Association between Serum Lipid Parameters and Cognitive Performance in Older Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurement of Serum Lipids Profiles
2.3. Measurement of DSST
2.4. Variables of Interest
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
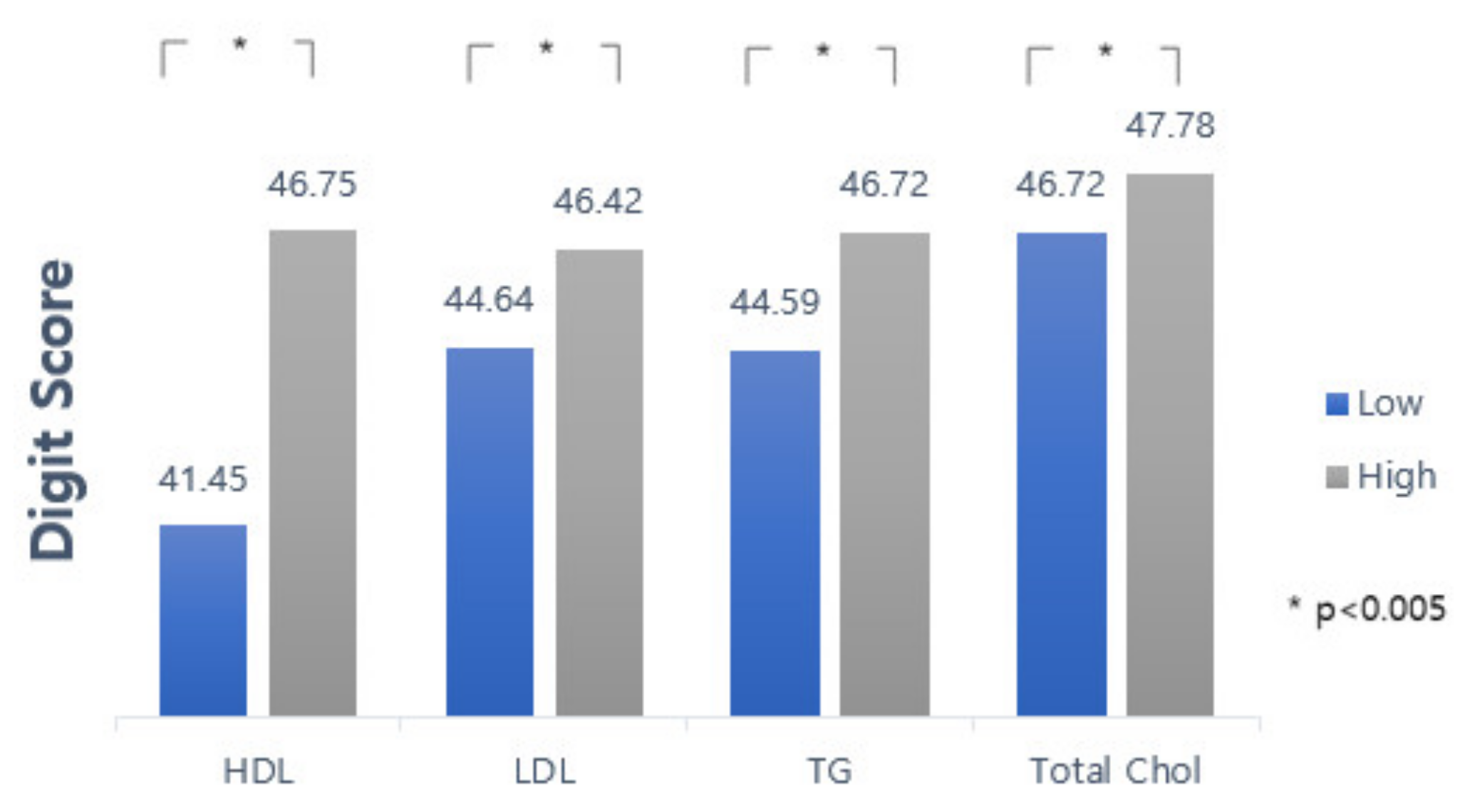
3.2. Comparison of the Means (SD) of Lipid Profiles and Cognitive Test Score
3.3. Pearson Correlation Structure of Lipid Profiles-DSST and among Lipid Profiles
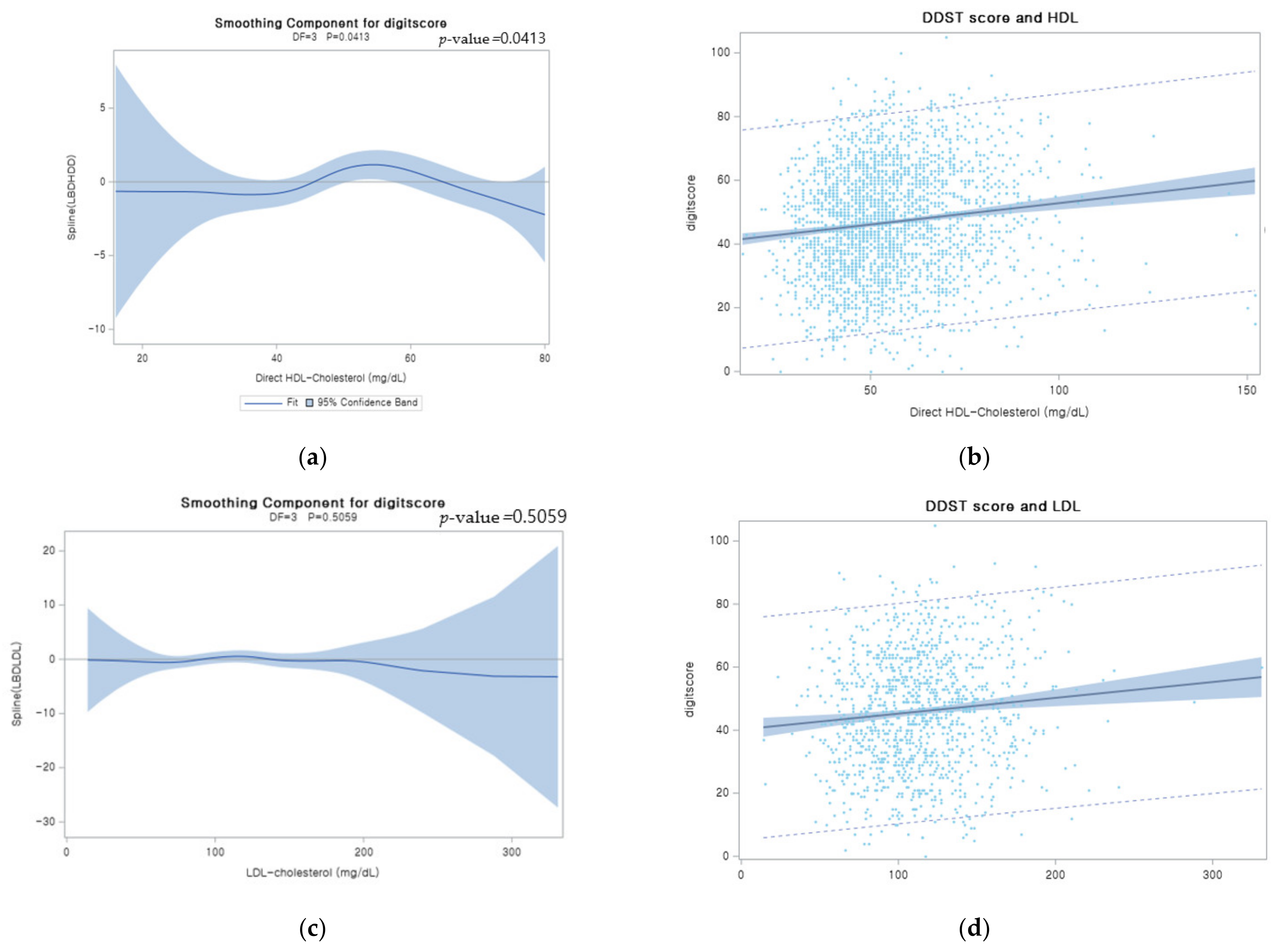
3.4. Multiple Linear Regression and Logistic Regression Analysis of the Association between Lipid Profiles and DSST
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodriguez, J.J.L.; Ferri, C.P.; Acosta, D.; Guerra, M.; Huang, Y.; Jacob, K.S.; Krishnamoorthy, E.S.; Salas, A.; Sosa, A.L.; Acosta, I.; et al. Prevalence of dementia in Latin America, India, and China: A population-based cross-sectional survey. Lancet 2008, 372, 464–474. [Google Scholar] [CrossRef] [Green Version]
- Majer, R.; Adeyi, O.; Bagoly, Z.; Simon, V.; Csiba, L.; Kardos, L.; Hortobágyi, T.; Frecska, E. Neuropsychiatric symptoms, quality of life and caregivers’ burden in dementia. Open Med. (Wars) 2020, 15, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2020 Alzheimer’s disease facts and figures. Alzheimers Dement. 2020, 16, 391–460. [Google Scholar] [CrossRef] [PubMed]
- Heun, R.; Schoepf, D.; Potluri, R.; Natalwala, A. Alzheimer’s disease and co-morbidity: Increased prevalence and possible risk factors of excess mortality in a naturalistic 7-year follow-up. Eur. Psychiatry 2013, 28, 40–48. [Google Scholar] [CrossRef]
