
Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria)
.png)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection and Data Collection Process
2.5. Data Items
2.6. Effect Measures
2.7. Synthesis Methods
2.8. Risk and Reporting of Bias Assessment
2.9. Certainty Assessment
3. Results
3.1. Study Selection
3.2. Results of Individual Studies
3.3. Results of Synthesis
3.3.1. Prevalence of Overall FGID
3.3.2. Prevalence of Sub-Category FGID
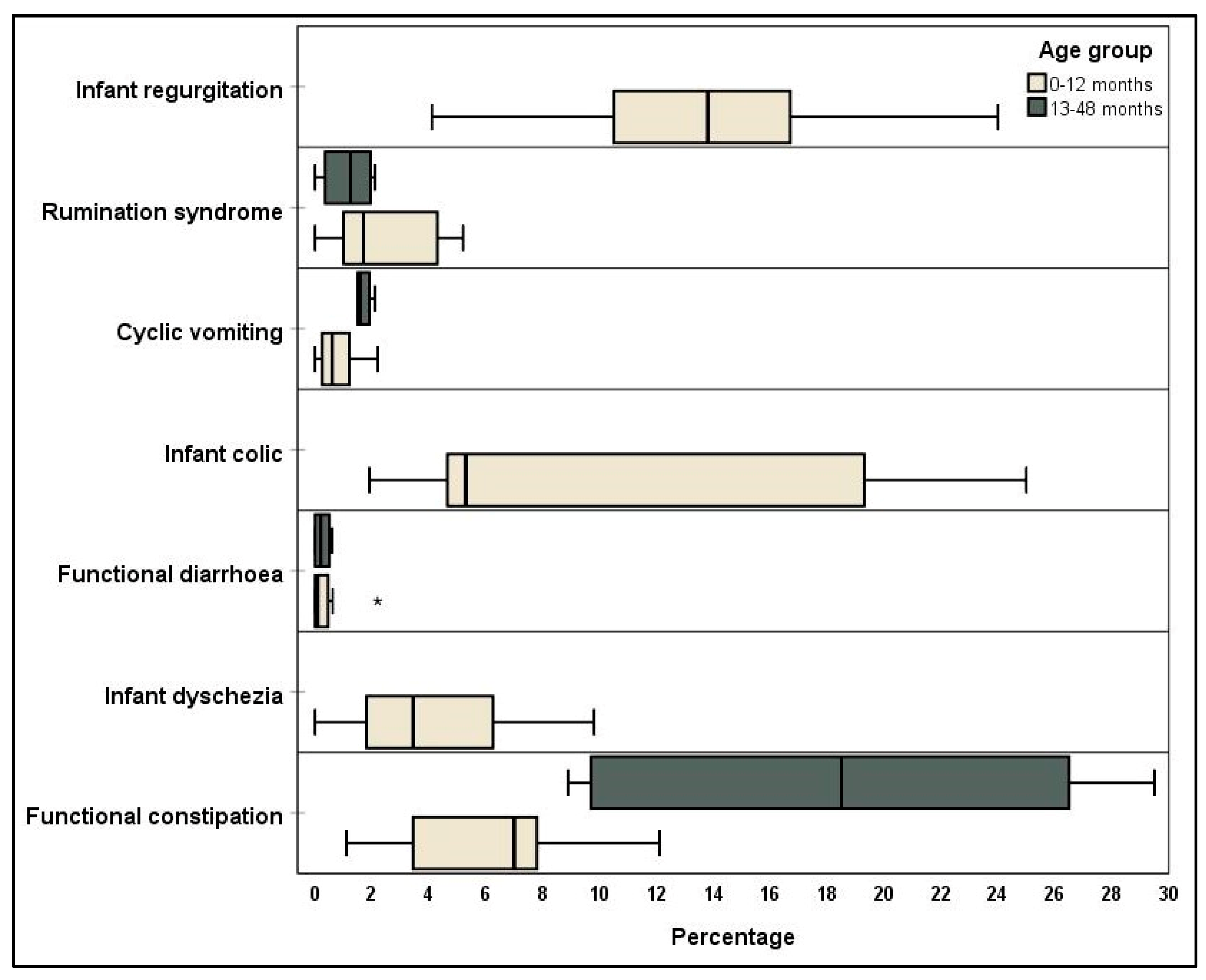
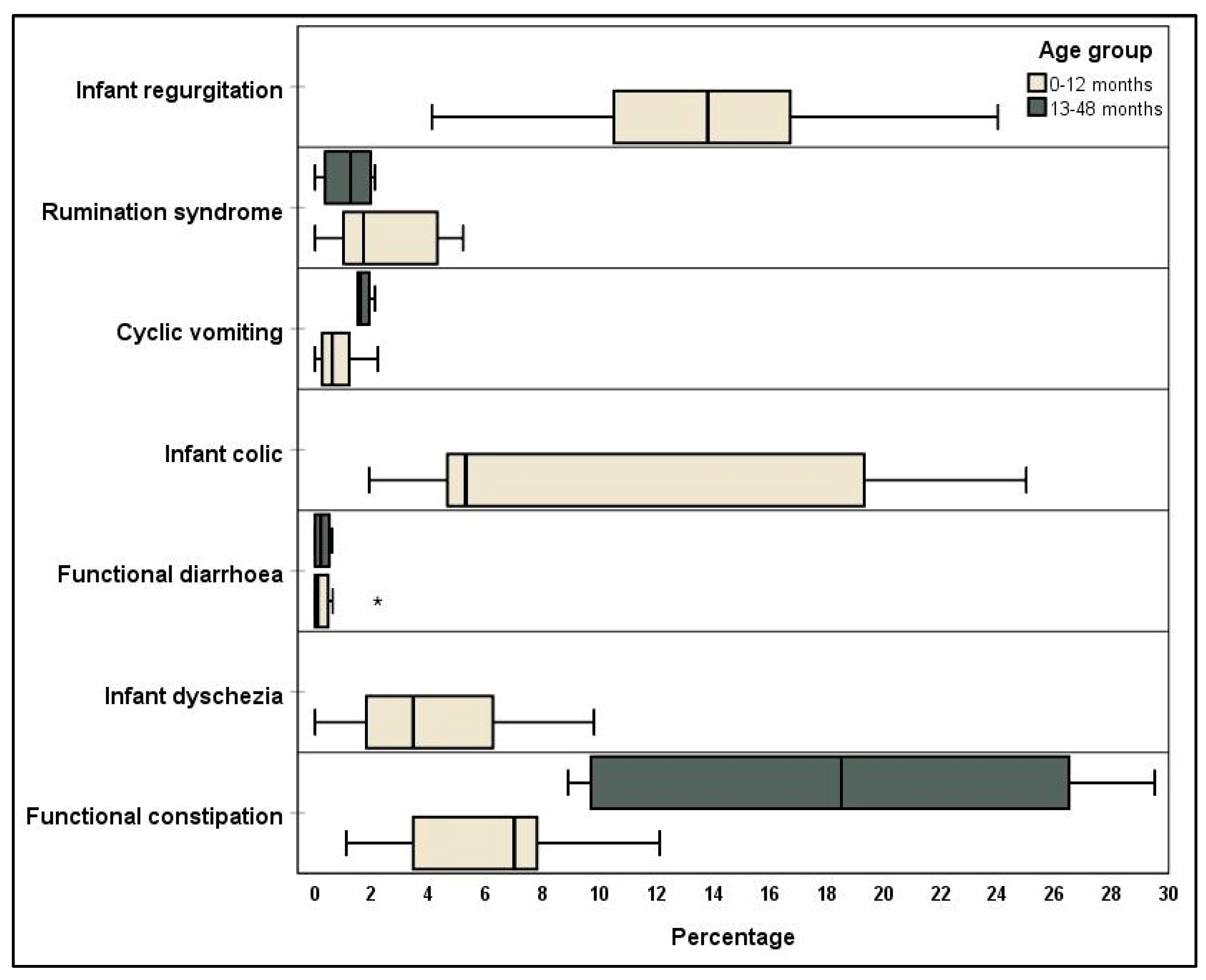
Infant/Toddler Categories
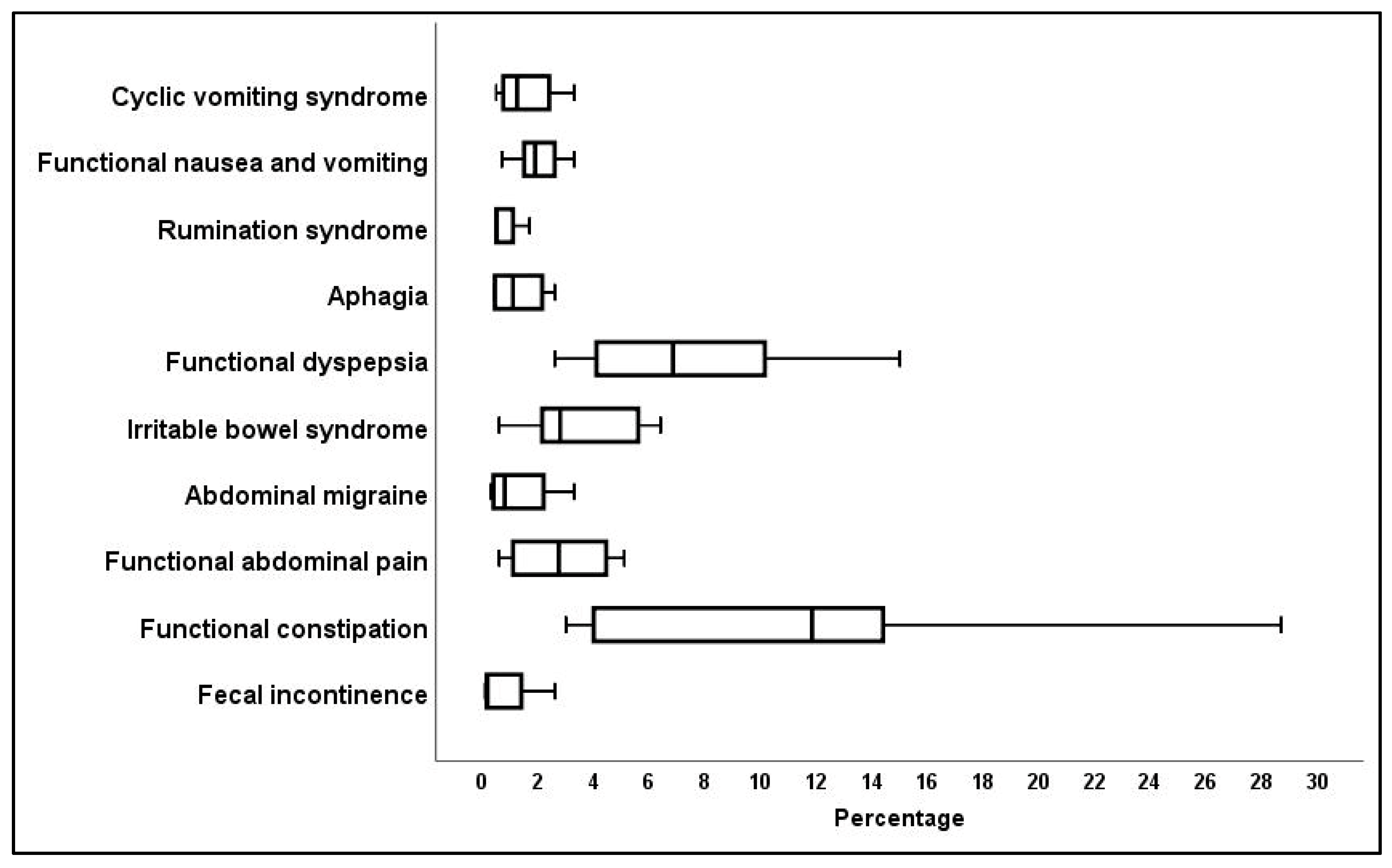
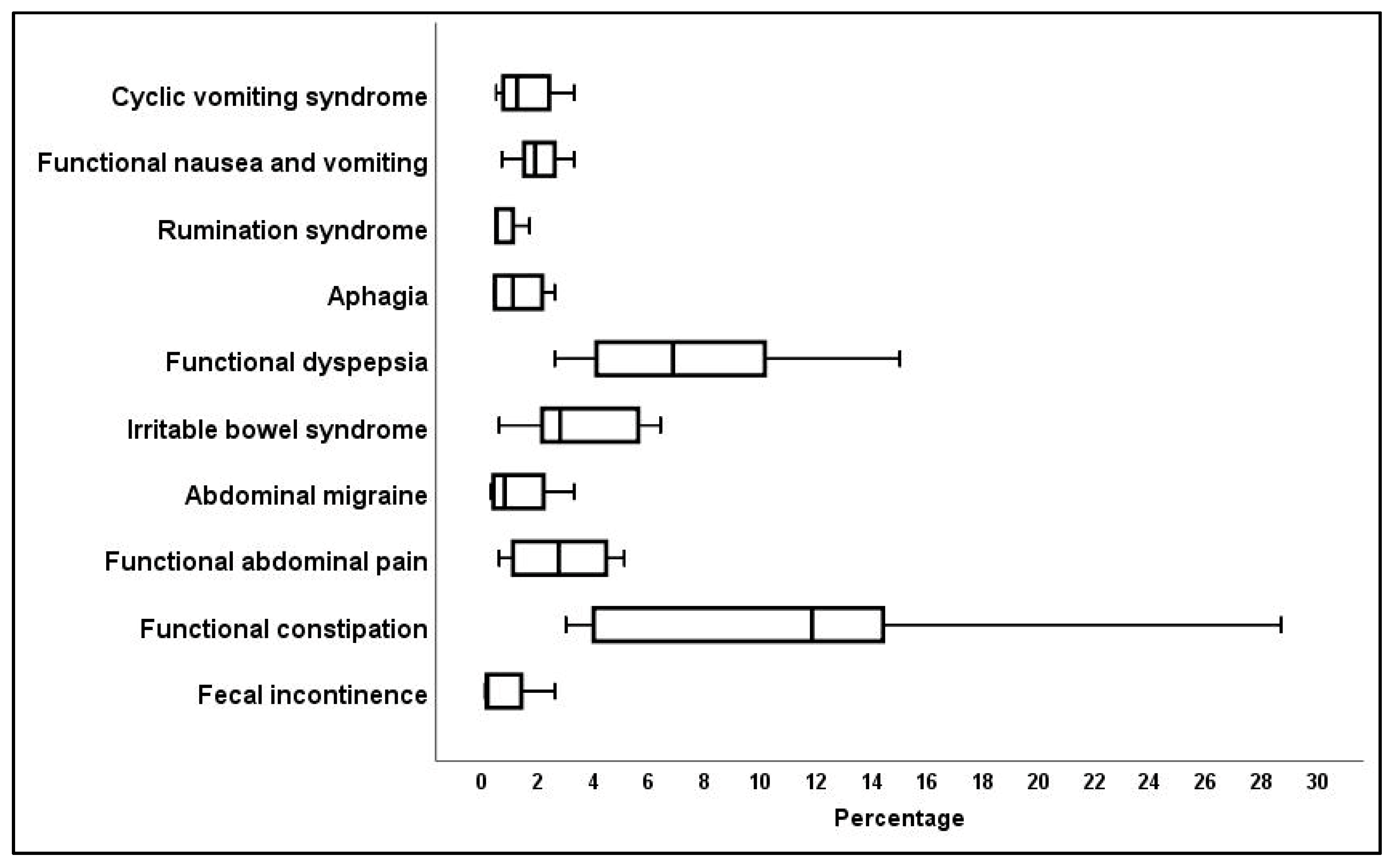
Children/Adolescent Categories
3.3.3. FGID Sub-Types
3.4. Risk of Bias of Studies
3.5. Certainty of Data
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Results for Health Literature Databases

{kind=link}
{kind=link}
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | Rome IV.mp. | 431 |
| 2 | limit 1 to yr = “2016 -Current” | 427 |
| 3 | functional gastro *.mp. | 3197 |
| 4 | GI disorder.mp. | 160 |
| 5 | FGID.mp. | 466 |
| 6 | gastro * disorder.mp. | 1475 |
| 7 | functional gut.mp. | 166 |
| 8 | 3 or 4 or 5 or 6 or 7 | 4316 |
| 9 | 2 and 8 | 160 |
| 10 | child *.mp. or Child/ | 2,503,644 |
| 11 | 9 and 10 | 55 |
| 12 | p *ediatric.mp. | 371,166 |
| 13 | 10 or 12 | 2,579,625 |
| 14 | 9 and 13 | 57 |
| 15 | Adolescent/ or adolescen *.mp. | 2,153,986 |
| 16 | 10 or 12 or 15 | 3,677,129 |
| 17 | 9 and 16 | 62 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | Rome IV.mp. | 1062 |
| 2 | limit 1 to yr = “2016 -Current” | 1042 |
| 3 | functional gastro *.mp. | 5412 |
| 4 | GI disorder.mp. | 397 |
| 5 | FGID.mp. | 1031 |
| 6 | gastro * disorder.mp. | 2902 |
| 7 | functional gut.mp. | 270 |
| 8 | 3 or 4 or 5 or 6 or 7 | 7847 |
| 9 | child *.mp. or child/ | 2,774,584 |
| 10 | p *ediatric.mp. | 573,340 |
| 11 | adolescent/ or adolescence/ or adolescen *.mp. | 1,636,092 |
| 12 | 9 or 10 or 11 | 3,615,317 |
| 13 | 2 and 8 and 12 | 130 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | Rome IV | |
| 2 | Child * OR p *ediatric OR adolescen * | |
| 3 | FGID OR functional gastro * OR gastro * disorder OR functional gut | |
| 4 | 1 and 2 and 3 | 37 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | Rome IV.mp. | 11 |
| 2 | limit 1 to yr = “2016 -Current” | 11 |
| 3 | functional gastro *.mp. | 376 |
| 4 | GI disorder.mp. | 31 |
| 5 | FGID.mp. | 58 |
| 6 | gastro * disorder.mp. | 164 |
| 7 | functional gut.mp. | 6 |
| 8 | 3 or 4 or 5 or 6 or 7 | 471 |
| 9 | child *.mp. | 821,999 |
| 10 | exp Pediatrics/ or p *ediatric.mp. | 49,253 |
| 11 | Adolescen *.mp. | 478,850 |
