
Urinary Beta-2-Microglobulin and Late Nephrotoxicity in Childhood Cancer Survivors

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Childhood Cancer Survivors Study. Chronic Health Conditions in Adult Survivors of Childhood Cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef]
- Krawczuk-Rybak, M.; Panasiuk, A.; Stachowicz-Stencel, T.; Zubowska, M.; Skalska-Sadowska, J.; Sęga-Pondel, D.; Czajńska-Deptuła, A.; Sławińska, D.; Badowska, W.; Kamieńska, E.; et al. Health Status of Polish Children and Adolescents after Cancer Treatment. Eur. J. Pediatr. 2018, 177, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Kooijmans, E.C.; Bökenkamp, A.; Tjahjadi, N.S.; Tettero, J.M.; van Dulmen-den Broeder, E.; van der Pal, H.J.; Veening, M.A. Early and Late Adverse Renal Effects after Potentially Nephrotoxic Treatment for Childhood Cancer. Cochrane Database Syst. Rev. 2019, 3, CD008944. [Google Scholar] [CrossRef] [PubMed]
- Skinner, R. Late Renal Toxicity of Treatment for Childhood Malignancy: Risk Factors, Long-Term Outcomes, and Surveillance. Pediatr. Nephrol. 2018, 33, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Zubowska, M.; Wyka, K.; Fendler, W.; Młynarski, W.; Zalewska-Szewczyk, B. Interleukin 18 as a marker of chronic nephropathy in children after anticancer treatment. Dis. Markers. 2013, 35, 811–818. [Google Scholar] [CrossRef]
- Sørensen, P.G.; Nissen, M.H.; Groth, S.; Rørth, M. Beta-2-microglobulin excretion: An indicator of long term nephrotoxicity during cis-platinum treatment? Cancer Chemother. Pharmacol. 1985, 14, 247–249. [Google Scholar] [CrossRef]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.H.; Roumelioti, M.E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering Beta-2 Microglobulin As a Biomarker across the Spectrum of Kidney Diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portman, R.J.; Kissane, J.M.; Robson, A.M. Use of beta 2 microglobulin to diagnose tubule-interstitial renal lesions in children. Kidney Int. 1986, 30, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Coca, S.G.; Parikh, C.R. Urinary biomarkers for acute kidney injury: Perspectives on translation. Clin. J. Am. Soc. Nephrol. 2008, 3, 481–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J. Hypertens. 