- Yao, S.; Liu, Y.; Zheng, X.; Zhang, Y.; Cui, S.; Tang, C.; Lu, L.; Xu, N. Do nonpharmacological interventions prevent cognitive decline? a systematic review and meta-analysis. Transl. Psychiatry 2020, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Cicconetti, P.; Riolo, N.; Priami, C.; Tafaro, L.; Ettore, E. Risk factors for cognitive impairment. Recenti Prog. Med. 2004, 95, 535–545. [Google Scholar]
- Zhou, H.; Deng, J.; Li, J.; Wang, Y.; Zhang, M.; He, H. Study of the relationship between cigarette smoking, alcohol drinking and cognitive impairment among elderly people in China. Age Ageing 2003, 32, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Knopman, D.; Boland, L.L.; Mosley, T.; Howard, G.; Liao, D.; Szklo, M.; McGovern, P.; Folsom, A.R. Cardiovascular risk factors and cognitive decline in middle-aged adults. Neurology 2001, 56, 42–48. [Google Scholar] [CrossRef]
- Ortega, R.M.; Requejo, A.M.; Andrés, P.; López-Sobaler, A.M.; Quintas, M.E.; Redondo, M.R.; Navia, B.; Rivas, T. Dietary intake and cognitive function in a group of elderly people. Am. J. Clin. Nutr. 1997, 66, 803–809. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Li, Q.; Zhao, J.; Wu, T.; Ji, L.; Huang, G.; Ma, F. Relationship between plasma lipids and mild cognitive impairment in the elderly Chinese: A case-control study. Lipids Health Dis. 2016, 15, 146. [Google Scholar] [CrossRef] [Green Version]
- Crichton, G.E.; Elias, M.F.; Davey, A.; Sullivan, K.J.; Robbins, M.A. Higher HDL cholesterol is associated with better cognitive function: The Maine-Syracuse study. J. Int. Neuropsychol. Soc. 2014, 20, 961–970. [Google Scholar] [CrossRef] [Green Version]
