
Methods Used to Evaluate the Immediate Effects of Airway Clearance Techniques in Adults with Cystic Fibrosis: A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Criteria
2.2. Search Procedure
2.3. Screening
2.4. Data Extraction and Coding
2.5. Risk of Bias
2.6. Data Analysis
2.7. Exploratory Analysis
3. Results
3.1. Study Characteristics
3.2. Coding According to Mechanism of Action
3.3. Description of Outcomes
3.4. Magnitude of Between-Group Change
3.5. Magnitude of Within-Group Change
3.5.1. Sputum Expectoration
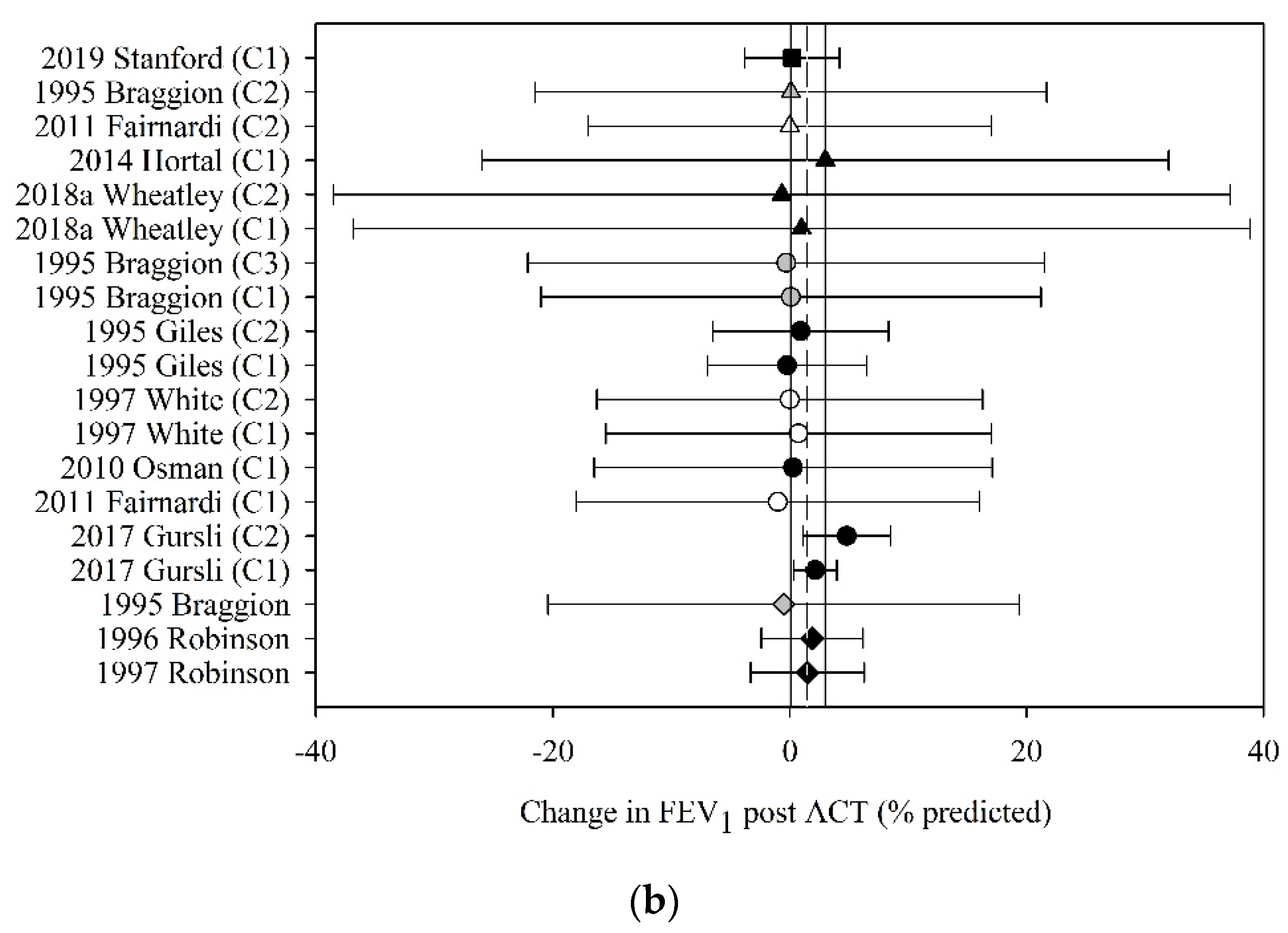
3.5.2. Spirometric Measures of Lung Function
3.5.3. Static Lung Volumes
3.5.4. Other Outcomes
4. Discussion
Strengths, Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A. Example Search Strategy for PubMed
References
- Elborn, J.S. Cystic fibrosis. Lancet 2016, 388, 2519–2531. [Google Scholar] [CrossRef]
- Rafeeq, M.M.; Murad, H.A.S. Cystic fibrosis: Current therapeutic targets and future approaches. J. Transl. Med. 2017, 15, 84. [Google Scholar] [CrossRef] [PubMed]
- Ruseckaite, R.; Ahern, S.; Ranger, T.; Tacey, M.; Dean, J.; Gardam, M.; Bell, S.; Burke, N. The Australian Cystic Fibrosis Data Registry Annual Report, 2016; Monash University, Department of Epidemiology and Preventive Medicine: Melbourne, Australia, 2018. [Google Scholar]
- Cohen-Cymberknoh, M.; Shoseyov, D.; Kerem, E. Managing cystic fibrosis: Strategies that increase life expectancy and improve quality of life. Am. J. Respir. Crit. Care Med. 2011, 183, 1463–1471. [Google Scholar] [CrossRef]
- Wilson, L.M.; Morrison, L.; Robinson, K.A. Airway clearance techniques for cystic fibrosis: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2019, 1, CD011231. [Google Scholar] [CrossRef]
- Button, B.M.; Wilson, C.; Dentice, R.; Cox, N.S.; Middleton, A.; Tannenbaum, E.; Bishop, J.; Cobb, R.; Burton, K.; Wood, M.; et al. Physiotherapy for cystic fibrosis in Australia and New Zealand: A clinical practice guideline. Respirology 2016, 21, 656–667. [Google Scholar] [CrossRef]
- Osadnik, C.R.; McDonald, C.F.; Holland, A.E. Airway clearance techniques in acute exacerbations of COPD: A survey of Australian physiotherapy practice. Physiotherapy 2013, 99, 101–106. [Google Scholar] [CrossRef]
- Ward, N.; Stiller, K.; Holland, A.E. Exercise is commonly used as a substitute for traditional airway clearance techniques by adults with cystic fibrosis in Australia: A survey. J. Physiother. 2019, 65, 43–50. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Guideline on the Clinical Development of Medicinal Products for the Treatment of Cystic Fibrosis; European Medicines Agency: London, UK, 2009. [Google Scholar]
- U.S. Food and Drug Administration. Table of Surrogate Endpoints That Were the Basis of Drug Approval or Licensure. Available online: https://www.fda.gov/drugs/development-resources/table-surrogate-endpoints-were-basis-drug-approval-or-licensure (accessed on 1 June 2021).
