
Potential Targets Other Than PSMA for Prostate Cancer Theranostics: A Systematic Review

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
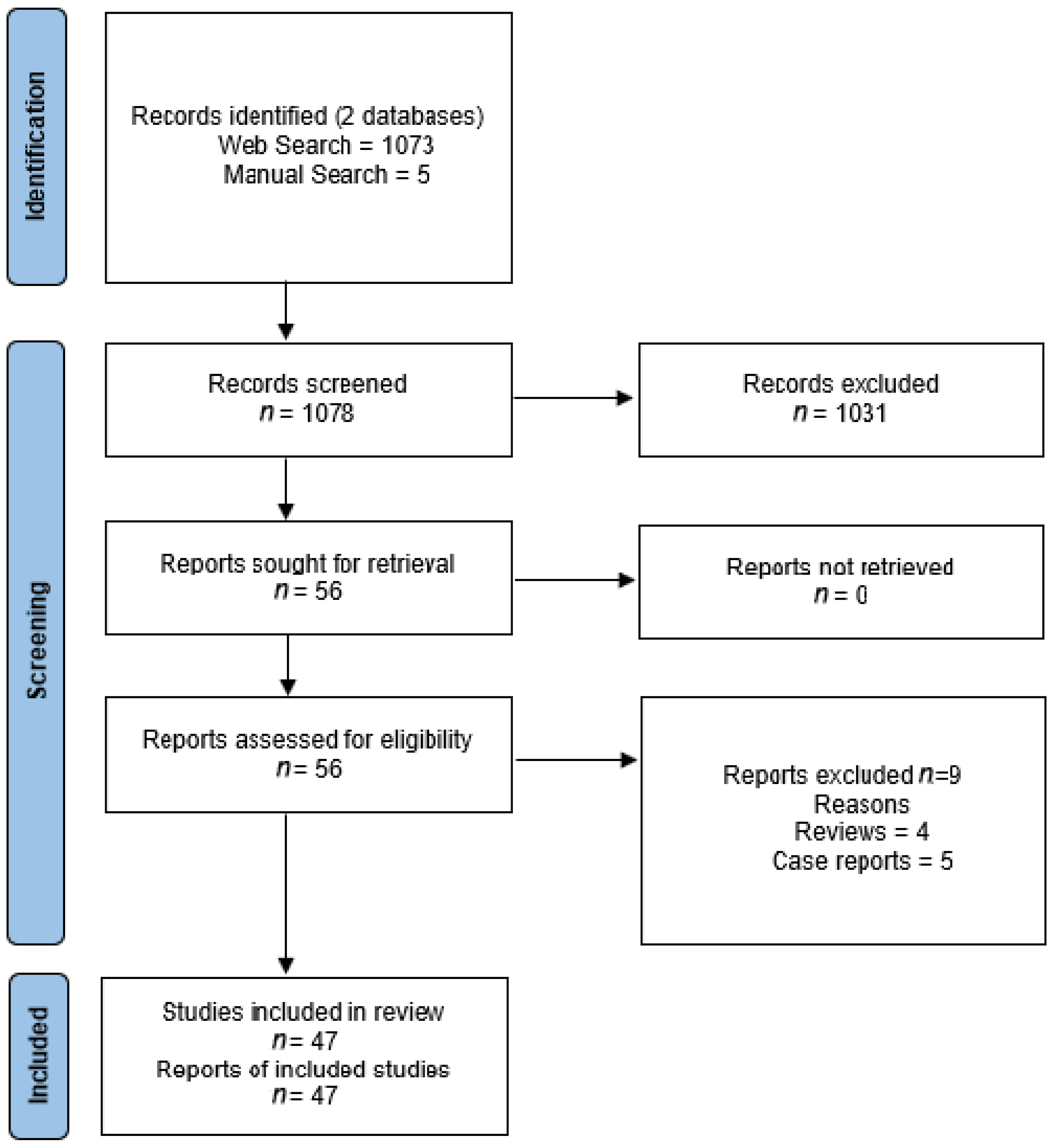
3.1. Study Selection
3.2. Current Targets Other Than PSMA for Prostate Cancer Theranostics
3.2.1. Gastrin-Releasing Peptide Receptors
3.2.2. Androgen Receptor
3.2.3. Somatostatin Receptors
3.2.4. Urokinase Plasminogen Activator Surface Receptor
3.2.5. Fibroblast Activation Protein
3.2.6. Integrin Receptors
4. Discussion
4.1. Current Targets Other Than PSMA for Prostate Cancer Theranostics
4.2. Future Directions for Prostate Cancer Theranostics in Nuclear Medicine
4.3. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- European Association of Urology EAU Guidelines: Oncology Guidelines. Available online: https://uroweb.org/individual-guidelines/oncology-guidelines/ (accessed on 11 August 2021).