- Elias, P.K.; Elias, M.F.; D’Agostino, R.B.; Sullivan, L.M.; Wolf, P.A. Serum cholesterol and cognitive performance in the Framingham Heart Study. Psychosom. Med. 2005, 67, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Shang, S.; Li, P.; Chen, C.; Dang, L.; Jiang, Y.; Wang, J.; Huo, K.; Deng, M.; Wang, J.; et al. The gender- and age- dependent relationships between serum lipids and cognitive impairment: A cross-sectional study in a rural area of Xi’an, China. Lipids Health Dis. 2019, 18, 4. [Google Scholar] [CrossRef] [Green Version]
- Mefford, M.T.; Chen, L.; Lewis, C.E.; Muntner, P.; Sidney, S.; Launer, L.J.; Monda, K.L.; Ruzza, A.; Kassahun, H.; Rosenson, R.S.; et al. Long-Term Levels of LDL-C and Cognitive Function: The CARDIA Study. J. Int. Neuropsychol. Soc. 2021, 27, 1–10. [Google Scholar] [CrossRef]
- Baune, B.T.; Brignone, M.; Larsen, K.G. A Network Meta-Analysis Comparing Effects of Various Antidepressant Classes on the Digit Symbol Substitution Test (DSST) as a Measure of Cognitive Dysfunction in Patients with Major Depressive Disorder. Int. J. Neuropsychopharmacol. 2018, 21, 97–107. [Google Scholar] [CrossRef] [Green Version]
- National Health and Nutrition Examination Survey Home Page. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/TCHOL_G.htm (accessed on 24 August 2021).
- National Health and Nutrition Examination Survey Home Page. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/HDL_G.htm (accessed on 24 August 2021).
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Kardiol. Pol. 2016, 74, 821–936. [Google Scholar] [CrossRef] [Green Version]
- Group, U.H.-C.C. Role of fibrates in reducing coronary risk: A UK Consensus. Curr. Med. Res. Opin. 2004, 20, 241–247. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/CFQ_G.htm) (accessed on 24 August 2021).
