
Levels of Biosimilar Infliximab during and after Induction Treatment in Crohn’s Disease and Ulcerative Colitis—A Prospective Polish Population Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
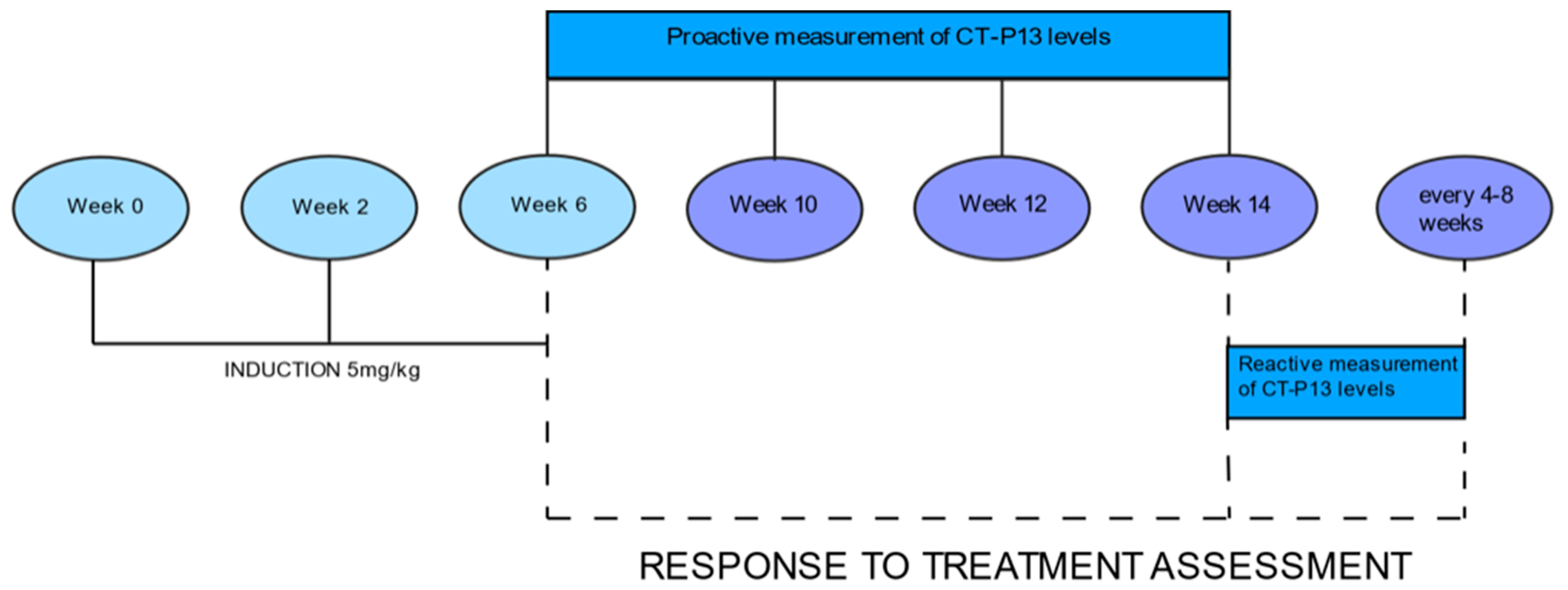
2.2. CT-P13 Concentrations
2.3. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Response to Treatment
3.3. Levels of CT-P13
3.4. Comparative Evaluation for Patients with Crohn’s Disease and Ulcerative Colitis
3.4.1. Response to Treatment
3.4.2. Secondary Loss of Response
3.4.3. Risk Factors
3.4.4. Highest CT-P13 Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, Y.Z.; Li, Y.Y. Inflammatory bowel disease: Pathogenesis. World J. Gastroenterol. 2014, 20, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.R.; Colombel, J.F.; Ungaro, R. The Role of Early Biologic Therapy in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 1896–1905. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohns Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef]
- Roberti, R.; Iannone, L.F.; Palleria, C.; De Sarro, C.; Spagnuolo, R.; Barbieri, M.A.; Vero, A.; Manti, A.; Pisana, V.; Fries, W.; et al. Safety profiles of biologic agents for inflammatory bowel diseases: A prospective pharmacovigilance study in Southern Italy. Curr. Med. Res. Opin. 2020, 36, 1457–1463. [Google Scholar] [CrossRef]
- Spagnuolo, R.; Dastoli, S.; Silvestri, M.; Cosco, C.; Garieri, P.; Bennardo, L.; Nisticò, S.P. Anti-interleukin 12/23 in the treatment of erythema nodosum and Crohn disease: A case report. Dermatol. Ther. 2019, 32, 12811. [Google Scholar] [CrossRef]
- Papamichael, K.; Vogelzang, E.H.; Lambert, J.; Wolbink, G.; Cheifetz, A.S. Therapeutic drug monitoring with biologic agents in immune mediated inflammatory diseases. Expert Rev. Clin. Immunol. 2019, 15, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Lee, J.H.; Hong, S.N.; Yoon, H.; Kang, H.W.; Lee, S.H.; Im, J.P.; Cha, J.M.; Eun, C.S.; Kim, J.W.; et al. Long-term efficacy and safety of CT-P13, a biosimilar of infliximab, in patients with inflammatory bowel disease: A retrospective multicenter study. J. Gastroenterol. Hepatol. 2019, 34, 1523–1532. [Google Scholar] [CrossRef]
- Park, S.H.; Kim, Y.H.; Lee, J.H.; Kwon, H.J.; Lee, S.H.; Park, D.I.; Kim, H.K.; Cheon, J.H.; Im, J.P.; Kim, Y.S.; et al. Post-marketing study of biosimilar infliximab (CT-P13) to evaluate its safety and efficacy in Korea. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Park, J.C.; Lukas, M.; Kolar, M.; Loftus, E.V. Biosimilars: Concept, current status, and future perspectives in inflammatory bowel diseases. Intest. Res. 2020, 18, 34–44. [Google Scholar] [CrossRef] [Green Version]
- van Deventer, S.J. Review article: Targeting TNF alpha as a key cytokine in the inflammatory processes of Crohn’s disease—The mechanisms of action of infliximab. Aliment. Pharmacol. Ther. 1999, 13, 3–8; discussion 38. [Google Scholar] [CrossRef]
- Guerbau, L.; Gerard, R.; Duveau, N.; Staumont-Salle, D.; Branche, J.; Maunoury, V.; Cattan, S.; Wils, P.; Boualit, M.; Libier, L.; et al. Patients with Crohn’s Disease with High Body Mass Index Present More Frequent and Rapid Loss of Response to Infliximab. Inflamm. Bowel Dis. 2017, 23, 1853–1859. [Google Scholar] [CrossRef] [Green Version]
