
Efficacy of Catheter Ablation for Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy—A Multicenter Study

 , ,
, ,  ,
,  ,
,  ,
,  , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Study Inclusion Criteria
- -
- An ARVC diagnosis in accordance with the 2010 International Task Force Criteria (ITFC) [14]. Only patients reaching a “definite” diagnosis were included in the final cohort.
- -
- Performance of CA for an atrial arrhythmia of interest at any point during the clinical course; atrial arrhythmias of interest were AF, left-sided atrial tachycardia (AT), and CTI-dependent AFl. No ablation strategy or ablation energy source was pre-specified for study enrollment.
- -
- A minimum follow-up time of 6 months, with at least one follow-up visit with an arrhythmic assessment after CA.
2.2. Data Collection
2.3. Study Definitions, Aims, and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Periprocedural Data
3.3. Procedural Data
3.4. Acute Procedural Data
3.5. Long-Term Outcome Data
4. Discussion
4.1. Atrial Arrhythmias and ARVC
4.2. Outcomes of Catheter Ablation of Atrial Arrhythmias in ARVC
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Corrado, D.; Link, M.S.; Calkins, H. Arrhythmogenic Right Ventricular Cardiomyopathy. N. Engl. J. Med. 2017, 376, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Fox, P.R.; Maron, B.J.; Basso, C.; Liu, S.-K.; Thiene, G. Spontaneously Occurring Arrhythmogenic Right Ventricular Cardiomyopathy in the Domestic Cat: A New Animal Model Similar to the Human Disease. Circulation 2000, 102, 1863–1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saguner, A.M.; Ganahl, S.; Kraus, A.; Baldinger, S.H.; Medeiros-Domingo, A.; Saguner, A.R.; Mueller-Burri, S.A.; Wolber, T.; Haegeli, L.M.; Krasniqi, N.; et al. Clinical Role of Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Dysplasia. Circ. J. 2014, 78, 2854–2861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zghaib, T.; Bourfiss, M.; van der Heijden, J.F.; Loh, P.; Hauer, R.N.; Tandri, H.; Calkins, H.; Nazarian, S.; te Riele, A.S.J.M.; Zimmerman, S.L.; et al. Atrial Dysfunction in Arrhythmogenic Right Ventricular Cardiomyopathy: Value of Quantitative Magnetic Resonance Analysis in Predicting Atrial Arrhythmias. Circ. Cardiovasc. Imaging 2018, 11, e007344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Fontaine, G.H.; Fan, S.; Yan, Y.; Bode, P.K.; Duru, F.; Frank, R.; Saguner, A.M. Right atrial pathology in arrhythmogenic right ventricular dysplasia. Cardiol. J. 2019, 26, 736–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platonov, P.G.; Christensen, A.H.; Holmqvist, F.; Carlson, J.; Haunsø, S.; Svendsen, J.H. Abnormal atrial activation is common in patients with arrhythmogenic right ventricular cardiomyopathy. J. Electrocardiol. 2011, 44, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camm, C.F.; James, C.A.; Tichnell, C.; Murray, B.; Bhonsale, A.; te Riele, A.S.J.M.; Judge, D.P.; Tandri, H.; Calkins, H. Prevalence of atrial arrhythmias in arrhythmogenic right ventricular dysplasia/cardiomyopathy. Heart Rhythm 2013, 10, 1661–1668. [Google Scholar] [CrossRef] [PubMed]
