
The Predictive Value of Systemic Immune-Inflammation Index on Bladder Recurrence on Upper Tract Urothelial Carcinoma Outcomes after Radical Nephroureterectomy

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Treatment and Follow-Up
2.3. Definitions of Inflammatory Indexes
2.4. Statistical Analysis
3. Results
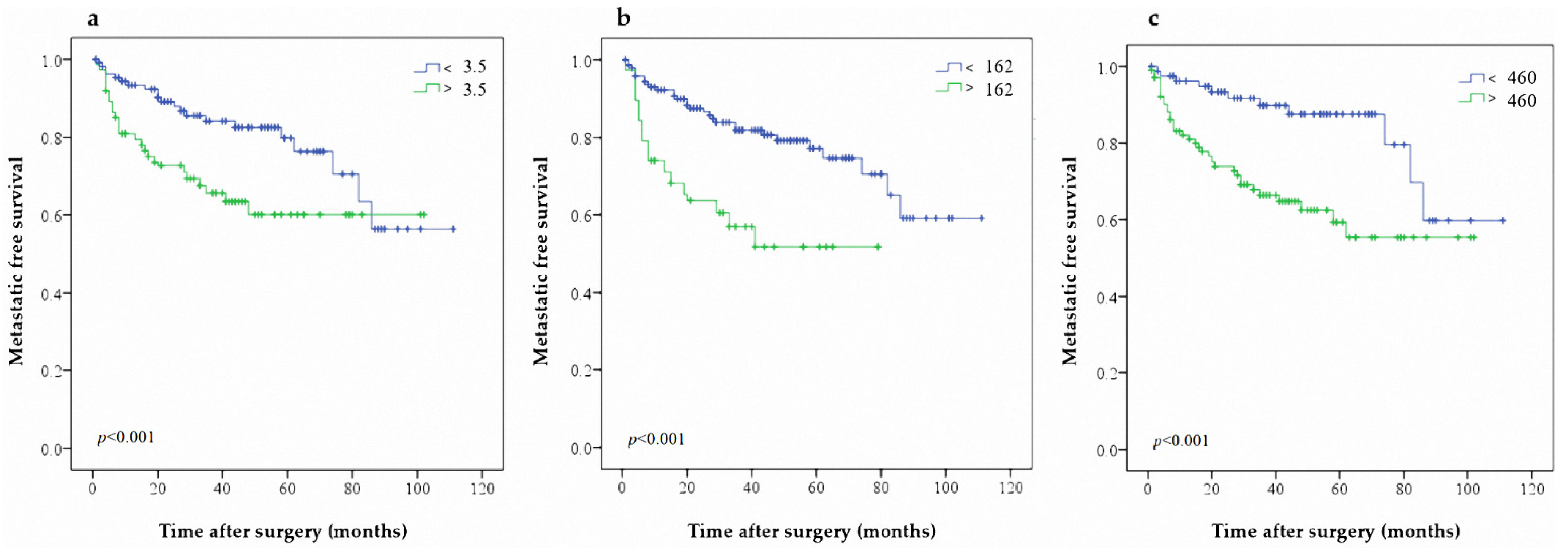
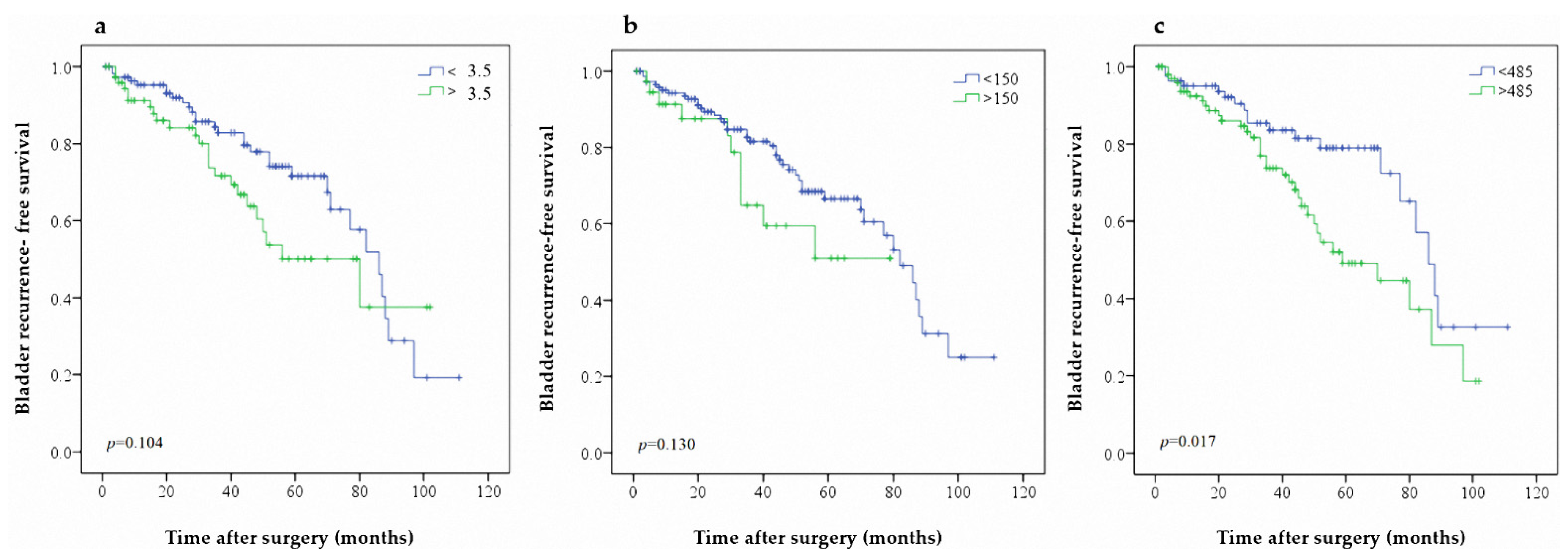
Kaplan–Meier Analysis for MFS, CSS, and BRFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar] [CrossRef]
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.; Wood, C.G.; et al. Outcomes of radical nephroureterectomy: A series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Chien, T.M.; Chan, T.C.; Huang, S.K.; Yeh, B.W.; Li, W.M.; Huang, C.N.; Li, C.C.; Wu, W.J.; Li, C.F. Role of microtu-bule-associated protein 1b in urothelial carcinoma: Overexpression predicts poor prognosis. Cancers (Basel) 2020, 12, 630. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.-C.; Chang, C.-H.; Huang, C.-P.; Huang, C.-Y.; Hong, J.-H.; Tai, T.-Y.; Weng, H.-Y.; Lo, C.-W.; Tsai, C.-Y.; Lee, Y.-K.; et al. Prognostic Significance of Primary Tumor Location in Upper Tract Urothelial Carcinoma Treated with Nephroureterectomy: A Retrospective, Multi-Center Cohort Study in Taiwan. J. Clin. Med. 2020, 9, 3866. [Google Scholar] [CrossRef]
- Mori, K.; Resch, I.; Miura, N.; Laukhtina, E.; Schuettfort, V.M.; Pradere, B.; Katayama, S.; D’Andrea, D.; Parizi, M.K.; Abufaraj, M.; et al. Prognostic role of the systemic immune–inflammation index in upper tract urothelial carcinoma treated with radical nephroureterectomy: Results from a large multicenter international collaboration. Cancer Immunol. Immunother. 2021, 70, 2641–2650. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzis, E.; Albo, G.; Longo, F.; Bebi, C.; Boeri, L.; Montanari, E. Current Knowledge on Genomic Profiling of Upper Tract Urothelial Carcinoma. Genes 2021, 12, 333. [Google Scholar] [CrossRef]
- Robinson, B.D.; Vlachostergios, P.; Bhinder, B.; Liu, W.; Li, K.; Moss, T.J.; Bareja, R.; Park, K.; Tavassoli, P.; Cyrta, J.; et al. Upper tract urothelial carcinoma has a luminal-papillary T-cell depleted contexture and activated FGFR3 signaling. Nat. Commun. 2019, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Janisch, F.; Shariat, S.; Baltzer, P.; Fajkovic, H.; Kimura, S.; Iwata, T.; Korn, P.; Yang, L.; Glybochko, P.; Rink, M.; et al. Diagnostic performance of multidetector computed tomographic (MDCTU) in upper tract urothelial carcinoma (UTUC): A systematic review and meta-analysis. World J. Urol. 2019, 38, 1165–1175. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.; Karin, M. Immunity, Inflammation, and Cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [Green Version]
