C.; Ellegala, D.B.; Reeves, S.T. Rapid ventricular pacing: A novel technique to decrease cardiac output for giant basilar aneurysm surgery. J. Clin. Anesthesia 2012, 24, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Konczalla, J.; Platz, J.; Fichtlscherer, S.; Mutlak, H.; Strouhal, U.; Seifert, V. Rapid ventricular pacing for clip reconstruction of complex unruptured intracranial aneurysms: Results of an interdisciplinary prospective trial. J. Neurosurg. 2018, 128, 1741–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnider, T.W.; Minto, C.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Shafer, S.; Youngs, E.J. The Influence of Method of Administration and Covariates on the Pharmacokinetics of Propofol in Adult Volunteers. Anesthesiology 1998, 88, 1170–1182. [Google Scholar] [CrossRef] [PubMed]
- Koch, F.; Thompson, J.; Chung, R.S. Giant cerebral aneurysm repair. Incorporating cardiopulmonary bypass and neurosurgery. AORN J. 1991, 54, 224–241. [Google Scholar] [CrossRef]
- Meling, T.R.; Lavé, A. What are the options for cardiac standstill during aneurysm surgery? A systematic review. Neurosurg. Rev. 2019, 42, 843–852. [Google Scholar] [CrossRef]
- Sollevi, A.; Lagerkranser, M.; Irestedt, L.; Gordon, E.; Lindquist, C. Controlled Hypotension with Adenosine in Cerebral Aneurysm Surgery. Anesthesiology 1984, 61, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Rovit, R.L. Operative hypotension for intracranial vascular surgery using pacemaker-induced ventricular tachycardia. J. Neurosurg. 1971, 35, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Kahn, R.A.; Marin, M.L.; Hollier, L.; Parsons, R.; Griepp, R. Induction of Ventricular Fibrillation to Facilitate Endovascular Stent Graft Repair of Thoracic Aortic Aneurysms. Anesthesiology 1998, 88, 534–536. [Google Scholar] [CrossRef] [PubMed]