| 12 | 9 or 10 or 11 | 1,094,309 |
| 13 | 2 and 8 and 12 | 2 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | Rome IV AND (child * OR adolescen * OR p *ediatric) | 601 |
| 2 | limit 1 to yr = “2016 -Current” | 289 |
| 3 | Rome IV.mp. | 4 |
| 4 | limit 3 to yr = “2016 -Current” | 4 |
| 5 | functional gastro *.mp. | 10 |
| 6 | GI disorder.mp. | 0 |
| 7 | FGID.mp. | 0 |
| 8 | gastro * disorder.mp. | 3 |
| 9 | functional gut.mp. | 0 |
| 10 | 5 or 6 or 7 or 8 or 9 | 13 |
| 11 | 4 and 10 | 1 |
| 12 | child *.mp. or Child/ | 2024 |
| 13 | 11 and 12 | 1 |
| 14 | p *ediatric.mp. | 874 |
| 15 | 12 or 14 | 2210 |
| 16 | 11 and 15 | 1 |
| 17 | Adolescent/ or adolescen *.mp. | 683 |
| 18 | 12 or 14 or 17 | 2281 |
| 19 | 11 and 18 | 1 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | (child * OR p *ediatric OR adolescent *) | |
| 2 | (Rome NEAR/1 IV) | |
| 3 | (FGID OR functional NEAR/1 gastro * OR functional NEAR/1 gut OR gastro * NEAR/1 disorder OR GI NEAR/1 disorder) | |
| 4 | 1 and 2 and 3 | 100 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | (TITLE-ABS-KEY ( rome w/1 iv ) ) | |
| 2 | (child * OR adolescen * or p *ediatric) | |
| 3 | (fgid OR gi w/1 disorder OR gastro * w/1 disorder OR functional w/1 gut OR functional w/1 gastro *) | |
| 4 | 1 and 2 and 3 | 31 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | child * | 182,167 |
| 2 | p *ediatric | 53,365 |
| 3 | Adolescen * | 142,978 |
| 4 | MeSH descriptor (child) explode all trees | 56,688 |
| 5 | MeSH descriptor (adolescent) explode all trees | 104,818 |
| 6 | Rome IV | 494 |
| 7 | FGID | 61 |
| 8 | “Functional gastro *” | 11 |
| 9 | “Gastro * disorder” | 0 |
| 10 | GI disorder | 55 |
| 11 | “Functional gut” | 36 |
| 12 | (#1 OR #2 OR #3 OR #4 OR #5) | 281,555 |
| 13 | (#7 OR #8 OR #9 OR #10 OR #11) | 160 |
| 14 | #12 AND #6 AND #13 | 3 |
| Search Line | Search Statement | Results |
|---|---|---|
| 1 | Functional + gastrointestinal + disorders | 10 |
| 2 | FGID | 0 |
| 3 | Rome + IV + gastrointestinal | 0 |
References
- Lewis, M.L.; Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A. Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents. J. Pediatr. 2016, 177, 39–43.e3. [Google Scholar] [CrossRef]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef]
- Caplan, A.; Walker, L.; Rasquin, A. Development and Preliminary Validation of the Questionnaire on Pediatric Gastrointestinal Symptoms to Assess Functional Gastrointestinal Disorders in Children and Adolescents. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 296–304. [Google Scholar] [CrossRef]