- Gakis, G.; Todenhöfer, T.; Stenzl, A. The prognostic value of hematological and systemic inflammatory disorders in invasive bladder cancer. Curr. Opin. Urol. 2011, 21, 428–433. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; Kimura, S.; Ferro, M.; Vartolomei, L.; Foerster, B.; Abufaraj, M.; Shariat, S. Is neutrophil-to-lymphocytes ratio a clinical relevant preoperative biomarker in upper tract urothelial carcinoma? A meta-analysis of 4385 patients. World J. Urol. 2018, 36, 1019–1029. [Google Scholar] [CrossRef]
- Bao, Y.; Wang, Y.; Li, X.; Pan, M.; Zhang, H.; Cheng, Z.; Wang, X. Prognostic significance of platelet-to-lymphocyte ratio in urothelial carcinoma patients: A meta-analysis. Cancer Cell Int. 2019, 19, 315. [Google Scholar] [CrossRef]
- Shao, Y.; Li, W.; Wang, D.; Wu, B. Prognostic value of preoperative lymphocyte-related systemic inflammatory biomarkers in upper tract urothelial carcinoma patients treated with radical nephroureterectomy: A systematic review and meta-analysis. World J. Surg. Oncol. 2020, 18, 273. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Gao, Y.; Wu, Y.; Lin, H. Prognostic value of systemic immune-inflammation index in patients with urologic cancers: A meta-analysis. Cancer Cell Int. 2020, 20, 499. [Google Scholar] [CrossRef]
- Li, N. Platelets in cancer metastasis: To help the “villain” to do evil. Int. J. Cancer 2016, 138, 2078–2087. [Google Scholar] [CrossRef]
- Schlesinger, M. Role of platelets and platelet receptors in cancer metastasis. J. Hematol. Oncol. 2018, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Masucci, M.T.; Minopoli, M.; Carriero, M.V. Tumor Associated Neutrophils. Their Role in Tumorigenesis, Metastasis, Prognosis and Therapy. Front. Oncol. 2019, 9, 1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Saxena, S.; Awaji, M.; Singh, R.K. Tumor-Associated Neutrophils in Cancer: Going Pro. Cancers 2019, 11, 564. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Huang, W.; Wu, Y.; Luo, Y.; Wu, B.; Cheng, J.; Chen, J.; Liu, D.; Li, C. Prognostic role of pretreatment blood lymphocyte count in patients with solid tumors: A systematic review and meta-analysis. Cancer Cell Int. 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Shen, J.; Xiao, Z.; Zhao, Q.; Li, M.; Wu, X.; Zhang, L.; Hu, W.; Cho, C.H. Anti-cancer therapy with TNFα and IFNγ: A com-prehensive review. Cell Prolif. 2018, 51, e12441. [Google Scholar] [CrossRef] [Green Version]
