
Cardiac Arrest Survival Postresuscitation In-Hospital (CASPRI) Score Predicts Neurological Favorable Survival in Emergency Department Cardiac Arrest

 and
and
Abstract
:1. Introduction
2. Materials and Methods
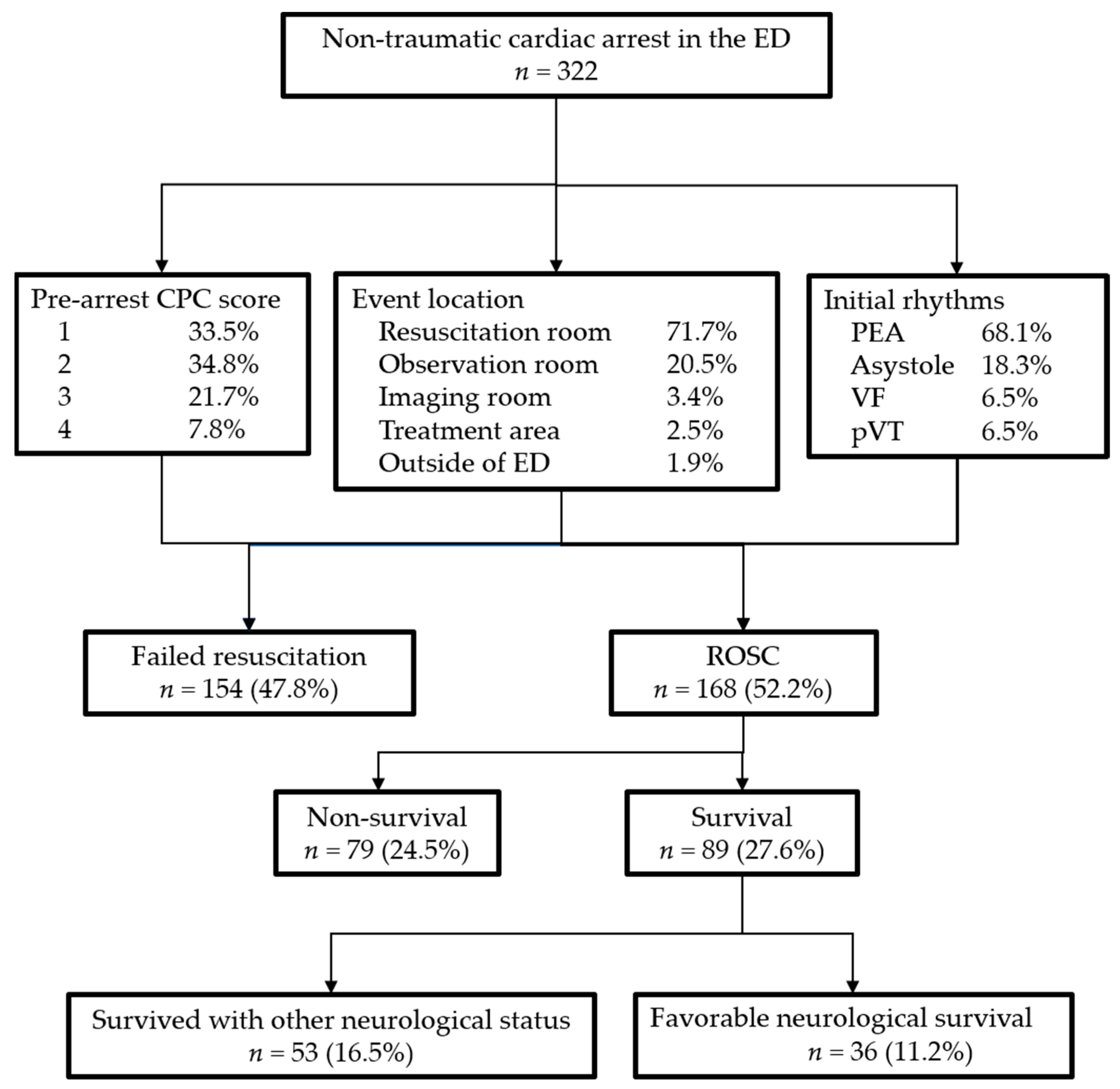
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Girotra, S.; Nallamothu, B.K.; Spertus, J.A.; Li, Y.; Krumholz, H.M.; Chan, P.S. Trends in survival after in-hospital cardiac arrest. N. Engl. J. Med 2012, 367, 1912–1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayser, R.G.; Ornato, J.P.; Peberdy, M.A. Cardiac arrest in the Emergency Department: A report from the National Registry of Cardiopulmonary Resuscitation. Resuscitation 2008, 78, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.W.; Holmberg, M.J.; Berg, K.M.; Donnino, M.W.; Granfeldt, A. In-Hospital Cardiac Arrest: A Review. JAMA 2019, 321, 1200–1210. [Google Scholar] [CrossRef]
- Donoghue, A.J.; Abella, B.S.; Merchant, R.; Praestgaard, A.; Topjian, A.; Berg, R.; Nadkarni, V.; American Heart Association’s Get with the Guidelines-Resuscitation Investigators. Cardiopulmonary resuscitation for in-hospital events in the emergency department: A comparison of adult and pediatric outcomes and care processes. Resuscitation 2015, 92, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.T.; Huang, W.C.; Yen, D.H.T.; Yeh, E.H.; Wu, S.Y.; Liao, H.H. The Potential Risk Factors for Mortality in Patients After In-Hospital Cardiac Arrest: A Multicenter Study. Front. Cardiovasc. Med. 2021. [Google Scholar] [CrossRef]
- Tan, S.C.; Leong, B.S. Cardiac arrests within the emergency department: An Utstein style report, causation and survival factors. Eur. J. Emerg. Med. 2018, 25, 12–17. [Google Scholar] [CrossRef]
- Chan, P.S.; Spertus, J.A.; Krumholz, H.M.; Berg, R.A.; Li, Y.; Sasson, C.; Nallamothu, B.K. A Validated Prediction Tool for Initial Survivors of In-Hospital Cardiac Arrest. Arch. Intern. Med. 2012, 172, 947–953. [Google Scholar] [CrossRef]
- Wang, C.H.; Chang, W.T.; Huang, C.H.; Tsai, M.S.; Yu, P.H.; Wu, Y.W.; Chen, W.J. Validation of the Cardiac Arrest Survival Postresuscitation In-hospital (CASPRI) score in an East Asian population. PLoS ONE 2018, 13, e0202938. [Google Scholar] [CrossRef]
- Nolan, J.P.; Berg, R.A.; Andersen, L.W.; Bhanji, F.; Chan, P.S.; Donnino, M.W.; Lim, S.H.; Ma, M.H.; Nadkarni, V.M.; Starks, M.A.; et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: Update of the Utstein Resuscitation Registry Template for In-Hospital Cardiac Arrest: A Consensus Report from a Task Force of the International Liaison Committee on Resuscitation. Circulation 2019, 140, e746–e757. [Google Scholar] [CrossRef] [Green Version]