- Biso, S.; Wongrakpanich, S.; Agrawal, A.; Yadlapati, S.; Kishlyansky, M.; Figueredo, V. A Review of Neurogenic Stunned Myocardium. Cardiovasc. Psychiatry Neurol. 2017, 2017, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| uIA Group | rIA Group | p Value | |
|---|---|---|---|
| number | 9 | 8 | |
| mean age | 49.2 ± 4.92 | 56.1 ± 4.03 | 0.29 |
| sex | 0.99 | ||
| male | 3 | 2 | |
| female | 6 | 6 | |
| mean BMI | 25.8 ± 1.96 | 28.7 ± 2.45 | 0.37 |
| arterial hypertension | 2 | 3 | 0.62 |
| uIA | ||||
|---|---|---|---|---|
| Location | Size (mm) | Hunt & Hess | Fisher | Procedure Related Complications |
| ICA-Pcom | 26 | n.a. | n.a. | None |
| MCA bifurcation | 18 | n.a. | n.a. | None |
| Acom | 6 | n.a. | n.a. | None |
| ICA-Pcom | 16 | n.a. | n.a. | None |
| ICA-bifurcation | 20 | n.a. | n.a. | None |
| Paraclinoid ICA | 19 | n.a. | n.a. | None |
| Paraclinoid ICA | 22 | n.a. | n.a. | None |
| MCA | 8 | n.a. | n.a. | None |
| Paraclinoid ICA | 22 | n.a. | n.a. | None |
| rIA | ||||
| Location | Size (mm) | Hunt & Hess | Fisher | Procedure Related Complications |
| ICA backwall | 25 | 5 | 3 | Ventricular fibrillation |
| MCA | 40 | 3 | 3 | None |
| ICA-Pcom | 27 | 4 | 3 | None |
| AICA | 6 | 2 | 3 | None |
| Paraclinoid ICA | 21 | 2 | 3 | None |
| ICA-PCom | 15 | 5 | 3 | None |
| Paraclinoid ICA | 11 | 1 | 1 | None |
| MCA bifurcation | 35 | 1 | 4 | None |
| uIA Group | rIA Group | p Value | |
|---|---|---|---|
| aneurysm size | 16.7 ± 2.13 | 22.5 ± 4.12 | 0.24 |
| aneurysm location | 0.62 | ||
| anterior circulation | 7 | 5 | |
| posterior circulation | 2 | 3 | |
| Hunt & Hess grade | 2.9 (1–5) | ||
