
Effect of Biofeedback Therapy during Temporary Stoma Period in Rectal Cancer Patients: A Prospective Randomized Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
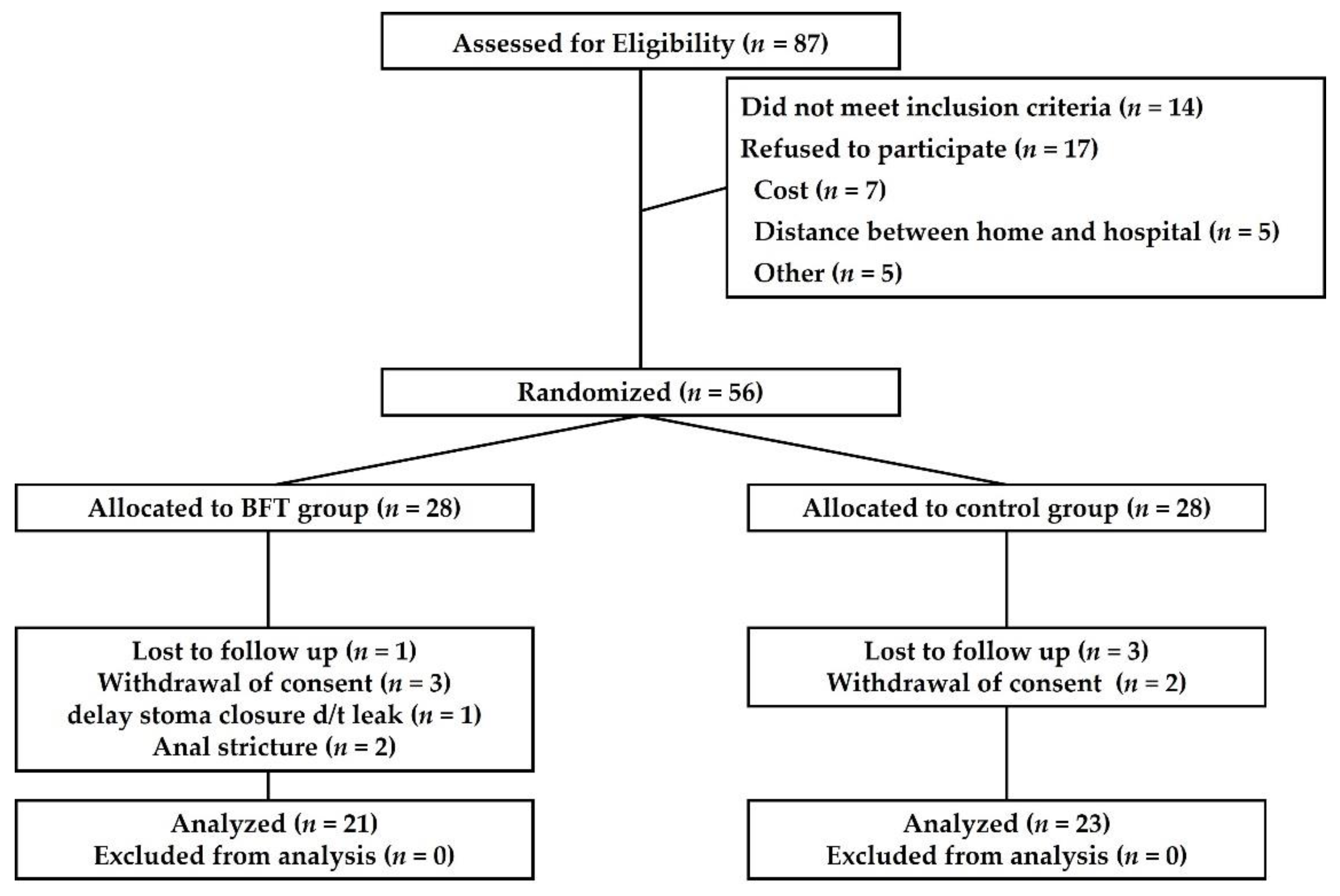
2.3. Randomization and Sample Size
2.4. Biofeedback Therapy & Kegel Exercise
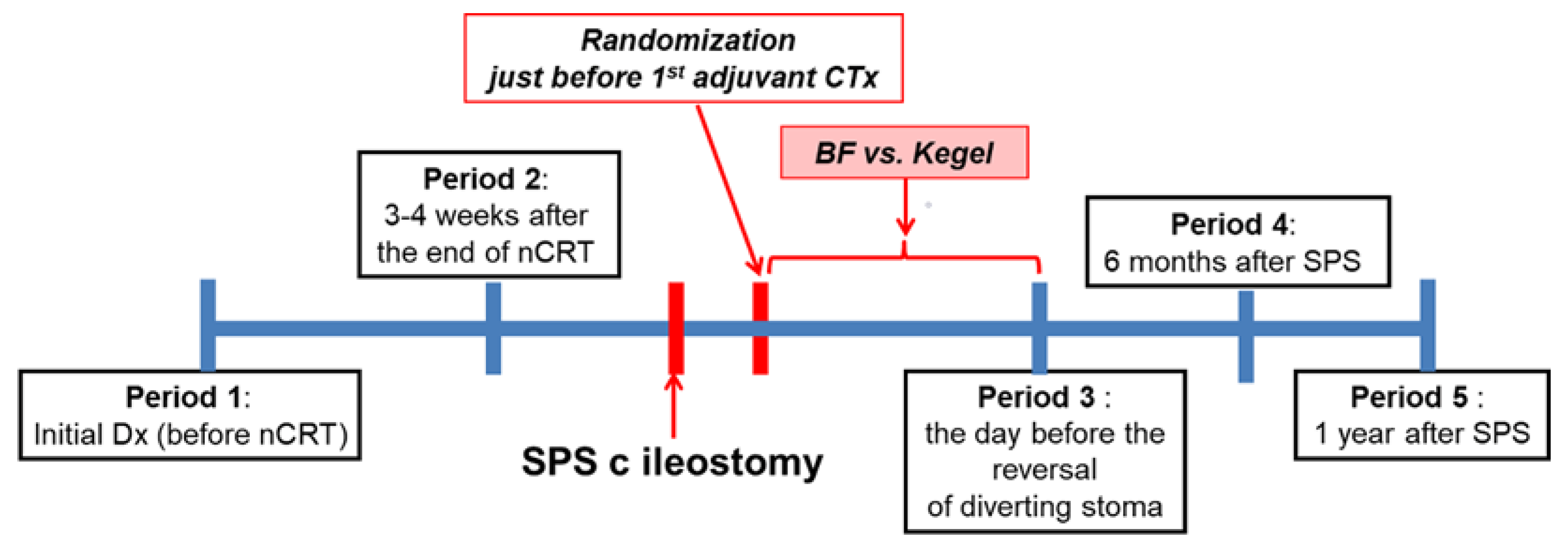
2.5. Study Design
2.6. Primary End Point
2.7. Secondary End Points
2.8. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leibold, T.; Guillem, J.G. The Role of Neoadjuvant Therapy in Sphincter-Saving Surgery for Mid and Distal Rectal Cancer. Cancer Investig. 2010, 28, 259–267. [Google Scholar] [CrossRef]
- Kulu, Y.; Ulrich, A.; Büchler, M.W. Resectable Rectal Cancer: Which Patient Does Not Need Preoperative Radiotherapy? Dig. Dis. 2012, 30, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Weiser, M.R.; Quah, H.-M.; Shia, J.; Guillem, J.G.; Paty, P.B.; Temple, L.K.; Goodman, K.A.; Minsky, B.D.; Wong, W.D. Sphincter Preservation in Low Rectal Cancer is Facilitated by Preoperative Chemoradiation and Intersphincteric Dissection. Ann. Surg. 2009, 249, 236–242. [Google Scholar] [CrossRef]
- Kye, B.-H.; Kim, J.-G.; Cho, H.-M.; Kim, H.-J.; Chun, C.-S. Laparoscopic Abdominal Transanal Proctocolectomy with Coloanal Anastomosis Is a Good Surgical Option in Selective Patients with Low-Lying Rectal Cancer: A Retrospective Analysis Based on a Single Surgeon’s Experience. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 269–277. [Google Scholar] [CrossRef]
- Kang, S.-B.; Cho, J.R.; Jeong, S.-Y.; Oh, J.H.; Ahn, S.; Choi, S.; Kim, D.-W.; Lee, B.H.; Youk, E.G.; Park, S.C.; et al. Quality of life after sphincter preservation surgery or abdominoperineal resection for low rectal cancer (ASPIRE): A long-term prospective, multicentre, cohort study. Lancet Reg. Health-West. 2020, 28, 100087. [Google Scholar] [CrossRef]
- Dulskas, A.; Kavaliauskas, P.; Pilipavicius, L.; Jodinskas, M.; Mikalonis, M.; Samalavicius, N.E. Long-term bowel dysfunction following low anterior resection. Sci. Rep. 2020, 10, 11882. [Google Scholar] [CrossRef]