- Jarrett, M.; Heitkemper, M.; Czyzewski, D.I.; Shulman, R. Recurrent Abdominal Pain in Children: Forerunner to Adult Irritable Bowel Syndrome? J. Spec. Pediatr. Nurs. 2003, 8, 81–89. [Google Scholar] [CrossRef]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2016, 150, 1456–1468.e2. [Google Scholar] [CrossRef] [PubMed]
- Benninga, M.A.; Nurko, S.; Faure, C.; Hyman, P.E.; Roberts, I.S.J.; Schechter, N.L. Childhood Functional Gastrointestinal Disorders: Neonate/Toddler. Gastroenterology 2016, 150, 1443–1455.e2. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Loney, P.L.; Chambers, L.W.; Bennett, K.J.; Roberts, J.G.; Stratford, P. Critical appraisal of the health research literature: Prevalence or incidence of a health problem. Chronic Dis. Can. 1998, 19, 170–176. [Google Scholar] [PubMed]
- Aydemir, Y.; Carman, K.B.; Yarar, C. Screening for functional gastrointestinal disorders in children with epilepsy. Epilepsy Behav. 2020, 111, 107267. [Google Scholar] [CrossRef]
- Beser, O.; Cokugras, F.; Vandenplas, Y. Prevalence and clinical characteristics of functional gastrointestinal disorders in infants [abstract]. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 391. [Google Scholar]
- Chanis, R.; Velasco-Benitez, C. Prevalence of functional gastrointestinal disorders in panamanian infants under 12 months: Comparison between the Rome III and Rome IV Criteria [abstract]. J. Pediatr. Gastroenterol. Nutr. 2019, 69. [Google Scholar]
- Chew, K.S.; Em, J.M.; Koay, Z.L.; Jalaludin, M.Y.; Ng, R.T.; Lum, L.C.S.; Lee, W.S. Low prevalence of infantile functional gastrointestinal disorders (FGIDs) in a multi-ethnic Asian population. Pediatr. Neonatol. 2020, 62, 49–54. [Google Scholar] [CrossRef]
- Chikunov, V.; Ilenkova, N. Prevalence of functional gastrointestinal disorders in Russian children [abstract]. Turk. J. Gastroenterol. 2019, 30, 279. [Google Scholar]
- Ekinci, R.M.K.; Balcı, S.; Akay, E.; Tumgor, G.; Dogruel, D.; Altintas, D.U.; Yilmaz, M. Frequency of functional gastrointestinal disorders in children with familial Mediterranean fever. Clin. Rheumatol. 2019, 38, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, R.M.K.; Balcı, S.; Mart, O.O.; Tumgor, G.; Yavuz, S.; Celik, H.; Dogruel, D.; Altintas, D.U.; Yilmaz, M. Is Henoch–Schönlein purpura a susceptibility factor for functional gastrointestinal disorders in children? Rheumatol. Int. 2018, 39, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Játiva-Mariño, E.; Rivera-Valenzuela, M.G.; Velasco-Benitez, C.A.; Saps, M. The prevalence of functional constipation in children was unchanged after the Rome IV criteria halved the diagnosis period in Rome III. Acta Paediatr. 2019, 108, 2274–2277. [Google Scholar] [CrossRef]