- Roblin, X.; Williet, N.; Boschetti, G.; Phelip, J.M.; Del Tedesco, E.; Berger, A.E.; Vedrines, P.; Duru, G.; Peyrin-Biroulet, L.; Nancey, S.; et al. Addition of azathioprine to the switch of anti-TNF in patients with IBD in clinical relapse with undetectable anti-TNF trough levels and antidrug antibodies: A prospective randomised trial. Gut 2020, 69, 1206–1212. [Google Scholar] [CrossRef]
- Viazis, N.; Koukouratos, T.; Anastasiou, J.; Giakoumis, M.; Triantos, C.; Tsolias, C.; Theocharis, G.; Karamanolis, D.G. Azathioprine discontinuation earlier than 6 months in Crohn’s disease patients started on anti-TNF therapy is associated with loss of response and the need for anti-TNF dose escalation. Eur. J. Gastroenterol. Hepatol. 2015, 27, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Chen, B.L.; Mao, R.; Zhang, S.H.; He, Y.; Zeng, Z.R.; Ben-Horin, S.; Chen, M.H. Systematic review with meta-analysis: Loss of response and requirement of anti-TNFalpha dose intensification in Crohn’s disease. J. Gastroenterol. 2017, 52, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Taxonera, C.; Olivares, D.; Mendoza, J.L.; Diaz-Rubio, M.; Rey, E. Need for infliximab dose intensification in Crohn’s disease and ulcerative colitis. World J. Gastroenterol. 2014, 20, 9170–9177. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Casteele, N.V.; Ferrante, M.; Gils, A.; Cheifetz, A.S. Therapeutic Drug Monitoring during Induction of Anti-Tumor Necrosis Factor Therapy in Inflammatory Bowel Disease: Defining a Therapeutic Drug Window. Inflamm. Bowel Dis. 2017, 23, 1510–1515. [Google Scholar] [CrossRef] [Green Version]
- Beltran, B.; Iborra, M.; Saez-Gonzalez, E.; Marques-Minana, M.R.; Moret, I.; Cerrillo, E.; Tortosa, L.; Bastida, G.; Hinojosa, J.; Poveda-Andres, J.L.; et al. Fecal Calprotectin Pretreatment and Induction Infliximab Levels for Prediction of Primary Nonresponse to Infliximab Therapy in Crohn’s Disease. Dig. Dis. 2019, 37, 108–115. [Google Scholar] [CrossRef]
- Clarkston, K.; Tsai, Y.T.; Jackson, K.; Rosen, M.J.; Denson, L.A.; Minar, P. Development of Infliximab Target Concentrations during Induction in Pediatric Crohn Disease Patients. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 68–74. [Google Scholar] [CrossRef] [PubMed]
- van Hoeve, K.; Dreesen, E.; Hoffman, I.; Van Assche, G.; Ferrante, M.; Gils, A.; Vermeire, S. Adequate Infliximab Exposure during Induction Predicts Remission in Paediatric Patients with Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 847–853. [Google Scholar] [CrossRef]
- Ilias, A.; Gonczi, L.; Kurti, Z.; Lakatos, P.L. Biosimilars in ulcerative colitis: When and for who? Best Pract. Res. Clin. Gastroenterol. 2018, 32–33, 35–42. [Google Scholar] [CrossRef]