2016, 34, 1887–1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, A.; Stevens, P.E. Summary of KDIGO 2012 CKD Guideline: Behind the Scenes, Need for Guidance, and a Framework for Moving Forward. Kidney Int. 2014, 85, 49–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjorth, L.; Wiebe, T.; Karpman, D. Hyperfiltration evaluated by glomerular filtration rate at diagnosis in children with cancer. Pediatr. Blood Cancer 2011, 56, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.R.; Faubel, S.; Edelstein, C.L. Biomarkers of Drug-Induced Kidney Toxicity. Ther. Drug Monit. 2019, 41, 213–226. [Google Scholar] [CrossRef]
- George, B.; Joy, M.S.; Aleksunes, L.M. Urinary Protein Biomarkers of Kidney Injury in Patients Receiving Cisplatin Chemotherapy. Exp. Biol. Med. 2018, 243, 272–282. [Google Scholar] [CrossRef]
- Finkel, K.W.; Foringer, J.R. Renal disease in patients with cancer. Nat. Clin. Pract. Nephrol. 2007, 3, 669–678. [Google Scholar] [CrossRef]
- Latoch, E.; Konończuk, K.; Taranta-Janusz, K.; Muszyńska-Rosłan, K.; Szymczak, E.; Wasilewska, A.; Krawczuk-Rybak, M. Urine NGAL and KIM-1: Tubular Injury Markers in Acute Lymphoblastic Leukemia Survivors. Cancer Chemother. Pharmacol. 2020, 86, 741–749. [Google Scholar] [CrossRef]
- Latoch, E.; Konończuk, K.; Muszyńska-Rosłan, K.; Taranta-Janusz, K.; Wasilewska, A.; Szymczak, E.; Trochim, J.; Krawczuk-Rybak, M. Urine NGAL and KIM-1-Tubular Injury Markers in Long-Term Survivors of Childhood Solid Tumors: A Cross-Sectional Study. J. Clin. Med. 2021, 10, 399. [Google Scholar] [CrossRef] [PubMed]
- Ylinen, E.; Jahnukainen, K.; Saarinen-Pihkala, U.M.; Jahnukainen, T. Assessment of renal function during high-dose methotrexate treatment in children with acute lymphoblastic leukemia. Pediatr. Blood Cancer 2014, 61, 2199–2202. [Google Scholar] [CrossRef] [PubMed]
- Mulder, R.L.; Knijnenburg, S.L.; Geskus, R.B.; van Dalen, E.C.; van der Pal, H.J.H.; Koning, C.C.E.; Bouts, A.H.; Caron, H.N.; Kremer, L.C.M. Glomerular Function Time Trends in Long-Term Survivors of Childhood Cancer: A Longitudinal Study. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1736–1746. [Google Scholar] [CrossRef] [Green Version]