- Scarlett, Y. Medical management of fecal incontinence. Gastroenterology 2004, 126, S55–S63. [Google Scholar] [CrossRef] [PubMed]
- Pachler, J.; Wille-Jørgensen, P. Quality of life after rectal resection for cancer, with or without permanent colostomy. Cochrane Database Syst. Rev. 2005, 2, CD004323. [Google Scholar]
- Cornish, J.A.; Tilney, H.S.; Heriot, A.G.; Lavery, I.C.; Fazio, V.W.; Tekkis, P.P. A Meta-Analysis of Quality of Life for Abdominoperineal Excision of Rectum versus Anterior Resection for Rectal Cancer. Ann. Surg. Oncol. 2007, 14, 2056–2068. [Google Scholar] [CrossRef]
- Temple, L.K.F. Expert Commentary on Low Anterior Resection Syndrome. Dis. Colon Rectum 2019, 62, 1423–1424. [Google Scholar] [CrossRef]
- Bryant, C.L.; Lunniss, P.J.; Knowles, C.H.; Thaha, M.A.; Chan, C.L. Anterior resection syndrome. Lancet Oncol. 2012, 13, 403–408. [Google Scholar] [CrossRef]
- Lee, K.H.; Kim, J.S.; Kim, J.Y. Efficacy of biofeedback therapy for objective improvement of pelvic function in low anterior resection syndrome. Ann. Surg. Treat. Res. 2019, 97, 194–201. [Google Scholar] [CrossRef]
- Kye, B.H.; Kim, H.J.; Kim, G.; Yoo, R.N.; Cho, H.M. The Effect of Biofeedback Therapy on Anorectal Function After the Reversal of Temporary Stoma When Administered During the Temporary Stoma Period in Rectal Cancer Patients with Sphincter-Saving Surgery The Interim Report of a Prospective Randomized Controlled Trial. Medicine 2016, 95, e3611. [Google Scholar] [PubMed]
- Croese, A.D.; Lonie, J.M.; Trollope, A.F.; Vangaveti, V.N.; Ho, Y.-H. A meta-analysis of the prevalence of Low Anterior Resection Syndrome and systematic review of risk factors. Int. J. Surg. 2018, 56, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Dulskas, A.; Smolskas, E.; Kildusiene, I.; Samalavicius, N.E. Treatment possibilities for low anterior resection syndrome: A review of the literature. Int. J. Colorectal Dis. 2018, 33, 251–260. [Google Scholar] [CrossRef]