- Novakovic, V.; Abdija, S.; Larsen, P.B.; Fenger, M.; Gredal, L.; Jacobsen, K.K. Comparison of the Quantum Blue(R) reader Point-of-Care system versus ELISA technique for therapeutic drug monitoring of Infliximab levels. Clin. Biochem. 2019, 74, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Mei, W.Q.; Hu, H.Z.; Liu, Y.; Li, Z.C.; Wang, W.G. Infliximab is superior to other biological agents for treatment of active ulcerative colitis: A meta-analysis. World J. Gastroenterol. 2015, 21, 6044–6051. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Hanauer, S.B. Assessing response and loss of response to biological therapies in IBD. Am. J. Gastroenterol. 2011, 106, 685–698. [Google Scholar] [CrossRef]
- Negoescu, D.M.; Enns, E.A.; Swanhorst, B.; Baumgartner, B.; Campbell, J.P.; Osterman, M.T.; Papamichael, K.; Cheifetz, A.S.; Vaughn, B.P. Proactive vs Reactive Therapeutic Drug Monitoring of Infliximab in Crohn’s Disease: A Cost-Effectiveness Analysis in a Simulated Cohort. Inflamm. Bowel Dis. 2020, 26, 103–111. [Google Scholar] [CrossRef]
- Papamichael, K.; Cheifetz, A.S.; Melmed, G.Y.; Irving, P.M.; Casteele, N.V.; Kozuch, P.L.; Raffals, L.E.; Baidoo, L.; Bressler, B.; Devlin, S.M.; et al. Appropriate Therapeutic Drug Monitoring of Biologic Agents for Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2019, 17, 1655–1668. [Google Scholar] [CrossRef] [Green Version]
- Casteele, N.V.; Ferrante, M.; Van Assche, G.; Ballet, V.; Compernolle, G.; Van Steen, K.; Simoens, S.; Rutgeerts, P.; Gils, A.; Vermeire, S. Trough concentrations of infliximab guide dosing for patients with inflammatory bowel disease. Gastroenterology 2015, 148, 1320–1329. [Google Scholar] [CrossRef]
- D’Haens, G.; Vermeire, S.; Lambrecht, G.; Baert, F.; Bossuyt, P.; Pariente, B.; Buisson, A.; Bouhnik, Y.; Filippi, J.; Woude, J.V.; et al. Increasing Infliximab dose Based on Symptoms, Biomarkers, and Serum Drug Concentrations does not Increase Clinical, Endoscopic, and Corticosteroid-Free Remission in Patients with Active Luminal Crohn’s Disease. Gastroenterology 2018, 154, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Chachu, K.A.; Vajravelu, R.K.; Vaughn, B.P.; Ni, J.; Osterman, M.T.; Cheifetz, A.S. Improved Long-term Outcomes of Patients with Inflammatory Bowel Disease Receiving Proactive Compared with Reactive Monitoring of Serum Concentrations of Infliximab. Clin. Gastroenterol. Hepatol. 2017, 15, 1580–1588. [Google Scholar] [CrossRef]
- Papamichael, K.; Cheifetz, A.S. Therapeutic Drug Monitoring in IBD: The New Standard-of-Care for Anti-TNF Therapy. Am. J. Gastroenterol. 2017, 112, 673–676. [Google Scholar] [CrossRef]
- Dreesen, E.; Baert, F.; Laharie, D.; Bossuyt, P.; Bouhnik, Y.; Buisson, A.; Lambrecht, G.; Louis, E.; Oldenburg, B.; Pariente, B.; et al. Monitoring a Combination of Calprotectin and Infliximab Identifies Patients with Mucosal Healing of Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 637–646. [Google Scholar] [CrossRef]
