
Cardiac Surgery Associated AKI Prevention Strategies and Medical Treatment for CSA-AKI

 ,
, 
Abstract
1. Background
1.1. Pathophysiology
1.2. Aki Diagnosis and Roles of Biomarkers
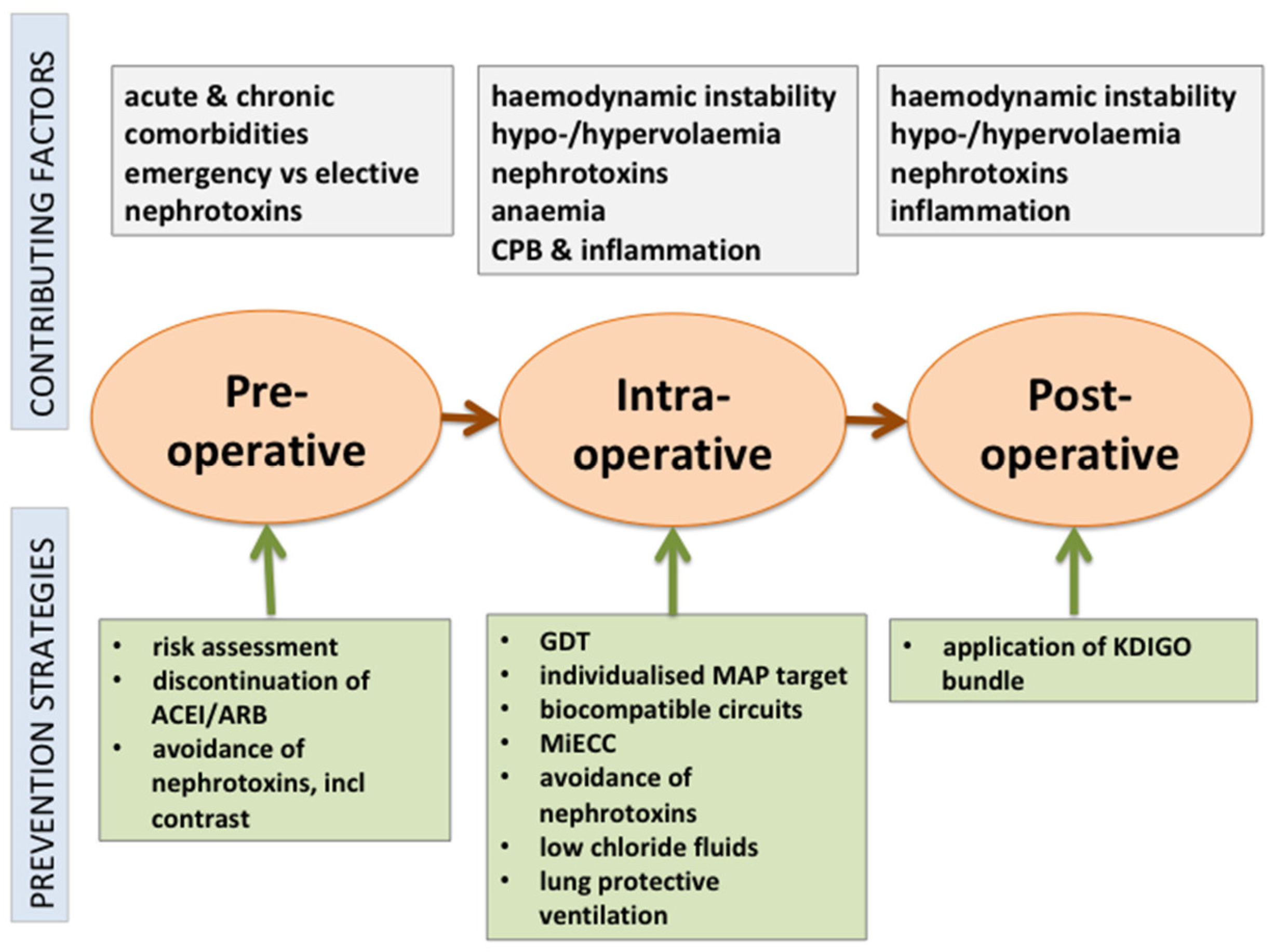
2. Prevention Strategies
2.1. Preoperative Measures
2.1.1. Pharmacological Interventions
- (i)
- Corticosteroids
- (ii)
- Albumin
- (iii)
- Erythropoietin
- (iv)
- Statins
- (v)
- N-acetylcysteine
- (vi)
- Sodium bicarbonate
- (vii)
- Others
- (viii)
- Novel therapies in development
2.1.2. Non-Pharmacological Interventions
- (i)
- Intra-Aortic Balloon Pump
- (ii)
- Contrast administration
2.2. Intraoperative Strategies
2.2.1. Surgical Techniques
2.2.2. CPB-Related Factors
- (i)
- Haemodynamics
- (ii)
- Biocompatible coatings
- (iii)
- Minimally invasive extracorporeal circulation
- (iv)
- Leucocyte depletion
- (v)
- Duration of CPB
2.2.3. Anaesthesia-Related Techniques
- (i)
- Remote ischaemic preconditioning
- (ii)
- Volatile versus intravenous anaesthesia
2.2.4. Intraoperative Fluid and Goal Directed Therapy
- (i)
- Fluids
- (ii)
- Goal-directed haemodynamic therapy
- (iii)
- Blood products
2.2.5. Mechanical Ventilation
2.2.6. Drugs
2.3. Postoperative Strategies
3. Limitations and Research Recommendations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACEI | angiotensin converting enzyme inhibitor |
| ARB | angiotensin receptor blocker |
| CPB | cardiopulmonary bypass |
| GDT | goal-directed therapy |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| MAP | mean arterial pressure |
| MiECC | minimally invasive extracorporeal circulation |
References
- Nadim, M.K.; Forni, L.G.; Bihorac, A.; Hobson, C.; Koyner, J.L.; Shaw, A.; Arnaoutakis, G.J.; Ding, X.; Engelman, D.T.; Gasparovic, H.; et al. Cardiac and Vascular Surgery-Associated Acute Kidney Injury: The 20th International Consensus Conference of the ADQI (Acute Disease Quality Initiative) Group. J. Am. Heart Assoc. 2018, 7, e008834. [Google Scholar] [CrossRef]
- Ostermann, M.; Cennamo, A.; Meersch, M.; Kunst, G. A narrative review of the impact of surgery and anaesthesia on acute kidney injury. Anaesthesia 2020, 75, e121–e133. [Google Scholar] [CrossRef]
- Ostermann, M.E.; Taube, D.; Morgan, C.J.; Evans, T.W. Acute renal failure following cardiopulmonary bypass: A changing picture. Intensive Care Med. 2000, 26, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Cerdá, J. The Burden of Acute Kidney Injury and Related Financial Issues. Contrib. Nephrol. 2018, 193, 100–112. [Google Scholar]
- Pickkers, P.; Darmon, M.; Hoste, E.; Joannidis, M.; Legrand, M.; Ostermann, M.; Prowle, J.R.; Schneider, A.; Schetz, M. Acute kidney injury in the critically ill: An updated review on pathophysiology and management. Intensive Care Med. 2021, 47, 835–850. [Google Scholar] [CrossRef]
- Ostermann, M.; Chang, R.W. Impact of different types of organ failure on outcome in intensive care unit patients with acute kidney injury. J. Crit. Care 2011, 26, 635.e1–635.e10. [Google Scholar] [CrossRef] [PubMed]
- Haines, R.W.; Powell-Tuck, J.; Leonard, H.; Crichton, S.; Ostermann, M. Long-term kidney function of patients discharged from hospital after an intensive care admission: Observational cohort study. Sci. Rep. 2021, 11, 9928. [Google Scholar] [CrossRef]
- Kunst, G.; Milojevic, M.; Boer, C.; De Somer, F.; Gudbjartsson, T.; van den Goor, J.; Jones, T.J.; Lomivorotov, V.; Merkle, F.; Ranucci, M.; et al. 2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery. Br. J. Anaesth. 2019, 123, 713–757. [Google Scholar] [CrossRef]
- Joannidis, M.; Druml, W.; Forni, L.G.; Groeneveld, A.B.J.; Honore, P.M.; Hoste, E.; Ostermann, M.; Oudemans-van Straaten, H.M.; Schetz, M. Prevention of acute kidney injury and protection of renal function in the intensive care unit: Update 2017: Expert opinion of the Working Group on Prevention, AKI section, European Society of Intensive Care Medicine. Intensive Care Med. 2017, 43, 730–749. [Google Scholar] [CrossRef] [PubMed]