- Byrne, C.M.; Solomon, M.J.; Young, J.M.; Rex, J.; Merlino, C.L. Biofeedback for Fecal Incontinence: Short-Term Outcomes of 513 Consecutive Patients and Predictors of Successful Treatment. Dis. Colon Rectum 2007, 50, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Pucciani, F.; Ringressi, M.N.; Redditi, S.; Masi, A.; Giani, I. Rehabilitation of Fecal Incontinence After Sphincter-Saving Surgery for Rectal Cancer: Encouraging Results. Dis. Colon Rectum 2008, 51, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Yu, C.S.; Yoon, Y.S.; Yoon, S.N.; Lim, S.-B.; Kim, J.C. Effectiveness of Biofeedback Therapy in the Treatment of Anterior Resection Syndrome After Rectal Cancer Surgery. Dis. Colon Rectum 2011, 54, 1107–1113. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus Postoperative Chemoradiotherapy for Rectal Cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [Green Version]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; Van Krieken, J.H.; et al. Preoperative Radiotherapy Combined with Total Mesorectal Excision for Resectable Rectal Cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [Green Version]
- Wells, C.; Vather, R.; Chu, M.J.J.; Robertson, J.P.; Bissett, I.P. Anterior Resection Syndrome—A Risk Factor Analysis. J. Gastrointest. Surg. 2015, 19, 350–359. [Google Scholar] [CrossRef]
- Bø, K. Can pelvic floor muscle training prevent and treat pelvic organ prolapse? Acta Obstet. Gynecol. Scand. 2006, 85, 263–268. [Google Scholar] [CrossRef]
- Hunter, K.F.; Moore, K.N.; Cody, D.J.; Glazener, C.M. Conservative management for postprostatectomy urinary incontinence. Cochrane Database Syst. Rev. 2004, 2, CD001843. [Google Scholar] [CrossRef] [Green Version]
- Nahon, I.; Dorey, G.; Waddington, G.; Adams, R. Systematic review of the treatment of post-prostatectomy incontinence. Urol. Nurs. 2006, 26, 461–475. [Google Scholar]
- Visser, W.S.; Riele, W.W.T.; Boerma, D.; Van Ramshorst, B.; Van Westreenen, H.L. Pelvic Floor Rehabilitation to Improve Functional Outcome After a Low Anterior Resection: A Systematic Review. Ann. Coloproctol. 2014, 30, 109–114. [Google Scholar] [CrossRef] [Green Version]
- Pehl, C.; Seidl, H.; Scalercio, N.; Gundling, F.; Schmidt, T.; Schepp, W.; Labermeyer, S. Accuracy of Anorectal Manometry in Patients with Fecal Incontinence. Digestion 2012, 86, 78–85. [Google Scholar] [CrossRef]