- Jan, H.C.; Yang, W.H.; Ou, C.H. Combination of the preoperative systemic immune-inflammation index and mono-cyte-lymphocyte ratio as a novel prognostic factor in patients with upper-tract urothelial carcinoma. Ann. Surg. Oncol. 2019, 26, 669–684. [Google Scholar] [CrossRef]
- Zheng, Y.; Yu, D.; Yu, Z.; Zhao, D.; Chen, Y.; Chen, W.; Li, Y.; Lin, B.; Gao, X. Association of preoperative systemic im-mune-inflammation index and prognostic nutritional index with survival in patients with upper tract urothelial carcinoma. J. Cancer 2020, 11, 5665–5677. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glo-merular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Thouvenin, J.; Chanzá, N.M.; Alhalabi, O.; Lang, H.; Tannir, N.M.; Barthélémy, P.; Malouf, G.G. Efficacy of Immune Checkpoint Inhibitors in Upper Tract Urothelial Carcinomas: Current Knowledge and Future Directions. Cancers 2021, 13, 4341. [Google Scholar] [CrossRef]
- Chovanec, M.; Cierna, Z.; Miskovska, V.; Machalekova, K.; Kalavska, K.; Rejlekova, K.; Svetlovska, D.; Macak, D.; Spanik, S.; Kajo, K.; et al. Systemic immune-inflammation index in germ-cell tumours. Br. J. Cancer 2018, 118, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Shang, J.; Han, X.; Zha, H.; Tao, H.; Li, X.; Yuan, F.; Chen, G.; Wang, L.; Ma, J.; Hu, Y. Systemic Immune-Inflammation Index and Changes of Neutrophil-Lymphocyte Ratio as Prognostic Biomarkers for Patients With Pancreatic Cancer Treated With Immune Checkpoint Blockade. Front. Oncol. 2021, 11, 585271. [Google Scholar] [CrossRef]
- Lalani, A.-K.A.; Xie, W.; Martini, D.; Steinharter, J.A.; Norton, C.K.; Krajewski, K.M.; Duquette, A.; Bossé, D.; Bellmunt, J.; Van Allen, E.M.; et al. Change in neutrophil-to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma. J. Immunother. Cancer 2018, 6, 5. [Google Scholar] [CrossRef]
- Wu, W.J.; Ke, H.-L.; Yang, Y.-H.; Li, C.-C.; Chou, Y.-H.; Huang, C.-H. Should Patients With Primary Upper Urinary Tract Cancer Receive Prophylactic Intravesical Chemotherapy After Nephroureterectomy? J. Urol. 2010, 183, 56–61. [Google Scholar] [CrossRef]