- Engelman, D.T.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society Recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Liu, K. Pathophysiology of AKI. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Ostermann, M. Diagnosis of acute kidney injury: Kidney Disease Improving Global Outcomes criteria and beyond. Curr. Opin. Crit. Care 2014, 20, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.E.; Blaine, C.; Dawnay, A.; Devonald, M.A.; Ftouh, S.; Laing, C.; Latchem, S.; Lewington, A.; Milford, D.V.; Ostermann, M. The definition of acute kidney injury and its use in practice. Kidney Int. 2015, 87, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Kashani, K.; Rosner, M.H.; Ostermann, M. Creatinine: From physiology to clinical application. Eur. J. Intern. Med. 2020, 72, 9–14. [Google Scholar] [CrossRef]
- Ostermann, M.; Joannidis, M. Acute kidney injury 2016: Diagnosis and diagnostic workup. Crit. Care 2016, 20, 299. [Google Scholar] [CrossRef]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers From the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA Netw. Open 2020, 3, e2019209. [Google Scholar] [CrossRef]
- Ostermann, M.; Karsten, E.; Lumlertgul, N. Biomarker-Based Management of AKI: Fact or Fantasy? Nephron 2021, 1–7. [Google Scholar] [CrossRef]
- Ostermann, M. Editorial: Management of acute kidney injury during critical illness—What is on the horizon? Curr. Opin. Crit. Care 2020, 26, 517–518. [Google Scholar]
- Zarbock, A.; Küllmar, M.; Ostermann, M.; Lucchese, G.; Baig, K.; Cennamo, A.; Rajani, R.; McCorkell, S.; Arndt, C.; Wulf, H.; et al. Prevention of Cardiac Surgery-Associated Acute Kidney Injury by Implementing the KDIGO Guidelines in High-Risk Patients Identified by Biomarkers: The PrevAKI-Multicenter Randomized Controlled Trial. Anesth. Analg. 2021, 133, 292–302. [Google Scholar] [CrossRef]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef]
- Chen, Y.; Garvin, L.M.; Nickola, T.J.; Watson, A.M.; Colberg-Poley, A.M.; Rose, M.C. IL-1β induction of MUC5AC gene expression is mediated by CREB and NF-κB and repressed by dexamethasone. Am. J. Physiol. Lung Cell Mol. Physiol. 2014, 306, L797–L807. [Google Scholar] [CrossRef]
- Dieleman, J.M.; Nierich, A.P.; Rosseel, P.M.; van der Maaten, J.M.; Hofland, J.; Diephuis, J.C.; Schepp, R.M.; Boer, C.; Moons, K.G.; van Herwerden, L.A.; et al. Intraoperative high-dose dexamethasone for cardiac surgery: A randomized controlled trial. JAMA 2012, 308, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Dvirnik, N.; Belley-Cote, E.P.; Hanif, H.; Devereaux, P.J.; Lamy, A.; Dieleman, J.M.; Vincent, J.; Whitlock, R.P. Steroids in cardiac surgery: A systematic review and meta-analysis. Br. J. Anaesth. 2018, 120, 657–667. [Google Scholar] [CrossRef]
- Whitlock, R.P.; Devereaux, P.J.; Teoh, K.H.; Lamy, A.; Vincent, J.; Pogue, J.; Paparella, D.; Sessler, D.I.; Karthikeyan, G.; Villar, J.C.; et al. Methylprednisolone in patients undergoing cardiopulmonary bypass (SIRS): A randomised, double-blind, placebo-controlled trial. Lancet 2015, 386, 1243–1253. [Google Scholar] [CrossRef]
- Jacob, K.A.; Leaf, D.E.; Dieleman, J.M.; van Dijk, D.; Nierich, A.P.; Rosseel, P.M.; van der Maaten, J.M.; Hofland, J.; Diephuis, J.C.; de Lange, F.; et al. Intraoperative High-Dose Dexamethasone and Severe AKI after Cardiac Surgery. J. Am. Soc. Nephrol. 2015, 26, 2947–2951. [Google Scholar] [CrossRef]
- Lee, E.H.; Kim, W.J.; Kim, J.Y.; Chin, J.H.; Choi, D.K.; Sim, J.Y.; Choo, S.J.; Chung, C.H.; Lee, J.W.; Choi, I.C. Effect of Exogenous Albumin on the Incidence of Postoperative Acute Kidney Injury in Patients Undergoing Off-pump Coronary Artery Bypass Surgery with a Preoperative Albumin Level of Less Than 4.0 g/dl. Anesthesiology 2016, 124, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Sølling, C.; Christensen, A.T.; Krag, S.; Frøkiaer, J.; Wogensen, L.; Krog, J.; Tønnesen, E.K. Erythropoietin administration is associated with short-term improvement in glomerular filtration rate after ischemia-reperfusion injury. Acta Anaesthesiol. Scand. 2011, 55, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Huang, T.; Cao, X.; Xu, G. Comparative Efficacy of Drugs for Preventing Acute Kidney Injury after Cardiac Surgery: A Network Meta-Analysis. Am. J. Cardiovasc. Drugs 2018, 18, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Putzu, A.; de Carvalho, E.S.C.; de Almeida, J.P.; Belletti, A.; Cassina, T.; Landoni, G.; Hajjar, L.A. Perioperative statin therapy in cardiac and non-cardiac surgery: A systematic review and meta-analysis of randomized controlled trials. Ann. Intensive Care 2018, 8, 95. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Jayaram, R.; Jiang, L.; Emberson, J.; Zhao, Y.; Li, Q.; Du, J.; Guarguagli, S.; Hill, M.; Chen, Z.; et al. Perioperative Rosuvastatin in Cardiac Surgery. N. Engl. J. Med. 2016, 374, 1744–1753. [Google Scholar] [CrossRef]