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia; Available online: https://www.covidence.org/home (accessed on 20 October 2019).
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Review Manager Web (RevMan Web). Version 3.1.2. 2021. Available online: https://revman.cochrane.org/#/myReviews (accessed on 3 March 2021).
- Morrison, L.; Milroy, S. Oscillating devices for airway clearance in people with cystic fibrosis. Cochrane Database Syst. Rev. 2020, 4, CD006842. [Google Scholar] [CrossRef]
- Warnock, L.; Gates, A. Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis. Cochrane Database Syst. Rev. 2015, 12, CD001401. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.M.; Moran, F.M.; Stuart Elborn, J. Evidence for physical therapies (airway clearance and physical training) in cystic fibrosis: An overview of five Cochrane systematic reviews. Respir. Med. 2006, 100, 191–201. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 48. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Cochrane: London, UK, 2021. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- App, E.M.; Kieselmann, R.; Reinhardt, D.; Lindemann, H.; Dasgupta, B.; King, M.; Brand, P. Sputum rheology changes in cystic fibrosis lung disease following two different types of physiotherapy: Flutter vs. autogenic drainage. Chest 1998, 114, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Aquino, E.S.; Shimura, F.; Santos, A.S.; Goto, D.M.; Coelho, C.C.; de Fuccio, M.B.; Saldiva, P.H.; Lorenzi-Filho, G.; Rubin, B.K.; Nakagawa, N.K. CPAP has no effect on clearance, sputum properties, or expectorated volume in cystic fibrosis. Respir. Care 2012, 57, 1914–1919. [Google Scholar] [CrossRef]
- Arens, R.; Gozal, D.; Omlin, K.J.; Vega, J.; Boyd, K.P.; Keens, T.G.; Woo, M.S. Comparison of high frequency chest compression and conventional chest physiotherapy in hospitalized patients with cystic fibrosis. Am. J. Respir. Crit. Care Med. 1994, 150, 1154–1157. [Google Scholar] [CrossRef]
- Baldwin, D.R.; Hill, A.L.; Peckham, D.G.; Knox, A.J. Effect of addition of exercise to chest physiotherapy on sputum expectoration and lung function in adults with cystic fibrosis. Respir. Med. 1994, 88, 49–53. [Google Scholar] [CrossRef][Green Version]
- Bilton, D.; Dodd, M.E.; Abbot, J.V.; Webb, A.K. The benefits of exercise combined with physiotherapy in the treatment of adults with cystic fibrosis. Respir. Med. 1992, 86, 507–511. [Google Scholar] [CrossRef]
- Bishop, J.R.; Erskine, O.J.; Middleton, P.G. Timing of dornase alpha inhalation does not affect the efficacy of an airway clearance regimen in adults with cystic fibrosis: A randomised crossover trial. J. Physiother. 2011, 57, 223–229. [Google Scholar] [CrossRef]
- Borka, P.; Gyurkovits, K.; Bodis, J. Comparative study of PEP mask and Flutter on expectoration in cystic fibrosis patients. Acta Physiol. Hung. 2012, 99, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Braggion, C.; Cappelletti, L.M.; Cornacchia, M.; Zanolla, L.; Mastella, G. Short-term effects of three chest physiotherapy regimens in patients hospitalized for pulmonary exacerbations of cystic fibrosis: A cross-over randomized study. Pediatr. Pulmonol. 1995, 19, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Cantin, A.M.; Bacon, M.; Berthiaume, Y. Mechanical airway clearance using the Frequencer electro-acoustical transducer in cystic fibrosis. Clin. Investig. Med. 2006, 29, 159–165. [Google Scholar]
- Carr, L.; Pryor, J.A.; Hodson, M.E. Self chest clapping Patients’ views and the effects on oxygen saturation. Physiotherapy 1995, 81, 753–757. [Google Scholar] [CrossRef]
- Chatham, K.; Ionescu, A.A.; Nixon, L.S.; Shale, D.J. A short-term comparison of two methods of sputum expectoration in cystic fibrosis. Eur. Respir. J. 2004, 23, 435–439. [Google Scholar] [CrossRef]
- Darbee, J.C.; Ohtake, P.J.; Grant, B.J.; Cerny, F.J. Physiologic evidence for the efficacy of positive expiratory pressure as an airway clearance technique in patients with cystic fibrosis. Phys. Ther. 2004, 84, 524–537. [Google Scholar] [CrossRef]
- DeCesare, J.A.; Babchyck, B.M.; Colten, H.R.; Treves, S. Radionuclide assessment of the effects of chest physical therapy on ventilation in cystic fibrosis. Phys. Ther. 1982, 62, 820–827. [Google Scholar] [CrossRef]
- Dwyer, T.J.; Alison, J.A.; McKeough, Z.J.; Daviskas, E.; Bye, P.T.; Dwyer, T.J.; Alison, J.A.; McKeough, Z.J.; Daviskas, E.; Bye, P.T.P. Effects of exercise on respiratory flow and sputum properties in patients with cystic fibrosis. Chest 2011, 139, 870–877. [Google Scholar] [CrossRef]
- Dwyer, T.J.; Robbins, L.; Kelly, P.; Piper, A.J.; Bell, S.C.; Bye, P.T. Non-invasive ventilation used as an adjunct to airway clearance treatments improves lung function during an acute exacerbation of cystic fibrosis: A randomised trial. J. Physiother. 2015, 61, 142–147. [Google Scholar] [CrossRef]
- Dwyer, T.J.; Zainuldin, R.; Daviskas, E.; Bye, P.T.; Alison, J.A. Effects of treadmill exercise versus Flutter(R) on respiratory flow and sputum properties in adults with cystic fibrosis: A randomised, controlled, cross-over trial. BMC Pulm. Med. 2017, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, T.J.; Daviskas, E.; Zainuldin, R.; Verschuer, J.; Eberl, S.; Bye, P.T.P.; Alison, J.A. Effects of exercise and airway clearance (positive expiratory pressure) on mucus clearance in cystic fibrosis: A randomised crossover trial. Eur. Resp. J. 2019, 53, 1801793. [Google Scholar] [CrossRef] [PubMed]