- Dawson, L.A.; Kavanagh, B.D.; Paulino, A.C.; Das, S.K.; Miften, M.; Li, X.A.; Pan, C.; Ten Haken, R.K.; Schultheiss, T.E. Radiation-associated kidney injury. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S108–S115. [Google Scholar] [CrossRef]
- Dekkers, I.A.; Blijdorp, K.; Cransberg, K.; Pluijm, S.M.; Pieters, R.; Neggers, S.J.; van den Heuvel-Eibrink, M.M. Long-term nephrotoxicity in adult survivors of childhood cancer. Clin. J. Am. Soc. Nephrol. 2013, 8, 922–929. [Google Scholar] [CrossRef] [Green Version]
- Schiavetti, A.; Altavista, P.; De Luca, L.; Andreoli, G.; Megaro, G.; Versacci, P. Long-term renal function in unilateral non-syndromic renal tumor survivors treated according to International Society of Pediatric Oncology protocols. Pediatr. Blood Cancer 2015, 62, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Rysz, J.; Gluba-Brzózka, A.; Franczyk, B.; Jabłonowski, Z.; Ciałkowska-Rysz, A. Novel Biomarkers in the Diagnosis of Chronic Kidney Disease and the Prediction of Its Outcome. Int. J. Mol. Sci. 2017, 18, 1702. [Google Scholar] [CrossRef] [PubMed]
- Puthiyottil, D.; Priyamvada, P.S.; Kumar, M.N.; Chellappan, A.; Zachariah, B.; Parameswaran, S. Role of Urinary Beta 2 Microglobulin and Kidney Injury Molecule-1 in Predicting Kidney Function at One Year Following Acute Kidney Injury. Int. J. Nephrol. Renovasc. Dis. 2021, 14, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Tibúrcio, F.R.; Rodrigues, K.; Belisário, A.R.; Simões-E-Silva, A.C. Glomerular hyperfiltration and β-2 microglobulin as biomarkers of incipient renal dysfunction in cancer survivors. Future Sci. OA 2018, 4, FSO333. [Google Scholar] [CrossRef] [Green Version]
- Musiol, K.; Sobol-Milejska, G.; Nowotka, Ł.; Torba, K.; Kniażewska, M.; Wos, H. Renal function in children treated for central nervous system malignancies. Childs Nerv. Syst. 2016, 32, 1431–1440. [Google Scholar] [CrossRef] [Green Version]
- Ikezumi, Y.; Uemura, O.; Nagai, T.; Ishikura, K.; Ito, S.; Hataya, H.; Fujita, N.; Akioka, Y.; Kaneko, T.; Iijima, K.; et al. Beta-2 microglobulin-based equation for estimating glomerular filtration rates in Japanese children and adolescents. Clin. Exp. Nephrol. 2015, 19, 450–457. [Google Scholar] [CrossRef]
