
Clinical Significance and Prognostic Value of Hemostasis Parameters in 337 Patients with Acute Infective Endocarditis



 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Laboratory Assays
2.4. Statistical Analysis
3. Results
3.1. Clinical Features and Coagulation Parameters of the Study Population
3.2. Hemostasis Parameters and IE Mortality
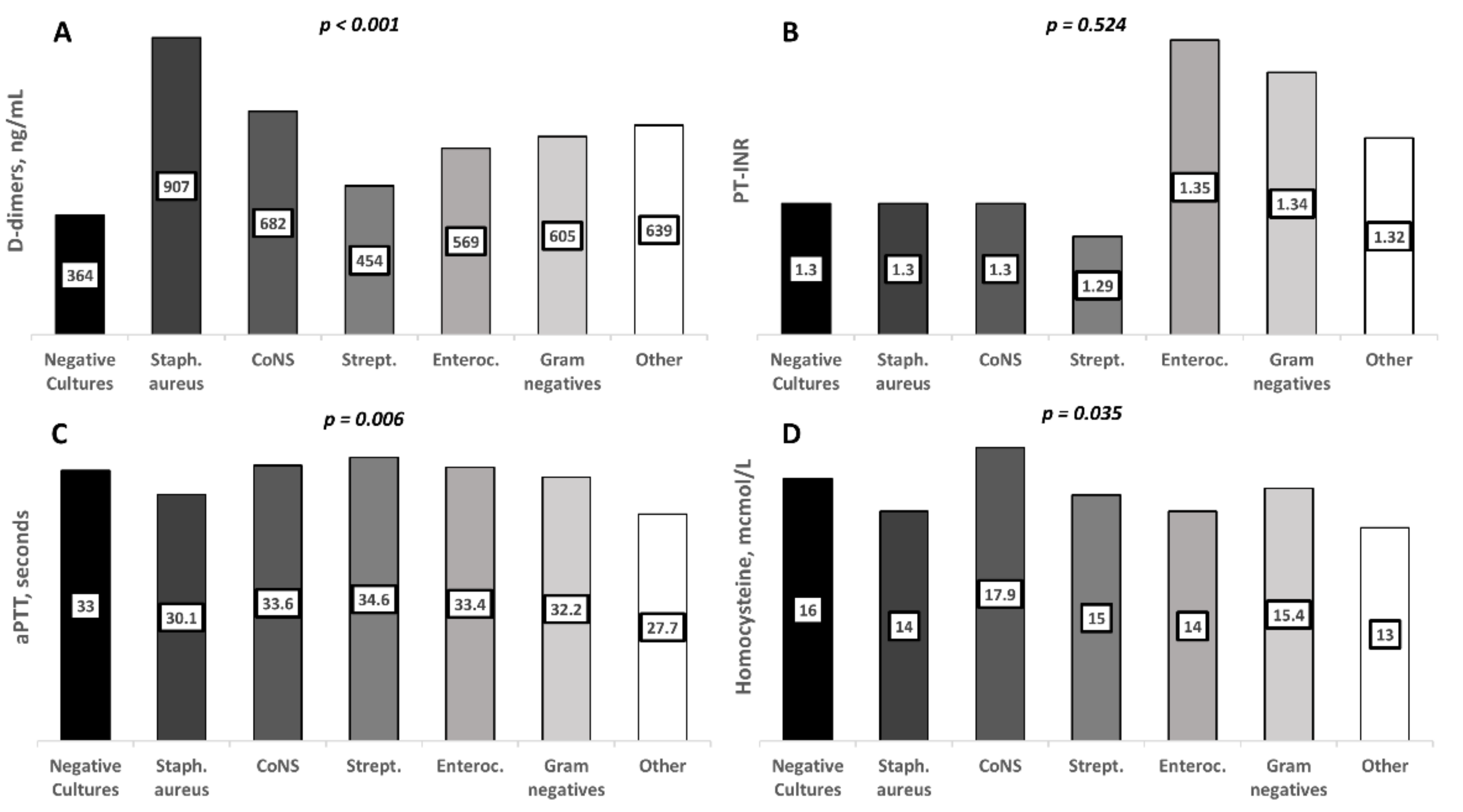
3.3. Hemostasis Parameters and IE Clinical Features
3.4. Hemostasis Parameters and Comorbidities
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef]
- Keynan, Y.; Rubinstein, E. Pathophysiology of Infective Endocarditis. Curr. Infect. Dis. Rep. 2013, 15, 342–346. [Google Scholar] [CrossRef]
- Schwarz, C.; Hoerr, V.; Töre, Y.; Hösker, V.; Hansen, U.; Van De Vyver, H.; Niemann, S.; Kuhlmann, M.T.; Jeibmann, A.; Wildgruber, M.; et al. Isolating Crucial Steps in Induction of Infective Endocarditis with Preclinical Modeling of Host Pathogen Interaction. Front. Microbiol. 2020, 11, 1325. [Google Scholar] [CrossRef] [PubMed]
- Hoerr, V.; Franz, M.; Pletz, M.; Diab, M.; Niemann, S.; Faber, C.; Doenst, T.; Schulze, P.; Deinhardt-Emmer, S.; Löffler, B. S. aureus endocarditis: Clinical aspects and experimental approaches. Int. J. Med. Microbiol. 2018, 308, 640–652. [Google Scholar] [CrossRef] [PubMed]
- Werdan, K.; Dietz, S.; Löffler, B.; Niemann, S.; Bushnaq, H.; Silber, R.-E.; Peters, G.; Müller-Werdan, U. Mechanisms of infective endocarditis: Pathogen–host interaction and risk states. Nat. Rev. Cardiol. 2013, 11, 35–50. [Google Scholar] [CrossRef]
- Liesenborghs, L.; Meyers, S.; Vanassche, T.; Verhamme, P. Coagulation: At the heart of infective endocarditis. J. Thromb. Haemost. 2020, 18, 995–1008. [Google Scholar] [CrossRef]
- Vanassche, T.; Peetermans, W.E.; Herregods, M.-C.; Herijgers, P.; Verhamme, P. Anti-thrombotic therapy in infective endocarditis. Expert Rev. Cardiovasc. Ther. 2011, 9, 1203–1219. [Google Scholar] [CrossRef]
- Verhamme, P.; Hoylaerts, M.F. Hemostasis and inflammation: Two of a kind? Thromb. J. 2009, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Liesenborghs, L.; Verhamme, P.; Vanassche, T. Staphylococcus aureus, master manipulator of the human hemostatic system. J. Thromb. Haemost. 2018, 16, 441–454. [Google Scholar] [CrossRef]
- Vanassche, T.; Kauskot, A.; Verhaegen, J.; Peetermans, W.E.; van Ryn, J.; Schneewind, O.; Hoylaerts, M.F.; Verhamme, P. Fibrin formation by staphylothrombin facilitates Staphylococcus aureus-induced platelet aggregation. Thromb. Haemost. 2012, 107, 1107–1121. [Google Scholar] [CrossRef]