- Li, W.-M.; Shen, J.-T.; Li, C.-C.; Ke, H.-L.; Wei, Y.-C.; Wu, W.J.; Chou, Y.-H.; Huang, C.-H. Oncologic Outcomes Following Three Different Approaches to the Distal Ureter and Bladder Cuff in Nephroureterectomy for Primary Upper Urinary Tract Urothelial Carcinoma. Eur. Urol. 2010, 57, 963–969. [Google Scholar] [CrossRef]
- Chen, C.-H.; Dickman, K.G.; Moriya, M.; Zavadil, J.; Sidorenko, V.S.; Edwards, K.L.; Gnatenko, D.V.; Wu, L.; Turesky, R.J.; Wu, X.-R.; et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc. Natl. Acad. Sci. USA 2012, 109, 8241–8246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.C.; Su, Y.L.; Luo, H.L.; Chen, Y.T.; Sio, T.T.; Hsu, H.C.; Lai, C.H. Sex is a significant prognostic factor for upper tract urothelial carcinoma: A large hospital-based cancer registry study in an endemic area. Front. Oncol. 2019, 9, 157. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Parameters | All | NLR | PLR | SII | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| >2.9 | ≤2.9 | p-Value | >150 | ≤150 | p-Value | >485 | ≤485 | p-Value | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||||
| Age | 0.006 | <0.001 | 0.972 | |||||||
| ≤70 | 208 (55.3) | 70 (46.7) | 138 (61.1) | 28 (35.9) | 180 (60.4) | 116 (55.2) | 92 (55.4) | |||
| >70 | 168 (44.7) | 80 (53.1) | 88 (38.9) | 50 (64.2) | 118 (39.6) | 94 (44.8) | 74 (44.6) | |||
| Gender | 0.214 | 0.263 | 0.601 | |||||||
| Male | 146 (38.8) | 64 (42.7) | 82 (36.3) | 26 (33.3) | 120 (40.3) | 84 (40.0) | 62 (37.3) | |||
| Female | 230 (61.2) | 86 (57.3) | 144 (63.7) | 52 (66.7) | 178 (59.7) | 126 (60.0) | 104 (62.7) | |||
| Hematuria | 0.296 | 0.196 | 0.681 | |||||||
| No | 83 (22.1) | 29 (19.3) | 54 (23.9) | 13 (16.7) | 70 (23.5) | 48 (22.9) | 35 (21.1) | |||
| Yes | 293 (77.9) | 121 (80.7) | 172 (76.1) | 65 (83.3) | 228 (76.5) | 162 (77.1) | 131 (78.9) | |||
| Symptomatic hydronephrosis | 0.014 | 0.572 | 0.021 | |||||||
| No | 330 (87.8) | 124 (82.7) | 206 (91.2) | 67 (85.9) | 263 (88.3) | 177 (84.3) | 153 (92.2) | |||
| Yes | 46 (12.2) | 26 (17.3) | 20 (8.8) | 11 (14.1) | 35 (11.7) | 33 (15.7) | 13 (7.8) | |||
| Bladder cancer history | 0.263 | 0.989 | 0.025 | |||||||
| No | 275 (73.1) | 105 (70.0) | 170 (75.2) | 57 (73.1) | 218 (73.2) | 144 (68.6) | 131 (78.9) | |||
| Yes | 101 (26.9) | 45 (30.0) | 56 (24.8) | 21 (26.9) | 80 (26.8) | 66 (31.4) | 35 (21.1) | |||
| BMI | 0.056 | 0.096 | 0.462 | |||||||
| >27 | 62 (16.5) | 18 (12.0) | 44 (19.5) | 8 (10.3) | 54 (18.1) | 32 (15.2) | 30 (18.1) | |||
| ≤27 | 314 (83.5) | 132 (88.0) | 182 (80.5) | 70 (89.7) | 244 (81.9) | 178 (84.8) | 136 (81.9) | |||
| ESRD | 0.044 | 0.479 | 0.151 | |||||||
