
Association of Plasma Branched-Chain and Aromatic Amino Acids with Reduction in Kidney Function Evaluated in Apparently Healthy Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
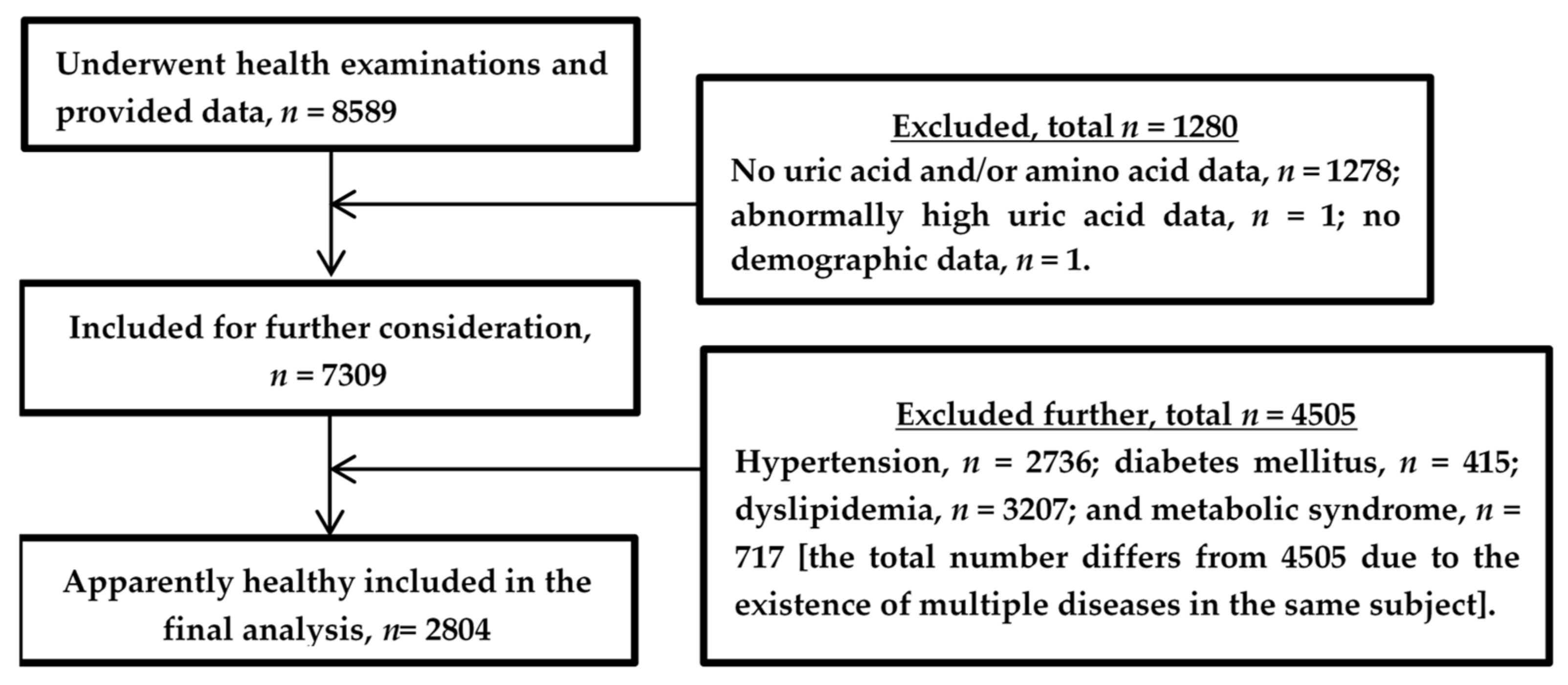
2.1. Study Design, Population, and Data Collection
2.2. Collection and Storage of Blood Samples
2.3. Measurement of Amino Acids and Other Laboratory Variables
2.4. Calculation of eGFR
2.5. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of the Study Subjects
3.2. Differences in the Concentrations of BCAAs and AAAs between eGFR Tertiles
3.3. Correlation between BCAAs and AAAs
3.4. Association of BCAAs and AAAs with eGFR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Said, S.; Hernandez, G.T. The link between chronic kidney disease and cardiovascular disease. J. Nephropathol. 2014, 3, 99–104. [Google Scholar] [CrossRef]
- Kelly, D.; Rothwell, P.M. Disentangling the multiple links between renal dysfunction and cerebrovascular disease. J. Neurol. Neurosurg. Psychiatry 2020, 91, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Zadrazil, J.; Horak, P. Pathophysiology of anemia in chronic kidney diseases: A review. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2015, 159, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Collins, A.J.; Yee, J. Infectious complications in patients with chronic kidney disease. Adv. Chronic Kidney Dis. 2006, 13, 197–198. [Google Scholar] [CrossRef]
- Michna, M.; Kovarova, L.; Valerianova, A.; Malikova, H.; Weichet, J.; Malik, J. Review of the structural and functional brain changes associated with chronic kidney disease. Physiol. Res. 2020, 69, 1013–1028. [Google Scholar] [CrossRef] [PubMed]
- Arinze, N.V.; Gregory, A.; Francis, J.M.; Farber, A.; Chitalia, V.C. Unique aspects of peripheral artery disease in patients with chronic kidney disease. Vasc. Med. 2019, 24, 51–260. [Google Scholar] [CrossRef]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckardt, K.U.; Coresh, J.; Devuyst, O.; Johnson, R.J.; Köttgen, A.; Levey, A.S.; Levin, A. Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 2013, 382, 158–169. [Google Scholar] [CrossRef] [Green Version]
- Yamakado, M.; Nagao, K.; Imaizumi, A.; Tani, M.; Toda, A.; Tanaka, T.; Jinzu, H.; Miyano, H.; Yamamoto, H.; Daimon, T.; et al. Plasma Free Amino Acid Profiles Predict Four-Year Risk of Developing Diabetes, Metabolic Syndrome, Dyslipidemia, and Hypertension in Japanese Population. Sci. Rep. 2015, 5, 11918. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Dai, J.; Kang, H. The construction of a panel of serum amino acids for the identification of early chronic kidney disease patients. J. Clin. Lab. Anal. 2018, 32, e22282. [Google Scholar] [CrossRef]