- Peetermans, M.; Liesenborghs, L.; Peerlinck, K.; Van Wijngaerden, E.; Gheysens, O.; Goffin, K.E.; Hoylaerts, M.F.; Jacquemin, M.; Verhaegen, J.; Peetermans, W.E.; et al. Targeting Coagulase Activity in Staphylococcus aureus Bacteraemia: A Randomized Controlled Single-Centre Trial of Staphylothrombin Inhibition. Thromb. Haemost. 2018, 118, 818–829. [Google Scholar] [CrossRef]
- Meini, S.; Sozio, E.; Bertolino, G.; Sbrana, F.; Ripoli, A.; Pallotto, C.; Viaggi, B.; Andreini, R.; Attanasio, V.; Rescigno, C.; et al. D-Dimer as Biomarker for Early Prediction of Clinical Outcomes in Patients with Severe Invasive Infections Due to Streptococcus Pneumoniae and Neisseria Meningitidis. Front. Med. 2021, 8, 627830. [Google Scholar] [CrossRef]
- Scharrer, I. Procoagulant activity during viral infections. Front. Biosci. 2018, 23, 1060–1081. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Rohatgi, A.; Bajaj, M.; Sprung, C.L.; Morales, R.C.; Kasdan, H.; Reiter, A.; Volker, T.; Meissonnier, J.; Beloborodova, N.; et al. Sepsis 2016 Agra, India. Crit. Care 2016, 20, 45. [Google Scholar] [CrossRef] [PubMed]
- Turak, O.; Canpolat, U.; Özcan, F.; Yayla, Ç.; Mendi, M.A.; Öksüz, F.; Tok, D.; Tok, D.; Çağlı, K.; Gölbaşı, Z. D-dimer level predicts in-hospital mortality in patients with infective endocarditis: A prospective single-centre study. Thromb. Res. 2014, 134, 587–592. [Google Scholar] [CrossRef]
- Lin, Y.-W.; Jiang, M.; Wei, X.-B.; Huang, J.-L.; Su, Z.; Wang, Y.; Chen, J.-Y.; Yu, D.-Q. Prognostic value of D-dimer for adverse outcomes in patients with infective endocarditis: An observational study. BMC Cardiovasc. Disord. 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Xu, N.; Fu, Y.; Wang, S.; Li, S.; Cai, D. High level of D-dimer predicts ischemic stroke in patients with infective endocarditis. J. Clin. Lab. Anal. 2020, 34, e23206. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Associ-ation for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Hear. J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, J.V.G.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, E.D.; Adinolfi, L.E.; Tripodi, M.F.; Andreana, A.; Gambardella, M.; Ragone, E.; Precone, D.F.; Utili, R.; Ruggiero, G. Risk factors for “major” embolic events in hospitalized patients with in-fective endocarditis. Am. Heart J. 2003, 146, 311–316. [Google Scholar] [CrossRef]