- Larkin, G.L.; Copes, W.S.; Nathanson, B.H.; Kaye, W. Pre-resuscitation factors associated with mortality in 49,130 cases of in-hospital cardiac arrest: A report from the National Registry for Cardiopulmonary Resuscitation. Resuscitation 2010, 81, 302–311. [Google Scholar] [CrossRef]
- Ebell, M.H.; Afonso, A.M. Pre-arrest predictors of failure to survive after in-hospital cardiopulmonary resuscitation: A meta-analysis. Fam. Pract. 2011, 28, 505–515. [Google Scholar] [CrossRef] [Green Version]
- Piscator, E.; Hedberg, P.; Goransson, K.; Djarv, T. Survival after in-hospital cardiac arrest is highly associated with the Age-combined Charlson Co-morbidity Index in a cohort study from a two-site Swedish University hospital. Resuscitation 2016, 99, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.C.; Lugton, J.; Spiller, J.A.; Carduff, E. CPR decision-making conversations in the UK: An integrative review. BMJ Supportive Palliat. Care 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared Decision Making: A Model for Clinical Practice. J. Gen. Intern. Med. 2012, 27, 1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, J.J.; Jayaraman, D.; Swinton, M.; Jiang, X.; Heyland, D.K. Supporting shared decision-making about cardiopulmonary resuscitation using a video-based decision-support intervention in a hospital setting: A multisite before–after pilot study. CMAJ Open 2019, 7, E630. [Google Scholar] [CrossRef] [Green Version]
- Camuglia, A.C.; Randhawa, V.K.; Lavi, S.; Walters, D.L. Cardiac catheterization is associated with superior outcomes for survivors of out of hospital cardiac arrest: Review and meta-analysis. Resuscitation 2014, 85, 1533–1540. [Google Scholar] [CrossRef]
- Zanuttini, D.; Armellini, I.; Nucifora, G.; Carchietti, E.; Trillò, G.; Spedicato, L.; Bernardi, G.; Proclemer, A. Impact of emergency coronary angiography on in-hospital outcome of unconscious survivors after out-of-hospital cardiac arrest. Am. J. Cardiol. 2012, 110, 1723–1728. [Google Scholar] [CrossRef]
- Larsen, J.M.; Ravkilde, J. Acute coronary angiography in patients resuscitated from out-of-hospital cardiac arrest—A systematic review and meta-analysis. Resuscitation 2012, 83, 1427–1433. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef]
- Chan, P.S.; Berg, R.A.; Tang, Y.; Curtis, L.H.; Spertus, J.A. Association Between Therapeutic Hypothermia and Survival After In-Hospital Cardiac Arrest. JAMA 2016, 316, 1375–1382. [Google Scholar] [CrossRef]