- Tamayo, E.; Alvarez, F.J.; Alonso, O.; Bustamante, R.; Castrodeza, J.; Soria, S.; Lajo, C. Effects of simvastatin on systemic inflammatory responses after cardiopulmonary bypass. J. Cardiovasc. Surg. 2009, 50, 687–694. [Google Scholar] [CrossRef]
- Almansob, M.A.; Xu, B.; Zhou, L.; Hu, X.X.; Chen, W.; Chang, F.J.; Ci, H.B.; Yao, J.P.; Xu, Y.Q.; Yao, F.J.; et al. Simvastatin reduces myocardial injury undergoing noncoronary artery cardiac surgery: A randomized controlled trial. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2304–2313. [Google Scholar] [CrossRef]
- Liakopoulos, O.J.; Choi, Y.H.; Haldenwang, P.L.; Strauch, J.; Wittwer, T.; Dörge, H.; Stamm, C.; Wassmer, G.; Wahlers, T. Impact of preoperative statin therapy on adverse postoperative outcomes in patients undergoing cardiac surgery: A meta-analysis of over 30,000 patients. Eur. Heart J. 2008, 29, 1548–1559. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Gu, C.; Gao, M.; Yu, W.; Yu, Y. Preoperative Statin Therapy and Renal Outcomes After Cardiac Surgery: A Meta-analysis and Meta-regression of 59,771 Patients. Can. J. Cardiol. 2015, 31, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Lewicki, M.; Ng, I.; Schneider, A.G. HMG CoA reductase inhibitors (statins) for preventing acute kidney injury after surgical procedures requiring cardiac bypass. Cochrane Database Syst. Rev. 2015, Cd010480. [Google Scholar] [CrossRef]
- Mei, M.; Zhao, H.W.; Pan, Q.G.; Pu, Y.M.; Tang, M.Z.; Shen, B.B. Efficacy of N-Acetylcysteine in Preventing Acute Kidney Injury After Cardiac Surgery: A Meta-Analysis Study. J. Investig. Surg. 2018, 31, 14–23. [Google Scholar] [CrossRef]
- Leaf, D.E.; Rajapurkar, M.; Lele, S.S.; Mukhopadhyay, B.; Rawn, J.D.; Frendl, G.; Waikar, S.S. Increased plasma catalytic iron in patients may mediate acute kidney injury and death following cardiac surgery. Kidney Int. 2015, 87, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- Leaf, D.E.; Swinkels, D.W. Catalytic iron and acute kidney injury. Am. J. Physiol. Renal. Physiol. 2016, 311, F871–f876. [Google Scholar] [CrossRef]
- Tie, H.T.; Luo, M.Z.; Luo, M.J.; Zhang, M.; Wu, Q.C.; Wan, J.Y. Sodium bicarbonate in the prevention of cardiac surgery-associated acute kidney injury: A systematic review and meta-analysis. Crit. Care 2014, 18, 517. [Google Scholar] [CrossRef]
- Bailey, M.; McGuinness, S.; Haase, M.; Haase-Fielitz, A.; Parke, R.; Hodgson, C.L.; Forbes, A.; Bagshaw, S.M.; Bellomo, R. Sodium bicarbonate and renal function after cardiac surgery: A prospectively planned individual patient meta-analysis. Anesthesiology 2015, 122, 294–306. [Google Scholar] [CrossRef]
- Soh, S.; Song, J.W.; Shim, J.K.; Kim, J.H.; Kwak, Y.L. Sodium bicarbonate does not prevent postoperative acute kidney injury after off-pump coronary revascularization: A double-blinded randomized controlled trial. Br. J. Anaesth. 2016, 117, 450–457. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, J.H.; Kim, H.J.; Kim, J.Y.; Ahn, H.; Ahn, I.M.; Choe, W.J.; Lim, C.H. Meta-Analysis of Sodium Bicarbonate Therapy for Prevention of Cardiac Surgery-Associated Acute Kidney Injury. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1248–1256. [Google Scholar] [CrossRef] [PubMed]
- Ling, Q.; Gu, Y.; Chen, J.; Chen, Y.; Shi, Y.; Zhao, G.; Zhu, Q. Consequences of continuing renin angiotensin aldosterone system antagonists in the preoperative period: A systematic review and meta-analysis. BMC Anesthesiol. 2018, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Garg, A.X.; Swaminathan, M.; Garwood, S.; Hong, K.; Thiessen-Philbrook, H.; Passik, C.; Koyner, J.L.; Parikh, C.R. Preoperative angiotensin-converting enzyme inhibitors and angiotensin receptor blocker use and acute kidney injury in patients undergoing cardiac surgery. Nephrol. Dial. Transplant. 2013, 28, 2787–2799. [Google Scholar] [CrossRef]
- Hollmann, C.; Fernandes, N.L.; Biccard, B.M. A Systematic Review of Outcomes Associated With Withholding or Continuing Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Before Noncardiac Surgery. Anesth. Analg. 2018, 127, 678–687. [Google Scholar] [CrossRef]