- Durante-Mangoni, E.; Molaro, R.; Iossa, D. The role of haemostasis in infective endocarditis. Curr. Infect. Dis. Rep. 2014, 16, 435. [Google Scholar] [CrossRef]
- Bakal, R.B.; Karakoyun, S.; Kahveci, G.; Ozveren, O.; Omaygenç, O.; Akpınar, S.H.; Akgün, T.; Ozdemir, N. Relationship between D-dimer and systemic embolism in patients with infective endocarditis. Turk Kardiyol Dern Ars 2013, 41, 589–594. [Google Scholar] [CrossRef][Green Version]
- Barış, V. Özgür D-Dimer is a Strong Predictor of in-hospital mortality in patients with Infective Endocarditis. Anatol. J. Cardiol. 2018, 21, 124–133. [Google Scholar] [CrossRef]
- DiNubile, M.J.; Calderwood, S.B.; Steinhaus, D.M.; Karchmer, A.W. Cardiac conduction abnormalities complicating native valve active infective endocarditis. Am. J. Cardiol. 1986, 58, 1213–1217. [Google Scholar] [CrossRef]
- Vongpatanasin, W.; Hillis, L.D.; Lange, R.A. Prosthetic heart valves. N. Engl. J. Med. 1996, 335, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Thuny, F.; Avierinos, J.-F. Prosthetic Valve Endocarditis: Current Approach and Therapeutic Options. Prog. Cardiovasc. Dis. 2008, 50, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Iossa, D.; Molaro, R.; Andini, R.; Parrella, A.; Ursi, M.P.; Mattucci, I.; De Vincentiis, L.; Dialetto, G.; Utili, R.; Durante-Mangoni, E. Clinical significance of hyperhomocysteinemia in Infective Endocarditis: A case-control study. Medicine 2016, 95, e4972. [Google Scholar] [CrossRef]
- Durante-Mangoni, E.; Iossa, D.; Molaro, R.; Andini, R.; Mattucci, I.; Malgeri, U.; Albisinni, R.; Utili, R. Prevalence and significance of two major inherited thrombophilias in infective endocarditis. Intern. Emerg. Med. 2015, 10, 587–594. [Google Scholar] [CrossRef]
- Hansen, L.; Ozga, A.-K.; Klusmeier, M.; Hillebrand, M.; Tulun, A.; Pannek, N.; Rieß, F.-C. The Freestyle Valve in Severe Necrotizing Aortic Root Endocarditis: Comorbidity Upon Outcome. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef]
- Nagai, T.; Takase, Y.; Hamabe, A.; Tabata, H. Observational Study of Infective Endocarditis at a Community-based Hospital: Dominance of Elderly Patients with Comorbidity. Intern. Med. 2018, 57, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Bradley, S.; Selton-Suty, C.; Tripodi, M.F.; Barsic, B.; Bouza, E.; Cabell, C.H.; de Oliveira Ramos, A.I.; Fowler, V.; Hoen, B.; et al. Current features of infective endocarditis in elderly patients: Results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch. Intern. Med. 2008, 168, 2095–2103. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Missing Data | Result |