- Fainardi, V.; Longo, F.; Faverzani, S.; Tripodi, M.C.; Chetta, A.; Pisi, G. Short-term effects of high-frequency chest compression and positive expiratory pressure in patients with cystic fibrosis. J. Clin. Med. Res. 2011, 3, 279–284. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Falk, M.; Kelstrup, M.; Andersen, J.B.; Kinoshita, T.; Falk, P.; Stovring, S.; Gothgen, I. Improving the ketchup bottle method with positive expiratory pressure, PEP, in cystic fibrosis. Eur. J. Respir. Dis. 1984, 65, 423–432. [Google Scholar]
- Giles, D.R.; Wagener, J.S.; Accurso, F.J.; Butler-Simon, N. Short-term effects of postural drainage with clapping vs. autogenic drainage on oxygen saturation and sputum recovery in patients with cystic fibrosis. Chest 1995, 108, 952–954. [Google Scholar] [CrossRef][Green Version]
- Grosse-Onnebrink, J.; Mellies, U.; Olivier, M.; Werner, C.; Stehling, F. Chest physiotherapy can affect the lung clearance index in cystic fibrosis patients. Pediatr. Pulmonol. 2017, 52, 625–631. [Google Scholar] [CrossRef]
- Guimaraes, F.S.; Lopes, A.J.; Moco, V.J.R.; de Souza, F.C.; de Menezes, S.L.S. Eltgol acutely improves airway clearance and reduces static pulmonary volumes in adult cystic fibrosis patients. J. Phys. Ther. Sci. 2014, 26, 813–816. [Google Scholar] [CrossRef][Green Version]
- Gursli, S.; Sandvik, L.; Bakkeheim, E.; Skrede, B.; Stuge, B. Evaluation of a novel technique in airway clearance therapy—Specific cough technique (SCT) in cystic fibrosis: A pilot study of a series of N-of-1 randomised controlled trials. SAGE Open Med. 2017, 5, 2050312117697505. [Google Scholar] [CrossRef]
- Helper, N.; Kodesh, E.; Sokol, G.; Hakimi, R.; Vilozni, D.; Efrati, O. The benefits of mechanical insufflator-exsufflator compared to autogenic drainage in adults with cystic fibrosis. Pediatr. Pulmonol. 2020, 55, 3046–3052. [Google Scholar] [CrossRef]
- Hofmeyr, J.L.; Webber, B.A.; Hodson, M.E. Evaluation of positive expiratory pressure as an adjunct to chest physiotherapy in the treatment of cystic fibrosis. Thorax 1986, 41, 951–954. [Google Scholar] [CrossRef]
- Holland, A.E.; Denehy, L.; Ntoumenopoulos, G.; Naughton, M.T.; Wilson, J.W. Non-invasive ventilation assists chest physiotherapy in adults with acute exacerbations of cystic fibrosis. Thorax 2003, 58, 880–884. [Google Scholar] [CrossRef]
- Hordvik, N.L.; Sammut, P.H.; Judy, C.G.; Strizek, S.J.; Colombo, J.L. The effects of albuterol on the lung function of hospitalized patients with cystic fibrosis. Am. J. Respir. Crit. Care Med. 1996, 154, 156–160. [Google Scholar] [CrossRef]
- Hortal, M.C.R.; Hjelte, L. Time point to perform lung function tests evaluating the effects of an airway clearance therapy session in cystic fibrosis. Respir. Care 2014, 59, 1537–1541. [Google Scholar] [CrossRef]
- Jarad, N.A.; Powell, T.; Smith, E. Evaluation of a novel sputum clearance technique-hydro-acoustic therapy (HAT) in adult patients with cystic fibrosis: A feasibility study. Chronic Respir. Dis. 2010, 7, 217–227. [Google Scholar] [CrossRef]
- Kempainen, R.R.; Williams, C.B.; Hazelwood, A.; Rubin, B.K.; Milla, C.E. Comparison of high-frequency chest wall oscillation with differing waveforms for airway clearance in cystic fibrosis. Chest 2007, 132, 1227–1232. [Google Scholar] [CrossRef]
- Kempainen, R.R.; Milla, C.; Dunitz, J.; Savik, K.; Hazelwood, A.; Williams, C.; Rubin, B.K.; Billings, J.L. Comparison of settings used for high-frequency chest-wall compression in cystic fibrosis. Respir. Care 2010, 55, 695–701. [Google Scholar]
- Konstan, M.W.; Stern, R.C.; Doershuk, C.F. Efficacy of the Flutter device for airway mucus clearance in patients with cystic fibrosis. J. Pediatr. 1994, 124, 689–693. [Google Scholar] [CrossRef]
- Kriemler, S.; Radtke, T.; Christen, G.; Kerstan-Huber, M.; Hebestreit, H. Short-Term Effect of Different Physical Exercises and Physiotherapy Combinations on Sputum Expectoration, Oxygen Saturation, and Lung Function in Young Patients with Cystic Fibrosis. Lung 2016, 194, 659–664. [Google Scholar] [CrossRef]
- Lannefors, L.; Wollmer, P. Mucus clearance with three chest physiotherapy regimes in cystic fibrosis: A comparison between postural drainage, PEP and physical exercise. Eur. Respir. J. 1992, 5, 748–753. [Google Scholar]
- Leemans, G.; Belmans, D.; Van Holsbeke, C.; Becker, B.; Vissers, D.; Ides, K.; Verhulst, S.; Van Hoorenbeeck, K. The effectiveness of a mobile high-frequency chest wall oscillation (HFCWO) device for airway clearance. Pediatr. Pulmonol. 2020, 55, 1984–1992. [Google Scholar] [CrossRef]
- Lyons, E.; Chatham, K.; Campbell, I.A.; Prescott, R.J. Evaluation of the flutter VRP1 device in young adults with cystic fibrosis. Med. Sci. Res. 1993, 21, 101–102. [Google Scholar]
- McCarren, B.; Alison, J.A. Physiological effects of vibration in subjects with cystic fibrosis. Eur. Respir. J. 2006, 27, 1204–1209. [Google Scholar] [CrossRef]
- Mentore, K.; Froh, D.K.; de Lange, E.E.; Brookeman, J.R.; Paget-Brown, A.O.; Altes, T.A. Hyperpolarized HHe 3 MRI of the lung in cystic fibrosis: Assessment at baseline and after bronchodilator and airway clearance treatment. Acad. Radiol. 2005, 12, 1423–1429. [Google Scholar] [CrossRef]
- Milne, S.M.; Eales, C.J. A pilot study comparing two physiotherapy techniques in patients with cystic fibrosis. S. Afr. J. Physiother. 2004, 60, 3. [Google Scholar] [CrossRef][Green Version]