- Lai, H.S.; Lee, J.C.; Lee, P.H.; Wang, S.T.; Chen, W.J. Plasma free amino acid profile in cancer patients. Semin. Cancer Biol. 2005, 15, 267–276. [Google Scholar] [CrossRef]
- Nagao, K.; Kimura, T. Use of plasma-free amino acids as biomarkers for detecting and predicting disease risk. Nutr. Rev. 2020, 78, 79–85. [Google Scholar] [CrossRef]
- Socha, E.; Koba, M.; Kośliński, P. Amino acid profiling as a method of discovering biomarkers for diagnosis of neurodegenerative diseases. Amino Acids 2019, 51, 367–371. [Google Scholar] [CrossRef]
- Yamaguchi, N.; Mahbub, M.H.; Takahashi, H.; Hase, R.; Ishimaru, Y.; Sunagawa, H.; Amano, H.; Kobayashi-Miura, M.; Kanda, H.; Fujita, Y.; et al. Plasma free amino acid profiles evaluate risk of metabolic syndrome, diabetes, dyslipidemia, and hypertension in a large Asian population. Environ. Health Prev. Med. 2017, 22, 35. [Google Scholar] [CrossRef] [Green Version]
- Newgard, C.B. Metabolomics and Metabolic Diseases: Where Do We Stand? Cell Metab. 2017, 25, 43–56. [Google Scholar] [CrossRef] [Green Version]
- Weng, L.; Quinlivan, E.; Gong, Y.; Beitelshees, A.L.; Shahin, M.H.; Turner, S.T.; Chapman, A.B.; Gums, J.G.; Johnson, J.A.; Frye, R.F.; et al. Association of branched and aromatic amino acids levels with metabolic syndrome and impaired fasting glucose in hypertensive patients. Metab. Syndr. Relat. Disord. 2015, 13, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Kumar, M.A.; Bitla, A.R.; Raju, K.V.; Manohar, S.M.; Kumar, V.S.; Narasimha, S.R. Branched chain amino acid profile in early chronic kidney disease. Saudi J. Kidney Dis. Transpl. 2012, 23, 1202–1207. [Google Scholar] [CrossRef]
- Li, Y.; Tang, A.G.; Mu, S. HPLC-FLD determination of serum aromatic amino acids: Application in chronic kidney disease patients. Clin. Chim. Acta 2011, 412, 1032–1035. [Google Scholar] [CrossRef]
- Suliman, M.E.; Qureshi, A.R.; Stenvinkel, P.; Pecoits-Filho, R.; Bárány, P.; Heimbürger, O.; Anderstam, B.; Rodríguez Ayala, E.; Divino Filho, J.C.; Alvestrand, A. Inflammation contributes to low plasma amino acid concentrations in patients with chronic kidney disease. Am. J. Clin. Nutr. 2005, 82, 342–349. [Google Scholar] [CrossRef]