- Bregendahl, S.; Emmertsen, K.J.; Fassov, J.; Krogh, K.; Zhao, J.; Gregersen, H.; Laurberg, S. Neorectal hyposensitivity after neoadjuvant therapy for rectal cancer. Radiother. Oncol. 2013, 108, 331–336. [Google Scholar] [CrossRef]
- Schiller, L.R. Faecal incontinence. Clin. Gastroenterol. 1986, 15, 687–704. [Google Scholar] [CrossRef]
- Yoo, R.N.; Cho, H.-M.; Kye, B.-H.; Kim, H.J.; Shin, S.; Kim, G. Rapid transit in the left-sided colon is related to poor defecatory function at early period after stoma closure. Sci. Rep. 2020, 10, 3739. [Google Scholar] [CrossRef]
- Gallas, S.; Michot, F.; Faucheron, J.L.; Barth, X.; Sielezneff, I.; Orsoni, P.; Desfourneaux, V.; Meurette, G.; Lehur, P.A.; Damon, H.; et al. Predictive factors for successful sacral nerve stimulation in the treatment of faecal incontinence: Results of trial stimulation in 200 patients. Colorectal Dis. 2010, 13, 689–696. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BFT Group (n = 21) | Control Group (n = 23) | p-Value | ||
|---|---|---|---|---|
| Age | ≤65 years | 15 (71.4%) | 12 (52.2%) | |
| >65 years | 6 (28.6%) | 11 (47.8%) | 0.228 | |
| Sex | male | 11 (52.4%) | 14 (60.9%) | |
| female | 10 (47.6%) | 9 (39.1%) | 0.761 | |
| Initial tumor location (cm from anal verge) | ≤5 cm | 5 (23.8%) | 5 (21.7%) | |
| >5 cm | 16 (76.2%) | 18 (78.3%) | 1.000 | |
| Mean ± SD | 7.26 ± 2.07 | 7.83 ± 2.59 | 0.433 | |
| Anastomosis method | S-CR | 16 (76.2%) | 21 (91.3%) | |
| H-CA | 5 (23.8%) | 2 (8.7%) | 0.232 | |
| Location of anastomosis (cm from anal verge) | <3 cm | 6 (28.6%) | 3 (13.0%) | |
| ≥3 cm | 15 (71.4%) | 20 (87.0%) | 0.272 | |
| Mean ± SD | 3.71 ± 1.48 | 3.96 ± 1.46 | 0.589 |
| Initial Tumor Location (From Anal Verge) | Anastomosis Method | Anastomosis Location (From Anal Verge) | Treatment | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤5 cm | >5 cm | p-Value | S-CR | H-CA | p-Value | < 3cm | ≥3 cm | p-Value | BFT Group | Control Group | p-Value | |||
| CCIS | ≤9 | 2 (20.0%) | 16 (47.1%) | 17 (45.9%) | 1 (14.3%) | 3 (33.3%) | 15 (42.9%) | 9 (42.9%) | 9 (39.1%) | |||||