- Llanos-Chea, A.; Velasco-Benitez, C.; Saps, M. Inter-observer reliability for stool consistency between the bristol stool scale and the Brussels Infant and Toddler Stool Scale (BITSS) when using Rome IV criteria in younger children [abstract]. J. Pediatr. Gastroenterol. Nutr. 2019, 69. [Google Scholar]
- Ozdemir, M.; Beser, O. Study on determination of functional gastrointestinal diseases in infants who were received the general pediatric outpatient clinic by using Rome Iv diagnostic criteria [abstract]. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 176. [Google Scholar]
- Robin, S.G.; Keller, C.; Zwiener, R.; Hyman, P.E.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Shulman, R.J.; Hyams, J.S.; Palsson, O.; et al. Prevalence of Pediatric Functional Gastrointestinal Disorders Utilizing the Rome IV Criteria. J. Pediatr. 2018, 195, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Saps, M.; Velasco-Benitez, C.A.; Langshaw, A.H.; Ramírez-Hernández, C.R. Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents: Comparison between Rome III and Rome IV Criteria. J. Pediatr. 2018, 199, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Saps, M.; Velasco-Benitez, C.A.; Valdes, L.F.; Mejia, J.; Villamarin, E.; Moreno, J.; Ramirez, C.; González, M.J.; Vallenilla, I.; Falcon, A.C.; et al. The impact of incorporating toilet-training status in the pediatric Rome IV criteria for functional constipation in infant and toddlers. Neurogastroenterol. Motil. 2020, 32, e13912. [Google Scholar] [CrossRef] [PubMed]
- Steutel, N.F.; Zeevenhooven, J.; Scarpato, E.; Vandenplas, Y.; Tabbers, M.M.; Staiano, A.; Benninga, M.A. Prevalence of Functional Gastrointestinal Disorders in European Infants and Toddlers. J. Pediatr. 2020, 221, 107–114. [Google Scholar] [CrossRef]
- Velasco-Benitez, C.; Campeon-Cruz, V.; Duenas-Armendariz, A. Reproducibility of the Rome IV questionnaire for pediatric digestive symptoms in Spanish for functional gastrointestinal disorders in schoolchildren and adolescents from Colombia, South America [abstract]. J. Pediatr. Gastroenterol. Nutr. 2018, 67, S41. [Google Scholar]
- Velasco-Benitez, C.; Villamarin-Betancourt, E.; Mejia-Lopez, J. Risk factors in children under 4 years of age with functional gas-trointestinal disorders according to the Rome IV criteria [abstract]. J. Pediatr. Gastroenterol. Nutr. 2019, 69. [Google Scholar]
- Velasco-Benitez, C.A.; Axelrod, C.; Gutierrez, S.; Saps, M. The Relationship Between Prematurity, Method of Delivery, and Functional Gastrointestinal Disorders in Children. J. Pediatr. Gastroenterol. Nutr. 2020, 70, e37–e40. [Google Scholar] [CrossRef]