- Association Française d’Urologie Recommandations de l’A.F.U. Classées Par Année | Urofrance. Available online: https://www.urofrance.org/outils-et-recommandations/recommandations/recommandations-afu/classees-par-annee.html (accessed on 11 August 2021).
- Thompson, I.M.; Valicenti, R.K.; Albertsen, P.C.; Davis, B.; Goldenberg, S.L.; Hahn, C.; Klein, A.E.; Michalski, J.M.; Roach, M.; Sartor, O.; et al. Adjuvant and Salvage Radiotherapy After Prostatectomy: AUA/ASTRO Guideline. J. Urol. 2013, 190, 441–449. [Google Scholar] [CrossRef]
- Virgo, K.S.; Rumble, R.B.; de Wit, R.; Mendelson, D.S.; Smith, T.J.; Taplin, M.-E.; Wade, J.L.; Bennett, C.L.; Scher, H.I.; Nguyen, P.L.; et al. Initial Management of Noncastrate Advanced, Recurrent, or Metastatic Prostate Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 1274–1305. [Google Scholar] [CrossRef] [PubMed]
- Virgo, K.S.; Basch, E.; Loblaw, D.A.; Oliver, T.K.; Rumble, R.B.; Carducci, M.A.; Nordquist, L.; Taplin, M.-E.; Winquist, E.; Singer, E.A. Second-Line Hormonal Therapy for Men With Chemotherapy-Naïve, Castration-Resistant Prostate Cancer: American Society of Clinical Oncology Provisional Clinical Opinion. J. Clin. Oncol. 2017, 35, 1952–1964. [Google Scholar] [CrossRef] [Green Version]
- Von Eyben, F.E.; Roviello, G.; Kiljunen, T.; Uprimny, C.; Virgolini, I.; Kairemo, K.; Joensuu, T. Third-line treatment and 177Lu-PSMA radioligand therapy of metastatic castration-resistant prostate cancer: A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2017, 45, 496–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Kasperzyk, J.L.; Finn, S.; Flavin, R.; Fiorentino, M.; Lis, R.; Hendrickson, W.K.; Clinton, S.K.; Sesso, H.D.; Giovannucci, E.L.; Stampfer, M.J.; et al. Prostate-Specific Membrane Antigen Protein Expression in Tumor Tissue and Risk of Lethal Prostate Cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 2354–2363. [Google Scholar] [CrossRef] [Green Version]
- Emmett, L.; Willowson, K.; Violet, J.; Shin, J.; Blanksby, A.; Lee, J. Lutetium177PSMA radionuclide therapy for men with prostate cancer: A review of the current literature and discussion of practical aspects of therapy. J. Med. Radiat. Sci. 2017, 64, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Van De Wiele, C.; Dumont, F.; Broecke, R.V.; Oosterlinck, W.; Cocquyt, V.; Serreyn, R.; Peers, S.; Thornback, J.; Slegers, G.; Dierckx, R.A. Technetium-99m RP527, a GRP analogue for visualisation of GRP receptor-expressing malignancies: A feasibility study. Eur. J. Nucl. Med. Mol. Imaging 2000, 27, 1694–1699. [Google Scholar] [CrossRef] [PubMed]
- De Vincentis, G.; Scopinaro, F.; Varvarigou, A.; Ussof, W.; Schillaci, O.; Archimandritis, S.; Corleto, V.; Longo, F.; Delle Fave, G. Phase I Trial of Technetium [Leu13] Bombesin as Cancer Seeking Agent: Possible Scintigraphic Guide for Surgery? Tumori 2002, 88, S28–S30. [Google Scholar] [CrossRef] [PubMed]
- Scopinaro, F.; De Vincentis, G.; Varvarigou, A.D.; Laurenti, C.; Iori, F.; Remediani, S.; Chiarini, S.; Stella, S. 99mTc-Bombesin Detects Prostate Cancer and Invasion of Pelvic Lymph Nodes. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Mather, S.J.; Nock, B.A.; Maina, T.; Gibson, V.; Ellison, D.; Murray, I.; Sobnack, R.; Colebrook, S.; Wan, S.; Halberrt, G.; et al. GRP Receptor Imaging of Prostate Cancer Using [99mTc]Demobesin 4: A First-in-Man Study. Mol. Imaging Biol. 2014, 16, 888–895. [Google Scholar] [CrossRef]