- Fliser, D.; Laville, M.; Covic, A.; Fouque, D.; Vanholder, R.; Juillard, L.; Van Biesen, W. A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines on acute kidney injury: Part 1: Definitions, conservative management and contrast-induced nephropathy. Nephrol. Dial. Transplant. 2012, 27, 4263–4272. [Google Scholar] [PubMed]
- Demirjian, S.; Ailawadi, G.; Polinsky, M.; Bitran, D.; Silberman, S.; Shernan, S.K.; Burnier, M.; Hamilton, M.; Squiers, E.; Erlich, S.; et al. Safety and Tolerability Study of an Intravenously Administered Small Interfering Ribonucleic Acid (siRNA) Post On-Pump Cardiothoracic Surgery in Patients at Risk of Acute Kidney Injury. Kidney Int. Rep. 2017, 2, 836–843. [Google Scholar] [CrossRef]
- Cohen, P.; Goedert, M. GSK3 inhibitors: Development and therapeutic potential. Nat. Rev. Drug Discov. 2004, 3, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Bao, H.; Ge, Y.; Wang, Z.; Zhuang, S.; Dworkin, L.; Peng, A.; Gong, R. Delayed administration of a single dose of lithium promotes recovery from AKI. J. Am. Soc. Nephrol. 2014, 25, 488–500. [Google Scholar] [CrossRef]
- Sharif, S.; Chen, B.; Brewster, P.; Chen, T.; Dworkin, L.; Gong, R. Rationale and Design of Assessing the Effectiveness of Short-Term Low-Dose Lithium Therapy in Averting Cardiac Surgery-Associated Acute Kidney Injury: A Randomized, Double Blinded, Placebo Controlled Pilot Trial. Front. Med. 2021, 8, 639402. [Google Scholar] [CrossRef] [PubMed]
- Serraino, G.F.; Marsico, R.; Musolino, G.; Ventura, V.; Gulletta, E.; Santè, P.; Renzulli, A. Pulsatile cardiopulmonary bypass with intra-aortic balloon pump improves organ function and reduces endothelial activation. Circ. J. 2012, 76, 1121–1129. [Google Scholar] [CrossRef]
- Wang, J.; Yu, W.; Gao, M.; Gu, C.; Yu, Y. Preoperative Prophylactic Intraaortic Balloon Pump Reduces the Incidence of Postoperative Acute Kidney Injury and Short-Term Death of High-Risk Patients Undergoing Coronary Artery Bypass Grafting: A Meta-Analysis of 17 Studies. Ann. Thorac. Surg. 2016, 101, 2007–2019. [Google Scholar] [CrossRef]
- Lundemoen, S.; Kvalheim, V.L.; Svendsen, Ø.S.; Mongstad, A.; Andersen, K.S.; Grong, K.; Husby, P. Intraaortic counterpulsation during cardiopulmonary bypass impairs distal organ perfusion. Ann. Thorac. Surg. 2015, 99, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Paolasso, E.; Straka, Z.; Piegas, L.S.; Akar, A.R.; Jain, A.R.; et al. Effects of off-pump and on-pump coronary-artery bypass grafting at 1 year. N. Engl. J. Med. 2013, 368, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Straka, Z.; Piegas, L.S.; Avezum, A.; Akar, A.R.; Lanas Zanetti, F.; et al. Five-Year Outcomes after Off-Pump or On-Pump Coronary-Artery Bypass Grafting. N. Engl. J. Med. 2016, 375, 2359–2368. [Google Scholar] [CrossRef]
- Shroyer, A.L.; Grover, F.L.; Hattler, B.; Collins, J.F.; McDonald, G.O.; Kozora, E.; Lucke, J.C.; Baltz, J.H.; Novitzky, D. On-pump versus off-pump coronary-artery bypass surgery. N. Engl. J. Med. 2009, 361, 1827–1837. [Google Scholar] [CrossRef]
- Diegeler, A.; Börgermann, J.; Kappert, U.; Breuer, M.; Böning, A.; Ursulescu, A.; Rastan, A.; Holzhey, D.; Treede, H.; Rieß, F.C.; et al. Off-pump versus on-pump coronary-artery bypass grafting in elderly patients. N. Engl. J. Med. 2013, 368, 1189–1198. [Google Scholar] [CrossRef]
- Vedel, A.G.; Holmgaard, F.; Rasmussen, L.S.; Langkilde, A.; Paulson, O.B.; Lange, T.; Thomsen, C.; Olsen, P.S.; Ravn, H.B.; Nilsson, J.C. High-Target Versus Low-Target Blood Pressure Management During Cardiopulmonary Bypass to Prevent Cerebral Injury in Cardiac Surgery Patients: A Randomized Controlled Trial. Circulation 2018, 137, 1770–1780. [Google Scholar] [CrossRef]
- Ono, M.; Arnaoutakis, G.J.; Fine, D.M.; Brady, K.; Easley, R.B.; Zheng, Y.; Brown, C.; Katz, N.M.; Grams, M.E.; Hogue, C.W. Blood pressure excursions below the cerebral autoregulation threshold during cardiac surgery are associated with acute kidney injury. Crit. Care Med. 2013, 41, 464–471. [Google Scholar] [CrossRef]
- Joshi, B.; Ono, M.; Brown, C.; Brady, K.; Easley, R.B.; Yenokyan, G.; Gottesman, R.F.; Hogue, C.W. Predicting the limits of cerebral autoregulation during cardiopulmonary bypass. Anesth. Analg. 2012, 114, 503–510. [Google Scholar] [CrossRef]