| >9 | 8 (80.0%) | 18 (52.9%) | 0.161 | 20 (54.1%) | 6 (85.7%) | 0.211 | 6 (66.7%) | 20 (57.1%) | 0.716 | 12 (57.1%) | 14 (60.9%) | 1.000 | ||
| Type of incontinence | Gas | Never | 0 | 7 (20.6%) | 0.066 | 7 (18.9%) | 0 | 0.245 | 1 (5.2%) | 6 (24%) | 0.017 | 4 (19.0%) | 3 (13.0%) | 0.071 |
| Rarely | 0 | 5 (14.7%) | 4 (10.8%) | 1 (14.3%) | 1 (5.2%) | 4 (16%) | 4 (19.0%) | 1 (4.3%) | ||||||
| Sometimes | 1 (10.0%) | 7 (20.6%) | 8 (21.6%) | 0 | 1 (5.2%) | 7 (28%) | 1 (4.8%) | 7 (30.4%) | ||||||
| Usually | 6 (60.0%) | 13 (38.2%) | 15 (40.5%) | 4 (57.1%) | 13 (68.4%) | 6 (24%) | 11 (52.4%) | 8 (34.8%) | ||||||
| Always | 3 (30.0%) | 2 (5.9%) | 3 (8.2%) | 2 (28.6%) | 3 (16.0%) | 2 (8%) | 1 (4.8%) | 4 (17.4%) | ||||||
| Liquid | Never | 1 (10.0%) | 6 (17.6%) | 0.368 | 7 (18.9%) | 0 | 0.372 | 1 (5.3%) | 6 (24.0%) | 0.051 | 1 (4.8%) | 6 (26.1%) | 0.06 | |
| Rarely | 0 | 4 (11.8%) | 4 (10.8%) | 0 | 0 | 4 (16.0%) | 4 (19.0%) | 0 | ||||||
| Sometimes | 1 (10.0%) | 9 (26.5%) | 9 (24.3%) | 1 (14.3%) | 4 (21.1%) | 6 (24.0%) | 6 (28.6%) | 4 (17.4%) | ||||||
| Usually | 7 (70.0%) | 13 (38.2%) | 15 (40.5%) | 5 (71.4%) | 13 (68.4%) | 7 (28.0%) | 8 (38.1%) | 12 (52.2%) | ||||||
| Always | 1 (10.0%) | 2 (5.9%) | 2 (5.4%) | 1 (14.3%) | 1 (5.3%) | 2 (8.0%) | 2 (9.5%) | 1 (4.3%) | ||||||
| Solid | Never | 1 (10.0%) | 6 (17.6%) | 0.851 | 7 (18.9%) | 0 | 0.752 | 2 (10.5%) | 5 (20.0%) | 0.542 | 3 (14.3%) | 4 (17.4%) | 0.276 | |
| Rarely | 1 (10.0%) | 6 (17.6%) | 6 (16.2%) | 1 (14.3%) | 2 (10.5%) | 5 (20.0%) | 6 (28.6%) | 1 (4.3%) | ||||||
| Sometimes | 4 (40.0%) | 8 (23.5%) | 10 (27.0%) | 2 (28.6%) | 6 (31.6%) | 6 (24.0%) | 5 (23.8%) | 7 (30.4%) | ||||||
| Usually | 3 (30.0%) | 11 (32.4%) | 11 (29.7%) | 3 (42.9%) | 8 (42.1%) | 6 (24.0%) | 5 (23.8%) | 9 (39.1%) | ||||||
| Always | 1 (10.0%) | 3 (8.8%) | 3 (8.1%) | 1 (14.3%) | 1 (5.3%) | 3 (12.0%) | 2 (9.5%) | 2 (8.7%) | ||||||
| Use of pad | Never | 4 (40.0%) | 19 (55.9%) | 0.321 | 20 (54.1%) | 3 (42.9%) | 0.588 | 10 (52.6%) | 13 (52.0%) | 0.553 | 10 (47.6%) | 13 (56.5%) | 0.790 | |
| Rarely | 0 | 1 (2.9%) | 1 (2.7%) | 0 | 0 | 1 (4.0%) | 0 | 1 (4.3%) | ||||||
| Sometimes | 0 | 5 (14.7%) | 5 (13.5%) | 0 | 1 (5.3%) | 4 (16.0%) | 3 (14.3%) | 2 (8.7%) | ||||||