- Young, G.A.; Swanepoel, C.R.; Croft, M.R.; Hobson, S.M.; Parsons, F.M. Anthropometry and plasma valine, amino acids, and proteins in the nutritional assessment of hemodialysis patients. Kidney Int. 1982, 21, 492–499. [Google Scholar] [CrossRef] [Green Version]
- Ceballos, I.; Chauveau, P.; Guerin, V.; Bardet, J.; Parvy, P.; Kamoun, P.; Jungers, P. Early alterations of plasma free amino acids in chronic renal failure. Clin. Chim. Acta 1990, 188, 101–108. [Google Scholar] [CrossRef]
- Mahbub, M.H.; Yamaguchi, N.; Takahashi, H.; Hase, R.; Yamamoto, H.; Kikuchi, S.; Tanabe, T. Relationship of reduced glomerular filtration rate with alterations in plasma free amino acids and uric acid evaluated in healthy control and hypertensive subjects. Sci. Rep. 2019, 9, 10252. [Google Scholar] [CrossRef]
- Mahbub, M.H.; Yamaguchi, N.; Hase, R.; Takahashi, H.; Ishimaru, Y.; Watanabe, R.; Saito, H.; Shimokawa, J.; Yamamoto, H.; Kikuchi, S.; et al. Plasma Branched-Chain and Aromatic Amino Acids in Relation to Hypertension. Nutrients 2020, 12, 3791. [Google Scholar] [CrossRef]
- Shimbo, K.; Oonuki, T.; Yahashi, A.; Hirayama, K.; Miyano, H. Precolumn derivatization reagents for high-speed analysis of amines and amino acids in biological fluid using liquid chromatography/electrospray ionization tandem mass spectrometry. Rapid Commun. Mass. Spectrom. 2009, 23, 1483–1492. [Google Scholar] [CrossRef]
- Shimbo, K.; Yahashi, A.; Hirayama, K.; Nakazawa, M.; Miyano, H. Multifunctional and highly sensitive precolumn reagents for amino acids in liquid chromatography/tandem mass spectrometry. Anal. Chem. 2009, 81, 5172–5179. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Garibotto, G.; Sofia, A.; Saffioti, S.; Bonanni, A.; Mannucci, I.; Verzola, D. Amino acid and protein metabolism in the human kidney and in patients with chronic kidney disease. Clin. Nutr. 2010, 29, 424–433. [Google Scholar] [CrossRef]
- Lynch, C.J.; Adams, S.H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 2014, 10, 723–736. [Google Scholar] [CrossRef] [Green Version]
- Bowe, B.; Xie, Y.; Xian, H.; Lian, M.; Al-Aly, Z. Geographic Variation and US County Characteristics Associated With Rapid Kidney Function Decline. Kidney Int. Rep. 2016, 2, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Wildman, R.P.; Gu, D.; Kusek, J.W.; Spruill, M.; Reynolds, K.; Liu, D.; Hamm, L.L.; Whelton, P.K.; He, J. Prevalence of decreased kidney function in Chinese adults aged 35 to 74 years. Kidney Int. 2005, 68, 2837–2845. [Google Scholar] [CrossRef] [Green Version]