| No | 300 (79.8) | 112 (74.7) | 188 (83.2) | 60 (76.9) | 240 (80.5) | 162 (77.1) | 138 (83.1) | |||
| Yes | 76 (20.2) | 38 (25.3) | 38 (16.8) | 18 (23.1) | 58 (19.5) | 48 (22.9) | 28 (16.9) | |||
| Anemia | 0.016 | <0.001 | 0.127 | |||||||
| No | 138 (36.7) | 44 (29.3) | 94 (41.6) | 14 (17.9) | 124 (41.6) | 70 (33.3) | 68 (41.0) | |||
| Yes | 238 (63.3) | 106 (70.7) | 132 (58.4) | 64 (82.1) | 174 (58.4) | 140 (66.7) | 98 (59.0) | |||
| CKD stage | 0.053 | 0.223 | 0.699 | |||||||
| Stage 1 | 36 (9.6) | 6 (4.0) | 30 (13.3) | 4 (5.1) | 32 (10.7) | 18 (8.6) | 18 (10.8) | |||
| Stage 2 | 78 (20.7) | 32 (21.3) | 46 (20.4) | 18 (23.1) | 60 (20.1) | 44 (21.0) | 34 (20.5) | |||
| Stage 3 | 154 (41.0) | 64 (42.7) | 90 (39.8) | 28 (35.9) | 126 (42.3) | 84 (40.0) | 70 (42.2) | |||
| Stage 4 | 24 (6.4) | 10 (6.7) | 14 (6.2) | 8 (10.3) | 16 (5.4) | 12 (5.7) | 12 (7.2) | |||
| Stage 5 | 84 (22.3) | 38 (25.3) | 46 (20.4) | 20 (25.6) | 64 (21.5) | 52 (24.8) | 32 (19.3) | |||
| Advanced CKD stage (Stage 4, 5) | 108 (28.7) | 48 (32.0) | 60 (26.5) | 0.253 | 28 (35.9) | 80 (26.8) | 0.116 | 64 (30.5) | 44 (26.5) | 0.398 |
| Type of operation | 0.304 | 0.712 | 0.093 | |||||||
| Open | 244 (64.9) | 48 (32.0) | 84 (37.2) | 52 (66.7) | 192 (66.4) | 144 (68.6) | 100 (60.2) | |||
| Laparoscopic | 132 (35.1) | 102 (68.0) | 142 (62.8) | 26 (33.3) | 106 (35.6) | 66 (31.4) | 66 (39.8) | |||
| Tumor location | 0.910 | 0.131 | 0.445 | |||||||
| Pyelocaliceal | 170 (45.2) | 68 (45.3) | 102 (45.1) | 42 (53.8) | 128 (43.0) | 98 (46.7) | 72 (43.4) | |||
| Ureteral | 132 (35.1) | 54 (36.0) | 78 (34.5) | 26 (33.3) | 106 (35.6) | 68 (32.4) | 64 (38.6) | |||
| Both | 74 (19.7) | 28 (18.7) | 46 (20.4) | 10 (12.8) | 64 (21.5) | 44 (21.0) | 30 (18.1) | |||
| Multifocality | 0.021 | 0.568 | 0.099 | |||||||
| Single | 298 (79.3) | 110 (73.3) | 188 (83.2) | 60 (76.9) | 238 (79.9) | 160 (76.2) | 138 (83.1) | |||
| Multiple | 78 (20.7) | 40 (26.7) | 38 (16.8) | 18 (23.1) | 60 (20.1) | 50 (23.8) | 28 (16.9) | |||
| Pathologic T stage | 0.001 | 0.018 | 0.017 | |||||||
| pTa/pTis/pT1 | 146 (38.8) | 46 (30.7) | 100 (44.2) | 26 (33.3) | 120 (40.3) | 70 (33.3) | 76 (45.8) | |||
| pT2 | 68 (23.4) | 38 (25.3) | 50 (22.1) | 20 (25.6) | 68 (22.8) | 52 (24.8) | 36 (21.7) | |||
| pT3 | 114 (30.3) | 46 (30.7) | 68 (30.1) | 20 (25.6) | 94 (31.5) | 66 (31.4) | 48 (28.9) | |||
| pT4 | 28 (7.4) | 20 (13.3) | 8 (3.5) | 12 (15.4) | 16 (5.4) | 22 (10.5) | 6 (3.6) | |||
| Advanced pT stage (pT3, pT4) | 0.042 | 0.505 | 0.063 | |||||||