- Hibi, Y.; Uemura, O.; Nagai, T.; Yamakawa, S.; Yamasaki, Y.; Yamamoto, M.; Nakano, M.; Kasahara, K. The ratios of urinary β2-microglobulin and NAG to creatinine vary with age in children. Pediatr. Int. 2015, 57, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Prizment, A.E.; Linabery, A.M.; Lutsey, P.L.; Selvin, E.; Nelson, H.H.; Folsom, A.R.; Church, T.R.; Drake, C.G.; Platz, E.A.; Joshu, C. Circulating Beta-2 Microglobulin and Risk of Cancer: The Atherosclerosis Risk in Communities Study (ARIC). Cancer Epidemiol. Biomark. Prev. 2016, 25, 657–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Qin, Y.; Zhou, S.; He, X.; Yang, J.; Kang, S.; Liu, P.; Yang, S.; Zhang, C.; Gui, L.; et al. Prognostic value of pretreatment serum beta-2 microglobulin level in advanced classical Hodgkin lymphoma treated in the modern era. Oncotarget 2016, 7, 72219–72228. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, K.; Dong, W.; Li, R.; Huang, R.; Zhang, H.; Shi, W.; Liu, S.; Li, Z.; Chen, Y.; et al. Raised Plasma Levels of Asymmetric Dimethylarginine Are Associated with Pathological Type and Predict the Therapeutic Effect in Lupus Nephritis Patients Treated with Cyclophosphamide. Kidney Dis. 2020, 6, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Behairy, O.G.; Abd Almonaem, E.R.; Abed, N.T.; Abdel Haiea, O.M.; Zakaria, R.M.; AbdEllaty, R.I.; Asr, E.H.; Mansour, A.I.; Abdelrahman, A.M.; Elhady, H.A. Role of serum cystatin-C and beta-2 microglobulin as early markers of renal dysfunction in children with beta thalassemia major. Int. J. Nephrol. J. Renovasc. Dis. 2017, 10, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, M.B.; Thieme, K.; Santos-Bezerra, D.P.; Queiroz, M.S.; Woronik, V.; Passarelli, M.; Machado, U.F.; Giannella-Neto, D.; Oliveira-Souza, M.; Corrêa-Giannella, M.L. Beta-2-microglobulin (B2M) expression in the urinary sediment correlates with clinical markers of kidney disease in patients with type 1 diabetes. Metab. Clin. Exp. 2016, 65, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Ugan, Y.; Korkmaz, H.; Dogru, A.; Koca, Y.S.; Balkarlı, A.; Aylak, F.; Tunc, S.E. The significance of urinary beta-2 microglobulin level for differential diagnosis of familial Mediterranean fever and acute appendicitis. Clin. Rheumatol. 2016, 35, 1669–1672. [Google Scholar] [CrossRef]