|---|---|---|
| Patient number | - | 337 |
| Age, years | - | 64 (51–73) |
| Male gender | - | 237 (70.3) |
| Chronic heart failure (prior to IE onset) | - | 100 (29.7) |
| Charlson Comorbidity Index | 139 | 5 (3–7) |
| Diabetes mellitus | - | 62 (18.4) |
| Chronic hepatitis | - | 61 (18.1) |
| Chronic kidney disease (Stages 3–5) | - | 59 (17.5) |
| Platelet count, cells 103/μL | - | 203 (149–262) |
| Creatinine, mg/dL | - | 1.0 (0.8–1.3) |
| Troponin I, ng/mL | 59 | 0.05 (0.02–0.53) |
| D-dimers, ng/mL | 32 | 605 (296–1101) |
| PT-INR | - | 1.3 (1.18–1.3) |
| Fibrinogen, mg/dL | 134 | 407 (322–532) |
| aPTT, seconds | 5 | 32.5 (29.7–38.1) |
| Homocysteine, mcmol/L | 82 | 15 (12–20) |
| C-reactive protein, mg/dL | 2 | 5.2 (2.4–9.9) |
| Vegetation location - Aortic valve - Mitral valve - Tricuspid/pulmonary valve - Cardiac implantable electronic device - Multivalve involvement - Other | 2 | 115 (34.3) 79 (23.6) 25 (7.5) 86 (25.7) 28 (8.4) 2 (0.6) |
| IE type: - Native valve - Prosthetic valve - Cardiac implantable electronic device - Other | 2 | 145 (43.3) 93 (27.8) 86 (25.7) 11 (3.3) |
| IE causative pathogen: - Streptococci - Coagulase-negative Staphylococci - Staphylococcus aureus - Enterococci - Negative cultures - Gram negatives - Other pathogens | - | 97 (28.8) 63 (18.7) 53 (15.7) 52 (15.4) 49 (14.5) 14 (4.2) 9 (2.7) |
| Vegetation size (max. dimension), mm (n. 257) | 80 | 14 (9–20) |
| Embolic event | - | 104 (30.9) |
| Cardiac surgery | - | 208 (62.3) |
| In-hospital mortality | - | 32 (9.5) |
| 1-year mortality | 70 | 76 (22.6) |
| D-Dimers | p-Value | Fibrinogen | p-Value | PT-INR | p-Value | aPTT | p-Value | PlateletCount | p-Value | Homocysteine | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender: | 0.246 | 0.775 | 0.058 | 0.741 | 0.728 | 0.357 | ||||||
| Male | 566 (280–1086) | 402 (313–536) | 1.30 (1.15–1.50) | 32.6 (30–38.1) | 205 (150–262) | 15 (12–20) | ||||||
| Female | 673 (345–1167) | 433 (332–532) | 1.40 (1.20–2.17) | 32.5 (29.4–37.8) | 200 (137–269) | 14 (12–19) | ||||||
| Age: | 0.047 | 0.099 | 0.270 | 0.729 | 0.001 | 0.003 | ||||||
| ≤64 | 558 (257–1015) | 417 (333–567) | 1.30 (1.14–1.50) | 32.7 (29.2–37.8) | 215 (162–285) | 14 (11–18.5) | ||||||
| >64 | 633 (358–1217) | 390 (300–501) | 1.30 (1.19–1.82) | 32.5 (29.6–38.4) | 190 (131–239) | 16 (13–22) | ||||||
| Embolic event: | <0.001 | 0.134 | 0.473 | <0.001 | 0.150 | 0.366 | ||||||