- Kähkönen, E.; Jambor, I.; Kemppainen, J.; Lehtiö, K.; Grönroos, T.J.; Kuisma, A.; Luoto, P.; Sipilä, H.J.; Tolvanen, T.; Alanen, K.; et al. In Vivo Imaging of Prostate Cancer Using [68Ga]-Labeled Bombesin Analog BAY86-7548. Clin. Cancer Res. 2013, 19, 5434–5443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wieser, G.; Mansi, R.; Grosu, A.L.; Schultze-Seemann, W.; Dumont-Walter, R.A.; Meyer, P.T.; Maecke, H.R.; Reubi, J.C.; Weber, W.A. Positron Emission Tomography (PET) Imaging of Prostate Cancer with a Gastrin Releasing Peptide Receptor Antagonist-from Mice to Men. Theranostics 2014, 4, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Sah, B.-R.; Burger, I.A.; Schibli, R.; Friebe, M.; Dinkelborg, L.; Graham, K.; Borkowski, S.; Bacher-Stier, C.; Valencia, R.; Srinivasan, A.; et al. Dosimetry and First Clinical Evaluation of the New 18F-Radiolabeled Bombesin Analogue BAY 864367 in Patients with Prostate Cancer. J. Nucl. Med. 2015, 56, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maina, T.; Bergsma, H.; Kulkarni, H.R.; Mueller, D.; Charalambidis, D.; Krenning, E.P.; Nock, B.A.; De Jong, M.; Baum, R.P. Preclinical and first clinical experience with the gastrin-releasing peptide receptor-antagonist [68Ga]SB3 and PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2015, 43, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Minamimoto, R.; Hancock, S.; Schneider, B.; Chin, F.T.; Jamali, M.; Loening, A.; Vasanawala, S.; Gambhir, S.S.; Iagaru, A. Pilot Comparison of 68Ga-RM2 PET and 68Ga-PSMA-11 PET in Patients with Biochemically Recurrent Prostate Cancer. J. Nucl. Med. 2015, 57, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nock, B.A.; Kaloudi, A.; Lymperis, E.; Giarika, A.; Kulkarni, H.R.; Klette, I.; Singh, A.; Krenning, E.P.; De Jong, M.; Maina-Nock, T.; et al. Theranostic Perspectives in Prostate Cancer with the Gastrin-Releasing Peptide Receptor Antagonist NeoBOMB1: Preclinical and First Clinical Results. J. Nucl. Med. 2016, 58, 75–80. [Google Scholar] [CrossRef]
- Wieser, G.; Popp, I.; Drendel, V.; Grosu, A.-L.; Bartholomä, M.; Mansi, R.; Wetterauer, U.; Schultze-Seemann, W.; Rischke, H.C.; Weber, W.A.; et al. Diagnosis of recurrent prostate cancer with PET/CT imaging using the gastrin-releasing peptide receptor antagonist 68Ga-RM2: Preliminary results in patients with negative or inconclusive [18F]Fluoroethylcholine-PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Minamimoto, R.; Sonni, I.; Hancock, S.; Vasanawala, S.; Loening, A.; Gambhir, S.S.; Iagaru, A. Prospective Evaluation of 68Ga-RM2 PET/MRI in Patients with Biochemical Recurrence of Prostate Cancer and Negative Findings on Conventional Imaging. J. Nucl. Med. 2017, 59, 803–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Niu, G.; Fan, X.; Lang, L.; Hou, G.; Chen, L.; Wu, H.; Zhu, Z.; Li, F.; Chen, X. PET Using a GRPR Antagonist 68Ga-RM26 in Healthy Volunteers and Prostate Cancer Patients. J. Nucl. Med. 2017, 59, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Gnesin, S.; Cicone, F.; Mitsakis, P.; Van Der Gucht, A.; Baechler, S.; Miralbell, R.; Garibotto, V.; Zilli, T.; Prior, J.O. First in-human radiation dosimetry of the gastrin-releasing peptide (GRP) receptor antagonist 68Ga-NODAGA-MJ9. EJNMMI Res. 2018, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Fassbender, T.F.; Schiller, F.; Mix, M.; Maecke, H.R.; Kiefer, S.; Drendel, V.; Meyer, P.T.; Jilg, C.A. Accuracy of [68Ga]Ga-RM2-PET/CT for diagnosis of primary prostate cancer compared to histopathology. Nucl. Med. Biol. 2019, 70, 32–38. [Google Scholar] [CrossRef]