- Mortensen, J.; Falk, M.; Groth, S.; Jensen, C. The effects of postural drainage and positive expiratory pressure physiotherapy on tracheobronchial clearance in cystic fibrosis. Chest 1991, 100, 1350–1357. [Google Scholar] [CrossRef][Green Version]
- Murphy, M.B.; Concannon, D.; FitzGerald, M.X. Chest percussion: Help or hindrance to postural drainage? Ir. Med. J. 1983, 76, 189–190. [Google Scholar]
- O’Neill, K.; Moran, F.; Tunney, M.M.; Elborn, J.S.; Bradbury, I.; Downey, D.G.; Rendall, J.; Bradley, J.M. Timing of hypertonic saline and airway clearance techniques in adults with cystic fibrosis during pulmonary exacerbation: Pilot data from a randomised crossover study. BMJ Open Respir. Res. 2017, 4, e000168. [Google Scholar] [CrossRef]
- Osman, L.P.; Roughton, M.; Hodson, M.E.; Pryor, J.A. Short-term comparative study of high frequency chest wall oscillation and European airway clearance techniques in patients with cystic fibrosis. Thorax 2010, 65, 196–200. [Google Scholar] [CrossRef]
- Pfleger, A.; Steinbacher, M.; Schwantzer, G.; Weinhandl, E.; Wagner, M.; Eber, E. Short-term effects of physiotherapy on ventilation inhomogeneity in cystic fibrosis patients with a wide range of lung disease severity. J. Cyst. Fibros. 2015, 14, 627–631. [Google Scholar] [CrossRef][Green Version]
- Placidi, G.; Cornacchia, M.; Polese, G.; Zanolla, L.; Assael, B.M.; Braggion, C. Chest physiotherapy with positive airway pressure: A pilot study of short-term effects on sputum clearance in patients with cystic fibrosis and severe airway obstruction. Respir. Care 2006, 51, 1145–1153. [Google Scholar]
- Pryor, J.A.; Webber, B.A.; Hodson, M.E.; Batten, J.C. Evaluation of the forced expiration technique as an adjunct to postural drainage in treatment of cystic fibrosis. Br. Med. J. 1979, 2, 417–418. [Google Scholar] [CrossRef]
- Pryor, J.A.; Webber, B.A. An evaluation of the forced expiration technique as an adjunct to postural drainage. Physiotherapy 1979, 65, 304–307. [Google Scholar]
- Pryor, J.A.; Parker, R.A.; Webber, B.A. A comparison of mechanical and manual percussion as adjuncts to postural drainage in the treatment of cystic fibrosis in adolescents and adults. Physiotherapy 1981, 67, 140–141. [Google Scholar]
- Pryor, J.A.; Webber, B.A.; Hodson, M.E. Effect of chest physiotherapy on oxygen saturation in patients with cystic fibrosis. Thorax 1990, 45, 77. [Google Scholar] [CrossRef][Green Version]
- Pryor, J.A.; Webber, B.A.; Hodson, M.E.; Warner, J.O. The Flutter VRP1 as an adjunct to chest physiotherapy in cystic fibrosis. Respir. Med. 1994, 88, 677–681. [Google Scholar] [CrossRef]
- Radtke, T.; Boeni, L.; Bohnacker, P.; Maggi-Bebba, M.; Fischer, P.; Kriemler, S.; Benden, C.; Dressel, H. Acute effects of combined exercise and oscillatory positive expiratory pressure therapy on sputum properties and lung diffusing capacity in cystic fibrosis: A randomized, controlled, crossover trial. Eur. Respir. J. 2018, 52, PA3418. [Google Scholar] [CrossRef]
- Robinson, M.; Regnis, J.A.; Bailey, D.L.; King, M.; Bautovich, G.J.; Bye, P.T. Effect of hypertonic saline, amiloride, and cough on mucociliary clearance in patients with cystic fibrosis. Am. J. Respir. Crit. Care Med. 1996, 153, 1503–1509. [Google Scholar] [CrossRef]
- Robinson, M.; Hemming, A.L.; Regnis, J.A.; Wong, A.G.; Bailey, D.L.; Bautovich, G.J.; King, M.; Bye, P.T. Effect of increasing doses of hypertonic saline on mucociliary clearance in patients with cystic fibrosis. Thorax 1997, 52, 900–903. [Google Scholar] [CrossRef] [PubMed]
- Rossman, C.M.; Waldes, R.; Sampson, D.; Newhouse, M.T. Effect of chest physiotherapy on the removal of mucus in patients with cystic fibrosis. Am. Rev. Respir. Dis. 1982, 126, 131–135. [Google Scholar] [CrossRef]
- San Miguel-Pagola, M.; Reychler, G.; Cebria, I.; Gomez-Romero, M.; Diaz-Gutierrez, F.; Herrero-Cortina, B. Impact of hypertonic saline nebulisation combined with oscillatory positive expiratory pressure on sputum expectoration and related symptoms in cystic fibrosis: A randomised crossover trial [with consumer summary. Physiotherapy 2020, 107, 243–251. [Google Scholar] [CrossRef]
- Scherer, T.A.; Barandun, J.; Martinez, E.; Wanner, A.; Rubin, E.M. Effect of high-frequency oral airway and chest wall oscillation and conventional chest physical therapy on expectoration in patients with stable cystic fibrosis. Chest 1998, 113, 1019–1027. [Google Scholar] [CrossRef]
- Sokol, G.; Vilozni, D.; Hakimi, R.; Lavie, M.; Sarouk, I.; Bar, B.E.; Dagan, A.; Ofek, M.; Efrati, O. The short-term effect of breathing tasks via an incentive spirometer on lung function compared with autogenic drainage in subjects with cystic fibrosis. Respir. Care 2015, 60, 1819–1825. [Google Scholar] [CrossRef]
- Stanford, G.; Parrott, H.; Bilton, D.; Agent, P.; Banya, W.; Simmonds, N. Randomised cross-over trial evaluating the short-term effects of non-invasive ventilation as an adjunct to airway clearance techniques in adults with cystic fibrosis. BMJ Open Respir. Res. 2019, 6, e000399. [Google Scholar] [CrossRef]
- Steven, M.H.; Pryor, J.A.; Webber, B.A.; Hodson, M.R. Physiotherapy versus cough alone in the treatment of cystic fibrosis. N. Z. J. Physiother. 1992, 20, 31–37. [Google Scholar]