- Kennedy, N.A.; Heap, G.A.; Green, H.D.; Hamilton, B.; Bewshea, C.; Walker, G.J.; Thomas, A.; Nice, R.; Perry, M.H.; Bouri, S.; et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: A prospective, multicentre, cohort study. Lancet Gastroenterol. Hepatol. 2019, 4, 341–353. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, K.; Van Stappen, T.; Casteele, N.V.; Gils, A.; Billiet, T.; Tops, S.; Claes, K.; Van Assche, G.; Rutgeerts, P.; Vermeire, S.; et al. Infliximab Concentration Thresholds during Induction Therapy Are Associated with Short-term Mucosal Healing in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2016, 14, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Casteele, N.V.; Papamichael, K.; Jeyarajah, J.; Osterman, M.T.; Cheifetz, A.S. DOP45 Adequate infliximab exposure during the induction phase is associated with early complete fistula response in patients with fistulizing Crohn’s disease: A post-hoc analysis of the ACCENT-2 trial. J. Crohns Colitis 2019, 13, S053–S054. [Google Scholar] [CrossRef]
- Pekala, A.; Filip, R.; Aebisher, D. Anti-Drug Antibodies in Patients with Inflammatory Bowel Diseases Treated with Biosimilar Infliximab: A Prospective Cohort Study. J. Clin. Med. 2021, 10, 2653. [Google Scholar] [CrossRef] [PubMed]
- Cornillie, F.; Hanauer, S.B.; Diamond, R.H.; Wang, J.; Tang, K.L.; Xu, Z.; Rutgeerts, P.; Vermeire, S. Postinduction serum infliximab trough level and decrease of C-reactive protein level are associated with durable sustained response to infliximab: A retrospective analysis of the ACCENT I trial. Gut 2014, 63, 1721–1727. [Google Scholar] [CrossRef] [PubMed]
- Casteele, N.V.; Jeyarajah, J.; Jairath, V.; Feagan, B.G.; Sandborn, W.J. Infliximab Exposure-Response Relationship and Thresholds Associated with Endoscopic Healing in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2019, 17, 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.; Dolce, P.; Devas, N.; Baldassano, R.; Martinelli, M. Post-induction infliximab trough levels and disease activity in the clinical evolution of pediatric ulcerative colitis. United Eur. Gastroenterol. J. 2020, 8, 425–435. [Google Scholar] [CrossRef]
- Syversen, S.W.; Goll, G.L.; Jorgensen, K.K.; Sandanger, O.; Sexton, J.; Olsen, I.C.; Gehin, J.E.; Warren, D.J.; Brun, M.K.; Klaasen, R.A.; et al. Effect of Therapeutic Drug Monitoring vs Standard Therapy during Infliximab Induction on Disease Remission in Patients with Chronic Immune-Mediated Inflammatory Diseases: A Randomized Clinical Trial. JAMA 2021, 325, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Brandse, J.F.; Mathot, R.A.; van der Kleij, D.; Rispens, T.; Ashruf, Y.; Jansen, J.M.; Rietdijk, S.; Lowenberg, M.; Ponsioen, C.Y.; Singh, S.; et al. Pharmacokinetic Features and Presence of Antidrug Antibodies Associate with Response to Infliximab Induction Therapy in Patients with Moderate to Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2016, 14, 251–258. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Crohn’s Disease Patients | Ulcerative Colitis Patients | |
|---|---|---|
| n | 32 | 33 |
| Females, n (%) | 17 (53.1) | 14 (42.4) |
| Males, n (%) | 15 (46.9) | 19 (57.6) |
| Age, median (range) years | 30.6 (21–54) | 38.9 (20–81) |
| Disease duration (IQR) years | 3.4 (0.5–13) | 5.2 (0.5–11) |
| Smoking status, n (%) | ||
| Never smoked | 27 (84.4) | 30 (90.9) |
| Ex-smoker | 3 (9.4) | 2 (6.0) |
| Current smoker | 2 (6.2) | 1 (3.1) |