| No | 234 (62.2) | 84 (56.0) | 150 (66.4) | 46 (59.0) | 188 (63.1) | 122 (58.1) | 112 (67.5) | |||
| Yes | 142 (37.8) | 66 (44.0) | 76 (33.6) | 32 (41.0) | 110 (36.9) | 88 (41.9) | 54 (32.5) | |||
| Pathologic N stage | 0.659 | 0.479 | 0.003 | |||||||
| pN0 | 68 (18.1) | 23 (15.3) | 36 (15.9) | 22 (22.4) | 42 (14.1) | 31 (14.8) | 35 (21.1) | |||
| pNx | 232 (61.7) | 95 (63.3) | 146 (64.6) | 58 (59.2) | 198 (66.4) | 125 (59.5) | 109 (65.7) | |||
| pN+ | 76 (20.2) | 32 (21.3) | 44 (19.5) | 18 (23.1) | 58 (19.5) | 54 (25.7) | 22 (13.3) | |||
| Grade | 0.257 | 0.941 | 0.527 | |||||||
| Low | 76 (20.2) | 26 (17.3) | 50 (22.1) | 16 (20.5) | 60 (20.1) | 40 (19.0) | 36 (21.7) | |||
| High | 300 (79.8) | 124 (82.7) | 176 (77.9) | 62 (79.5) | 238 (79.9) | 170 (81.0) | 130 (78.3) | |||
| Concomitant CIS | 0.323 | 0.235 | 0.028 | |||||||
| No | 331 (88.0) | 129 (86.0) | 202 (89.4) | 62 (79.5) | 169 (85.4) | 178 (84.8) | 153 (92.2) | |||
| Yes | 45 (12.0) | 21 (14.0) | 24 (10.6) | 16 (20.5) | 29 (14.6) | 32 (15.2) | 13 (7.8) | |||
| Adjuvant chemotherapy | 0.015 | 0.009 | <0.001 | |||||||
| No | 308 (81.9) | 114 (76.0) | 194 (85.8) | 56 (71.8) | 252 (84.6) | 158 (75.2) | 150 (90.4) | |||
| Yes | 68 (18.1) | 36 (24.0) | 32 (14.2) | 22 (28.2) | 46 (15.4) | 52 (24.8) | 16 (9.6) | |||
| NLR | <0.001 | <0.001 | ||||||||
| >2.9 | - | - | - | 76 (97.4) | 74 (24.8) | 140 (66.7) | 10 (6.0) | |||
| ≤2.9 | - | - | - | 2 (2.6) | 224 (75.2) | 70 (33.3) | 156 (94.0) | |||
| PLR | <0.001 | <0.001 | ||||||||
| >150 | 78 (20.7) | 76 (50.7) | 2 (0.9) | - | - | 78 (37.1) | 0 (0.0) | |||
| ≤150 | 298 (79.3) | 74 (49.3) | 224 (99.1) | - | - | 132 (62.9) | 166 (100.0) | |||
| SII | <0.001 | <0.001 | ||||||||
| >485 | 210 (55.9) | 140 (93.3) | 70 (31.0) | 78 (100.0) | 132 (44.3) | - | - | |||
| ≤485 | 166 (44.1) | 10 (6.7) | 156 (69.0) | 0 (0.0) | 166 (55.7) | - | - | |||
| Parameters | MFS | CSS | BRFS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | p | Multivariate Analysis | p | Univariate Analysis | p | Multivariate Analysis | p | Univariate Analysis | p | Multivariate Analysis | p | |
| HR (95%CI) | HR (95%CI) | HR (95%CI) | HR (95%CI) | HR (95%CI) | HR (95%CI) | |||||||
| Age (Years) | ||||||||||||
| Over 70 years | 1.1 (0.7–1.8) | 0.632 | 1.3 (0.7–2.2) | 0.366 | 1.2 (0.8–1.9) | 0.391 | ||||||
| Gender | ||||||||||||
| Male vs. Female | 1.0 (0.9–1.2) | 0.509 | 1.2 (0.9–1.6) | 0.329 | 2.2 (1.4–3.4) | 0.001 | 2.4 (1.5–4.0) | 0.001 | ||||