- Van Ginderdeuren, F.; Verbanck, S.; Van Cauwelaert, K.; Vanlaethem, S.; Schuermans, D.; Vincken, W.; Malfroot, A. Chest physiotherapy in cystic fibrosis: Short-term effects of autogenic drainage preceded by wet inhalation of saline versus autogenic drainage preceded by intrapulmonary percussive ventilation with saline. Respir 2008, 76, 175–180. [Google Scholar] [CrossRef]
- Varekojis, S.M.; Douce, F.H.; Flucke, R.L.; Filbrun, D.A.; Tice, J.S.; McCoy, K.S.; Castile, R.G. A comparison of the therapeutic effectiveness of and preference for postural drainage and percussion, intrapulmonary percussive ventilation, and high-frequency chest wall compression in hospitalized cystic fibrosis patients. Respir. Care 2003, 48, 24–28. [Google Scholar] [PubMed]
- Verboon, J.M.; Bakker, W.; Sterk, P.J. The value of the forced expiration technique with and without postural drainage in adults with cystic fibrosis. Eur. J. Respir. Dis. 1986, 69, 169–174. [Google Scholar]
- Wallaert, E.; Perez, T.; Prevotat, A.; Reychler, G.; Wallaert, B.; Le Rouzic, O. The immediate effects of a single autogenic drainage session on ventilatory mechanics in adult subjects with cystic fibrosis. PLoS ONE 2018, 13, e0195154. [Google Scholar] [CrossRef]
- Warwick, W.J.; Wielinski, C.L.; Hansen, L.G. Comparison of expectorated sputum after manual chest physical therapy and high-frequency chest compression. Biomed. Instrum. Technol. 2004, 38, 470–475. [Google Scholar]
- Webber, B.; Parker, R.; Hofmeyr, J.; Hodson, M. Evaluation of self-percussion during postural drainage using the forced expiration technique. Physiother. Pract. 1985, 1, 42–45. [Google Scholar] [CrossRef]
- Webber, B.A.; Hofmeyr, J.L.; Morgan, M.D.; Hodson, M.E. Effects of postural drainage, incorporating the forced expiration technique, on pulmonary function in cystic fibrosis. Br. J. Dis. Chest 1986, 80, 353–359. [Google Scholar] [CrossRef]
- Wheatley, C.M.; Baker, S.E.; Daines, C.M.; Phan, H.; Martinez, M.G.; Morgan, W.J.; Snyder, E.M. Influence of the Vibralung Acoustical Percussor on pulmonary function and sputum expectoration in individuals with cystic fibrosis. Ther. Adv. Respir. Dis. 2018, 12, 1753466618770997. [Google Scholar] [CrossRef]
- White, D.; Stiller, K.; Willson, K. The role of thoracic expansion exercises during the active cycle of breathing techniques. Physiother. Theory Pract. 1997, 13, 155–161. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- McCormack, P.; Burnham, P.; Southern, K.W. Autogenic drainage for airway clearance in cystic fibrosis. Cochrane Database Syst. Rev. 2017, 10, CD009595. [Google Scholar] [CrossRef] [PubMed]
- McKoy, N.A.; Wilson, L.M.; Saldanha, I.J.; Odelola, O.A.; Robinson, K.A. Active cycle of breathing technique for cystic fibrosis. Cochrane Database Syst. Rev. 2016, 7, Cd007862. [Google Scholar] [CrossRef]
- McIlwaine, M.; Button, B.; Nevitt, S.J. Positive expiratory pressure physiotherapy for airway clearance in people with cystic fibrosis. Cochrane Database Syst. Rev. 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Moran, F.; Bradley, J.M.; Piper, A.J. Non-invasive ventilation for cystic fibrosis. Cochrane Database Syst. Rev. 2017, 2, CD002769. [Google Scholar] [CrossRef]
- Franks, L.J.; Walsh, J.R.; Hall, K.; Morris, N.R. Measuring airway clearance outcomes in bronchiectasis: A review. Eur. Respir. Rev. 2020, 29, 190161. [Google Scholar] [CrossRef] [PubMed]
- Osadnik, C.R.; McDonald, C.F.; Jones, A.P.; Holland, A.E. Airway clearance techniques for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2012, 3, CD008328. [Google Scholar] [CrossRef]
- Campbell, A.H.; O’CONNELL, J.M.; Wilson, F. The effect of chest physiotherapy upon the FEV1 in chronic bronchitis. Med. J. Aust. 1975, 1, 33–35. [Google Scholar] [CrossRef]
- McDonnell, T.; McNicholas, W.T.; FitzGerald, M.X. Hypoxaemia during chest physiotherapy in patients with cystic fibrosis. Ir. J. Med. Sci. 1986, 155, 345–348. [Google Scholar] [CrossRef]
- Button, B.M.; Heine, R.G.; Catto-Smith, A.G.; Phelan, P.D.; Olinsky, A. Postural drainage and gastro-oesophageal reflux in infants with cystic fibrosis. Arch. Dis. Child. 1997, 76, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Van der Schans, C.P.; Postma, D.S.; Koeter, G.H.; Rubin, B.K. Physiotherapy and bronchial mucus transport. Eur. Respir. J. 1999, 13, 1477–1486. [Google Scholar] [CrossRef]
- Van der Schans, C.P. Bronchial mucus transport. Respir. Care 2007, 52, 1150–1156. [Google Scholar] [PubMed]
- Standards of Care and Good Clinical Practice for the Physiotherapy Management of Cystic Fibrosis Version 4; Cystic Fibrosis Trust: London, UK, 2020.
- Flume, P.A.; Robinson, K.A.; O’Sullivan, B.P.; Finder, J.D.; Vender, R.L.; Willey-Courand, D.B.; White, T.B.; Marshall, B.C. Cystic fibrosis pulmonary guidelines: Airway clearance therapies. Respir. Care 2009, 54, 522–537. [Google Scholar]
- Stanojevic, S.; Ratjen, F. Physiologic endpoints for clinical studies for cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2016, 15, 416–423. [Google Scholar] [CrossRef]
- Jones, P.W.; Beeh, K.M.; Chapman, K.R.; Decramer, M.; Mahler, D.A.; Wedzicha, J.A. Minimal clinically important differences in pharmacological trials. Am. J. Respir. Crit. Care Med. 2014, 189, 250–255. [Google Scholar] [CrossRef]
- Marques, A.; Cruz, J.; Jácome, C.; Oliveira, A. Outcome measures for respiratory physiotherapy in cystic fibrosis—challenges and advances. Cyst. Fibros. Light New Res. 2015, 37. [Google Scholar]