- Katsoufis, C.P. Clinical predictors of chronic kidney disease in congenital lower urinary tract obstruction. Pediatr. Nephrol. 2020, 35, 1193–1201. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.; Al Hadidi, S.; Usmani, S.; Yee, A.J.; Raje, N.; Davies, F.E. How to Treat High-Risk Myeloma at Diagnosis and Relapse. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, 291–309. [Google Scholar] [CrossRef]
- Gao, A.; Cachat, F.; Faouzi, M.; Bardy, D.; Mosig, D.; Meyrat, B.J.; Girardin, E.; Chehade, H. Comparison of the glomerular filtration rate in children by the new revised Schwartz formula and a new generalized formula. Kidney Int. 2013, 83, 524–530. [Google Scholar] [CrossRef] [Green Version]
- Kanemasa, Y.; Shimoyama, T.; Sasaki, Y.; Tamura, M.; Sawada, T.; Omuro, Y.; Hishima, T.; Maeda, Y. Beta-2 microglobulin as a significant prognostic factor and a new risk model for patients with diffuse large B-cell lymphoma. Hematol. Oncol. 2017, 35, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Krawczuk-Rybak, M.; Latoch, E. Risk Factors for Premature Aging in Childhood Cancer Survivors. Dev. Period. Med. 2019, 23, 97–103. [Google Scholar] [PubMed]
- Ariffin, H.; Azanan, M.S.; Abd Ghafar, S.S.; Oh, L.; Lau, K.H.; Thirunavakarasu, T.; Sedan, A.; Ibrahim, K.; Chan, A.; Chin, T.F.; et al. Young Adult Survivors of Childhood Acute Lymphoblastic Leukemia Show Evidence of Chronic Inflammation and Cellular Aging. Cancer 2017, 123, 4207–4214. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Total | Male | Female | |
|---|---|---|---|
| Patients (n, %) | 165 (100%) | 80 (48.5%) | 85 (51.5%) |
| Age at diagnosis (years) | 5.31 ± 4.16 4.24 (2.66–7.20) | 5.36 ± 4.16 3.82 (2.83–6.9) | 5.9 ± 4.67 4.38 (2.34–7.57) |
| Age at study (years) | 13.40 ± 5.96 14.21 (8.62–17.67) | 12.25 ± 4.94 12.35 (8.09–16.21) | 13.78 ± 5.94 14.5 (9.18–17.42) |
| Follow-up after treatment (years) | 7.01 ± 5.28 6.55 (2.25–10.39) | 6.22 ± 5.09 5.51 (2.03–9.25) | 7.75 ± 5.27 7.45 (3.83–11.15) |
| Diagnosis: | 165 (100%) | ||
| Acute lymphoblastic leukemia | 84 (50.9%) | 41 (49%) | 43 (51%) |
| Wilms tumor | 17 (10.3%) | 7 (41%) | 10 (59%) |
| Sarcoma | 14 (8.5%) | 8 (57%) | 6 (43%) |
| Non-Hodgkin lymphoma | 13 (7.9%) | 4 (31%) | 9 (69%) |
| Hodgkin lymphoma | 10 (6.1%) | 4 (40%) | 6 (10%) |
| Neuroblastoma | 9 (5.5%) | 3 (33%) | 6 (64%) |
| Acute myeloid leukemia | 8 (4.8%) | 3 (37%) | 5 (63%) |