- Touijer, K.A.; Michaud, L.; Alvarez, H.A.V.; Gopalan, A.; Kossatz, S.; Gonen, M.; Beattie, B.; Sandler, I.; Lyaschenko, S.; Eastham, J.A.; et al. Prospective Study of the Radiolabeled GRPR Antagonist BAY86-7548 for Positron Emission Tomography/Computed Tomography Imaging of Newly Diagnosed Prostate Cancer. Eur. Urol. Oncol. 2018, 2, 166–173. [Google Scholar] [CrossRef]
- Hoberück, S.; Michler, E.; Wunderlich, G.; Löck, S.; Hölscher, T.; Froehner, M.; Braune, A.; Ivan, P.; Seppelt, D.; Zöphel, K.; et al. 68Ga-RM2 PET in PSMA- positive and -negative prostate cancer patients. Nuklearmedizin 2019, 58, 352–362. [Google Scholar] [CrossRef]
- Fassbender, T.F.; Schiller, F.; Zamboglou, C.; Drendel, V.; Kiefer, S.; Jilg, C.A.; Grosu, A.-L.; Mix, M. Voxel-based comparison of [68Ga]Ga-RM2-PET/CT and [68Ga]Ga-PSMA-11-PET/CT with histopathology for diagnosis of primary prostate cancer. EJNMMI Res. 2020, 10, 62. [Google Scholar] [CrossRef] [PubMed]
- Bakker, I.L.; Fröberg, A.C.; Busstra, M.B.; Verzijlbergen, J.F.; Konijnenberg, M.; van Leenders, G.J.L.H.; Schoots, I.G.; de Blois, E.; van Weerden, W.M.; Dalm, S.U.; et al. GRPr antagonist 68Ga-SB3 PET/CT-imaging of primary prostate cancer in therapy-naive patients. J. Nucl. Med. 2021, 62. [Google Scholar] [CrossRef]
- Baratto, L.; Song, H.; Duan, H.; Hatami, N.; Bagshaw, H.; Buyyounouski, M.; Hancock, S.; Shah, S.A.; Srinivas, S.; Swift, P.; et al. PSMA- and GRPR-targeted PET: Results from 50 Patients with Biochemically Recurrent Prostate Cancer. J. Nucl. Med. 2021, 62. [Google Scholar] [CrossRef]
- Kurth, J.; Krause, B.J.; Schwarzenböck, S.M.; Bergner, C.; Hakenberg, O.W.; Heuschkel, M. First-in-human dosimetry of gastrin-releasing peptide receptor antagonist [177Lu]Lu-RM2: A radiopharmaceutical for the treatment of metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 47, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Niu, G.; Lang, L.; Li, F.; Fan, X.; Yan, X.; Yao, S.; Yan, W.; Huo, L.; Chen, L.; et al. Clinical Translation of a Dual Integrin α v β 3—and Gastrin-Releasing Peptide Receptor–Targeting PET Radiotracer, 68Ga-BBN-RGD. J. Nucl. Med. 2017, 58, 228–234. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Bravo, B.; Ramírez-Nava, G.; Mendoza-Figueroa, M.J.; Ocampo-García, B.; Ferro-Flores, G.; Ávila-Rodríguez, M.A.; Santos-Cuevas, C. [68Ga]Ga-iPSMA-Lys3-Bombesin: Biokinetics, dosimetry and first patient PET/CT imaging. Nucl. Med. Biol. 2021, 96–97, 54–60. [Google Scholar] [CrossRef]
- Larson, S.M.; Morris, M.; Gunther, I.; Beattie, B.; Humm, J.L.; Akhurst, T.A.; Finn, R.D.; Erdi, Y.; Pentlow, K.; Dyke, J.; et al. Tumor Localization of 16β-18F-Fluoro-5α-Dihydrotestosterone Versus 18F-FDG in Patients with Progressive, Metastatic Prostate Cancer. J. Nucl. Med. 2004, 45, 366–373. [Google Scholar] [PubMed]
- Zanzonico, P.B.; Finn, R.; Pentlow, K.S.; Erdi, Y.; Beattie, B.; Akhurst, T.; Squire, O.; Morris, M.J.; Scher, H.; McCarthy, T.; et al. PET-based radiation dosimetry in man of 18F-fluorodihydrotestosterone, a new radiotracer for imaging prostate cancer. J. Nucl. Med. 2004, 45, 1966–1971. [Google Scholar] [PubMed]