- Tiddens, H.; Puderbach, M.; Venegas, J.G.; Ratjen, F.; Donaldson, S.H.; Davis, S.D.; Rowe, S.M.; Sagel, S.D.; Higgins, M.; Waltz, D.A. Novel outcome measures for clinical trials in cystic fibrosis. Pediatr. Pulmonol. 2015, 50, 302–315. [Google Scholar] [CrossRef] [PubMed]
- Van der Schans, C.P. Airway clearance: Assessment of techniques. Paediatr. Respir. Rev. 2002, 3, 110–114. [Google Scholar] [CrossRef]
- Stanford, G.; Cathcart, F.; Beverley, Z.; Short, C.; Jones, M.; Bilton, D.; Davies, J.C.; Simmonds, N.J. Investigating outcome measures for assessing airway clearance techniques in adults with cystic fibrosis: Protocol of a single-centre randomised controlled crossover trial. BMJ Open Respir. Res. 2020, 7, e000694. [Google Scholar] [CrossRef] [PubMed]
- Hartman, J.E.; Ten Hacken, N.H.; Klooster, K.; Boezen, H.M.; de Greef, M.H.; Slebos, D.J. The minimal important difference for residual volume in patients with severe emphysema. Eur. Respir. J. 2012, 40, 1137–1141. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Sample | Clinical Status | Mechanism of Action and Airway Clearance Technique Used (G1, G2, C1, C2 Links with Figure 4 and Figure 5) | Outcomes and Useability (✓/✕/*) of These Data in Meta-Analyses |
|---|---|---|---|---|---|
| App 1998 [22] | RXT | n = 14 FEV1: 75% | Stable | C1: PEP (Flutter) [a = first, b = second] C2: OT (autogenic drainage) | Sputum wet weight ✓ Spirometry ✓ |
| Aquino 2012 [23] | RXT | n = 15 FEV1: 54% | Stable | Cough alone C1: PPD (CPAP) C2: PPD (CPAP + hypertonic NaCl 7%) | Sputum volume ✓ Sputum rheology * |
| Arens 1994 [24] | RCT | n = 25 FEV1: 34% vs. 38% | Mix | G1: OT (external oscillation device) G2: OT (postural drainage & percussion) | Sputum wet and dry weight ✓ |
| Baldwin 1994 [25] | RXT | n = 8 FEV1: 64% | Stable | C1: Exercise (aerobic)# C2: OT (postural drainage & ACBT & percussion & vibrations) | Sputum wet weight ✓ Spirometry ✓ Peak expiratory/cough flow * |
| Bilton 1992 [26] | RXT | n = 18 FEV1: N/A | Stable | C1: Exercise (cycling at 60%VO2max)# C2: Exercise (cycling at 60%VO2max then ACBT)# C3: Exercise (ACBT then cycling at 60%VO2max) # C4: OT (postural drainage & ACBT) | Sputum wet weight ✓ Spirometry ✕ Respiratory mechanics ✕ |
| Bishop 2011 [27] | RXT | n = 17 FEV1: 67% vs. 68% | Stable | C1: Usual ACT (Dornase alpha after usual ACT)# C2: Usual ACT (Dornase alpha before usual ACT)# | Sputum wet weight ✕ |
| Borka 2012 [28] | ?RXT | n = 10 FEV1: 57% | Stable | C1: PEP (Flutter then PEP) C2: PEP (PEP then Flutter) | Sputum wet weight ✓ |
| Braggion 1995 [29] | RXT | n = 16 FEV1: 53% | Mix | Cough alone C1: OT (external oscillation device) C2: PEP (PEP mask) C3: OT (postural drainage) | Sputum wet and dry weight ✓ Spirometry ✓ |
| Cantin 2006 [30] | ?RXT | n = 22 FEV1: 58% | Stable | C1: OT (external oscillation device) C2: OT (postural drainage & percussion) | Sputum wet weight ✓ |
| Carr 1995 [31] | Other | n = 20 FEV1: 32% | Stable | OT (ACBT & percussion) | Sputum wet weight ✕ |
| Chatham 2004 [32] | RXT | n = 20 FEV1: 60% vs. 48% (geometric mean) | Stable | C1: OT (resistive inspiratory manoeuvres) C2: OT (postural drainage & ACBT) | Sputum wet weight ✕ Sputum inflammatory markers ✕ |
| Darbee 2004 [33] | RXT | n = 5 FEV1: 52% | Stable | Cough alone C1: PEP (PEP mask-low) C2: PEP (PEP mask-high) | Sputum wet and dry weight ✕ Spirometry ✕ Inert gas washout ✕ Lung volumes ✕ |
| DeCesare 1982 [34] | Other | n = 10 FEV1: mild 68%, mod 43%, severe 24% | Mix | Cough alone C1: OT (postural drainage & percussion & vibrations) | Sputum volume ✕ Spirometry ✕ Peak expiratory/cough flow ✕ Imaging ✕ |
| Dwyer 2011 [35] | RXT | n = 14 FEV1: 55% | Stable | Cough alone C1: Exercise (20min walk at 60%VO2max)# C2: Exercise (20min cycle at 60%VO2max)# | Sputum rheology * Peak expiratory/cough flow ✕ |
| Dwyer 2015 [36] | RCT | n = 40 FEV1: 36% vs. 39% | Mix | G1: PPD (usual ACT & NIV) G2: Usual ACT# | Respiratory muscle strength * |
| Dwyer 2017 [37] | RXT | n = 25 FEV1: 51% | Stable | Cough alone C1: Exercise (20min walk at 60%VO2max)# C2: PEP (Flutter) | Sputum rheology * Peak expiratory/cough flow ✕ |
| Dwyer 2019 [38] | RXT | n = 14 FEV1: 65% | Stable | Cough alone C1: Exercise (20min walk at 60%VO2max)# C2: PEP (Pari PEP) | Imaging * |
| Fainardi 2011 [39] | RXT | n = 34 FEV1: 67% | Acute | C1: OT (external oscillation device) C2: PEP (PEP mask) | Sputum volume ✓ Spirometry ✓ |
| Falk 1984 [40] | RXT | n = 14 FEV1: 34% | Mix | C1: OT (postural drainage & percussion & huff/cough) C2: PEP (postural drainage & PEP mask & huff/cough) C3: PEP (PEP mask & huff/cough) C4: OT (pursed lip breathing & huff/cough) | Sputum wet weight ✓ Spirometry ✕ Peak expiratory/cough flow ✕ |
| Giles 1995 [41] | RXT | n = 10 FEV1: N/A | Stable | C1: OT (postural drainage & percussion) C2: OT (autogenic drainage) | Sputum wet weight ✓ Spirometry ✓ Peak expiratory/cough flow * |
| Grosse-Onnebrink 2017 [42] | RCT | n = 41 FEV1: 57% vs. 51% | Acute | Cough alone G1: OT (external oscillation device) | Inert gas washout * |
| Guimaraes 2014 [43] | RXT | n = 14 FEV1: 34% | Stable | C1: OT (ELTGOL) C2: PEP (Flutter) | Sputum dry weight ✓ Spirometry ✓ Lung volumes ✓ Respiratory mechanics * |
| Gursli 2017 [44] | Other | n = 6 FEV1: 68% | Stable | C1: OT (huff) C2: OT (specific cough technique) | Sputum wet weight ✓ Spirometry ✓ |
| Helper 2020 [45] | RXT | n = 22 FEV1: 54% | Stable | C1: PPD (MI-E Phillips E70 cough assist) C2: OT (autogenic drainage) | Sputum wet weight ✓ Spirometry ✓ Lung volumes ✓ Peak expiratory/cough flow * |