- Velasco-Benítez, C.A.; Gómez-Oliveros, L.F.; Rubio-Molina, L.M.; Tovar-Cuevas, J.R.; Saps, M. Diagnostic Accuracy of the Rome IV Criteria for the Diagnosis of Functional Gastrointestinal Disorders in Children. J. Pediatr. Gastroenterol. Nutr. 2020, 72, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Vlad, R.; Dijmarescu, I.; Smadeanu, R. Functional gastrointestinal disorders, up to date topic. Applying Rome iv criteria to a Romanian cohort of young children [abstract]. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 456. [Google Scholar]
- Zeevenhooven, J.; Biesbroek, A.; Schappin, R. Functional gastrointestinal disorders and behavioral problems in adolescents with a history of infant colic [abstract]. Gastroenterology 2019, 156, S157. [Google Scholar] [CrossRef]
- Koppen, I.J.N.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Benninga, M.A. The pediatric Rome IV criteria: What’s new? Expert Rev. Gastroenterol. Hepatol. 2017, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.-P. Epidemiology of functional gastrointestinal disorders in infants and toddlers: A systematic review. World J. Gastroenterol. 2016, 22, 6547–6558. [Google Scholar] [CrossRef]
- Boronat, A.; Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.-P. Epidemiology of functional gastrointestinal disorders in children and adolescents: A systematic review. World J. Gastroenterol. 2017, 23, 3915–3927. [Google Scholar] [CrossRef]
- Diederen, K.; Hoekman, D.R.; Hummel, T.Z.; De Meij, T.G.; Koot, B.G.P.; Tabbers, M.M.; Vlieger, A.M.; Kindermann, A.; Benninga, M.A. The prevalence of irritable bowel syndrome-type symptoms in paediatric inflammatory bowel disease, and the relationship with biochemical markers of disease activity. Aliment. Pharmacol. Ther. 2016, 44, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Halpin, S.J.; Ford, A. Prevalence of Symptoms Meeting Criteria for Irritable Bowel Syndrome in Inflammatory Bowel Disease: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2012, 107, 1474–1482. [Google Scholar] [CrossRef]
- Silvester, J.A.; Graff, L.A.; Rigaux, L.; Bernstein, C.N.; Leffler, D.A.; Kelly, C.P.; Walker, J.R.; Duerksen, D.R. Symptoms of Functional Intestinal Disorders Are Common in Patients with Celiac Disease Following Transition to a Gluten-Free Diet. Dig. Dis. Sci. 2017, 62, 2449–2454. [Google Scholar] [CrossRef]
- Kovacic, K.; Chelimsky, T.C.; Sood, M.R.; Simpson, P.; Nugent, M.; Chelimsky, G. Joint Hypermobility: A Common Association with Complex Functional Gastrointestinal Disorders. J. Pediatr. 2014, 165, 973–978. [Google Scholar] [CrossRef]