- Ranucci, M.; Romitti, F.; Isgrò, G.; Cotza, M.; Brozzi, S.; Boncilli, A.; Ditta, A. Oxygen delivery during cardiopulmonary bypass and acute renal failure after coronary operations. Ann. Thorac. Surg. 2005, 80, 2213–2220. [Google Scholar] [CrossRef] [PubMed]
- Sievert, A.; Sistino, J. A meta-analysis of renal benefits to pulsatile perfusion in cardiac surgery. J. Extra-Corpor. Technol. 2012, 44, 10–14. [Google Scholar] [PubMed]
- Tyson, N.; Efthymiou, C. Predictive risk factors for intra-abdominal hypertension after cardiac surgery. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Mazzeffi, M.A.; Stafford, P.; Wallace, K.; Bernstein, W.; Deshpande, S.; Odonkor, P.; Grewal, A.; Strauss, E.; Stubbs, L.; Gammie, J.; et al. Intra-abdominal Hypertension and Postoperative Kidney Dysfunction in Cardiac Surgery Patients. J. Cardiothorac. Vasc. Anesth. 2016, 30, 1571–1577. [Google Scholar] [CrossRef]
- Svenmarker, S.; Häggmark, S.; Jansson, E.; Lindholm, R.; Appelblad, M.; Sandström, E.; Aberg, T. Use of heparin-bonded circuits in cardiopulmonary bypass improves clinical outcome. Scand. Cardiovasc. J. 2002, 36, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Isgrò, G.; Soro, G.; Canziani, A.; Menicanti, L.; Frigiola, A. Reduced systemic heparin dose with phosphorylcholine coated closed circuit in coronary operations. Int. J. Artif. Organs 2004, 27, 311–319. [Google Scholar] [CrossRef]
- Mangoush, O.; Purkayastha, S.; Haj-Yahia, S.; Kinross, J.; Hayward, M.; Bartolozzi, F.; Darzi, A.; Athanasiou, T. Heparin-bonded circuits versus nonheparin-bonded circuits: An evaluation of their effect on clinical outcomes. Eur. J. Cardio-Thorac. Surg. 2007, 31, 1058–1069. [Google Scholar] [CrossRef]
- Benedetto, U.; Luciani, R.; Goracci, M.; Capuano, F.; Refice, S.; Angeloni, E.; Roscitano, A.; Sinatra, R. Miniaturized cardiopulmonary bypass and acute kidney injury in coronary artery bypass graft surgery. Ann. Thorac. Surg. 2009, 88, 529–535. [Google Scholar] [CrossRef]
- Chew, S.T.; Ng, R.R.; Liu, W.; Goh, S.G.; Caleb, M.G.; Ti, L.K. Miniaturized versus conventional cardiopulmonary bypass and acute kidney injury after cardiac surgery. Perfusion 2016, 31, 60–67. [Google Scholar] [CrossRef]
- Bolisetty, S.; Agarwal, A. Neutrophils in acute kidney injury: Not neutral any more. Kidney Int. 2009, 75, 674–676. [Google Scholar] [CrossRef] [PubMed]
- Scrascia, G.; Guida, P.; Rotunno, C.; de Luca Tupputi Schinosa, L.; Paparella, D. Anti-inflammatory strategies to reduce acute kidney injury in cardiac surgery patients: A meta-analysis of randomized controlled trials. Artif. Organs 2014, 38, 101–112. [Google Scholar] [CrossRef]
- Spencer, S.; Tang, A.; Khoshbin, E. Leukodepletion for patients undergoing heart valve surgery. Cochrane Database Syst. Rev. 2013, Cd009507. [Google Scholar] [CrossRef]
- Karim, H.M.; Yunus, M.; Saikia, M.K.; Kalita, J.P.; Mandal, M. Incidence and progression of cardiac surgery-associated acute kidney injury and its relationship with bypass and cross clamp time. Ann. Card. Anaesth. 2017, 20, 22–27. [Google Scholar]
- Rosner, M.H.; Okusa, M.D. Acute kidney injury associated with cardiac surgery. Clin. J. Am. Soc. Nephrol. CJASN 2006, 1, 19–32. [Google Scholar] [CrossRef]
- Heyman, S.N.; Leibowitz, D.; Mor-Yosef Levi, I.; Liberman, A.; Eisenkraft, A.; Alcalai, R.; Khamaisi, M.; Rosenberger, C. Adaptive response to hypoxia and remote ischaemia pre-conditioning: A new hypoxia-inducible factors era in clinical medicine. Acta Physiol. 2016, 216, 395–406. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Candilio, L.; Evans, R.; Ariti, C.; Jenkins, D.P.; Kolvekar, S.; Knight, R.; Kunst, G.; Laing, C.; Nicholas, J.; et al. Remote Ischemic Preconditioning and Outcomes of Cardiac Surgery. N. Engl. J. Med. 2015, 373, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Meybohm, P.; Bein, B.; Brosteanu, O.; Cremer, J.; Gruenewald, M.; Stoppe, C.; Coburn, M.; Schaelte, G.; Böning, A.; Niemann, B.; et al. A Multicenter Trial of Remote Ischemic Preconditioning for Heart Surgery. N. Engl. J. Med. 2015, 373, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- Zarbock, A.; Kellum, J.A.; Schmidt, C.; Van Aken, H.; Wempe, C.; Pavenstädt, H.; Boanta, A.; Gerß, J.; Meersch, M. Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial. JAMA 2016, 315, 2190–2199. [Google Scholar] [CrossRef]