- Bellomo, G.; Venanzi, S.; Verdura, C.; Saronio, P.; Esposito, A.; Timio, M. Association of uric acid with change in kidney function in healthy normotensive individuals. Am. J. Kidney Dis. 2010, 56, 264–272. [Google Scholar] [CrossRef]
- Giordano, C.; Karasik, O.; King-Morris, K.; Asmar, A. Uric Acid as a Marker of Kidney Disease: Review of the Current Literature. Dis. Markers 2015, 2015, 382918. [Google Scholar] [CrossRef] [Green Version]
- Tizianello, A.; Deferrari, G.; Garibotto, G.; Robaudo, C.; Salvidio, G.; Saffioti, S. Renal ammoniagenesis in the postprandial period. Contrib. Nephrol. 1985, 47, 44–57. [Google Scholar] [CrossRef]
- Van de Poll, M.C.; Soeters, P.B.; Deutz, N.E.; Fearon, K.C.; Dejong, C.H. Renal metabolism of amino acids: Its role in interorgan amino acid exchange. Am. J. Clin. Nutr. 2004, 79, 185–197. [Google Scholar] [CrossRef] [Green Version]
- Fernstrom, J.D. Branched-chain amino acids and brain function. J. Nutr. 2005, 135, 1539S–1546S. [Google Scholar] [CrossRef]
- Shah, S.H.; Crosslin, D.R.; Haynes, C.S.; Nelson, S.; Turer, C.B.; Stevens, R.D.; Muehlbauer, M.J.; Wenner, B.R.; Bain, J.R.; Laferrère, B.; et al. Branched-chain amino acid levels are associated with improvement in insulin resistance with weight loss. Diabetologia 2012, 55, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Jones, M.R.; Kopple, J.D.; Swendseid, M.E. Phenylalanine metabolism in uremic and normal man. Kidney Int. 1978, 14, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Jang, H.B.; Yoo, M.G.; Park, S.I.; Lee, H.J. Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study. Biomedicines 2020, 8, 222. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total | Tertile 1 | Tertile 2 | Tertile 3 | P1 | P2 | P3 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 2804) | (n = 935) | (n = 933) | (n = 936) | ||||||||
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | ||||
| or n | or % | or n | or % | or n | or % | or n | or % | ||||
| Age (years) | 44.0 | 26.0 | 59.0 | 23.0 | 44.0 | 22.0 | 34.0 | 15.0 | <0.001 | <0.001 | <0.001 |
| Sex | |||||||||||
| Male | 1191 | 42.5 | 413 | 44.2 | 427 | 45.8 | 351 | 29.5 | <0.005 | <0.01 | <0.001 |
| Female | 1613 | 57.5 | 522 | 55.8 | 506 | 54.2 | 585 | 36.3 | |||
| BMI (kg/m2) | 21.2 | 3.7 | 21.5 | 3.7 | 21.4 | 3.8 | 20.8 | 3.6 | <0.001 | <0.001 | <0.005 |
| FPG (mg/dL) | 91 | 10 | 92 | 10 | 91 | 10 | 90 | 9 | <0.001 | <0.001 | <0.005 |
| HbA1c (%) | 5.5 | 0.5 | 5.6 | 0.4 | 5.5 | 0.5 | 5.4 | 0.4 | <0.001 | <0.001 | <0.001 |
| HDLC (mg/dL) | 68 | 22 | 67 | 22 | 69 | 22 | 68 | 20 | <0.05 | <0.05 | 1.000 |