- Dehdashti, F.; Picus, J.; Michalski, J.M.; Dence, C.S.; Siegel, B.A.; Katzenellenbogen, J.A.; Welch, M.J. Positron tomographic assessment of androgen receptors in prostatic carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Beattie, B.J.; Smith-Jones, P.M.; Jhanwar, Y.S.; Schöder, H.; Schmidtlein, C.R.; Morris, M.J.; Zanzonico, P.; Squire, O.; Meirelles, G.S.; Finn, R.; et al. Pharmacokinetic Assessment of the Uptake of 16β-18F-Fluoro-5α-Dihydrotestosterone (FDHT) in Prostate Tumors as Measured by PET. J. Nucl. Med. 2010, 51, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Fox, J.J.; Autran-Blanc, E.; Morris, M.J.; Gavane, S.; Nehmeh, S.; Van Nuffel, A.; Gönen, M.; Schöder, H.; Humm, J.L.; Scher, H.I.; et al. Practical Approach for Comparative Analysis of Multilesion Molecular Imaging Using a Semiautomated Program for PET/CT. J. Nucl. Med. 2011, 52, 1727–1732. [Google Scholar] [CrossRef] [Green Version]
- Vargas, H.A.; Wassberg, C.; Fox, J.J.; Wibmer, A.G.; Goldman, D.A.; Kuk, D.; Gonen, M.; Larson, S.; Morris, M.J.; Scher, H.I.; et al. Bone Metastases in Castration-Resistant Prostate Cancer: Associations between Morphologic CT Patterns, Glycolytic Activity, and Androgen Receptor Expression on PET and Overall Survival. Radiology 2014, 271, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, J.J.; Gavane, S.C.; Blanc-Autran, E.; Nehmeh, S.; Gönen, M.; Beattie, B.; Vargas, H.A.; Schöder, H.; Humm, J.L.; Fine, S.W.; et al. Positron Emission Tomography/Computed Tomography–Based Assessments of Androgen Receptor Expression and Glycolytic Activity as a Prognostic Biomarker for Metastatic Castration-Resistant Prostate Cancer. JAMA Oncol. 2018, 4, 217–224. [Google Scholar] [CrossRef]
- Vargas, H.A.; Kramer, G.M.; Scott, A.M.; Weickhardt, A.; Meier, A.A.; Parada, N.; Beattie, B.J.; Humm, J.L.; Staton, K.D.; Zanzonico, P.B.; et al. Reproducibility and Repeatability of Semiquantitative 18F-Fluorodihydrotestosterone Uptake Metrics in Castration-Resistant Prostate Cancer Metastases: A Prospective Multicenter Study. J. Nucl. Med. 2018, 59, 1516–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, B.H.E.; Kramer, G.M.; Cysouw, M.C.F.; Yaqub, M.M.; de Keizer, B.; Lavalaye, J.; Booij, J.; Vargas, H.A.; Morris, M.J.; Vis, A.N.; et al. Healthy Tissue Uptake of 68Ga-Prostate-Specific Membrane Antigen, 18F-DCFPyL, 18F-Fluoromethylcholine, and 18F-Dihydrotestosterone. J. Nucl. Med. 2019, 60, 1111–1117. [Google Scholar] [CrossRef] [Green Version]
- Kramer, G.M.; Yaqub, M.; Vargas, H.A.; Schuit, R.C.; Windhorst, A.D.; Eertwegh, A.J.V.D.; Van Der Veldt, A.A.; Bergman, A.M.; Burnazi, E.M.; Lewis, J.S.; et al. Assessment of Simplified Methods for Quantification of 18F-FDHT Uptake in Patients with Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2019, 60, 1221–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cysouw, M.C.F.; Kramer, G.M.; Heijtel, D.; Schuit, R.C.; Morris, M.J.; Eertwegh, A.J.M.V.D.; Voortman, J.; Hoekstra, O.S.; Oprea-Lager, D.E.; Boellaard, R. Sensitivity of 18F-fluorodihydrotestosterone PET-CT to count statistics and reconstruction protocol in metastatic castration-resistant prostate cancer. EJNMMI Res. 2019, 9, 70. [Google Scholar] [CrossRef]