- Baturova, M.A.; Haugaa, K.H.; Jensen, H.K.; Svensson, A.; Gilljam, T.; Bundgaard, H.; Madsen, T.; Hansen, J.; Chivulescu, M.; Christiansen, M.K.; et al. Atrial fibrillation as a clinical characteristic of arrhythmogenic right ventricular cardiomyopathy: Experience from the Nordic ARVC Registry. Int. J. Cardiol. 2020, 298, 39–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rujirachun, P.; Wattanachayakul, P.; Charoenngam, N.; Winijkul, A.; Ungprasert, P. Prevalence of atrial arrhythmia in patients with arrhythmogenic right ventricular cardiomyopathy: A systematic review and meta-analysis. J. Cardiovasc. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.-P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, A.F.; Zado, E.; Marchlinski, F.E. Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia and Ventricular Tachycardia. Am. J. Cardiol. 2010, 106, 720–722. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Guarache, R.; Åström-Aneq, M.; Oesterle, A.; Asirvatham, R.; Svetlichnaya, J.; Marcus, G.M.; Gerstenfeld, E.P.; Klein, L.; Scheinman, M.M. Atrial arrhythmias in patients with arrhythmogenic right ventricular cardiomyopathy: Prevalence, echocardiographic predictors, and treatment. J. Cardiovasc. Electrophysiol. 2019, 30, 1801–1810. [Google Scholar] [CrossRef] [PubMed]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.; Basso, C.; Bauce, B.; Bluemke, D.A.; Calkins, H.; Corrado, D.; Cox, M.G.P.J.; Daubert, J.P.; et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: Proposed Modification of the Task Force Criteria. Eur. Heart J. 2010, 31, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, T.F.; Yilmaz, D.; Lindeboom, R.; Buiten, M.S.; Olde Nordkamp, L.R.A.; Schalij, M.J.; Wilde, A.A.; van Erven, L.; Knops, R.E. Long-Term Clinical Outcomes of Subcutaneous versus Transvenous Implantable Defibrillator Therapy. J. Am. Coll. Cardiol. 2016, 68, 2047–2055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzanti, A.; Ng, K.; Faragli, A.; Maragna, R.; Chiodaroli, E.; Orphanou, N.; Monteforte, N.; Memmi, M.; Gambelli, P.; Novelli, V.; et al. Arrhythmogenic Right Ventricular Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 68, 2540–2550. [Google Scholar] [CrossRef]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of Catheter Ablation vs. Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest among Patients with Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1261. [Google Scholar] [CrossRef]