- Chen, C.T.; Chen, C.H.; Chen, T.Y.; Yen, D.H.; How, C.K.; Hou, P.C. Comparison of in-hospital and out-of-hospital cardiac arrest patients receiving targeted temperature management: A matched case-control study. J. Chin. Med. Assoc. 2020, 83, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Engsig, M.; Søholm, H.; Folke, F.; Gadegaard, P.J.; Wiis, J.T.; Molin, R.; Mohr, T.; Engsig, F.N. Similar long-term survival of consecutive in-hospital and out-of-hospital cardiac arrest patients treated with targeted temperature management. Clin. Epidemiol. 2016, 8, 761–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, Y.S.; Tsai, M.S.; Huang, C.H.; Lai, C.H.; Huang, W.C.; Chan, L.; Kuo, L.K. Outcomes of Targeted Temperature Management for In-Hospital and Out-Of-Hospital Cardiac Arrest: A Matched Case-Control Study Using the National Database of Taiwan Network of Targeted Temperature Management for Cardiac Arrest (TIMECARD) Registry. Med. Sci. Monit. 2021, 27, e931203. [Google Scholar] [CrossRef]
- Roedl, K.; Jarczak, D.; Blohm, R.; Winterland, S.; Müller, J.; Fuhrmann, V.; Westermann, D.; Söffker, G.; Kluge, S. Epidemiology of intensive care unit cardiac arrest: Characteristics, comorbidities, and post-cardiac arrest organ failure—A prospective observational study. Resuscitation 2020, 156, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Leloup, M.; Briatte, I.; Langlois, A.; Cariou, A.; Lesieur, O.; ACIR Study Group. Unexpected cardiac arrests occurring inside the ICU: Outcomes of a French prospective multicenter study. Intensive Care Med. 2020, 46, 1005–1015. [Google Scholar] [CrossRef]

{kind=link}
| Patient Data | All (n = 321) | Survival (n = 89) | Non-Survival (n = 232) | p Value |
|---|---|---|---|---|
| Age, mean (S.D.) | 67.2 (15.5) | 64.9 (15.6) | 68.1 (15.8) | N.S. |
| Sex | N.S. | |||
| Male (n, %) | 221 (68.8%) | 57 (64.0%) | 164 (70.7%) | |
| Female | 100 (31.2%) | 32 (36.0%) | 68 (29.3%) | |
| OHCA | 0.155 * | |||
| Yes | 16 (5.0%) | 7 (8.0%) | 9 (3.9%) | |
| No | 303 (95.0%) | 81 (92.0%) | 222 (96.1%) | |
| CPC before cardiac arrest | N.S. | |||
| 1 | 107 (34.1%) | 34 (38.6%) | 73 (32.3%) | |
| 2 | 112 (35.7%) | 30 (34.1%) | 82 (36.3%) | |
| 3 | 70 (22.3%) | 20 (22.7%) | 50 (22.1%) | |
| 4 | 25 (8.0%) | 4 (4.5%) | 21 (9.3%) | |
| Preexisting conditions | ||||
| Heart failure | 0.005 | |||
| Yes | 37 (11.6%) | 18 (20.2%) | 19 (8.2%) | |
| No | 283 (88.4%) | 71 (79.8%) | 212 (91.8%) | |
| Myocardial infarct | <0.001 | |||
| Yes | 37 (11.6%) | 21 (23.6%) | 16 (6.9%) | |