| LDLC (mg/dL) | 107 | 31 | 112 | 28 | 108 | 31 | 102 | 30 | <0.001 | <0.001 | <0.001 |
| SBP (mmHg) | 118 | 17 | 120 | 17 | 119 | 16 | 116 | 15 | <0.001 | <0.001 | <0.001 |
| DBP (mmHg) | 73 | 13 | 74 | 12 | 74 | 12.5 | 71 | 13 | <0.001 | <0.001 | <0.001 |
| TG (mg/dL) | 64 | 38 | 71 | 36 | 64 | 38 | 58 | 35 | <0.001 | <0.001 | <0.001 |
| UA (mg/dL) | 4.6 | 1.8 | 4.9 | 1.8 | 4.6 | 1.9 | 4.3 | 1.7 | <0.001 | <0.001 | <0.001 |
| Waist (cm) | 76 | 11.5 | 78 | 11.5 | 76.5 | 10.5 | 74 | 11 | <0.001 | <0.001 | <0.001 |
| eGFR (mL/min/1.73 m2) | 84.9 | 21.2 | 70.9 | 9.7 | 84.9 | 6.6 | 101.7 | 13.5 | <0.001 | <0.001 | <0.001 |
| Tertile 1 | Tertile 2 | Tertile 3 | P1 | P2 | P3 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Amino | (n = 935) | (n = 937) | (n = 932) | ||||||
| Acids | Median | IQR | Median | IQR | Median | IQR | |||
| Ile | 52.7 | 16.6 | 51.5 | 16.7 | 50.8 | 14.6 | <0.005 | <0.001 | 0.128 |
| Leu | 105.1 | 28.9 | 103.1 | 30.0 | 99.2 | 29.0 | <0.001 | <0.001 | <0.005 |
| Val | 194.6 | 52.8 | 191.6 | 49.7 | 187.0 | 49.0 | <0.001 | <0.001 | <0.05 |
| Phe | 56.4 | 10.3 | 53.7 | 9.0 | 51.3 | 9.0 | <0.001 | <0.001 | <0.001 |
| Trp | 51.6 | 11.7 | 51.6 | 12.1 | 50.6 | 12.0 | 0.059 | 0.074 | 0.084 |
| Tyr | 59.4 | 14.8 | 57.4 | 14.6 | 54.3 | 13.3 | <0.001 | <0.001 | <0.001 |
| Amino | Tertile 1 | Tertile 2 | Tertile 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Acids | Phe | Trp | Tyr | Phe | Trp | Tyr | Phe | Trp | Tyr |
| Ile | 0.49 * | 0.51 * | 0.43 * | 0.48 * | 0.53 * | 0.41 * | 0.48 * | 0.51 * | 0.41 * |
| Leu | 0.56 * | 0.54 * | 0.44 * | 0.59 * | 0.57 * | 0.47 * | 0.59 * | 0.58 * | 0.47 * |
| Val | 0.51 * | 0.54 * | 0.44 * | 0.53 * | 0.55 * | 0.49 * | 0.51 * | 0.56 * | 0.45 * |
| eGFR | Model 1 a | Model 2 b | Model 3 c | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amino | Tertile | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Acids | Categories | Lower | Upper | Lower | Upper | Lower | Upper | ||||||
| Ile | Tertile 3 | Ref | Ref | Ref | |||||||||
| Tertile 2 | 1.05 | 0.92 | 1.19 | 0.461 | 1.10 | 0.97 | 1.26 | 0.152 | 1.08 | 0.94 | 1.24 | 0.271 | |
| Tertile 1 | 1.29 | 1.13 | 1.47 | <0.001 | 1.29 | 1.11 | 1.49 | <0.005 | 1.21 | 1.04 | 1.41 | <0.05 | |
| Leu | Tertile 3 | Ref | Ref | Ref | |||||||||
| Tertile 2 | 1.12 | 0.98 | 1.28 | 0.103 | 1.17 | 1.02 | 1.35 | 0.027 | 1.12 | 0.97 | 1.29 | 0.124 | |
| Tertile 1 | 1.42 | 1.23 | 1.64 | <0.001 | 1.38 | 1.18 | 1.62 | <0.001 | 1.24 | 1.06 | 1.46 | <0.01 | |
| Val | Tertile 3 | Ref | Ref | Ref | |||||||||