- Müssigbrodt, A.; Knopp, H.; Efimova, E.; Weber, A.; Bertagnolli, L.; Hilbert, S.; Kosiuk, J.; Dinov, B.; Bode, K.; Kircher, S.; et al. Supraventricular arrhythmias in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy associate with long-term outcome after catheter ablation of ventricular tachycardias. EP Eur. 2018, 20, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Mugnai, G.; Hünük, B.; Ströker, E.; Ruggiero, D.; Coutino-Moreno, H.E.; Takarada, K.; De Regibus, V.; Choudhury, R.; Abugattas de Torres, J.P.; Moran, D.; et al. Long-term outcome of pulmonary vein isolation in patients with paroxysmal atrial fibrillation and Brugada syndrome. EP Eur. 2018, 20, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Jiang, W.; Dai, J.; Li, K.; Shi, H.; Wu, W.; Liu, X.; He, B.; Qiu, X.; Song, Z. Five-year outcomes after catheter ablation for atrial fibrillation in patients with hypertrophic cardiomyopathy. J. Cardiovasc. Electrophysiol. 2020, 31, 621–628. [Google Scholar] [CrossRef]


{kind=link}
| ARVC Diagnostic Characteristics | |
|---|---|
| Age at ARVC diagnosis (years), mean ± s.d. | 50.2 ± 16.6 |
| Sustained VAs before/at ARVC diagnosis, n (%) | 24 (65) |
| ARVC score, median [IQR] | 5 (4–6) |
| Category I—Global or regional dysfunction | |
| Major, n (%) | 20 (54) |
| Minor, n (%) | 11 (30) |
| Category II—Tissue characterization of the wall | |
| Major, n (%) | 4 (11) |
| Minor, n (%) | 3 (8) |
| Category III—Repolarization abnormalities | |
| Major, n (%) | 13 (35) |
| Minor, n (%) | 9 (26) |
| Category IV—Depolarization abnormalities | |
| Major, n (%) | 10 (27) |
| Minor, n (%) | 12 (32) |
| Category V—Ventricular arrhythmias | |
| Major, n (%) | 19 (51) |
| Minor, n (%) | 16 (43) |
| Category VI—Family history | |
| Major, n (%) | 3 (8) |
| Minor, n (%) | 4 (11) |
| Genetic testing performed, n (%) | 13 (35) |
| Negative, n (%) | 6 (46) * |
| Positive, n (%) | 7 (54) * |
| PKP-2, n (%) | 5 (71) * |
| DSG-2, n (%) | 2 (29) * |
| Baseline Characteristics (Overall Cohort, n = 37) | |
|---|---|
| Male, n (%) | 31 (84) |
| Age at first atrial arrhythmia presentation (years), mean ± s.d. | 48.7 ± 15.3 |
| First atrial arrhythmia type | |
| Atrial fibrillation, n (%) | 23 (62) |
| Paroxysmal, n (%) | 16 (43) |
| Persistent, n (%) | 5 (14) |
| Long-standing persistent, n (%) | 2 (5) |
| Focal left-sided atrial tachycardia, n (%) | 5 (14) |
| Cavotricuspid isthmus-dependent atrial flutter, n (%) | 9 (24) |
| Probands, n (%) | 32 (87) |
| Athletes, n (%) | 7 (19) |
| BSA (m2), median [IQR] | 1.9 (1.8–2.1) |
| CHA2DS2VASc, median [IQR] | 1 (1,2) |
| Age > 64 y.o., n (%) | 7 (19) |
| Age > 74 y.o., n (%) | 2 (5) |
| History of CHF, n (%) | 15 (41) |
| Female gender, n (%) | 6 (16) |
| Hypertension, n (%) | 12 (32) |
| Previous stroke/TIA, n (%) | 3 (8) |
| Vascular disease history, n (%) | 4 (11) |