| No | 283 (88.4%) | 68 (76.4%) | 215 (93.1%) | |
| Respiratory failure | 0.155 * | |||
| Yes | 46 (14.4%) | 17 (19.1%) | 29 (12.6%) | |
| No | 274 (85.6%) | 72 (80.9%) | 202 (87.4%) | |
| Hepatic failure | 0.042 | |||
| Yes | 12 (3.8%) | 7 (7.9%) | 5 (2.2%) | |
| No | 308 (96.3%) | 82 (92.1%) | 226 (97.8%) | |
| Hypotension/shock | <0.001 | |||
| Yes | 64 (20.0%) | 31 (34.8%) | 33 (14.3%) | |
| No | 256 (80.0%) | 58 (65.2%) | 198 (85.7%) | |
| Metabolic illness | 0.006 | |||
| Yes | 32 (10.0%) | 16 (18.0%) | 16 (6.9%) | |
| No | 288 (90.0%) | 73 (82.0%) | 215 (93.1%) | |
| Diabetes mellitus | < 0.001 | |||
| Yes | 49 (15.3%) | 27 (30.3%) | 22 (9.5%) | |
| No | 271 (84.7%) | 62 (69.7%) | 209 (90.5%) | |
| Pneumonia | 0.185 * | |||
| Yes | 40 (12.5%) | 15 (16.9%) | 25 (10.8%) | |
| No | 280 (87.5%) | 74 (83.1%) | 206 (89.2%) | |
| Sepsis | 0.009 | |||
| Yes | 25 97.8%) | 13 (14.6%) | 12 (5.2%) | |
| No | 295 (92.2%) | 76 (85.4%) | 219 (94.8%) | |
| Malignancy | 0.131 * | |||
| Yes | 21 (6.6%) | 9 (10.1%) | 12 (5.2%) | |
| No | 299 (93.4%) | 80 (89.9%) | 219 (94.8%) | |
| Renal failure | 0.007 | |||
| Yes | 73 (22.8%) | 30 (33.7%) | 43 (18.6%) | |
| No | 247 (77.2%) | 59 (66.3%) | 188 (81.4%) | |
| Pre-event data | ||||
| Cause of cardiac arrest | <0.001 | |||
| Cardiac | 166 (51.7%) | 53 (59.6%) | 113 (48.7%) | |
| Respiratory | 57 (17.8%) | 2 (2.2%) | 55 (23.7%) | |
| Others | 98 (30.5%) | 34 (38.2%) | 64 (27.6%) | |
| Cardiac arrest process | ||||
| Initial rhythm | <0.001 | |||
| Asystole | 59 (18.6%) | 13 (14.9%) | 46 (20.0%) | |
| PEA | 216 (68.1%) | 50 (57.5%) | 166 (72.2%) | |
| VF | 21 (6.6%) | 13 (14.9%) | 8 (3.5%) | |
| pVT | 21 (6.6%) | 11 (12.6%) | 10 (4.3%) | |
| Resuscitation time of ROSC | <0.001 | |||
| 0–4 min | 56 (17.4%) | 32 (36.0%) | 24 (10.3%) | |
| 5–9 min | 52 (16.2%) | 20 (22.5%) | 32 (13.8%) | |
| 10–14 min | 21 (6.5%) | 9 (10.1%) | 12 (5.2%) | |
| 15–29 min | 50 (15.6%) | 18 (20.2%) | 32 (13.8%) | |
| ≥30 min | 142 (44.2%) | 10 (11.2%) | 132 (56.9%) | |
| Postresuscitation process | ||||
| Coronary angiography | <0.001 | |||
| Urgent | 22 (8.2%) | 15 (16.9%) | 7 (3.9%) | |
| Delayed | 15 (5.6%) | 12 (13.5%) | 3 (1.7%) | |
| None | 231 (86.2%) | 62 (69.7%) | 169 (94.4%) | |
| Coronary reperfusion attempted | <0.001 | |||
| Yes | 33 (12.4%) | 23 (25.8%) | 10 (5.6%) | |
| No | 233 (87.6%) | 66 (74.2%) | 167 (94.4%) | |
| Targeted temperature management | 0.007 | |||
| Yes | 11 (4.1%) | 8 (9.0%) | 3 (1.7%) | |
| No | 257 (95.9%) | 81 (91.0%) | 176 (98.3%) | |
| CASPRI score | <0.001 | |||