| Bladder cancer history | ||||||||||||
| Yes vs. No | 1.3 (1.1–1.5) | 0.004 | 1.2 (0.9–1.4) | 0.586 | 1.2 (0.9–1.5) | 0.126 | 1.8 (1.5–2.1) | <0.001 | 1.6 (1.4–1.9) | <0.001 | ||
| BMI (Kg/m2) | ||||||||||||
| Over 27 Kg/m2 | 1.7 (0.9–3.0) | 0.078 | 2.8 (1.0–7.3) | 0.025 | 6.1 (1.7–21.1) | 0.005 | 1.1 (0.7–1.8) | 0.579 | ||||
| Advanced CKD (Stage 4, 5) | ||||||||||||
| Yes vs. No | 2.0 (1.2–3.2) | 0.004 | 1.2 (0.5–2.7) | 0.686 | 1.6 (0.9–2.9) | 0.103 | 1.2 (0.7–2.0) | 0.453 | ||||
| Hematuria | ||||||||||||
| Yes vs. No | 0.7 (0.6–0.9) | <0.001 | 0.9 (0.7–1.1) | 0.162 | 0.6 (0.5–0.8) | <0.001 | 0.8 (0.6–0.9) | 0.034 | 0.9 (0.8–1.1) | 0.385 | ||
| Symptomatic hydronephrosis | ||||||||||||
| Yes vs. No | 1.5 (1.2–1.8) | <0.001 | 1.4 (1.1–1.7) | 0.002 | 1.9 (1.5–2.4) | <0.001 | 1.6 (1.2–2.1) | <0.001 | 0.7 (0.7–1.1) | 0.051 | ||
| Type of operation | ||||||||||||
| Laparoscopic vs. open | 0.9 (0.6–1.5) | 0.803 | 0.6 (0.3–1.2) | 0.135 | 0.7 (0.4–1.1) | 0.158 | ||||||
| Tumor location | ||||||||||||
| Ureteral vs. Pyelocaliceal | 2.5 (1.1–5.7) | 0.029 | 4.2 (1.3–13.7) | 0.019 | 1.2 (0.7–2.3) | 0.058 | 1.0 (0.6–1.7) | 0.967 | ||||
| Both vs. Ureteral | 1.5 (0.5–4.4) | 0.318 | 1.2 (0.6–2.6) | 0.211 | 1.2 (0.6–2.5) | 0.683 | 1.4 (0.8–2.7) | 0.238 | ||||
| Both vs. Pyelocaliceal | 1.6 (0.6–4.2) | 0.430 | 2.8 (0.8–9.0) | 0.095 | 1.4 (0.7–2.9) | 0.342 | 1.5 (0.8–2.6) | 0.204 | ||||
| Multifocality | ||||||||||||
| Multiple vs. Single | 2.0 (1.2–3.4) | 0.013 | 1.6 (0.7–3.9) | 0.285 | 1.5 (0.8–2.8) | 0.217 | 1.1 (0.7–1.9) | 0.654 | ||||
| Pathologic T stage | ||||||||||||
| pT2 vs. pTa/pTis/pT1 | 3.0 (1.3–7.0) | 0.008 | 1.2 (0.2–6.8) | 0.185 | 1.7 (0.6–4.8) | 0.289 | 1.4 (0.4–4.1) | 0.593 | 1.0 (0.6–1.7) | 0.924 | 1.2 (0.6–2.2) | 0.683 |
| pT3 vs. pTa/pTis/pT1 | 12.2 (5.8–25.7) | <0.001 | 1.8 (0.9–3.5) | 0.177 | 7.3 (3.2–16.6) | <0.001 | 2.2 (1.4–3.5) | 0.001 | 1.1 (0.6–1.8) | 0.803 | 1.4 (0.9–2.1) | 0.133 |
| pT4 vs. pTa/pTis/pT1 | 13.6 (5.1–36.3) | <0.001 | 2.6 (1.5–4.7) | <0.001 | 9.6 (3.3–27.4) | <0.001 | 1.6 (1.1–2.4) | 0.032 | 4.2 (1.1–16.4) | 0.011 | 1.8 (1.1–3.2) | 0.032 |
| Pathologic N stage | ||||||||||||
| pN+ vs. pN0/pNx | 3.8 (2.2–6.4) | <0.001 | 1.2 (0.5–2.9) | 0.640 | 2.3 (1.3–4.3) | 0.006 | 1.3 (0.6–3.0) | 0.467 | 1.1 (0.7–1.7) | 0.604 | ||
| Grade | ||||||||||||
| High vs. Low | 5.7 (2.2–15.0) | <0.001 | 4.4 (1.1–17.9) | 0.039 | 2.3 (1.3–4.2) | 0.032 | 1.1 (0.4–3.6) | 0.830 | 1.9 (1.1–3.1) | 0.020 | 2.5 (1.4–4.4) | 0.010 |
| Concomitant CIS | ||||||||||||