- Phatak, U.P.; Pashankar, D.S. Prevalence of functional gastrointestinal disorders in obese and overweight children. Int. J. Obes. 2014, 38, 1324–1327. [Google Scholar] [CrossRef]
- Saps, M.; Sansotta, N.; Bingham, S.; Magazzu, G.; Grosso, C.; Romano, S.; Pusatcioglu, C.; Guandalini, S. Abdominal Pain-Associated Functional Gastrointestinal Disorder Prevalence in Children and Adolescents with Celiac Disease on Gluten-Free Diet: A Multinational Study. J. Pediatr. 2017, 182, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Benítez, C.A.; Ruiz-Extremera, Á.; Saps, M. Case–control study on generalised joint hypermobility in schoolchildren with functional gastrointestinal disorders according to Rome IV criteria in Spanish. An. Pediatr. 2019, 91, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, L.C.; McFatrich, M.; Lucas, N.; Walker, J.S.; Withycombe, J.S.; Hinds, P.S.; Sung, L.; Tomlinson, D.; Freyer, D.R.; Mack, J.W.; et al. Child and adolescent self-report symptom measurement in pediatric oncology research: A systematic literature review. Qual. Life Res. 2017, 27, 291–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, E.; Stewart-Brown, S.; Fitzpatrick, R. Agreement between adolescent self-report and parent reports of health and well-being: Results of an epidemiological study. Child Care Health Dev. 2003, 29, 501–509. [Google Scholar] [CrossRef] [PubMed]
| Author | Year | Country | Population Sampling | Recruitment Site | Rome IV Completion | Cohort Number | Age | Gender |
|---|---|---|---|---|---|---|---|---|
| * Aydemir [9] | 2020 | Turkey | Matched controls | - | Researcher | 78 | - | 53% F |
| Beser [10] | 2019 | Turkey | Random sampling | Regional out-patient clinics | Physician | 2383 | Range 0 to 12 m | - |
| Chanis [11] | 2019 | Panama | Random sampling | One well-child clinic | Parent | 65 | Mean 6.9 m (SD 3.9) | 44.6% F |
| Chew [12] | 2021 | Malaysia | Whole population | Regional well-baby clinics | Parent | 534 | Mean 6.8 m (SD 3.4) Range 1 to 12 m | 54.1% F |
| Chikunov [13] | 2019 | Russia | Random sampling | One University clinic | Unclear | 300 0–6 m: 180 7 m−4 y: 120 | Range 0 to 4 y | Age 0–6 m 38.9% F Age 7 m−4 y 58.3% F |
| * Ekinci [14] | 2019 | Turkey | Matched controls | - | Child/family | 100 | Mean 9.7 (SD 3.6) Range 4 to 18 y | 34% F |
| * Ekinci [15] | 2019 | Turkey | Matched controls | - | Unclear | 78 | Median 9.2 y (IQR 4.5–17.7) Range 4 to 18 y | 33% F |
| Jativa-Marino [16] | 2019 | Ecuador | Random sampling | Regional schools | Child | 951 | Mean 11.2 y (SD 1.8) | 39.3% F |
| Llanos-Chea [17] | 2019 | Colombia | Random sampling | Regional well-child clinics | Parent | 815 | Mean 17.6 m Range 1 to 48 m | - |