| Diabetes, n (%) | 3 (8) |
| HAS-BLED, median [IQR] | 1 (0–2) |
| Age > 65 y.o, n (%) | 9 (24) |
| Hypertension, n (%) | 12 (32) |
| Renal disease, n (%) | 4 (11) |
| Liver disease, n (%) | 0 |
| Stroke history, n (%) | 3 (8) |
| Prior major bleeding, n (%) | 1 (3) |
| Labile INR, n (%) | 1 (3) |
| Medication predisposing bleeding, n (%) | 14 (38) |
| Alcohol abuse, n (%) | 3 (8) |
| EHRA score, median [IQR] | 1 (0–2) |
| ICD, n (%) | 28 (76) |
| Inappropriate discharge due to atrial arrhythmia, n (%) | 3 (8) |
| Periprocedural and Procedural Characteristics | |
|---|---|
| Age at CA (years), mean ± s.d. | 49.0 ± 15.4 |
| Pharmacological therapy at the time of CA | |
| Oral anticoagulation, n (%) | 23 (62) |
| VKA, n (%) | 10 (27) |
| DOAC, n (%) | 13 (35) |
| Anti-arrhythmic therapy, n (%) | 11 (30) |
| Class Ic, n (%) | 3 (8) |
| Class III, n (%) | 8 (22) |
| Morphology and functional data at the time of CA | |
| Right atrial dimension available, n (%) | 30 (81) |
| Normal dimension, n (%) | 17 (57) * |
| Moderate dilation, n (%) | 9 (30) * |
| Severe dilation, n (%) | 4 (13) * |
| Left atrial dimension available, n (%) | 32 (86) |
| Normal dimension, n (%) | 29 (91) * |
| Moderate dilation, n (%) | 1 (3) * |
| Severe dilation, n (%) | 2 (6) * |
| RVEF available, n (%) | 21 (57) |
| Normal (>49%), n (%) | 4 (19) * |
| Reduced (26–49%), n (%) | 15 (71) * |
| Severely reduced (<26%), n (%) | 2 (10) * |
| LVEF (%), mean ± s.d. | 52.4 ± 6.8 |
| Area targeted during CA | |
| Pulmonary vein isolation, n (%) | 23 (62) |
| PVI only, n (%) | 16 (43) |
| PVI + anterior mitral line, n (%) | 4 (11) |
| PVI + posterior wall isolation, n (%) | 2 (5) |
| PVI + roof line, n (%) | 1 (3) |
| Non-PVI-based left-sided procedures, n (%) | 5 (14) |
| Focal ablation, n (%) | 4 (11) |
| Anterior mitral line, n (%) | 1 (3) |
| Stand-alone CTI ablation, n (%) | 9 (24) |
| Power settings for ablation, Watts [IQR] | 40 (35–40) |
| Procedural time | |
| Left-sided procedure (min), median [IQR] | 140 (105–143) |
| Right-sided procedure (min), median [IQR] | 70 (60–110) |
| Fluoroscopy time | |
| Left-sided procedure (min), median [IQR] | 18.5 (11.7–19.5) |
| Right-sided procedure (min), median [IQR] | 13.5 (12.0–14.0) |
| Acute Success, n (%) | 36 (97) |
| Pulmonary vein isolation, n (%) | 23 (100) |
| Non PVI-based left-sided procedure, n (%) | 4 (80) |
| Stand-alone CTI, n (%) | 9 (100) |
| Need for ECV during procedure, n (%) | 6 (16) |
| Complications, n (%) | 2 (5.4) |
| Vascular access hematoma, n (%) | 1 (2.7) |
| PV stenosis, n (%) | 1 (2.7) |
| Outcome Analysis | |
|---|---|
| Follow-up time (months), median [IQR] | 27 (13–67) |
| Single-procedural freedom from any atrial arrhythmia | |
| At 6 months, n (%) | 35/37 (95) |
| After PVI, n (%) | 22/23 (96) |