- Deferrari, G.; Bonanni, A.; Bruschi, M.; Alicino, C.; Signori, A. Remote ischaemic preconditioning for renal and cardiac protection in adult patients undergoing cardiac surgery with cardiopulmonary bypass: Systematic review and meta-analysis of randomized controlled trials. Nephrol. Dial. Transplant. 2018, 33, 813–824. [Google Scholar] [CrossRef]
- Xie, J.; Zhang, X.; Xu, J.; Zhang, Z.; Klingensmith, N.J.; Liu, S.; Pan, C.; Yang, Y.; Qiu, H. Effect of Remote Ischemic Preconditioning on Outcomes in Adult Cardiac Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Studies. Anesth. Analg. 2018, 127, 30–38. [Google Scholar] [CrossRef]
- Lee, H.T.; Ota-Setlik, A.; Fu, Y.; Nasr, S.H.; Emala, C.W. Differential protective effects of volatile anesthetics against renal ischemia-reperfusion injury in vivo. Anesthesiology 2004, 101, 1313–1324. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.C.; Shim, J.K.; Song, Y.; Yang, S.Y.; Kwak, Y.L. Anesthetics influence the incidence of acute kidney injury following valvular heart surgery. Kidney Int. 2014, 86, 414–422. [Google Scholar] [CrossRef]
- Landoni, G.; Lomivorotov, V.V.; Nigro Neto, C.; Monaco, F.; Pasyuga, V.V.; Bradic, N.; Lembo, R.; Gazivoda, G.; Likhvantsev, V.V.; Lei, C.; et al. Volatile Anesthetics versus Total Intravenous Anesthesia for Cardiac Surgery. N. Engl. J. Med. 2019, 380, 1214–1225. [Google Scholar] [CrossRef]
- Bonanni, A.; Signori, A.; Alicino, C.; Mannucci, I.; Grasso, M.A.; Martinelli, L.; Deferrari, G. Volatile Anesthetics versus Propofol for Cardiac Surgery with Cardiopulmonary Bypass: Meta-analysis of Randomized Trials. Anesthesiology 2020, 132, 1429–1446. [Google Scholar] [CrossRef] [PubMed]
- Si, Y.; Bao, H.; Han, L.; Shi, H.; Zhang, Y.; Xu, L.; Liu, C.; Wang, J.; Yang, X.; Vohra, A.; et al. Dexmedetomidine protects against renal ischemia and reperfusion injury by inhibiting the JAK/STAT signaling activation. J. Transl. Med. 2013, 11, 141. [Google Scholar] [CrossRef]
- Gu, J.; Sun, P.; Zhao, H.; Watts, H.R.; Sanders, R.D.; Terrando, N.; Xia, P.; Maze, M.; Ma, D. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit. Care 2011, 15, R153. [Google Scholar] [CrossRef]
- Peng, K.; Li, D.; Applegate, R.L., II; Lubarsky, D.A.; Ji, F.H.; Liu, H. Effect of Dexmedetomidine on Cardiac Surgery-Associated Acute Kidney Injury: A Meta-Analysis With Trial Sequential Analysis of Randomized Controlled Trials. J. Cardiothorac. Vasc. Anesth. 2020, 34, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sheng, B.; Wang, S.; Lu, F.; Zhen, J.; Chen, W. Dexmedetomidine prevents acute kidney injury after adult cardiac surgery: A meta-analysis of randomized controlled trials. BMC Anesthesiol. 2018, 18, 7. [Google Scholar] [CrossRef]
- Haase-Fielitz, A.; Haase, M.; Bellomo, R.; Calzavacca, P.; Spura, A.; Baraki, H.; Kutschka, I.; Albert, C. Perioperative Hemodynamic Instability and Fluid Overload are Associated with Increasing Acute Kidney Injury Severity and Worse Outcome after Cardiac Surgery. Blood Purif. 2017, 43, 298–308. [Google Scholar] [CrossRef]
- Shen, Y.; Zhang, W.; Cheng, X.; Ying, M. Association between postoperative fluid balance and acute kidney injury in patients after cardiac surgery: A retrospective cohort study. J. Crit. Care 2018, 44, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Bellomo, R.; Burdmann, E.A.; Doi, K.; Endre, Z.H.; Goldstein, S.L.; Kane-Gill, S.L.; Liu, K.D.; Prowle, J.R.; Shaw, A.D.; et al. Controversies in acute kidney injury: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. 2020, 98, 294–309. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Liu, K.; Kashani, K. Fluid Management in Acute Kidney Injury. Chest 2019, 156, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, M.L.; Raghunathan, K.; Paluszkiewicz, S.M.; Schermer, C.R.; Shaw, A.D. Meta-analysis of high- versus low-chloride content in perioperative and critical care fluid resuscitation. Br. J. Surg. 2015, 102, 24–36. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Arumugam, G.; Vinay Kumar, P.V. A prospective, randomized, comparison study on effect of perioperative use of chloride liberal intravenous fluids versus chloride restricted intravenous fluids on postoperative acute kidney injury in patients undergoing off-pump coronary artery bypass grafting surgeries. Ann. Card. Anaesth. 2018, 21, 413–418. [Google Scholar]