- Todorovic-Tirnanic, M.V.; Gajic, M.M.; Obradovic, V.B.; Baum, R.P. Gallium-68 DOTATOC PET/CT In Vivo Characterization of Somatostatin Receptor Expression in the Prostate. Cancer Biother. Radiopharm. 2014, 29, 108–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, S.; Reubi, J.C.; Kalkner, K.-M.; Laissue, J.A.; Horisberger, U.; Olerud, C.; Westlin, J.-E. Metastatic Hormone-Refractory Prostatic Adenocarcinoma Expresses Somatostatin Receptors and Is Visualized in Vivo by [€˜111n]-LabeledDTPA-D-[Phe’]-Octreotide Scintigraphy’. Cancer Res. 1995, 55, 5805s–5810s. [Google Scholar]
- Luboldt, W.; Zöphel, K.; Wunderlich, G.; Abramyuk, A.; Luboldt, H.-J.; Kotzerke, J. Visualization of Somatostatin Receptors in Prostate Cancer and its Bone Metastases with Ga-68–DOTATOC PET/CT. Mol. Imaging Biol. 2009, 12, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Gofrit, O.N.; Frank, S.; Meirovitz, A.; Nechushtan, H.; Orevi, M. PET/CT with 68Ga-DOTA-TATE for Diagnosis of Neuroendocrine: Differentiation in Patients With Castrate-Resistant Prostate Cancer. Clin. Nucl. Med. 2017, 42, 1–6. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, G.; García Fontes, M.; Engler, H.; Alonso, O. Comparación intraindividual de la PET/TC con 68Ga-DOTATATE vs. PET/TC con 11C-colina en pacientes con cáncer de próstata en recaída bioquímica: Evaluación in vivo de la expresión de receptores de la somatostatina. Rev. Esp. De Med. Nucl. E Imagen Mol. 2019, 38, 29–37. [Google Scholar] [CrossRef]
- Iravani, A.; Mitchell, C.; Akhurst, T.; Sandhu, S.; Hofman, M.S.; Hicks, R.J. Molecular Imaging of Neuroendocrine Differentiation of Prostate Cancer: A Case Series. Clin. Genitourin. Cancer 2021, 19, e200–e205. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Skovgaard, D.; Brandt-Larsen, M.; Christensen, C.; Madsen, J.; Nielsen, C.H.; Thurison, T.; Klausen, T.L.; Holm, S.; Loft, A.; et al. First-in-human uPAR PET: Imaging of Cancer Aggressiveness. Theranostics 2015, 5, 1303–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skovgaard, D.; Persson, M.; Brandt-Larsen, M.; Christensen, C.; Madsen, J.; Klausen, T.L.; Holm, S.; Andersen, F.L.; Loft, A.; Berthelsen, A.K.; et al. Safety, Dosimetry, and Tumor Detection Ability of 68Ga-NOTA-AE105: First-in-Human Study of a Novel Radioligand for uPAR PET Imaging. J. Nucl. Med. 2016, 58, 379–386. [Google Scholar] [CrossRef] [Green Version]
- Fosbøl, M.; Kurbegovic, S.; Johannesen, H.H.; Røder, M.A.; Hansen, A.E.; Mortensen, J.; Loft, A.; Petersen, P.M.; Madsen, J.; Brasso, K.; et al. Urokinase-Type Plasminogen Activator Receptor (uPAR) PET/MRI of Prostate Cancer for Noninvasive Evaluation of Aggressiveness: Comparison with Gleason Score in a Prospective Phase 2 Clinical Trial. J. Nucl. Med. 2020, 62, 354–359. [Google Scholar] [CrossRef]
- Fosbøl, M.; Mortensen, J.; Petersen, P.; Loft, A.; Madsen, J.; Kjaer, A. uPAR PET/CT for Prognostication and Response Assessment in Patients with Metastatic Castration-Resistant Prostate Cancer Undergoing Radium-223 Therapy: A Prospective Phase II Study. Diagnostics 2021, 11, 1087. [Google Scholar] [CrossRef]
- Giesel, F.L.; Kratochwil, C.; Lindner, T.; Marschalek, M.M.; Loktev, A.; Lehnert, W.; Debus, J.; Jäger, D.; Flechsig, P.; Altmann, A.; et al. 68Ga-FAPI PET/CT: Biodistribution and Preliminary Dosimetry Estimate of 2 DOTA-Containing FAP-Targeting Agents in Patients with Various Cancers. J. Nucl. Med. 2018, 60, 386–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Beer, A.J.; Schwarzenböck, S.M.; Zantl, N.; Souvatzoglou, M.; Maurer, T.; Watzlowik, P.; Kessler, H.; Wester, H.-J.; Schwaiger, M.; Krause, B.J. Non-invasive assessment of inter-and intrapatient variability of integrin expression in metastasized prostate cancer by PET. Oncotarget 2016, 7, 28151–28159. [Google Scholar] [CrossRef] [PubMed]