| No | 512 (237–995) | 402 (306–515) | 1.30 (1.17–1.80) | 33.7 (30.6–38.9) | 204 (146–258) | 15 (12–20) | ||||||
| Yes | 765 (532–1592) | 446 (338–585) | 1.30 (1.18–1.50) | 30.6 (28.4–34.8) | 203 (153–286) | 14.3 (11.7–18.1) | ||||||
| Surgery indication: | 0.309 | 0.595 | <0.001 | 0.266 | 0.917 | 0.840 | ||||||
| No | 525 (310–1027) | 433 (364–504) | 1.41 (1.21–2.35) | 33.7 (29.6–39) | 206 (150–261) | 15.2 (12–19) | ||||||
| Yes | 617 (296–1167) | 399 (308–555) | 1.29 (1.12–1.50) | 32.1 (29.6–37.3) | 203(148–265) | 14.5 (12–20) | ||||||
| Surgery performed: | 0.164 | 0.252 | <0.001 | 0.230 | 0.782 | 0.523 | ||||||
| No | 525 (286–965) | 424 (331–555) | 1.40 (1.20–2.20) | 33.7 (29.1–39.1) | 204 (151–261) | 15.1 (12–19) | ||||||
| Yes | 627 (312–1196) | 397 (302–528) | 1.29 (1.12–1.50) | 32.1 (29.9–37.3) | 203 (147–266) | 14.2(11.4–20.2) | ||||||
| Hospitalization outcome: | 0.012 | 0.933 | 0.013 | 0.090 | 0.398 | 0.886 | ||||||
| Alive | 582 (274–1041) | 407 (324–535) | 1.30 (1.15–1.70) | 32.3 (29.6–37.8) | 204 (152–262) | 15 (12–20) | ||||||
| Dead | 869 (498–1927) | 419 (299–527) | 1.50 (1.22–2.6) | 36.6 (31.5–43) | 201 (103–279) | 15 (12–22) | ||||||
| 1-year outcome: | 0.390 | 0.821 | 0.078 | 0.021 | 0.275 | 0.059 | ||||||
| Alive | 567 (315–1028) | 424 (331–56) | 1.30 (1.15–1.60) | 32.3 (30.1–37.6) | 209 (154–275) | 14.2 (11.4–19) | ||||||
| Dead | 667 (290–1326) | 438 (322–546) | 1.30 (1.20–2.28) | 36.6 (31.5–44) | 201 (143–266) | 16 (12–22) |
| A | ||||||
|---|---|---|---|---|---|---|
| Parameter | In-Hospital Mortality | Univariate Analysis | Multivariate Logistic Regression Analysis | |||
| Survived (n = 305) | Deceased (n = 32) | Odds Ratio (95% C.I.) | p-Value ^ | Odds Ratio (95% C.I.) | p-Value | |
| Age | 64 (50–73) | 68 (55–75) | 0.113 | |||
| Gender: | ||||||
| Male | 213 (69.84) | 24 (75) | 0.77 (0.33–1.78) | 0.685 | ||
| Female | 92 (30.16) | 8 (25) | ||||
| IE etiology: | 0.004 | 1.57 (1.16–2.13) | 0.003 | |||
| S. aureus | 47 (15.4) | 6 (18.75) | ||||
| Coagulase-negative Staphylococci | 55 (18.03) | 8 (25) | ||||
| Streptococci | 95 (31.1) | 2 (6.25) | ||||
| Enterococci | 48 (15.7) | 4 (12.5) | ||||
| Gram negatives | 10 (3.2) | 4 (12.5) | ||||
| Other pathogens | 6 (1.9) | 3 (9.3) | ||||
| Negative cultures | 44 (14.4) | 5 (15.7) | ||||
| Infection type: | (n = 218) | (n = 20) | 4.10 (1.51–11.10) | 0.004 | 10.49 (2.79–39.48) | 0.001 |
| Native | 139 (63.7) | 6 (30) | ||||
| Prosthetic | 79 (36.3) | 14 (70) | ||||