- Bates, K.A.; Sohrabi, H.R.; Rainey-Smith, S.R.; Weinborn, M.; Bucks, R.S.; Rodrigues, M.; Beilby, J.; Howard, M.; Taddei, K.; Martins, G.; et al. Serum high-density lipoprotein is associated with better cognitive function in a cross-sectional study of aging women. Int. J. Neurosci. 2017, 127, 243–252. [Google Scholar] [CrossRef]
- Pancani, S.; Sofi, F.; Cecchi, F.; Macchi, C. HDL Cholesterol Is Independently Associated with Cognitive Function in Males But Not in Females within a Cohort of Nonagenarians: The MUGELLO Study. J. Nutr. Health Aging 2019, 23, 552–557. [Google Scholar] [CrossRef]
- Ma, C.; Yin, Z.; Zhu, P.; Luo, J.; Shi, X.; Gao, X. Blood cholesterol in late-life and cognitive decline: A longitudinal study of the Chinese elderly. Mol. Neurodegener. 2017, 12, 24. [Google Scholar] [CrossRef] [Green Version]
- Muldoon, M.F.; Ryan, C.M.; Sheu, L.; Yao, J.K.; Conklin, S.M.; Manuck, S.B. Serum phospholipid docosahexaenonic acid is associated with cognitive functioning during middle adulthood. J. Nutr. 2010, 140, 848–853. [Google Scholar] [CrossRef]
- Muldoon, M.F.; Ryan, C.M.; Yao, J.K.; Conklin, S.M.; Manuck, S.B. Long-chain omega-3 fatty acids and optimization of cognitive performance. Mil. Med. 2014, 179, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.Q.; Dong, B.R.; Wu, H.M.; Zhang, Y.L.; Wu, J.H.; Lu, Z.C.; Flaherty, J.H. Association of cognitive impairment with serum lipid/lipoprotein among Chinese nonagenarians and centenarians. Dement. Geriatr. Cogn. Disord. 2009, 27, 111–116. [Google Scholar] [CrossRef]
- Reitz, C.; Luchsinger, J.; Tang, M.X.; Manly, J.; Mayeux, R. Impact of plasma lipids and time on memory performance in healthy elderly without dementia. Neurology 2005, 64, 1378–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparks, D.L.; Schreurs, B.G. Trace amounts of copper in water induce beta-amyloid plaques and learning deficits in a rabbit model of Alzheimer’s disease. Proc. Natl. Acad. Sci. USA 2003, 100, 11065–11069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreurs, B.G.; Smith-Bell, C.A.; Darwish, D.S.; Stankovic, G.; Sparks, D.L. Classical conditioning of the rabbit’s nictitating membrane response is a function of the duration of dietary cholesterol. Nutr. Neurosci. 2007, 10, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Wolf, H.; Hensel, A.; Arendt, T.; Kivipelto, M.; Winblad, B.; Gertz, H.J. Serum lipids and hippocampal volume: The link to Alzheimer’s disease? Ann. Neurol. 2004, 56, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.V.; Cuchel, M.; de la Llera-Moya, M.; Rodrigues, A.; Burke, M.F.; Jafri, K.; French, B.C.; Phillips, J.A.; Mucksavage, M.L.; Wilensky, R.L.; et al. Cholesterol efflux capacity, high-density lipoprotein function, and atherosclerosis. N. Engl. J. Med. 2011, 364, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Mauch, D.H.; Nägler, K.; Schumacher, S.; Göritz, C.; Müller, E.C.; Otto, A.; Pfrieger, F.W. CNS synaptogenesis promoted by glia-derived cholesterol. Science 2001, 294, 1354–1357. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Gimeno, D.; Kivimaki, M.; Brunner, E.; Marmot, M.G. Low HDL cholesterol is a risk factor for deficit and decline in memory in midlife: The Whitehall II study. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1556–1562. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.A.; Bendlin, B.B.; McLaren, D.G.; Hess, T.M.; Gallagher, C.L.; Kastman, E.K.; Rowley, H.A.; Asthana, S.; Carlsson, C.M.; Sager, M.A.; et al. Low HDL Cholesterol is Associated with Lower Gray Matter Volume in Cognitively Healthy Adults. Front. Aging Neurosci. 2010, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variables | Mean (SD) or n (%) |