- Ananias, H.J.; Heuvel, M.C.V.D.; Helfrich, W.; de Jong, I.J. Expression of the gastrin-releasing peptide receptor, the prostate stem cell antigen and the prostate-specific membrane antigen in lymph node and bone metastases of prostate cancer. Prostate 2009, 69, 1101–1108. [Google Scholar] [CrossRef]
- Anastasi, A.; Erspamer, V.; Bucci, M. Isolation and Structure of Bombesin and Alytesin, 2 Analogous Active Peptides from the Skin of the European Amphibians Bombina and Alytes. Experientia 1971, 27, 166–167. [Google Scholar] [CrossRef]
- Benya, R.V.; Kusui, T.; Pradhan, T.K.; Battey, J.F.; Jensen, R.T. Expression and characterization of cloned human bombesin receptors. Mol. Pharmacol. 1995, 47, 10–20. [Google Scholar] [PubMed]
- Van de Wiele, C.; Dumont, F.; van Belle, S.; Slegers, G.; Peers, S.H.; Dierckx, R.A. Is There a Role for Agonist Gastrin-Releasing Peptide Receptor Radioligands in Tumour Imaging? Nucl. Med. Commun. 2001, 22, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Cescato, R.; Maina, T.; Nock, B.; Nikolopoulou, A.; Charalambidis, D.; Piccand, V.; Reubi, J.C. Bombesin Receptor Antagonists May Be Preferable to Agonists for Tumor Targeting. J. Nucl. Med. 2008, 49, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beer, M.; Montani, M.; Gerhardt, J.; Wild, P.J.; Hany, T.F.; Hermanns, T.; Müntener, M.; Kristiansen, G. Profiling gastrin-releasing peptide receptor in prostate tissues: Clinical implications and molecular correlates. Prostate 2011, 72, 318–325. [Google Scholar] [CrossRef]
- Porter, B.; Ortiz, M.A.; Bratslavsky, G.; Kotula, L. Structure and Function of the Nuclear Receptor Superfamily and Current Targeted Therapies of Prostate Cancer. Cancers 2019, 11, 1852. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Ye, Z.; Wang, F.; Qin, Y.; Xu, X.; Yu, X.; Ji, S. Role of Somatostatin Receptor in Pancreatic Neuroendocrine Tumor Development, Diagnosis, and Therapy. Front. Endocrinol. 2021, 12, 537. [Google Scholar] [CrossRef]
- Jansen, K.; Heirbaut, L.; Cheng, J.D.; Joossens, J.; Ryabtsova, O.; Cos, P.; Maes, L.; Lambeir, A.-M.; De Meester, I.; Augustyns, K.; et al. Selective Inhibitors of Fibroblast Activation Protein (FAP) with a (4-Quinolinoyl)-glycyl-2-cyanopyrrolidine Scaffold. ACS Med. Chem. Lett. 2013, 4, 491–496. [Google Scholar] [CrossRef]
- Zi, F.; He, J.; He, D.; Li, Y.; Yang, L.; Cai, Z. Fibroblast activation protein α in tumor microenvironment: Recent progression and implications (Review). Mol. Med. Rep. 2015, 11, 3203–3211. [Google Scholar] [CrossRef] [Green Version]
- Kesch, C.; Yirga, L.; Dendl, K.; Handke, A.; Darr, C.; Krafft, U.; Radtke, J.P.; Tschirdewahn, S.; Szarvas, T.; Fazli, L.; et al. High fibroblast-activation-protein expression in castration-resistant prostate cancer supports the use of FAPI-molecular theranostics. Eur. J. Nucl. Med. Mol. Imaging 2021. [Google Scholar] [CrossRef]
- Campbell, I.D.; Humphries, M.J. Integrin Structure, Activation, and Interactions. Cold Spring Harb. Perspect. Biol. 2011, 3, a004994. [Google Scholar] [CrossRef] [Green Version]
- Zheng, D.Q.; Woodard, A.S.; Fornaro, M.; Tallini, G.; Languino, L.R. Prostatic carcinoma cell migration via alpha(v)beta3 integrin is modulated by a focal adhesion kinase pathway. Cancer Res. 1999, 59, 1655–1664. [Google Scholar]