| Charlson Comorbidity Index | (n = 180) 5 (3–7) | (n = 18) 6 (4–7) | 0.253 | |||
| Embolic event *: | 1.19 (0.55–2.57) | 0.689 | ||||
| Yes | 93 (30.5) | 11 (34.4) | ||||
| No | 212 (69.5) | 21 (65.6) | ||||
| Intracardiac abscess | 2.34 (0.98–5.58) | 0.059 | ||||
| Yes | 38 (12.4) | 8 (25) | ||||
| No | 267 (87.6) | 24 (75) | ||||
| Surgery indication: | (n = 303) | (n = 32) | 3.83 (1.13–12.90) | 0.020 | 14.07 (2.68–73.80) | 0.002 |
| Yes | 217 (71.6) | 29 (90.6) | ||||
| No | 86 (28.4) | 3 (9.4) | ||||
| D-dimers, ng/mL | 582 (274–1041) | 869 (498–1927) | 0.012 | 1.00 (1.00–1.00) | 0.005 | |
| Fibrinogen, mg/dL | 407 (324–535) | 419 (299–527) | 0.933 | |||
| PT-INR | 1.30 (1.15–1.70) | 1.50 (1.22–2.6) | 0.013 | 1.61 (0.94–2.74) | 0.077 | |
| aPTT, seconds | 32.3 (29.6–37.8) | 36.6 (31.5–43) | 0.090 | |||
| Platelet count, cells 103/μL | 204 (152–262) | 201 (103–279) | 0.398 | |||
| Homocysteine, mcmol/L | 15 (12–20) | 15 (12–22) | 0.886 | |||
| B | ||||||
| Parameter | 1-Year Mortality | Univariate Analysis | Multivariate Logistic Regression Analysis | |||
| Survived (n = 191) | Deceased (n = 76) | Odds Ratio (95% C.I.) | p-Value ^ | Odds Ratio (95% C.I.) | p-Value | |
| Age | 62 (49–73) | 65 (55–75) | 0.058 | |||
| Gender: | 0.81 (0.45–1.46) | 0.558 | ||||
| Male | 130 (68.1) | 55 (72.3) | ||||
| Female | 61 (31.9) | 21 (27.7) | ||||
| IE etiology: | 0.017 | 1.34 (0.92–1.96) | 0.123 | |||
| S. aureus | 25 (13.1) | 12 (15.8) | ||||
| Coagulase-negative Staphylococci | 34 (17.8) | 18 (23.7) | ||||
| Streptococci | 69 (36.1) | 12 (15.8) | ||||
| Enterococci | 34 (17.8) | 11 (14.5) | ||||
| Gram negatives | 6 (3.1) | 5 (6.6) | ||||
| Other pathogens | 3 (1.6) | 3 (3.9) | ||||
| Negative cultures | 20 (10.5) | 15 (19.7) | ||||
| Infection type: | (n = 141) | (n = 51) | 2.18 (1.13–4.17) | 0.020 | 12.90 (3.02–55.09) | 0.001 |
| Native | 93 (66) | 24 (47) | ||||
| Prosthetic | 48 (34) | 27 (53) | ||||
| Charlson Comorbidity Index | (n = 110) 5 (2–7) | (n = 36) 6 (4.2–7) | 0.009 | 1.32 (1.00–1.74) | 0.049 | |
| Embolic event *: | 0.76 (0.42–1.37) | 0.461 | ||||
| Yes | 61 (32) | 20 (26.3) | ||||
| No | 130 (68) | 56 (73.7) | ||||
| Intracardiac abscess | 1.37 (0.66–1.84) | 0.439 | ||||
| Yes | 25 (15.5) | 13 (17.1) | ||||
| No | 136 (84.5) | 63 (82.9) | ||||
| Surgery indication: | 3.83 (1.13–12.90) | 0.005 | 2.59 (4.515–235.17) | 0.001 | ||
| Yes | 133 (70) | 66 (86.8) | ||||
| No | 57 (30) | 10 (13.2) | ||||
| D-dimers, ng/mL | 567 (315–1028) | 667 (290–1326) | 0.390 | |||