| Usually | 2 (20.0%) | 3 (8.8%) | 4 (10.8%) | 1 (14.3%) | 2 (10.5%) | 3 (12.0%) | 3 (14.3%) | 2 (8.7%) | ||||||
| Always | 4 (40.0%) | 6 (17.6%) | 7 (18.9%) | 3 (42.9%) | 6 (31.6%) | 4 (16.0%) | 5 (23.8%) | 5 (21.7%) | ||||||
| Lifestyle alteration | Never | 0 | 7 (20.6%) | 0.011 | 7 (18.9%) | 0 | 0.426 | 2 (10.5%) | 5 (20.0%) | 0.195 | 2 (9.5%) | 5 (21.7%) | 0.096 | |
| Rarely | 0 | 5 (14.7%) | 4 (10.8%) | 1 (14.3%) | 2 (10.5%) | 3 (12.0%) | 5 (23.8%) | 0 | ||||||
| Sometimes | 0 | 10 (29.4%) | 9 (24.3%) | 1 (14.3%) | 2 (10.5%) | 8 (32.0%) | 5 (23.8%) | 5 (21.7%) | ||||||
| Usually | 8 (80.0%) | 9 (26.5%) | 14 (37.8%) | 3 (42.9%) | 11 (57.9%) | 6 (24.0%) | 6 (28.6%) | 11 (47.8%) | ||||||
| Always | 2 (20.0%) | 3 (8.8%) | 3 (8.1%) | 2 (28.6%) | 2 (10.5%) | 3 (12.0%) | 3 (14.3%) | 2 (8.7%) | ||||||
| Severity of incontinence | no | 0 | 5 (14.7%) | 5 (13.5%) | 0 | 0 | 5 (14.3%) | 1 (4.8%) | 4 (17.4%) | |||||
| urgency to evacuate | 7 (70.0%) | 23 (67.6%) | 25 (67.6%) | 5 (71.4%) | 8 (88.9%) | 22 (62.9%) | 16 (76.2%) | 14 (60.9%) | ||||||
| soling | 1 (10.0%) | 6 (17.6%) | 6 (16.2%) | 1 (14.3%) | 0 | 7 (20.0%) | 3 (14.3%) | 4 (17.4%) | ||||||
| accidents | 2 (20.0%) | 0 | 0.036 | 1 (2.7%) | 1 (14.3%) | 0.439 | 1 (11.1%) | 1 (2.9%) | 0.182 | 1 (4.8%) | 1 (4.3%) | 0.575 | ||
| Use of loperamide | no | 0 | 11 (32.4%) | 10 (27.0%) | 1 (14.3%) | 2 (22.2%) | 9 (25.7%) | 7 (33.3%) | 4 (17.4%) | |||||
| yes | 10 (100%) | 23 (67.6%) | 0.046 | 27 (73.0%) | 6 (85.7%) | 0.659 | 7 (77.8%) | 26 (74.3%) | 1.000 | 14 (66.7%) | 19 (82.6%) | 0.303 | ||
| No of daily defecation | 8.6 ± 4.4 | 6.1 ± 4.3 | 0.119 | 6.5 ± 4.6 | 7.1 ± 2.7 | 0.767 | 8.4 ± 5.1 | 6.2 ± 4.1 | 0.182 | 7.71 ± 4.9 | 5.74 ± 3.7 | 0.145 | ||
| Initial Tumor Location (from Anal Verge) | Anastomosis Method | Anastomosis Location (from Anal Verge) | Treatment | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ‘Degree of Change’ at Peirod 5 | ≤5cm | >5cm | p-Value | S-CR | H-CA | p-Value | <3cm | ≥3cm | p-Value | BFT Group | Control Group | p-Value |