| Fisher grade | 2.9 (1–4) |
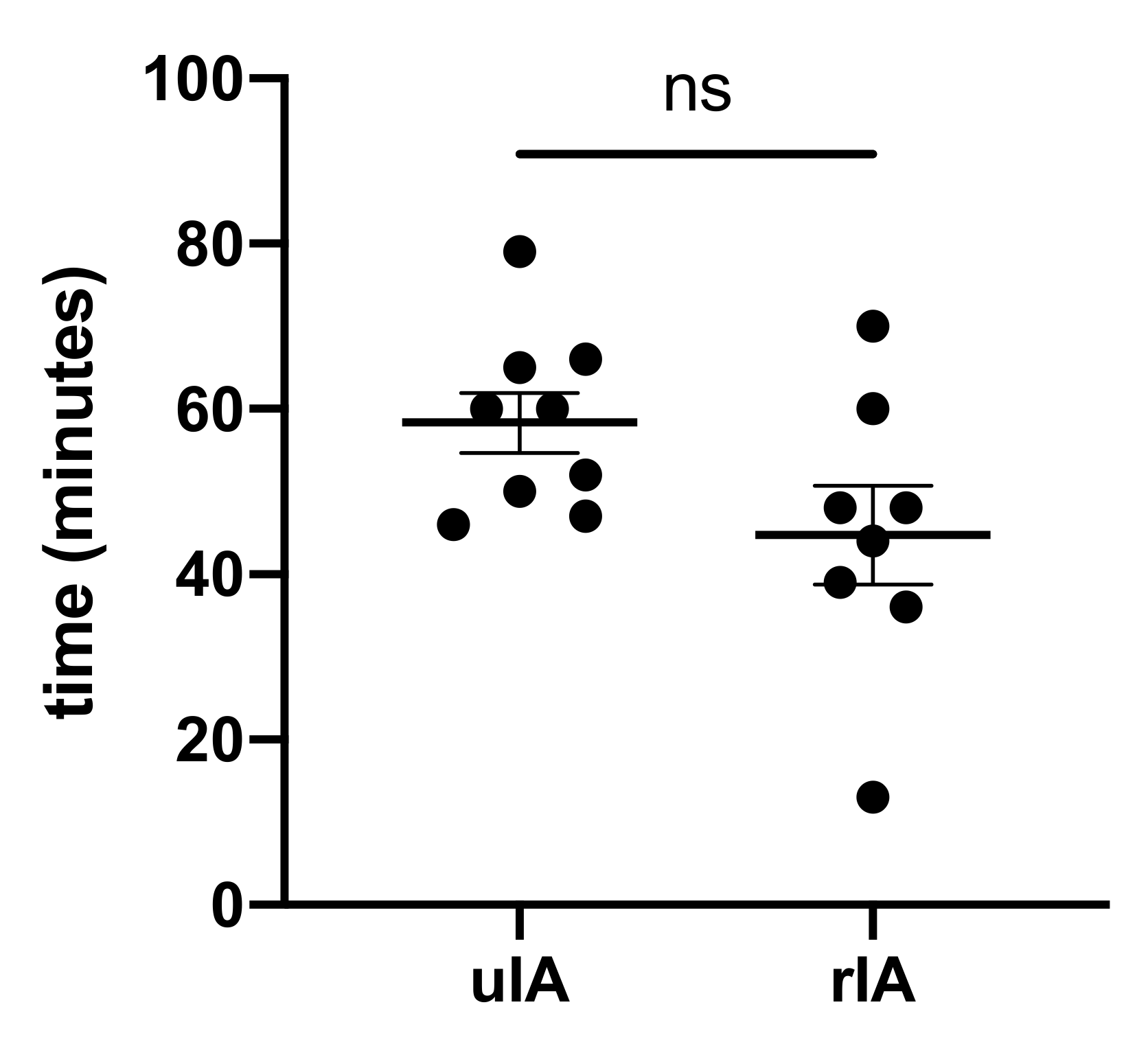
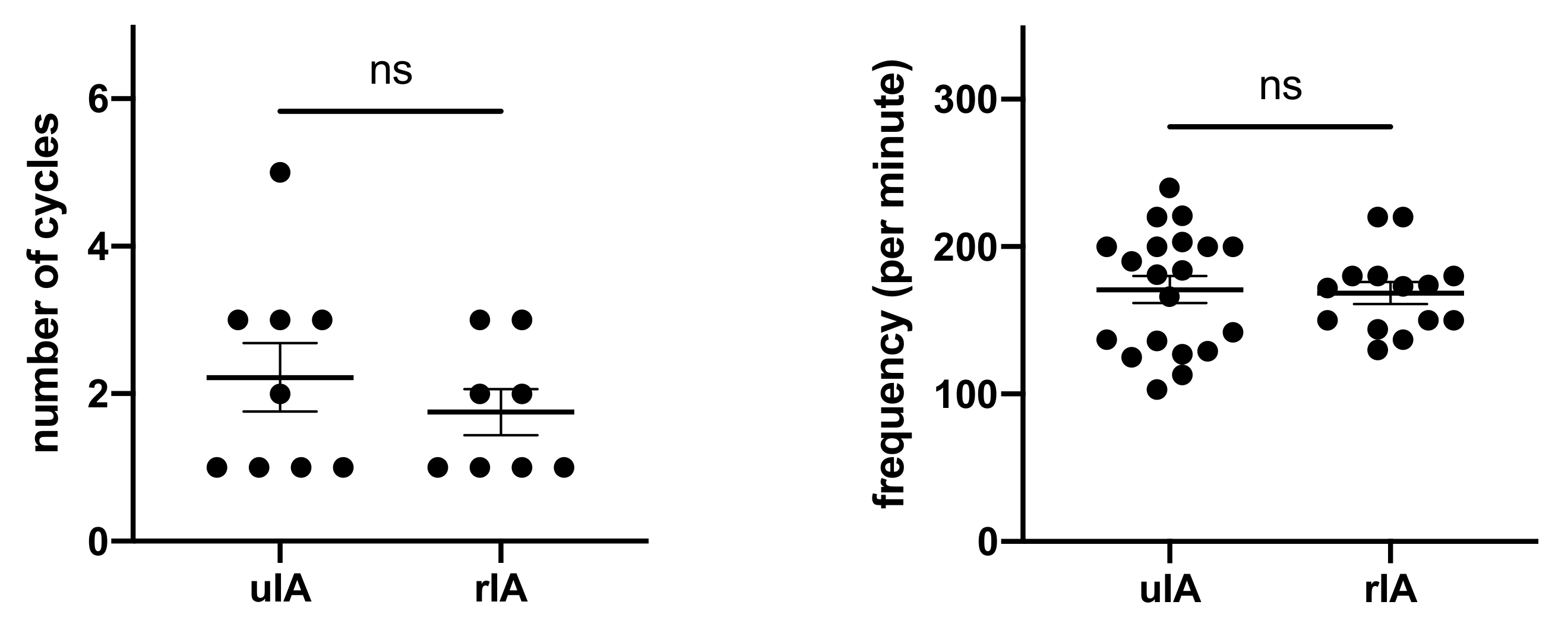
| uIA Group | rIA Group | p Value | |
|---|---|---|---|
| RVP cycles | 2.2 | 1.8 | 0.41 |
| RVP frequency | 170.9 ± 9.1 | 168.6 ± 7.4 | 0.85 |
| MAP before RVP | 76.8 ± 1.2 | 64.5 ± 4.1 | 0.0119 |
| MAP during RVP | 53.0 ± 3.5 | 41.0 ± 2.2 | 0.0071 |
| MAP after RVP | 73.9 ± 2.3 | 57.4 ± 3.1 | 0.0002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grabert, J.; Huber-Petersen, S.; Lampmann, T.; Eichhorn, L.; Vatter, H.; Coburn, M.; Velten, M.; Güresir, E. Rapid Ventricular Pacing as a Safe Procedure for Clipping of Complex Ruptured and Unruptured Intracranial Aneurysms. J. Clin. Med. 2021, 10, 5406. https://doi.org/10.3390/jcm10225406
Grabert J, Huber-Petersen S, Lampmann T, Eichhorn L, Vatter H, Coburn M, Velten M, Güresir E. Rapid Ventricular Pacing as a Safe Procedure for Clipping of Complex Ruptured and Unruptured Intracranial Aneurysms. Journal of Clinical Medicine. 2021; 10(22):5406. https://doi.org/10.3390/jcm10225406
Chicago/Turabian StyleGrabert, Josefin, Stefanie Huber-Petersen, Tim Lampmann, Lars Eichhorn, Hartmut Vatter, Mark Coburn, Markus Velten, and Erdem Güresir. 2021. "Rapid Ventricular Pacing as a Safe Procedure for Clipping of Complex Ruptured and Unruptured Intracranial Aneurysms" Journal of Clinical Medicine 10, no. 22: 5406. https://doi.org/10.3390/jcm10225406
APA StyleGrabert, J., Huber-Petersen, S., Lampmann, T., Eichhorn, L., Vatter, H., Coburn, M., Velten, M., & Güresir, E. (2021). Rapid Ventricular Pacing as a Safe Procedure for Clipping of Complex Ruptured and Unruptured Intracranial Aneurysms. Journal of Clinical Medicine, 10(22), 5406. https://doi.org/10.3390/jcm10225406