- Thomson, R.; Meeran, H.; Valencia, O.; Al-Subaie, N. Goal-directed therapy after cardiac surgery and the incidence of acute kidney injury. J. Crit. Care 2014, 29, 997–1000. [Google Scholar] [CrossRef]
- Magruder, J.T.; Crawford, T.C.; Harness, H.L.; Grimm, J.C.; Suarez-Pierre, A.; Wierschke, C.; Biewer, J.; Hogue, C.; Whitman, G.R.; Shah, A.S.; et al. A pilot goal-directed perfusion initiative is associated with less acute kidney injury after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2017, 153, 118–125.e1. [Google Scholar] [CrossRef] [PubMed]
- Oprea, A.D.; Del Rio, J.M.; Cooter, M.; Green, C.L.; Karhausen, J.A.; Nailer, P.; Guinn, N.R.; Podgoreanu, M.V.; Stafford-Smith, M.; Schroder, J.N.; et al. Pre- and postoperative anemia, acute kidney injury, and mortality after coronary artery bypass grafting surgery: A retrospective observational study. Can. J. Anaesth. 2018, 65, 46–59. [Google Scholar] [CrossRef]
- Khan, U.A.; Coca, S.G.; Hong, K.; Koyner, J.L.; Garg, A.X.; Passik, C.S.; Swaminathan, M.; Garwood, S.; Patel, U.D.; Hashim, S.; et al. Blood transfusions are associated with urinary biomarkers of kidney injury in cardiac surgery. J. Thorac. Cardiovasc. Surg. 2014, 148, 726–732. [Google Scholar] [CrossRef]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Médicis, É.; McGuinness, S.; et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery. N. Engl. J. Med. 2017, 377, 2133–2144. [Google Scholar] [CrossRef]
- Reeves, B.C.; Pike, K.; Rogers, C.A.; Brierley, R.C.; Stokes, E.A.; Wordsworth, S.; Nash, R.L.; Miles, A.; Mumford, A.D.; Cohen, A.; et al. A multicentre randomised controlled trial of Transfusion Indication Threshold Reduction on transfusion rates, morbidity and health-care resource use following cardiac surgery (TITRe2). Health Technol. Assess. 2016, 20, 1–260. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, J.U.; Lancé, M.D.; de Korte, M.; Artmann, T.; Aleksic, I.; Kranke, P. The effect of different lung-protective strategies in patients during cardiopulmonary bypass: A meta-analysis and semiquantitative review of randomized trials. J. Cardiothorac. Vasc. Anesth. 2012, 26, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Joannidis, M.; Forni, L.G.; Klein, S.J.; Honore, P.M.; Kashani, K.; Ostermann, M.; Prowle, J.; Bagshaw, S.M.; Cantaluppi, V.; Darmon, M.; et al. Lung-kidney interactions in critically ill patients: Consensus report of the Acute Disease Quality Initiative (ADQI) 21 Workgroup. Intensive Care Med. 2020, 46, 654–672. [Google Scholar] [CrossRef]
- Smith, M.N.; Best, D.; Sheppard, S.V.; Smith, D.C. The effect of mannitol on renal function after cardiopulmonary bypass in patients with established renal dysfunction. Anaesthesia 2008, 63, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Yallop, K.G.; Sheppard, S.V.; Smith, D.C. The effect of mannitol on renal function following cardio-pulmonary bypass in patients with normal pre-operative creatinine. Anaesthesia 2008, 63, 576–582. [Google Scholar] [CrossRef]
- Fakhari, S.; Bavil, F.M.; Bilehjani, E.; Abolhasani, S.; Mirinazhad, M.; Naghipour, B. Prophylactic furosemide infusion decreasing early major postoperative renal dysfunction in on-pump adult cardiac surgery: A randomized clinical trial. Res. Rep. Urol. 2017, 9, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Bayat, F.; Faritous, Z.; Aghdaei, N.; Dabbagh, A. A study of the efficacy of furosemide as a prophylaxis of acute renal failure in coronary artery bypass grafting patients: A clinical trial. ARYA Atheroscler. 2015, 11, 173–178. [Google Scholar]
- Nigwekar, S.U.; Navaneethan, S.D.; Parikh, C.R.; Hix, J.K. Atrial natriuretic peptide for preventing and treating acute kidney injury. Cochrane Database Syst. Rev. 2009, Cd006028. [Google Scholar] [CrossRef]
- Gillies, M.A.; Kakar, V.; Parker, R.J.; Honoré, P.M.; Ostermann, M. Fenoldopam to prevent acute kidney injury after major surgery-a systematic review and meta-analysis. Crit. Care 2015, 19, 449. [Google Scholar] [CrossRef]
- Sun, H.; Xie, Q.; Peng, Z. Does Fenoldopam Protect Kidney in Cardiac Surgery? A Systemic Review and Meta-Analysis With Trial Sequential Analysis. Shock 2019, 52, 326–333. [Google Scholar] [CrossRef]