| Concomitant treatment, n (%) | ||
| Thiopurines | 26 (81.2) | 30 (90.9) |
| Steroids | 15 (46.80) | 21 (63.6) |
| Mesalazine | 16 (50.0) | 33 (100.0) |
| Crohn’s disease | ||
| Age at diagnosis, n (%) | A1 (diagnosed <17 years of age) | 4 (12.5) |
| A2 (diagnosed 17–40 years of age) | 29 (90.6) | |
| A3 (diagnosed >40 years of age) | 0 | |
| Disease location, n (%) | L1(ileal) | 6 (18.7) |
| L2 (colonic) | 7 (21.8) | |
| L3 (ileocolonic) | 18 (56.2) | |
| L3 + (ileocolonic) ++ L4 (upper gastrointestinal tract) | 1 (3.1) | |
| Disease behavior, n (%) | B1 (nonstricturing, nonpenetrating) | 22 (68.7) |
| B2 (stricturing) | 3 (9.4) | |
| B3 (penetrating) | 7 (21.9) | |
| CDAI indicator at the start of treatment, mean (range) | 266.6 (150–435) | |
| Ulcerative colitis | ||
| Extent, n (%) | E1 (proctitis) | 2 (6.0) |
| E2 (left-sided colitis) | 21 (63.6) | |
| E3 (pancolitis) | 10 (30.3) | |
| Severity, n (%) | S1 (mild) | 5 (15.2) |
| S2 (moderate) | 20 (60.6) | |
| S3 (severe) | 8 (24.2) | |
| Mayo score at the start of treatment, mean (range) | 8.3 (7–12) | |
| Week 6 | Week 10 | Week 12 | Week 14 | |
|---|---|---|---|---|
| Crohn’s disease | 84.4% | 84.0% | 80.0% | 68.7% |
| Ulcerative colitis | 84.8% | 88.5% | 88.5% | 57.6% |
| Crohn’s Disease | Ulcerative Colitis | p-Value | |
|---|---|---|---|
| n | 32 | 33 | |
| Response to treatment (in total) | 26/32 (81.2%) | 27/33 (81.8%) | >0.999 |
| Primary lack of response (in total) | 6/32 (18.8%) | 6/33 (18.2%) | |
| Secondary loss of response (in total) | 14/26 (53.8%) | 10/27 (37.0%) | 0.341 |
| Week 6 | |||
| Patients who achieved CT-P13 levels of 3 μg/mL at week 6 | 27/32 (84.4%) | 28/33 (84.8%) | >0.999 |
| Primary response | 24/27 (88.9%) | 26/28 (92.8%) | 0.670 |
| Primary lack of response | 3/27 (11.1%) | 2/28 (7.2%) | |
| Secondary loss of response | 12/24 (50%) | 5/26 (19.2%) | 0.046 |
| Patients who did not achieve CT-P13 levels of 3 μg/mL at week 6 | 5/32 (15.6%) | 5/33 (15.1%) | >0.999 |
| Primary response | 2/5 (40.0%) | 1/5 (20.0%) | >0.999 |
| Primary lack of response | 3/5 (60.0%) | 4/5 (80.0%) | |
| Secondary loss of response | 2/2 (100%) | 0/1 (0%) | 0.333 |
| Week 14 | |||
| Patients who achieved therapeutic CT-P13 levels of 3 μg/mL at week 14 | 23/32 (71.9%) | 19/33 (57.6%) | 0.499 |
| Primary response | 21/23 (91.3%) | 18/19 (94.7%) | >0.999 |
| Primary lack of response | 2/23 (8.7%) | 1/19 (5.3%) | |
| Secondary loss of response | 9/21 (42.8%) | 5/18 (27.8%) | 0.272 |
| Patients who did not achieve therapeutic CT-P13 levels of 3 μg/mL at week 14 | 9/32 (28.1%) | 14/33 (42.4%) | 0.344 |
| Primary response | 5/9 (55.5%) | 9/14 (64.3%) | >0.999 |
| Primary lack of response | 4/9 (44.4%) | 5/14 (35.7%) | |
| Secondary loss of response | 5/5 (100%) | 5/9 (55.5%) | 0.221 |
| Crohn’s Disease (n = 32) | Ulcerative Colitis (n = 33) | |||||
|---|---|---|---|---|---|---|
| Primary Lack of Response | Response to Treatment | p | Primary Lack of Response | Response to Treatment | p | |
| n = 6 | n = 26 | n = 6 | n = 27 | |||
| Sex | ||||||
| Women | 3 (50.0%) | 14 (53.8%) | >0.999 | 3 (50.0%) | 11 (40.7%) | >0.999 |