| Ozdemir [18] | 2018 | Turkey | Random sampling | One out-patient clinic | Unclear | 481 | Range 0 to 12 m | - |
| Robin [19] | 2018 | United States | Random but mothers only | Internet survey | Mother | 1255 0–12 m: 58 1–3 y: 238 4–18 y: 959 | Mean 8.35 y Range 0 to 18 y | 53.2% F |
| Saps [20] | 2018 | Colombia | Random sampling | Regional schools | Child | 3567 | Mean 13.7 y (SD 2.4) | 56.5% F |
| Saps [21] | 2020 | Colombia | Random sampling | Regional out-patient clinics | Parent | 1334 0–12 m: 389 13–48 m: 945 | Mean 24.4 m (SD 15) | 51% F |
| Steutel [22] | 2020 | Belgium Italy Netherlands | Random sampling | Regional well-child clinics | Researcher | 2751 0–12 m: 1698 13–48 m: 1053 | Age 0–1 m: Median 4.1 m (IQR 2.1–7.5) Age 13–48 m: Median 26.4 m (IQR 18.7–38.7) | Age 0–1 m 47.4% F Age 13–48 m 48.2% F |
| Velasco-Benitez [23] | 2018 | Colombia | Random sampling | One school | Child | 330 | Range 10 to 18 y | 50.3% F |
| Velasco-Benitez [24] | 2019 | Colombia | Random sampling | - | Parents | 1298 | Mean 24.9 m (SD 15.1) | 51.2% F |
| Velasco-Benitez [25] | 2020 | Colombia | Random sampling | Regional schools | Child/family | 1497 | Mean 13.4 y (SD 2.1) Range 10 to 18 y | 71% F |
| Velasco-Benítez [26] | 2021 | Colombia | Random sampling | Regional schools | Child | 465 | Mean 12.9 y (SD 1.3) Range 10 to 18 y | 48.2% F |
| Vlad [27] | 2019 | Romania | Random sampling | Regional family clinics | Unclear | 308 0–12 m: 174 1–3 y: 134 | Mean 12.2 m Range 0 to 3 y | - |
| Zeevenhooven [28] | 2019 | Netherlands | Selected cohort | Follow up clinic | Child/family | 102 | Median 17 y (IQR 17–17) | 56% F |
| First Author | Age Range | Cohort Number | % with at Least One FGID | Infant Regurgitation | Rumination Syndrome | Cyclic Vomiting | Infant Colic | Functional Diarrhoea | Infant Dyschezia | Functional Constipation |
|---|---|---|---|---|---|---|---|---|---|---|
| Beser [10] | 0–12 m | 2383 | 35.1 | 13.4 | - | - | 19.2 | - | 9.8 | - |
| Chanis [11] | 0–12 m | 65 | 40 | 21 | 0 | 0 | 25 | 0 | 2.3 | 7.7 |
| Chew [12] | 1–12 m | 534 | 14.6 | 10.5 | 1.7 | 0 | 1.9 | 0.3 | 1.3 | 1.1 |
| Chikunov [13] | 0–6 m | 180 | 23 | 5.6 | 1 | 0.6 | 19.4 | 2.2 | 5.6 | 3.9 |
| 7 m−4 y | 120 | 18 | 0.8 | 0.8 | 3.3 | 1.65 | 6.7 | 0.8 | 31.7 | |
| Llanos-Chea [17] | 1–48 m | 815 | 21.2 | - | - | - | - | - | - | 9.6 # |
| Ozdemir [18] | 0–12 m | 481 | 5.8 | 4.1 | - | - | 2.2 | - | 0.62 | - |
| Robin [19] | 0–12 m | 58 | 37.9 | 24 | 1.7 | 1.7 | 5.2 | 0 | 0 | 12.1 |
| Robin [19] | 13–36 m | 238 | 21.4 | * | 2.1 | 2.1 | * | 0 | * | 18.5 |