- Bove, T.; Zangrillo, A.; Guarracino, F.; Alvaro, G.; Persi, B.; Maglioni, E.; Galdieri, N.; Comis, M.; Caramelli, F.; Pasero, D.C.; et al. Effect of fenoldopam on use of renal replacement therapy among patients with acute kidney injury after cardiac surgery: A randomized clinical trial. JAMA 2014, 312, 2244–2253. [Google Scholar] [CrossRef] [PubMed]
- Küllmar, M.; Weiß, R.; Ostermann, M.; Campos, S.; Grau Novellas, N.; Thomson, G.; Haffner, M.; Arndt, C.; Wulf, H.; Irqsusi, M.; et al. A Multinational Observational Study Exploring Adherence with the Kidney Disease: Improving Global Outcomes Recommendations for Prevention of Acute Kidney Injury After Cardiac Surgery. Anesth. Analg. 2020, 130, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; et al. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit. Care 2013, 17, R25. [Google Scholar] [CrossRef]
- Ostermann, M.; Wu, V.; Sokolov, D.; Lumlertgul, N. Definitions of acute renal dysfunction: An evolving clinical and biomarker paradigm. Curr. Opin. Crit. Care 2021, 27, 553. [Google Scholar] [CrossRef] [PubMed]
- Choon, X.Y.; Lumlertgul, N.; Cameron, L.; Jones, A.; Meyer, J.; Slack, A.; Vollmer, H.; Barrett, N.A.; Leach, R.; Ostermann, M. Discharge Documentation and Follow-Up of Critically Ill Patients With Acute Kidney Injury Treated With Kidney Replacement Therapy: A Retrospective Cohort Study. Front. Med. 2021, 8, 710228. [Google Scholar] [CrossRef]


{kind=link}
| Component of KDIGO Care Bundle | Rationale for Nephroprotection |
|---|---|
| Close monitoring of renal function | Close and regular monitoring is required to ensure early the diagnosis of AKI. Whilst the exact intervals for checking serum creatinine are not defined, close monitoring of renal function after cardiac surgery is strongly recommended. |
| Functional haemodynamic monitoring | Several studies have confirmed that cardiac output, systemic oxygen delivery, central venous pressure and systemic haemodynamics are associated with risk of AKI. Functional haemodynamic monitoring allows the early identification of high-risk patients and opportunities for early intervention. |
| Optimising fluid status and haemodynamics | Both severity and duration of intraoperative hypotension are strong risk factors for postoperative AKI. Similarly, both hypo- and hypervolaemia are associated with an increased risk of AKI. Although the target blood pressure in individual patients and the optimal type and volume of fluid to prevent AKI have not been identified yet, the detection of hypotension and hypo- or hypervolaemia should prompt immediate resuscitation. |
| Avoidance of hyperglycaemia | Uncontrolled hyperglycaemia significantly increases the incidence of AKI post cardiac surgery via multiple pathways, including the increased production of inflammatory cytokines, the overproduction of superoxide by the mitochondrial electron transport chain, and osmotic diuresis. Conversely, intensive glycaemic control can have adverse effects. |
| Avoidance of radiocontrast and discontinuation of nephrotoxic medications | Many medications, including radiocontrast media, are risk factors for the development of AKI due to mechanisms such as reduced glomerular perfusion, tubular cell toxicity, intratubular crystal formation and the alteration of the tubular microcirculation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostermann, M.; Kunst, G.; Baker, E.; Weerapolchai, K.; Lumlertgul, N. Cardiac Surgery Associated AKI Prevention Strategies and Medical Treatment for CSA-AKI. J. Clin. Med. 2021, 10, 5285. https://doi.org/10.3390/jcm10225285
Ostermann M, Kunst G, Baker E, Weerapolchai K, Lumlertgul N. Cardiac Surgery Associated AKI Prevention Strategies and Medical Treatment for CSA-AKI. Journal of Clinical Medicine. 2021; 10(22):5285. https://doi.org/10.3390/jcm10225285
Chicago/Turabian StyleOstermann, Marlies, Gudrun Kunst, Eleanor Baker, Kittisak Weerapolchai, and Nuttha Lumlertgul. 2021. "Cardiac Surgery Associated AKI Prevention Strategies and Medical Treatment for CSA-AKI" Journal of Clinical Medicine 10, no. 22: 5285. https://doi.org/10.3390/jcm10225285
APA StyleOstermann, M., Kunst, G., Baker, E., Weerapolchai, K., & Lumlertgul, N. (2021). Cardiac Surgery Associated AKI Prevention Strategies and Medical Treatment for CSA-AKI. Journal of Clinical Medicine, 10(22), 5285. https://doi.org/10.3390/jcm10225285