| Hepatoblastoma | 4 (2.4%) | 2 (50%) | 2 (50%) |
| Germ tumors | 3 (1.8%) | 2 (67%) | 1 (33%) |
| Langerhans cell histiocytosis | 3 (1.8%) | 1 (33%) | 2 (67%) |
| Chemotherapy: | |||
| Methotrexate (cumulative dose in mg/m2), n = 100 (60.6%) | 13,373 ± 19,972 8000 (8000–10,000) | 14,300 ± 20,059 8000 (8000–20,000) | 12,409 ± 20,044 8000 (8000–8000) b |
| Cumulative corticosteroid a (dose in mg/m2), n = 109 (66.1%) | 1800 ± 791 1711 (1711–1711) b | 1764 ± 763 1711 (1711–1711) b | 1838 ± 825 1711 (1711–1748) |
| Cyclophosphamide (cumulative dose in mg/m2), n = 113 (68.5%) | 3893.36 ± 2448.33 3000 (3000–4000) | 3868 ± 235 3000 (3000–3000) b | 3919 ± 2557 3000 (3000–3000) b |
| Ifosfamide (cumulative dose in mg/m2), n = 14 (8.5%) | 74,857 ± 71,888 54,000 (36,000–84,000) | 65,500 ± 40,242 54,000 (51,750–78,750) | 87,333 ± 104,128 60,000 (18,500–139,500) |
| Cisplatin (cumulative dose in mg/m2), n = 16 (9.7%) | 430 ± 241.99 400 (240–480) | 400 ± 153 400 (240–570) | 460 ± 316 400 (240–480) |
| Radiotherapy (RT): | 41 (24.8%) | 19 (46%) | 22 (54%) |
| Cranial radiotherapy (CRT) (cumulative dose in Gray), n = 19 (11.5%) | 19.33 ± 14.04 12.0 (12–18) | 21.2 ± 16.67 12.0 (12.0–34.2) | 17.64 ± 11.85 12.0 (12.0–18.0) |
| Abdominal radiotherapy (cumulative dose in Gray), n = 19 (11.5%) | 22.45 ± 10.26 21.0 (19.80–21) | 21.98 ± 12.09 19.8 (13.95–21.0) | 22.08 ± 9.32 21.0 (19.8–21) |
| Total body irradiation (TBI) (cumulative dose in Gray), n = 5 (3%) | 12.0 ± 0.00 12.0 (12.0–12.0) b | 12.0 ± 0.0 12.0 (12.0–12.0) b | 12.0 ± 0.0 12.0 (12.0–12.0) b |
| No radiotherapy, n = 124 (75.2%) | 124 (75.2%) | ||
| Nephrectomy (unilateral) | 16 (9.7%) | 6 (37.5%) | 10 (62.5%) |
| Hematopoietic stem cell transplantation (HSCT) | 20 (12.1%) | 9 (45%) | 11 (55%) |
| Childhood Cancer Survivors n = 165 | Control Group n = 50 | p Value | |
|---|---|---|---|
| Serum creatinine (mg/dL) | 0.58 (0.43; 0.75) | 0.50 (0.41; 0.63) | 0.035 |
| Urine creatinine (mg/L) | 120.64 (73.67; 178.52) | 89.40 (65.78; 116.44) | 0.001 |
| eGFR (mL/min/1.73 m2) | 117.47 (98.79; 139.87) | 118.95 (103.25; 136.02) | 0.792 |
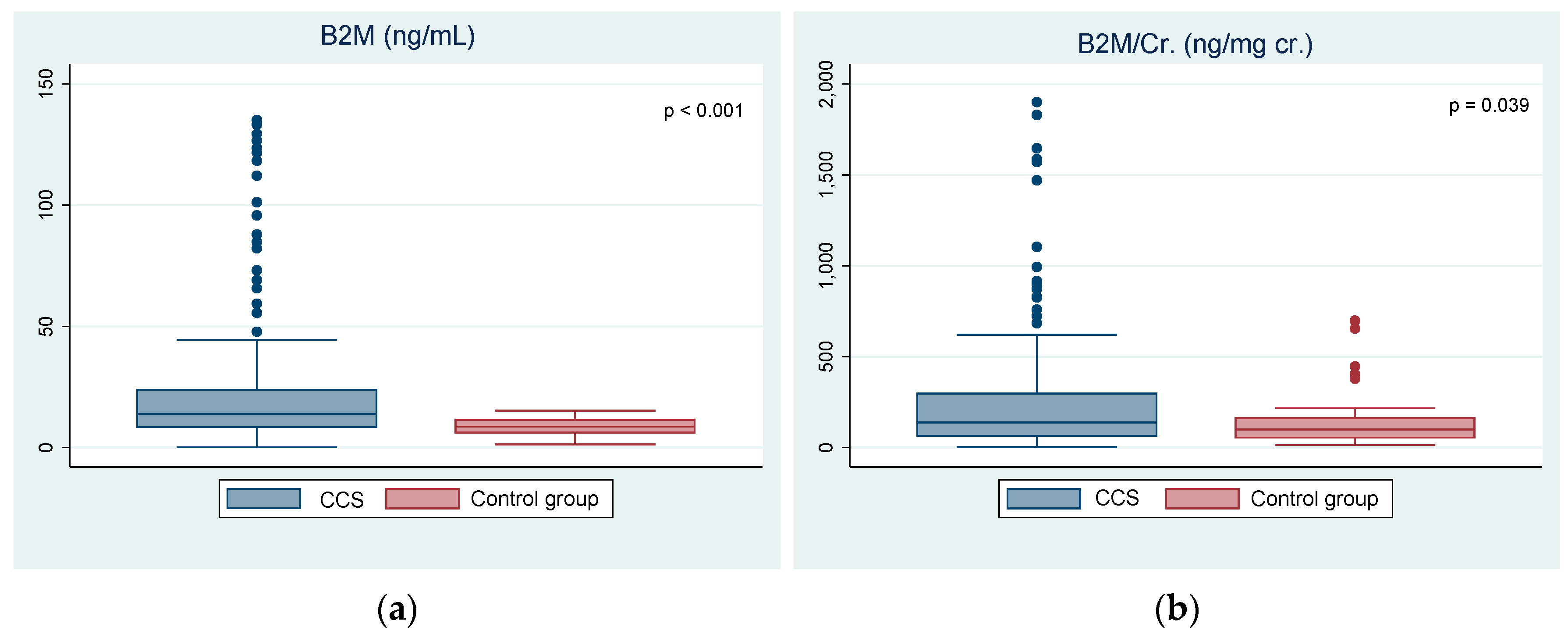
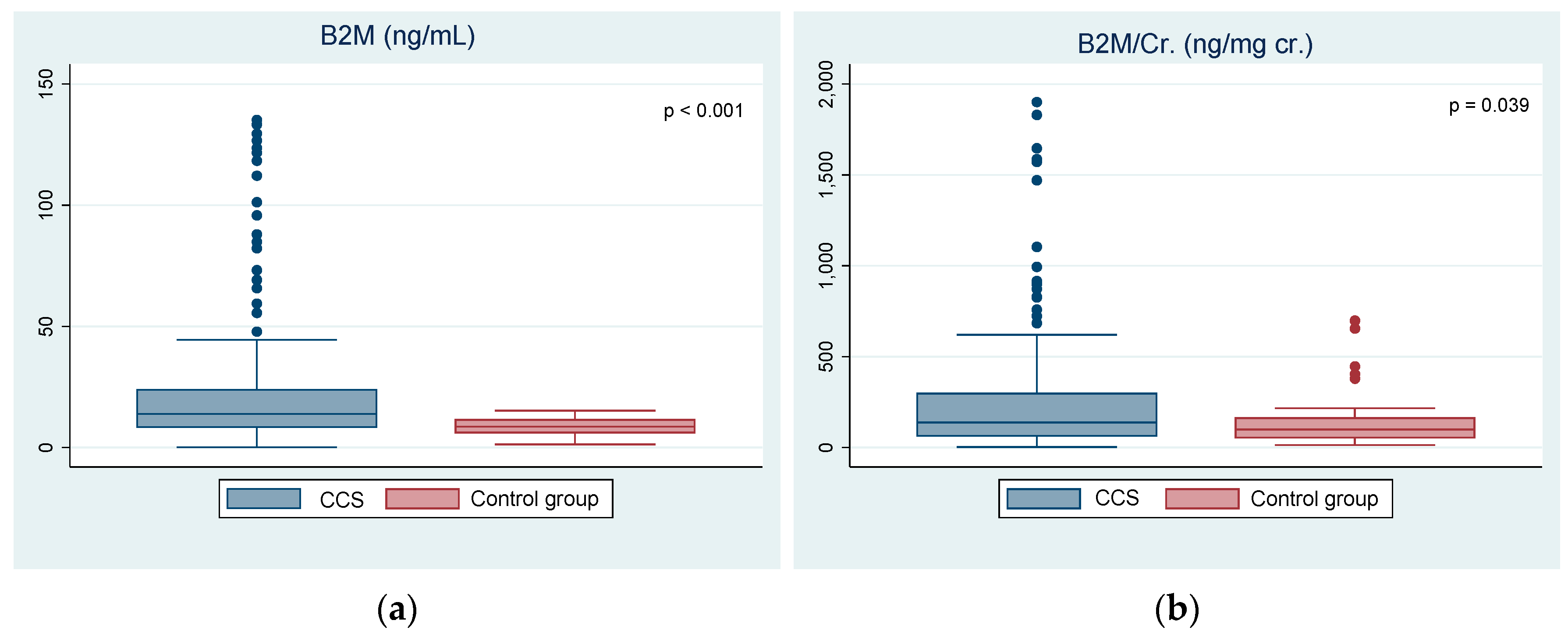
| β2M (ng/mL) | 14.30 (8.62; 26.10) | 8.67 (6.18; 11.48) | <0.001 |
| β2M /cr. (ng/mg cr.) | 139.87 (66.41; 305.48) | 99.63 (55.34; 162.37) | 0.039 |