| Tertile 2 | 0.99 | 0.87 | 1.13 | 0.933 | 1.06 | 0.92 | 1.21 | 0.451 | 1.01 | 0.87 | 1.16 | 0.948 | |
| Tertile 1 | 1.13 | 0.98 | 1.30 | 0.102 | 1.10 | 0.94 | 1.28 | 0.242 | 0.98 | 0.83 | 1.15 | 0.782 | |
| Phe | Tertile 3 | Ref | Ref | Ref | |||||||||
| Tertile 2 | 1.22 | 1.06 | 1.39 | <0.005 | 1.24 | 1.08 | 1.43 | <0.005 | 1.21 | 1.05 | 1.39 | <0.01 | |
| Tertile 1 | 1.59 | 1.38 | 1.83 | <0.001 | 1.65 | 1.41 | 1.92 | <0.001 | 1.53 | 1.31 | 1.78 | <0.001 | |
| Trp | Tertile 3 | Ref | Ref | Ref | |||||||||
| Tertile 2 | 0.95 | 0.84 | 1.07 | 0.399 | 0.93 | 0.82 | 1.06 | 0.265 | 0.92 | 0.81 | 1.04 | 0.165 | |
| Tertile 1 | 0.93 | 0.82 | 1.06 | 0.293 | 0.89 | 0.78 | 1.03 | 0.121 | 0.87 | 0.76 | 1.01 | 0.064 | |
| Tyr | Tertile 3 | Ref | Ref | Ref | |||||||||
| Tertile 2 | 0.98 | 0.86 | 1.12 | 0.775 | 1.01 | 0.88 | 1.17 | 0.897 | 0.97 | 0.84 | 1.12 | 0.681 | |
| Tertile 1 | 0.98 | 0.86 | 1.12 | 0.775 | 0.98 | 0.83 | 1.15 | 0.776 | 0.89 | 0.76 | 1.05 | 0.169 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahbub, M.; Yamaguchi, N.; Nakagami, Y.; Hase, R.; Takahashi, H.; Ishimaru, Y.; Watanabe, R.; Saito, H.; Shimokawa, J.; Yamamoto, H.; et al. Association of Plasma Branched-Chain and Aromatic Amino Acids with Reduction in Kidney Function Evaluated in Apparently Healthy Adults. J. Clin. Med. 2021, 10, 5234. https://doi.org/10.3390/jcm10225234
Mahbub M, Yamaguchi N, Nakagami Y, Hase R, Takahashi H, Ishimaru Y, Watanabe R, Saito H, Shimokawa J, Yamamoto H, et al. Association of Plasma Branched-Chain and Aromatic Amino Acids with Reduction in Kidney Function Evaluated in Apparently Healthy Adults. Journal of Clinical Medicine. 2021; 10(22):5234. https://doi.org/10.3390/jcm10225234
Chicago/Turabian StyleMahbub, MH, Natsu Yamaguchi, Yuki Nakagami, Ryosuke Hase, Hidekazu Takahashi, Yasutaka Ishimaru, Rie Watanabe, Hiroyuki Saito, Junki Shimokawa, Hiroshi Yamamoto, and et al. 2021. "Association of Plasma Branched-Chain and Aromatic Amino Acids with Reduction in Kidney Function Evaluated in Apparently Healthy Adults" Journal of Clinical Medicine 10, no. 22: 5234. https://doi.org/10.3390/jcm10225234
APA StyleMahbub, M., Yamaguchi, N., Nakagami, Y., Hase, R., Takahashi, H., Ishimaru, Y., Watanabe, R., Saito, H., Shimokawa, J., Yamamoto, H., Kikuchi, S., & Tanabe, T. (2021). Association of Plasma Branched-Chain and Aromatic Amino Acids with Reduction in Kidney Function Evaluated in Apparently Healthy Adults. Journal of Clinical Medicine, 10(22), 5234. https://doi.org/10.3390/jcm10225234