| Hofmeyr 1986 [46] | RXT | n = 18 FEV1: N/A | Stable | C1: PEP (PEP mask in sitting) C2: PEP (PEP mask & postural drainage) C3: OT (postural drainage & ACBT) | Sputum wet weight ✕ Spirometry ✕ |
| Holland 2003 [47] | RXT | n = 26 FEV1: 34% | Acute | C1: PPD (ACBT & NIV) C2: OT (ACBT) | Sputum wet weight ✓ Spirometry ✓ Respiratory muscle strength * |
| Hordvik 1996 [48] | RXT | n= 24 FEV1: 56% | Acute | C1: OT (postural drainage & external percussive device & albuterol) C2: OT (postural drainage & external percussive device & 0.9% NaCl) | Spirometry * |
| Hortal 2014 [49] | Other | n = 16 FEV1: 56% | Stable | PEP (PEP & autogenic drainage & huff) | Spirometry ✓ |
| Jarad 2010 [50] | RXT | n = 18 FEV1: N/A | Stable | Cough alone (sham hydro acoustic therapy) C1: OT (external oscillation device) C2: PEP (external oscillation device & Flutter) | Sputum wet and dry weight ✓ Spirometry ✓ |
| Kempainen 2007 [51] | RXT | n = 15 FEV1: 72% | Stable | C1: OT (external oscillation device with sine waveform) C2: OT (external oscillation device with triangular waveform) | Sputum wet and dry weight ✓ Sputum rheology ✕ Spirometry ✓ Inert gas washout * Lung volumes ✓ |
| Kempainen 2010 [52] | RXT | n = 16 FEV1: 68% | Stable | C1: OT (external oscillation device with higher pressure/variable frequency) C2: OT (external oscillation device with lower pressure/mid frequency) | Sputum wet and dry weight ✓ Sputum rheology ✕ Spirometry ✓ Inert gas washout * Lung volumes ✓ |
| Konstan 1994 [53] | RXT | n = 17 FEV1: N/A | Stable | Cough alone C1: OT (postural drainage) C2: PEP (Flutter) | Sputum wet and dry weight ✓ |
| Kriemler 2016 [54] | RXT | n = 12 FEV1: 63% | NA | C1: Exercise (trampolining then Flutter & thoracic expansion exercises & slow expiration)# C2: Exercise (cycling then Flutter & thoracic expansion exercises & slow expiration)# C3: PEP (billiards then Flutter & thoracic expansion exercises & slow expiration) | Sputum wet weight ✓ Spirometry ✓ |
| Lannefors 1992 [55] | RXT | n = 9 FEV1: 51% | Stable | C1: PEP (PEP mask & huff) C2: Exercise (cycling & huff)# C3: OT (postural drainage & thoracic expansion exercises & huff) | Imaging ✕ |
| Leemans 2020 [56] | RXT | n = 8 FEV1: 61% vs. 62% | Stable | C1: OT (mobile external oscillation device) C2: OT (external oscillation device) | Sputum wet weight ✓ Sputum volume ✓ |
| Lyons 1993 [57] | RXT | n = 12 FEV1: N/A | Stable | C1: PEP (Flutter) C2: PEP (usual ACT & Flutter) C3: OT (usual ACT & sham Flutter)# C4: Usual ACT# | Peak expiratory/cough flow ✕ |
| McCarren 2006 [58] | RXT | n = 18 FEV1: 55% | Stable | Cough alone C1: OT (vibrations) C2: OT (percussion) C3: PEP (PEP mask) C4: PEP (Flutter) C5: PEP (Acapella) C6: OT (total lung capacity with passive expiration) C7: OT (high lung volume huff) | Peak expiratory/cough flow ✕ |
| Mentore 2005 [59] | Other | n = 8, FEV1: 67% | N/A | Chest PT – nil other info# | Imaging ✕ |
| Milne 2004 [60] | RXT | n = 7 FEV1: NA | N/A | C1: PEP (Flutter) C2: OT (ACBT) | Spirometry ✕ Peak expiratory/cough flow ✕ |
| Mortensen 1991 [61] | RXT | n = 10 FEV1: 47% | Stable | Cough alone C1: OT (postural drainage & huff) C2: PEP (PEP mask & huff) | Sputum wet weight ✓ Imaging * |
| Murphy 1983 [62] | RXT | n = 2FEV1: NA | N/A | C1: OT (postural drainage & external percussive device) C2: OT (postural drainage & percussion) C3: OT (postural drainage & huff) | Sputum wet weight ✓ Spirometry ✕ Peak expiratory/cough flow ✕ |
| O’Neill 2017 [63] | RXT | n = 13 FEV1: 51% | Stable | C1: PEP (hypertonic NaCl pre Acapella Duet) C2: PEP (hypertonic NaCl during Acapella Duet) | Sputum wet weight ✓ Inert gas washout * |
| Osman 2010 [64] | RXT | n = 29 FEV1: 38% | Stable | C1: OT (external oscillation device) C2: Usual ACT# | Sputum wet weight ✓ Spirometry ✓ |
| Pfleger 2015 [65] | Other | n = 29 FEV1: 70% | Stable | PEP (PEP mask) | Spirometry ✕ Inert gas washout ✕ Lung volumes ✕ Respiratory mechanics ✕ |
| Placidi 2006 [66] | RXT | n = 17 FEV1: 25% | Mix | Cough alone C1: PEP (PEP mask) C2: PPD (CPAP) C3: PPD (NIV) | Sputum wet and dry weight ✓ Spirometry ✓ |
| Pryor 1979a [67] | RXT | n = 16 FEV1: N/A | Stable | C1: OT (postural drainage & thoracic expansion exercises & shakes & therapist percussion & cough) C2: OT (postural drainage & thoracic expansion exercises & self-percussion & huff & cough) | Spirometry ✕ Peak expiratory/cough flow ✕ |
| Pryor 1979b [67] | RXT | n = 8 FEV1: N/A | Mix | C1: OT (postural drainage & thoracic expansion exercises & self-percussion & huff & cough) C2: OT (postural drainage & shakes & therapist percussion & huff) | Spirometry ✕ Peak expiratory/cough flow ✕ |
| Pryor 1979c [68] | RXT | n = 24 FEV1: N/A | Stable | C1: OT (postural drainage & thoracic expansion exercises & percussion & cough) C2: OT (postural drainage & thoracic expansion exercises & percussion & huff & cough) | Sputum wet weight ✕ Spirometry ✕ |
| Pryor 1981 [69] | RXT | n = 12 FEV1: NA | Stable | C1: OT (postural drainage & external percussive device & huff) C2: OT (postural drainage & percussion & huff) | Sputum wet weight ✕ Spirometry ✕ |
| Pryor 1990 [70] | Other | n = 20 FEV1: N/A | N/A | OT (postural drainage & ACBT) | Sputum wet weight ✕ |
| Pryor 1994 [71] | RXT | n = 20 FEV1: N/A | Stable | C1: OT (ACBT) C2: PEP (Flutter & ACBT) | Sputum wet weight ✕ Spirometry ✕ |