| <5 Years | >5 Years | p Value | |
|---|---|---|---|
| n = 64 | n = 101 | ||
| Age at study (years) | 6.90 (5.42; 11.67) | 15.94 (12.99; 19.15) | <0.001 |
| eGFR (mL/min/1.73 m2) | 127.00 (103.73; 151.96) | 112.43 (98.01; 134.98) | 0.047 |
| β2M (ng/mL) | 10.99 (5.31; 24.50) | 16.59 (11.22; 39.82) | <0.0001 |
| β2M /cr. (ng/mg cr.) | 110.14 (41.00; 246.49) | 151.56 (74.87; 328.48) | 0.049 |
| Variables | Coefficient | p |
|---|---|---|
| Ifosfamide (cumulative dose) | −17.6 | 0.120 |
| Cyclophosphamide (cumulative dose) | 0.02 | 0.368 |
| Cisplatin (cumulative dose) | 0.14 | 0.728 |
| Methotrexate (cumulative dose) | −2.92 | 0.965 |
| Abdominal radiotherapy (yes vs. no) | −89.6 | 0.368 |
| Age at diagnosis (years) | 6.43 | 0.372 |
| Follow-up time (years) | −0.66 | 0.922 |
| BMI (kg/m2) | 14.5 | 0.046 |
| Hypertension (yes vs. no) | 43.2 | 0.610 |
| Nephrectomy (yes vs. no) | −10.7 | 0.361 |
| HSCT (yes vs. no) | −45.4 | 0.642 |
| Diagnosis (leukemia vs. lymphoma vs. solid tumors) | −29.2 | 0.401 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latoch, E.; Konończuk, K.; Taranta-Janusz, K.; Muszyńska-Rosłan, K.; Sawicka, M.; Wasilewska, A.; Krawczuk-Rybak, M. Urinary Beta-2-Microglobulin and Late Nephrotoxicity in Childhood Cancer Survivors. J. Clin. Med. 2021, 10, 5279. https://doi.org/10.3390/jcm10225279
Latoch E, Konończuk K, Taranta-Janusz K, Muszyńska-Rosłan K, Sawicka M, Wasilewska A, Krawczuk-Rybak M. Urinary Beta-2-Microglobulin and Late Nephrotoxicity in Childhood Cancer Survivors. Journal of Clinical Medicine. 2021; 10(22):5279. https://doi.org/10.3390/jcm10225279
Chicago/Turabian StyleLatoch, Eryk, Katarzyna Konończuk, Katarzyna Taranta-Janusz, Katarzyna Muszyńska-Rosłan, Magdalena Sawicka, Anna Wasilewska, and Maryna Krawczuk-Rybak. 2021. "Urinary Beta-2-Microglobulin and Late Nephrotoxicity in Childhood Cancer Survivors" Journal of Clinical Medicine 10, no. 22: 5279. https://doi.org/10.3390/jcm10225279
APA StyleLatoch, E., Konończuk, K., Taranta-Janusz, K., Muszyńska-Rosłan, K., Sawicka, M., Wasilewska, A., & Krawczuk-Rybak, M. (2021). Urinary Beta-2-Microglobulin and Late Nephrotoxicity in Childhood Cancer Survivors. Journal of Clinical Medicine, 10(22), 5279. https://doi.org/10.3390/jcm10225279