| Saps [21] | 0–12 m | 389 | 30.6 | - | - | - | - | - | - | 7.7 # |
| 13–48 m | 945 | - | - | - | - | - | - | 26.5 # | ||
| Steutel [22] | 0–12 m | 1698 | 24.7 | 13.8 | 4.3 | 0.7 | 4.2 | 0.1 | 4.0 | 3.0 |
| 13–48 m | 1053 | 11.3 | * | 0 | 1.5 | * | 0.6 | * | 9.7 | |
| Velasco-Benitez [24] | 0–12 m | 1298 | 32.1 | 16.7 | - | - | 5.4 | - | 2.9 | 7.9 |
| 13–48 m | * | 1.8 | 1.7 | * | 0.4 | * | 29.5 | |||
| Vlad [27] | 0–12 m | 174 | 21.4 | 15.5 | 5.2 | 0.5 | 5.1 | 0 | 6.9 | 6.3 |
| 13–48 m | 134 | * | 0.7 | 1.5 | * | 0 | * | 8.9 |
| Functional Nausea and Vomiting Disorders | Functional abdominal Pain disorders | Functional Defecation Disorders | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First author | Cohort number | % with at least one FGID | Cyclic vomiting | Functional nausea and vomiting | Rumination syndrome | Aerophagia | Functional dyspepsia | Irritable bowel syndrome | Abdominal migraine | Functional abdominal pain | Functional constipation | Fecal incontinence |
| Aydemir [9] | 78 | 19.2 | 0 | 2.6 | 0 | 0 | 0 | 6.4 | 0 | 1.3 | 6.4 | 2.6 |
| Ekinci [14] | 100 | 19 | 0 | 0 | 0 | 0 | 10 | 3 | 0 | 4 | 4 | 0 |
| Ekinci [15] | 78 | 19.2 | 0 | 0 | 0 | 0 | 10.3 | 2.6 | 0 | 5.1 | 3.8 | 0 |
| Jativa-Marino [16] | 951 | 22.3 | - | - | - | - | - | - | - | - | 14.4 # | - |
| Robin [19] | 959 | 25 | 2 | 1.9 | 0 | 2.6 | 7.6 | 5.1 | 1.1 | 3.1 | 14.1 | 0.2 |
| Saps [20] | 3567 | 21.2 | 0.5 | 0.7 | 0.5 | 0.5 | 3 | 2.3 | 0.5 | 2.4 | 10.7 | 0.1 |
| Velasco-Benítez [26] | 465 | 20.8 | 3.3 | 3.3 | 1.7 | 1.7 | 6.1 | 0.6 | 3.3 | 0.6 | 28.7 | 0 |
| Velasco-Benitez [23] | 330 | 40.0 | - | - | - | - | 5.2 | 6.1 | - | 4.9 | 22.7 | - |
| Velasco-Benitez [25] | 1497 | 22.7 | 1.5 | 1.5 | 0.5 | 0.4 | 2.6 | 2.0 | 0.3 | 0.9 | 13 | 0 |
| Zeevenhooven [28] | 102 | 27 | 1 | 0 | 0 | 0 | 15 | 0 | 0 | 0 | 3 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vernon-Roberts, A.; Alexander, I.; Day, A.S. Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). J. Clin. Med. 2021, 10, 5087. https://doi.org/10.3390/jcm10215087
Vernon-Roberts A, Alexander I, Day AS. Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). Journal of Clinical Medicine. 2021; 10(21):5087. https://doi.org/10.3390/jcm10215087
Chicago/Turabian StyleVernon-Roberts, Angharad, India Alexander, and Andrew S. Day. 2021. "Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria)" Journal of Clinical Medicine 10, no. 21: 5087. https://doi.org/10.3390/jcm10215087
APA StyleVernon-Roberts, A., Alexander, I., & Day, A. S. (2021). Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). Journal of Clinical Medicine, 10(21), 5087. https://doi.org/10.3390/jcm10215087