| Yes vs. No | 1.4 (1.2–1.6) | 0.002 | 1.3 (1.3–2.2) | 0.018 | 1.5 (1.2–3.6) | <0.001 | 1.4 (1.2–2.4) | 0.038 | 1.1 (0.8–1.3) | 0.791 | ||
| Adjuvant chemotherapy | ||||||||||||
| Yes vs. No | 43.8 (20.6–93.3) | <0.001 | 40.7 (16.3–101.7) | <0.001 | 8.9 (4.8–16.4) | <0.001 | 6.6 (3.2–13.7) | <0.001 | 4.3 (2.5–7.4) | <0.001 | 4.8 (2.7–8.5) | <0.001 |
| Post-operative installation chemotherapy | ||||||||||||
| Yes vs. No | 0.9 (0.8–1.2) | 0.785 | 1.0 (0.6–1.3) | 0.788 | 1.1 (1.0–1.2) | 0.028 | 1.0 (0.9–1.1) | 0.678 | ||||
| NLR | (>3.5 vs. ≤3.5) | (>2.9 vs. ≤2.9) | (>3.5 vs. ≤3.5) | |||||||||
| 2.3 (1.4–3.7) | <0.001 | 2.2 (1.1–4.3) | 0.021 | 2.7 (1.5–4.7) | <0.001 | 2.3 (1.2–4.3) | 0.009 | 1.3 (0.8–2.0) | 0.253 | |||
| PLR | (>162 vs. ≤162) | (>150 vs. ≤150) | (>160 vs. ≤160) | |||||||||
| 3.1 (1.8–5.2) | <0.001 | 3.6 (1.4–9.4) | 0.009 | 2.2 (1.2–4.1) | 0.009 | 2.0 (1.1–4.0) | 0.046 | 1.0 (0.7–1.5) | 0.910 | |||
| SII | (>460 vs. ≤460) | (>485 vs. ≤485) | (>490 vs. ≤490) | |||||||||
| 3.4 (2.0–5.8) | <0.001 | 2.9 (1.4–6.1) | 0.004 | 3.8 (2.0–7.4) | <0.001 | 3.3 (1.3–8.5) | 0.014 | 1.7 (1.1–2.7) | 0.026 | 1.7 (1.1–2.8) | 0.016 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, T.-M.; Li, C.-C.; Lu, Y.-M.; Chou, Y.-H.; Chang, H.-W.; Wu, W.-J. The Predictive Value of Systemic Immune-Inflammation Index on Bladder Recurrence on Upper Tract Urothelial Carcinoma Outcomes after Radical Nephroureterectomy. J. Clin. Med. 2021, 10, 5273. https://doi.org/10.3390/jcm10225273
Chien T-M, Li C-C, Lu Y-M, Chou Y-H, Chang H-W, Wu W-J. The Predictive Value of Systemic Immune-Inflammation Index on Bladder Recurrence on Upper Tract Urothelial Carcinoma Outcomes after Radical Nephroureterectomy. Journal of Clinical Medicine. 2021; 10(22):5273. https://doi.org/10.3390/jcm10225273
Chicago/Turabian StyleChien, Tsu-Ming, Ching-Chia Li, Yen-Man Lu, Yii-Her Chou, Hsueh-Wei Chang, and Wen-Jeng Wu. 2021. "The Predictive Value of Systemic Immune-Inflammation Index on Bladder Recurrence on Upper Tract Urothelial Carcinoma Outcomes after Radical Nephroureterectomy" Journal of Clinical Medicine 10, no. 22: 5273. https://doi.org/10.3390/jcm10225273
APA StyleChien, T.-M., Li, C.-C., Lu, Y.-M., Chou, Y.-H., Chang, H.-W., & Wu, W.-J. (2021). The Predictive Value of Systemic Immune-Inflammation Index on Bladder Recurrence on Upper Tract Urothelial Carcinoma Outcomes after Radical Nephroureterectomy. Journal of Clinical Medicine, 10(22), 5273. https://doi.org/10.3390/jcm10225273