| After non-PVI-based left-sided procedure, n (%) | 4/5 (80) |
| After CTI ablation, n (%) | 9/9 (100) |
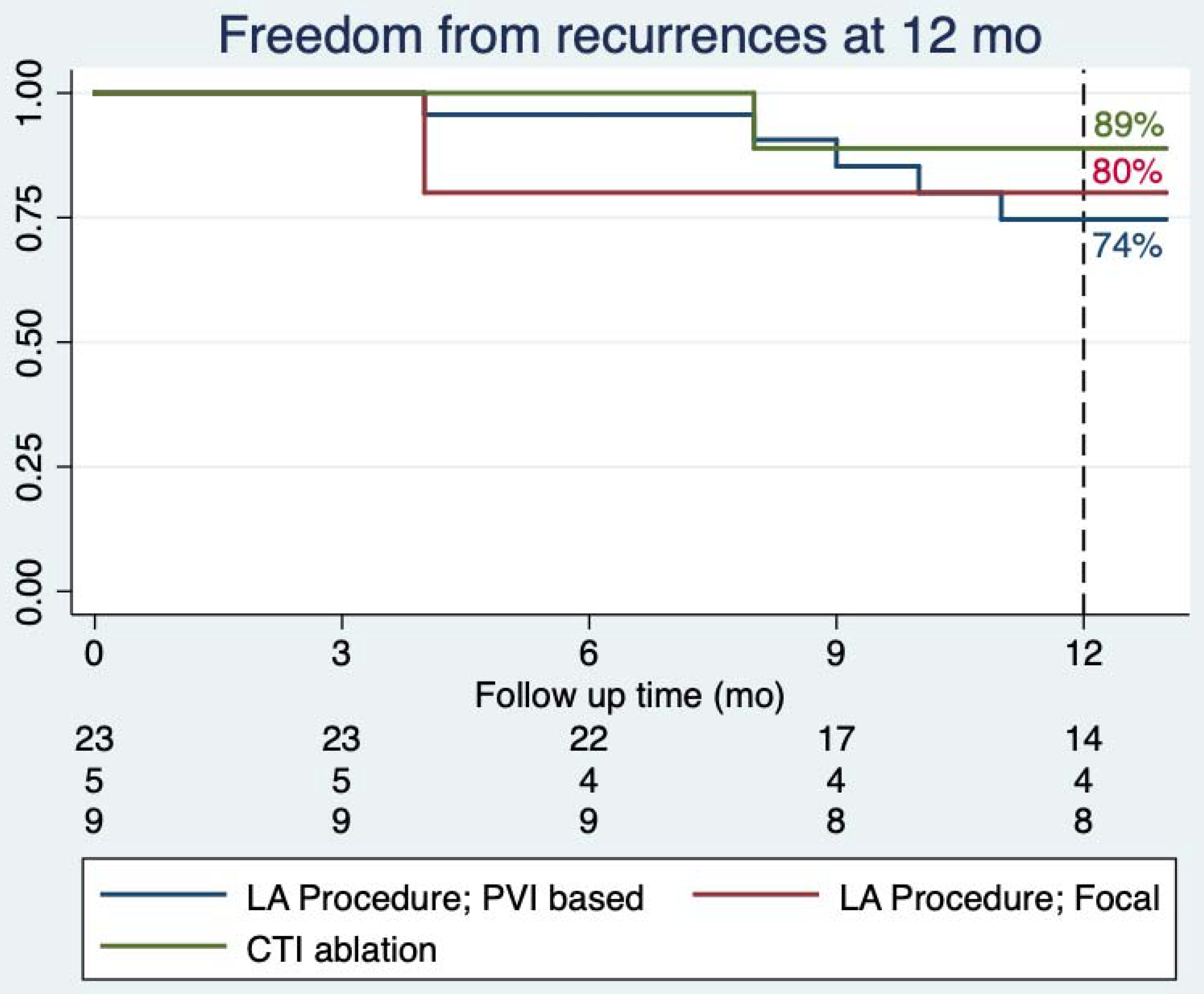
| At 12 months, n (%) | 26/33 (79) |
| After PVI, n (%) | 14/19 (74) |
| After non-PVI-based left-sided procedure, n (%) | 4/5 (80) |
| After CTI ablation, n (%) | 8/9 (89) |
| At last available follow-up, n (%) | 25/37 (68) |
| After PVI, n (%) | 14/23 (61) |
| After non-PVI-based left-sided procedure, n (%) | 3/5 (60) |
| After CTI ablation, n (%) | 8/9 (89) |
| Pharmacological therapy at last available follow-up | |
| Oral anticoagulation, n (%) | 17 (46) |
| VKA, n (%) | 8 (22) |
| DOAC, n (%) | 9 (24) |
| Anti-arrhythmic therapy, n (%) | 9 (24) |
| Class Ib, n (%) | 1 (3) |
| Class Ic, n (%) | 5 (14) |
| Class III, n (%) | 3 (8) |
| LVEF at last available follow-up, mean ± standard deviation | 49.4 ± 12.4 |
| Major bleeding during follow-up, n (%) | 0 |
| Stroke/TIA during follow-up, n (%) | 0 |
| Inappropriate ICD shock due to atrial arrhythmias at follow-up, n (%) | 0 |
| Patients undergoing a repeat procedure, n (%) | 7 (19) |
| PVI, n (%) | 3 (8) |
| Anterior mitral line, n (%) | 2 (5) |
| Focal ablation, n (%) | 1 (3) |
| CTI ablation, n (%) | 1 (3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasperetti, A.; James, C.A.; Chen, L.; Schenker, N.; Casella, M.; Kany, S.; Mathew, S.; Compagnucci, P.; Müssigbrodt, A.; Jensen, H.K.; et al. Efficacy of Catheter Ablation for Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy—A Multicenter Study. J. Clin. Med. 2021, 10, 4962. https://doi.org/10.3390/jcm10214962
Gasperetti A, James CA, Chen L, Schenker N, Casella M, Kany S, Mathew S, Compagnucci P, Müssigbrodt A, Jensen HK, et al. Efficacy of Catheter Ablation for Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy—A Multicenter Study. Journal of Clinical Medicine. 2021; 10(21):4962. https://doi.org/10.3390/jcm10214962
Chicago/Turabian StyleGasperetti, Alessio, Cynthia A. James, Liang Chen, Niklas Schenker, Michela Casella, Shinwan Kany, Shibu Mathew, Paolo Compagnucci, Andreas Müssigbrodt, Henrik K. Jensen, and et al. 2021. "Efficacy of Catheter Ablation for Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy—A Multicenter Study" Journal of Clinical Medicine 10, no. 21: 4962. https://doi.org/10.3390/jcm10214962
APA StyleGasperetti, A., James, C. A., Chen, L., Schenker, N., Casella, M., Kany, S., Mathew, S., Compagnucci, P., Müssigbrodt, A., Jensen, H. K., Svensson, A., Costa, S., Forleo, G. B., Platonov, P. G., Tondo, C., Song, J.-P., Dello Russo, A., Ruschitzka, F., Brunckhorst, C., ... Saguner, A. M. (2021). Efficacy of Catheter Ablation for Atrial Arrhythmias in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy—A Multicenter Study. Journal of Clinical Medicine, 10(21), 4962. https://doi.org/10.3390/jcm10214962