| 0–9 | 22 (6.9%) | 15 (16.9%) | 7 (3.0%) | |
| 10–14 | 55 (17.1%) | 26 (29.2%) | 29 (12.5%) | |
| 15–19 | 112 (34.9%) | 23 (25.8%) | 89 (38.4%) | |
| ≥20 | 132 (41.1%) | 25 (28.1%) | 107 (46.1%) | |
| mean ± SD | 18.2 ± 6.0 | 15.3 ± 6.4 | 19.4 ± 5.4 | <0.001 |
| Patient Data | All (n = 168) | Favorable Neurological Survival (n = 36) | Others (n = 132) | p Value |
|---|---|---|---|---|
| Preexisting conditions | ||||
| Myocardial infarct | 0.178 | |||
| Yes | 37 (22.0%) | 11 (30.6%) | 26 (19.7%) | |
| No | 131 (78.0) | 25 (69.4%) | 106 (80.3%) | |
| Hypotension/shock | 0.033 | |||
| Yes | 65 (38.7%) | 8 (22.2%) | 57 (43.2%) | |
| No | 103 (61.3%) | 28 (77.8%) | 75 (56.8%) | |
| Pre-event data | ||||
| Cause of cardiac arrest | 0.025 | |||
| Cardiac | 87 (51.8%) | 17 (47.2%) | 70 (53.2%) | |
| Respiratory | 17 (10.1%) | 0 (0.0%) | 17 (12.9%) | |
| Others | 64 (38.1%) | 19 (52.8%) | 45 (34.1%) | |
| Postresuscitation process | ||||
| Coronary angiography | 0.004 | |||
| Urgent | 22 (13.1%) | 10 (27.8%) | 12 (9.1%) | |
| Delayed | 15 (8.9%) | 5 (13.9%) | 10 (7.6%) | |
| None | 131 (78.0%) | 21 (58.3%) | 110 (83.3%) | |
| Coronary reperfusion attempted | 0.009 | |||
| Yes | 33 (19.9%) | 13 (36.1%) | 20 (15.4%) | |
| No | 133 (80.1%) | 23 (63.9%) | 110 (84.6%) |
| Patient Data | CASPRI Points | All (n = 168) | Favorable Neurological Survival (n = 36) | Others (n = 132) | p Value |
|---|---|---|---|---|---|
| Age group (years) | N.S. | ||||
| <60 | 0 | 63 (37.5%) | 13 (36.1%) | 50 (37.9%) | |
| 60–69 | 1 | 43 (25.6%) | 13 (36.1%) | 30 (22.7%) | |
| 70–79 | 2 | 26 (15.5%) | 6 (16.7%) | 20 (15.2%) | |
| ≥80 | 4 | 36 (21.4%) | 4 (11.1%) | 32 (24.2%) | |
| Initial rhythm | <0.001 | ||||
| Witnessed VF/pVT | 0 | 28 (16.7%) | 11 (30.6%) | 17 (12.9%) | |
| Non-witnessed VF/pVT | 3 | 8 (4.8%) | 5 (13.9%) | 3 (2.3%) | |
| PEA | 6 | 103 (61.3%) | 18 (50.0%) | 85 (64.4%) | |
| Asystole | 7 | 29 (17.3%) | 2 (5.6%) | 27 (20.5%) | |
| Pre-arrest CPC score | 0.039 | ||||
| 1 | 0 | 64 (38.1%) | 19 (52.8%) | 45 (34.1%) | |
| 2 | 2 | 54 (32.1%) | 12 (33.3%) | 42 (31.58%) | |
| 3 or 4 | 9 | 50 (29.8) | 5 (13.9%) | 45 (34.1%) | |
| Resuscitation time of ROSC | N.S. | ||||
| 0–4 min | 0 | 50 (29.8%) | 17 (47.2%) | 33 (25.0%) | |
| 5–9 min | 3 | 38 (22.6%) | 9 (25.0%) | 29 (22.0%) | |
| 10–14 min | 5 | 16 (9.5%) | 3 (8.3%) | 13 (9.8%) | |
| 15–29 min | 6 | 33 (19.6%) | 4 (11.1%) | 29 (22.0%) | |
| ≥30 min | 8 | 31 (18.5) | 3 (8.3%) | 28 (21.2%) | |
| Monitored | N.S. | ||||
| Yes | 0 | 136 (81.0%) | 30 (83.3%) | 106 (80.3%) | |