| MRP | 0.54 ± 0.49 | 0.75 ± 0.34 | 0.137 | 0.71 ± 0.40 | 0.67 ± 0.30 | 0.806 | 0.76 ± 0.49 | 0.69 ± 0.36 | 0.606 | 0.69 ± 0.35 | 0.72 ± 0.42 | 0.793 |
| MSP | 0.48 ± 0.41 | 0.72 ± 0.34 | 0.073 | 0.68 ± 0.38 | 0.61 ± 0.32 | 0.662 | 0.63 ± 0.34 | 0.68 ± 0.38 | 0.715 | 0.65 ± 0.31 | 0.68 ± 0.43 | 0.797 |
| R asymmetry | 1.22 ± 1.60 | 1.02 ± 0.38 | 0.710 | 1.06 ± 0.86 | 1.10 ± 0.53 | 0.907 | 1.56 ± 1.59 | 0.94 ± 0.39 | 0.278 | 1.03 ± 0.46 | 1.10 ± 1.04 | 0.768 |
| S asymmetry | 0.91 ± 0.65 | 1.20 ± 0.46 | 0.125 | 1.11 ± 0.46 | 1.28 ± 0.81 | 0.443 | 1.38 ± 0.76 | 1.08 ± 0.43 | 0.122 | 1.07 ± 0.59 | 1.33 ± 1.07 | 0.343 |
| First RST | 0.75 ± 0.62 | 0.71 ± 0.36 | 0.856 | 0.69 ± 0.40 | 0.89 ± 0.53 | 0.271 | 0.93 ± 0.51 | 0.67 ± 0.39 | 0.095 | 0.72 ± 0.48 | 0.73 ± 0.37 | 0.943 |
| Max RST | 0.40 ± 0.35 | 0.64 ± 0.43 | 0.122 | 0.59 ± 0.34 | 0.57 ± 0.41 | 0.905 | 0.66 ± 0.39 | 0.57 ± 0.34 | 0.571 | 0.61 ± 0.51 | 0.57 ± 0.32 | 0.790 |
| Rectal Compliance | 1.60 ± 2.46 | 1.07 ± 0.78 | 0.524 | 1.13 ± 1.37 | 1.51 ± 1.18 | 0.498 | 2.16 ± 2.47 | 0.94 ± 0.72 | 0.179 | 1.06 ± 0.86 | 1.31 ± 1.67 | 0.547 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.-M.; Kim, H.; Yoo, R.; Kim, G.; Kye, B.-H. Effect of Biofeedback Therapy during Temporary Stoma Period in Rectal Cancer Patients: A Prospective Randomized Trial. J. Clin. Med. 2021, 10, 5172. https://doi.org/10.3390/jcm10215172
Cho H-M, Kim H, Yoo R, Kim G, Kye B-H. Effect of Biofeedback Therapy during Temporary Stoma Period in Rectal Cancer Patients: A Prospective Randomized Trial. Journal of Clinical Medicine. 2021; 10(21):5172. https://doi.org/10.3390/jcm10215172
Chicago/Turabian StyleCho, Hyeon-Min, Hyungjin Kim, RiNa Yoo, Gun Kim, and Bong-Hyeon Kye. 2021. "Effect of Biofeedback Therapy during Temporary Stoma Period in Rectal Cancer Patients: A Prospective Randomized Trial" Journal of Clinical Medicine 10, no. 21: 5172. https://doi.org/10.3390/jcm10215172
APA StyleCho, H.-M., Kim, H., Yoo, R., Kim, G., & Kye, B.-H. (2021). Effect of Biofeedback Therapy during Temporary Stoma Period in Rectal Cancer Patients: A Prospective Randomized Trial. Journal of Clinical Medicine, 10(21), 5172. https://doi.org/10.3390/jcm10215172