| Radtke 2018 [72] | RXT | n = 15 FEV1: 56% | Stable | C1: PEP (Flutter & interval cycling) C2: Exercise (continuous cycling)# | Sputum rheology * Pulmonary diffusion capacity * |
| Robinson 1996 [73] | RXT | n = 12 FEV1: 61% | Stable | Cough alone C1: 0.9% NaCl# C2: Amiloride in 0.12% NaCl# C3: Hypertonic NaCl 7%# C4: Amiloride & hypertonic NaCl 7%# | Spirometry ✓ Imaging ✕ |
| Robinson 1997 [74] | RXT | n = 10 FEV1: 52% | Stable | Cough & 0.9% NaCl C2: Hypertonic NaCl 3%# C3: Hypertonic NaCl 7%# C4: Hypertonic NaCl 12%# | Spirometry ✓ Imaging ✕ |
| Rossman 1982 [75] | RXT | n = 6 FEV1: 38% | Stable | Cough alone (spontaneous) Cough alone 2 (directed) C1: OT (postural drainage) C2: OT (postural drainage & external percussive device) C3: OT (postural drainage & thoracic expansion exercises & vibrations & therapist percussion) | Sputum volume ✕ Imaging * |
| San Miguel-Pagola 2020 [76] | RXT | n = 22 FEV1: 67% | Stable | C1: PEP (Hypertonic NaCl 7% & hyaluronic acid 0.1% via Acapella Duet pre autogenic drainage) C2: OT (Hypertonic NaCl 7% & hyaluronic acid 0.1% neb pre autogenic drainage) | Sputum volume ✓ |
| Scherer 1998 [77] | RXT | n = 14 FEV1: 59% | Stable | C1: PPD (Sensormedics Oscillatory oral Ventilator 3100B) C2: PPD (Sensormedics MCT1 oral airway oscillator) C3: OT (external oscillation device at optimal settings) C4: OT (external oscillation device using secretion clearance mode) C5: OT (postural drainage & percussion & external percussive device & cough) | Percentage of baseline wet and dry sputum expectorated * Spirometry * |
| Sokol 2015 [78] | Other | n = 40 vs. 32 FEV1: 57% vs. 66% | Stable | G1: PEP (Tri-Gym incentive spirometer) G2: OT (autogenic drainage) | Spirometry * Peak expiratory/cough flow * |
| Stanford 2019 [79] | RXT | n = 14 FEV1: 49% | Stable | C1: PPD (NIV & usual ACT) C2: PEP (PEP/oscillating PEP) C3: OT (ACBT & autogenic drainage) | Sputum wet weight ✓ Spirometry ✓ |
| Steven 1992 [80] | RXT | n = 24 FEV1: N/A | Stable | Cough alone C1: OT (ACBT & cough in sitting) C2: OT (postural drainage & ACBT & cough) | Sputum wet weight ✓ Spirometry ✕ |
| Van Ginderdeuren 2008 [81] | RXT | n = 20 FEV1: 65% | Stable | C1: OT (0.9% NaCl neb pre autogenic drainage) C2: PPD (0.9% NaCl via IPV pre autogenic drainage) | Sputum wet weight ✓ |
| Varekojis 2003 [82] | RXT | n = 24 FEV1: 55% | Acute | C1: OT (postural drainage & percussion) C2: OT (external oscillation device) C3: PPD (IPV & 0.9% NaCl) | Sputum wet and dry weight ✓ |
| Verboon 1986 [83] | RXT | n = 8 FEV1: 38% | Stable | C1: OT (huff post sleeping in postural drainage position) C2: OT (huff in upright post sleeping in horizontal position) | Sputum wet weight ✕ Spirometry ✕ Peak expiratory/cough flow ✕ |
| Wallaert 2018 [84] | Other | n = 30 FEV1: 40% | Stable | OT (autogenic drainage) | Sputum wet and dry weight ✓ Spirometry ✓ Respiratory mechanics * |
| Warwick 2004 [85] | RXT | n = 12 FEV1: N/A | Stable | C1: OT (percussion & huff & directed coughing) C2: OT (external oscillation device & huff) | Sputum wet and dry weight ✓ |
| Webber 1985 [86] | RXT | n = 16 FEV1: 32% | Stable | C1: OT (postural drainage & thoracic expansion exercises & percussion & huff) C2: OT (postural drainage & thoracic expansion exercises & huff) | Sputum wet weight✕ Spirometry ✕ |
| Webber 1986 [87] | Other | n = 11 FEV1: 61% | Stable | OT (postural drainage & ACBT & percussion & vibrations & shakes) | Sputum wet weight ✕ |
| Wheatley 2018a [88] | RXT | n = 10 FEV1: 76% | Stable | C1: PEP (Vibralung sham) C2: PEP (Vibralung) | Spirometry ✓ Pulmonary diffusion capacity * |
| Wheatley 2018b [88] | RXT | n = 11 FEV1: 57% | Acute | C1: PEP (Vibralung day 1–5) C2: PEP (Vibralung day 7–11) C3: OT (external oscillation device) | Sputum wet and dry weight ✕ |
| White 1997 [89] | RXT | n = 15 FEV1: mild (>70%) = 3, mod (41–70%) = 4, severe (≤40) = 8 | Acute | C1: OT (postural drainage & ACBT) C2: OT (postural drainage & ACBT without thoracic expansion exercises) | Sputum wet weight ✓ Spirometry ✓ Peak expiratory/cough flow ✕ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chapman, N.; Watson, K.; Hatton, T.; Cavalheri, V.; Wood, J.; Gucciardi, D.F.; Smith, E.F.; Hill, K. Methods Used to Evaluate the Immediate Effects of Airway Clearance Techniques in Adults with Cystic Fibrosis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5280. https://doi.org/10.3390/jcm10225280
Chapman N, Watson K, Hatton T, Cavalheri V, Wood J, Gucciardi DF, Smith EF, Hill K. Methods Used to Evaluate the Immediate Effects of Airway Clearance Techniques in Adults with Cystic Fibrosis: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(22):5280. https://doi.org/10.3390/jcm10225280
Chicago/Turabian StyleChapman, Naomi, Kathryn Watson, Tamara Hatton, Vinicius Cavalheri, Jamie Wood, Daniel F. Gucciardi, Elizabeth F. Smith, and Kylie Hill. 2021. "Methods Used to Evaluate the Immediate Effects of Airway Clearance Techniques in Adults with Cystic Fibrosis: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 22: 5280. https://doi.org/10.3390/jcm10225280
APA StyleChapman, N., Watson, K., Hatton, T., Cavalheri, V., Wood, J., Gucciardi, D. F., Smith, E. F., & Hill, K. (2021). Methods Used to Evaluate the Immediate Effects of Airway Clearance Techniques in Adults with Cystic Fibrosis: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(22), 5280. https://doi.org/10.3390/jcm10225280