| No | 3 | 32 (19.0%) | 6 (16.7%) | 26 (19.7%) | |
| Factors present prior to arrest | 0.004. | ||||
| None | 0 | 25 (14.9%) | 12 (33.3%) | 13 (9.8%) | |
| Renal failure | 2 | 19 (11.3%) | 5 (13.9%) | 14 (10.6%) | |
| Mechanical ventilation /Sepsis/Hypotension | 3 | 108 (64.3%) | 17 (47.2%) | 91 (68.9%) | |
| Hepatic failure/Malignancy | 4 | 16 (9.5%) | 2 (5.6%) | 14 (10.6%) | |
| CAPRI score | <0.001 | ||||
| 0–9 | 21 (12.5%) | 11 (30.6) | 10 (7.6%) | ||
| 10–14 | 44 (26.2%) | 13 (36.1%) | 31 (23.5%) | ||
| 15–19 | 51 (30.4%) | 8 (22.2%) | 43 (32.6%) | ||
| ≥20 | 52 (31.0%) | 4 (11.1%) | 48 (36.4%) | ||
| mean ± SD | 16.5 ± 6.5 | 11.1 ± 5.6 | 17.8 ± 6.1 | <0.001 |
| Independent Variable | Odd Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Survival | |||
| Hypotension/shock | 2.3 | 1.2–4.6 | 0.014 |
| Metabolic illness | 3.4 | 1.4–7.9 | 0.005 |
| Resuscitation time of ROSC | 0.7 | 0.6–0.8 | <0.001 |
| Coronary angiography | 3.6 | 1.9–6.9 | <0.001 |
| Targeted temperature management | 8.0 | 1.8–35.4 | 0.006 |
| Favorable neurological survival | |||
| Coronary angiography(urgent vs. other groups) | 5.5 | 1.8–16.7 | 0.003 |
| CASPRI score(0–9 vs. other groups) | 9.2 | 2.2–37.4 | 0.002 |
| CASPRI score(10–14 vs. other groups) | 7.7 | 2.1–28.2 | 0.002 |
| AUROCC of CASPRI score | 0.77 | 0.68–0.85 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, J.C.-H.; Ma, J.-W.; Liu, S.-C.; Lin, T.-C.; Hu, S.-Y. Cardiac Arrest Survival Postresuscitation In-Hospital (CASPRI) Score Predicts Neurological Favorable Survival in Emergency Department Cardiac Arrest. J. Clin. Med. 2021, 10, 5131. https://doi.org/10.3390/jcm10215131
Tsai JC-H, Ma J-W, Liu S-C, Lin T-C, Hu S-Y. Cardiac Arrest Survival Postresuscitation In-Hospital (CASPRI) Score Predicts Neurological Favorable Survival in Emergency Department Cardiac Arrest. Journal of Clinical Medicine. 2021; 10(21):5131. https://doi.org/10.3390/jcm10215131
Chicago/Turabian StyleTsai, Jeffrey Che-Hung, Jen-Wen Ma, Shih-Chia Liu, Tzu-Chieh Lin, and Sung-Yuan Hu. 2021. "Cardiac Arrest Survival Postresuscitation In-Hospital (CASPRI) Score Predicts Neurological Favorable Survival in Emergency Department Cardiac Arrest" Journal of Clinical Medicine 10, no. 21: 5131. https://doi.org/10.3390/jcm10215131
APA StyleTsai, J. C.-H., Ma, J.-W., Liu, S.-C., Lin, T.-C., & Hu, S.-Y. (2021). Cardiac Arrest Survival Postresuscitation In-Hospital (CASPRI) Score Predicts Neurological Favorable Survival in Emergency Department Cardiac Arrest. Journal of Clinical Medicine, 10(21), 5131. https://doi.org/10.3390/jcm10215131