| Men | 3 (50.0%) | 12 (46.1%) | 3 (50.0%) | 16 (59.3%) | ||
| Concomitant treatment with thiopurines | ||||||
| Yes | 5 (83.3%) | 21 (80.8%) | >0.999 | 6 (100%) | 24 (88.9%) | >0.999 |
| No | 1 (16.7%) | 5 (19.2%) | 0 (0%) | 3 (11.1%) | ||
| History of treatment with infliximab | ||||||
| Yes | 1 (16.7%) | 2 (7.6%) | 0.476 | 0 (0%) | 2 (7.4%) | >0.999 |
| No | 5 (83.3%) | 24 (92.3%) | 6 (100%) | 25 (92.6%) | ||
| Crohn’s Disease (n = 32) | Ulcerative Colitis (n = 33) | |||||
|---|---|---|---|---|---|---|
| Secondary Loss of Response | Response to Treatment | p | Secondary Loss of Response | Response to Treatment | p | |
| n = 14 | n = 18 | n = 10 | n = 23 | |||
| Sex | ||||||
| Women | 9 (64.3%) | 8 (44.4%) | 0.265 | 5 (50.0%) | 9 (39.1%) | 0.562 |
| Men | 5 (35.7%) | 10 (55.6%) | 5 (50.0%) | 14 (60.9%) | ||
| Concomitant treatment with thiopurines | ||||||
| Yes | 13 (92.9%) | 13 (72.2%) | 0.196 | 10 (100%) | 20 (87.0%) | 0.536 |
| No | 1 (7.1%) | 5 (27.8%) | 0 (0%) | 3 (13.0%) | ||
| History of treatment with infliximab | ||||||
| Yes | 1 (7.1%) | 2 (11.1%) | >0.999 | 1 (10.0%) | 1 (4.3%) | 0.521 |
| No | 13 (92.9%) | 16 (88.9%) | 9 (90.0%) | 22 (95.6%) | ||
| Crohn’s Disease | Ulcerative Colitis | |||||
|---|---|---|---|---|---|---|
| Level >20 μg/mL at Weeks 6 and 10 | Level <20 μg/mL at Weeks 6 and 10 | p | Level >20 μg/mL at Weeks 6 and 10 | Level <20 μg/mL at Weeks 6 and 10 | p | |
| n = 14 | n = 18 | n = 13 | n = 20 | |||
| Response to treatment | 12/14 (85.8%) | 12/18 (66.6%) | 0.412 | 12/13 (92.3%) | 14/20 (70.0%) | 0.202 |
| Therapeutic levels of CT-P13 at week 14 | 12/12 (100%) | 9/12 (75.0%) | 0.217 | 9/12 (75.0%) | 8/14 (57.1%) | 0.429 |
| Secondary loss of response | 6/12 (50.0%) | 8/12 (66.6%) | 0.680 | 3/12 (25.0%) | 7/14 (50.0%) | 0.248 |
| Lack of response | 2/14 (14.2%) | 6/18 (33.4%) | 0.412 | 1/13 (7.7%) | 6/20 (30.0%) | 0.202 |
| Therapeutic levels of CT-P13 at week 14 | 2/2 (100%) | 0/6 (0%) | 0.036 | 1/1 (100%) | 1/6 (16.7%) | 0.286 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pękala, A.; Filip, R. Levels of Biosimilar Infliximab during and after Induction Treatment in Crohn’s Disease and Ulcerative Colitis—A Prospective Polish Population Study. J. Clin. Med. 2021, 10, 5311. https://doi.org/10.3390/jcm10225311
Pękala A, Filip R. Levels of Biosimilar Infliximab during and after Induction Treatment in Crohn’s Disease and Ulcerative Colitis—A Prospective Polish Population Study. Journal of Clinical Medicine. 2021; 10(22):5311. https://doi.org/10.3390/jcm10225311
Chicago/Turabian StylePękala, Anna, and Rafał Filip. 2021. "Levels of Biosimilar Infliximab during and after Induction Treatment in Crohn’s Disease and Ulcerative Colitis—A Prospective Polish Population Study" Journal of Clinical Medicine 10, no. 22: 5311. https://doi.org/10.3390/jcm10225311
APA StylePękala, A., & Filip, R. (2021). Levels of Biosimilar Infliximab during and after Induction Treatment in Crohn’s Disease and Ulcerative Colitis—A Prospective Polish Population Study. Journal of Clinical Medicine, 10(22), 5311. https://doi.org/10.3390/jcm10225311