| Fibrinogen, mg/dL | 424 (331–567) | 438 (322–546) | 0.821 | |||
| PT-INR | 1.30 (1.15–1.60) | 1.30 (1.20–2.28) | 0.078 | |||
| aPTT, seconds | 32.3 (30.1–37.6) | 36.6 (31.5–44) | 0.021 | 1.09 (1.02–1.17) | 0.012 | |
| Platelet count, cells 10 3/μL | 209 (154–275) | 201 (143–266) | 0.275 | |||
| Homocysteine, μmol/L | 14.2 (11.4–19) | 16 (12–22) | 0.059 | |||
| CI | 0–1 (n = 22) | 2–3 (n = 34) | ≥4 (n = 142) | p-Value ^ |
|---|---|---|---|---|
| D-dimers, ng/mL | 452 (215–866) | 649 (337–1037) | 614 (259–1222) | 0.439 |
| Fibrinogen, mg/dL | 439 (383–605) | 423 (355–580) | 409 (306–537) | 0.323 |
| PT-INR | 1.35 (1.25–1.58) | 1.20 (1.09–1.37) | 1.33 (1.20–2.14) | 0.006 |
| aPTT, seconds | 33.2 (29.3–38.2) | 30.9 (29–34) | 33 (30.1–38.4) | 0.057 |
| Platelet count, cells103/μL | 209 (149–302.7) | 229 (183–280) | 201 (139–259) | 0.089 |
| Homocysteine, mcmol/L | 14 (11–16.2) | 12 (11–18) | 15 (12–21) | 0.060 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zampino, R.; Iossa, D.; Ursi, M.P.; Bertolino, L.; Karruli, A.; Molaro, R.; Esposito, G.; Vitrone, M.; D’Amico, F.; Albisinni, R.; et al. Clinical Significance and Prognostic Value of Hemostasis Parameters in 337 Patients with Acute Infective Endocarditis. J. Clin. Med. 2021, 10, 5386. https://doi.org/10.3390/jcm10225386
Zampino R, Iossa D, Ursi MP, Bertolino L, Karruli A, Molaro R, Esposito G, Vitrone M, D’Amico F, Albisinni R, et al. Clinical Significance and Prognostic Value of Hemostasis Parameters in 337 Patients with Acute Infective Endocarditis. Journal of Clinical Medicine. 2021; 10(22):5386. https://doi.org/10.3390/jcm10225386
Chicago/Turabian StyleZampino, Rosa, Domenico Iossa, Maria Paola Ursi, Lorenzo Bertolino, Arta Karruli, Rosa Molaro, Gennaro Esposito, Martina Vitrone, Fabiana D’Amico, Rosina Albisinni, and et al. 2021. "Clinical Significance and Prognostic Value of Hemostasis Parameters in 337 Patients with Acute Infective Endocarditis" Journal of Clinical Medicine 10, no. 22: 5386. https://doi.org/10.3390/jcm10225386
APA StyleZampino, R., Iossa, D., Ursi, M. P., Bertolino, L., Karruli, A., Molaro, R., Esposito, G., Vitrone, M., D’Amico, F., Albisinni, R., Durante-Mangoni, E., & on behalf of the Monaldi Hospital CardiovascularInfection Group. (2021). Clinical Significance and Prognostic Value of Hemostasis Parameters in 337 Patients with Acute Infective Endocarditis. Journal of Clinical Medicine, 10(22), 5386. https://doi.org/10.3390/jcm10225386