|---|---|
| Age (y) | 68.96 ± 6.65 |
| Sex | |
| Male | 47.27 (%) |
| Female | 52.73 (%) |
| Race/Ethnicity | |
| Mexican American | 9.16 (%) |
| White | 47.22 (%) |
| Black | 23.34 (%) |
| Asian | 8.26 (%) |
| Other Race | 12.01 (%) |
| Income | |
| Low | 24.24 (%) |
| High | 75.76 (%) |
| Education | |
| Non High School Grad | 23.79 (%) |
| High School Grad | 23.02 (%) |
| College Grad or above | 53.18 (%) |
| Smoking | |
| Non experience at all | 12.33 (%) |
| Experienced at the past | 36.30 (%) |
| Current Smoking | 51.38 (%) |
| Exercise | |
| Non | 40.27 (%) |
| Regularly | 59.73 (%) |
| BMI (kg/m2) | |
| Underweight | 1.58 (%) |
| Normal | 26.95 (%) |
| Overweight | 36.03 (%) |
| Obesity | 37.02 (%) |
| Depressive feeling | |
| Yes | 22.84 (%) |
| No | 77.16 (%) |
| Diabetes | |
| Yes | 4.56 (%) |
| No | 95.44 (%) |
| Chestpain | |
| Yes | 20.90 (%) |
| No | 79.10 (%) |
| Hypertension | |
| Yes | 35.25 (%) |
| No | 64.75 (%) |
| Statin | |
| Yes | 37.79 (%) |
| No | 62.21 (%) |
| Mean | SD | |
|---|---|---|
| Lipid profiles | ||
| HDL | 55.11 | 16.27 |
| LDL | 113.05 | 35.35 |
| TG | 120.89 | 70.9 |
| Total Chol | 194.61 | 42.63 |
| Cognitive Test | ||
| DSST | 47.27 | 17.33 |
| DSST | |||
|---|---|---|---|
| No. | R | p-Value | |
| HDL | 2215 | 0.127 | <0.0001 |
| LDL | 1078 | 0.107 | 0.0005 |
| TG | 1088 | 0.019 | 0.5372 |
| Total Chol | 2215 | 0.111 | <0.0001 |
| Lipid Profiles | |||
| No. | R | p-value | |
| HDL-LDL | 1078 | 0.079 | 0.0039 |
| HDL-TG | 1088 | −0.419 | <0.0001 |
| HDL-Total Chol | 2215 | 0.288 | <0.0001 |
| LDL-TG | 1078 | 0.089 | 0.0012 |
| LDL-Total Chol | 1078 | 0.925 | <0.0001 |
| TG-Total Chol | 1088 | 0.111 | <0.0001 |
| DSST | Beta Cofficient (SE) | p-Value | DSST (Low/High) | Odds Ratio (95% Confidence Limits) | p-Value |
|---|---|---|---|---|---|
| HDL | 0.036 (0.018) | 0.0447 | 0.994 (0.986–1.002) | 0.1506 | |
| LDL | 0.018 (0.011) | 0.1166 | 0.998 (0.993–1.004) | 0.5631 | |
| TG | 0.003 (0.005) | 0.5689 | 1.000 (0.998–1.002) | 0.9897 | |
| Total Chol | 0.013 (0.007) | 0.0514 | 0.997 (0.994–1.000) | 0.0852 | |
| Categorization of Lipid Profiles | |||||
| High | 3.113 (0.647) | <0.0001 | 0.701 (0.523–0.938) | 0.0167 | |
| Low | |||||
| High | |||||
| Low | −0.837 (0.925) | 0.3658 | 1.420 (0.946–2.131) | 0.0911 | |
| High | |||||
| Low | −1.837 (0.920) | 0.0461 | 1.194 (0.798–1.788) | 0.3888 | |
| High | |||||
| Low | −0.468 (0.574) | 0.4151 | 1.131 (0.875–1.462) | 0.3457 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Lee, S.; Min, J.-y.; Min, K.-b. Association between Serum Lipid Parameters and Cognitive Performance in Older Adults. J. Clin. Med. 2021, 10, 5405. https://doi.org/10.3390/jcm10225405
Lee J, Lee S, Min J-y, Min K-b. Association between Serum Lipid Parameters and Cognitive Performance in Older Adults. Journal of Clinical Medicine. 2021; 10(22):5405. https://doi.org/10.3390/jcm10225405
Chicago/Turabian StyleLee, Jaeho, Sohyae Lee, Jin-young Min, and Kyoung-bok Min. 2021. "Association between Serum Lipid Parameters and Cognitive Performance in Older Adults" Journal of Clinical Medicine 10, no. 22: 5405. https://doi.org/10.3390/jcm10225405
APA StyleLee, J., Lee, S., Min, J.-y., & Min, K.-b. (2021). Association between Serum Lipid Parameters and Cognitive Performance in Older Adults. Journal of Clinical Medicine, 10(22), 5405. https://doi.org/10.3390/jcm10225405