- Baum, R.P.; Schuchardt, C.; Singh, A.; Chantadisai, M.; Robiller, F.C.; Zhang, J.; Mueller, D.; Eismant, A.; Almaguel, F.; Zboralski, D.; et al. Feasibility, Biodistribution and Preliminary Dosimetry in Peptide-Targeted Radionuclide Therapy (PTRT) of Diverse Adenocarcinomas using 177Lu-FAP-2286: First-in-Human Results. J. Nucl. Med. 2021, 62. [Google Scholar] [CrossRef]
- Alzubi, J.; Dettmer-Monaco, V.; Kuehle, J.; Thorausch, N.; Seidl, M.; Taromi, S.; Schamel, W.; Zeiser, R.; Abken, H.; Cathomen, T.; et al. PSMA-Directed CAR T Cells Combined with Low-Dose Docetaxel Treatment Induce Tumor Regression in a Prostate Cancer Xenograft Model. Mol. Ther.-Oncolytics 2020, 18, 226–235. [Google Scholar] [CrossRef]

{kind=link}
| Author Year | Peptide Radionuclide | n | Clinical Context | Positivity Rate | Se | Sp | Acc |
|---|---|---|---|---|---|---|---|
| Kähkonen et al. 2013 [15] | RM2 Gallium-68 | 14 | Primary staging = 11 Recurrence = 3 | 48% | T = 89% N = 67% | T = 81% | T = 83% |
| Wieser et al. 2014 [16] | CB-TE2A-AR06 Copper-64 | 4 | Primary staging = 4 | 75% | Ns | Ns | Ns |
| Sah et al. 2015 [17] | BAY 864367 Fluorine-18 | 10 | Primary staging = 5 Recurrence = 5 | 50% | Ns | Ns | Ns |
| Maina et al. 2016 [18] | SB3 Gallium-68 | 9 | Metastatic = 9 | 55% | Ns | Ns | Ns |
| Minamimoto et al. 2016 [19] | RM2 Gallium-68 | 7 | Recurrence = 7 | 86% | Ns | Ns | Ns |
| Nock et al. 2017 [20] | NeoBOMB1 Gallium-68 | 4 | Ns | Ns | Ns | Ns | Ns |
| Wieser et al. 2017 [21] | RM2 Gallium-68 | 16 | Recurrence = 16 | 63% | Ns | Ns | Ns |
| Minamimoto et al. 2018 [22] | RM2 Gallium-68 | 32 | Recurrence = 32 | 72% | Ns | Ns | Ns |
| Zhang et al. 2018 [23] | RM26 Gallium-68 | 28 | Primary staging = 17 Recurrence = 11 | 82% | Ns | Ns | Ns |
| Gnesin et al. 2018 [24] | MJ9 Gallium-68 | 5 | Recurrence = 5 | Ns | Ns | Ns | Ns |
| Fassbender et al. 2019 [25] | RM2 Gallium-68 | 15 | Primary staging = 15 | 93% | 69% | 63% | |
| Touijer et al. 2019 [26] | RM2 Gallium-68 | 16 | Primary staging = 16 | 100% | 85% | 67% | 79% |
| Hoberück et al. 2019 [27] | RM2 Gallium-68 | 16 | Primary staging = 2 Recurrence = 12 Other = 2 | 31% | Ns | Ns | Ns |
| Fassbender et al. 2020 [28] | RM2 Gallium-68 | 8 | Primary staging = 8 | Ns | Ns | Ns | Ns |
| Bakker et al. 2021 [29] | SB3 Gallium-68 | 10 | Primary staging = 10 | 80% | 88% | 88% | Ns |
| Baratto et al. 2021 [30] | RM2 Gallium-68 | 50 | Recurrence = 50 | 70% | Ns | Ns | Ns |
| Author | n | Population | Positivity Rate | |
|---|---|---|---|---|
| Year | Patient-Level | Lesion-Level | ||
| Larson et al. 2004 [34] | 7 | mCRPC | 100% | 97% |
| Zanzonico et al. 2004 [35] | 7 | Recurrence | Ns | Ns |
| Dehdashti et al. 2005 [36] | 20 | Advanced PCa (8 mCRPC) | 63% | 59% |
| Beattie et al. 2010 [37] | 13 | mCRPC | Ns | Ns |
| Fox et al. 2011 [38] | 20 | mCRPC | Ns | Ns |
| Vargas et al. 2014 [39] | 38 | mCRPC | 74–95% | 44–55% |
| Fox et al. 2018 [40] | 133 | mCRPC | Ns | 87% |
| Vargas et al. 2018 [41] | 27 | mCRPC | Ns | Ns |
| Jansen et al. 2019 [42] | 27 | mCRPC | Ns | Ns |
| Kramer et al. 2019 [43] | 14 | mCRPC | Ns | Ns |
| Cysouw et al. 2019 [44] | 14 | mCRPC | Ns | Ns |
| NCT Number | Category Type | Peptide Radionuclide | Phase | Population Number of Planned Patients | Endpoints |
|---|---|---|---|---|---|
| NCT04264208 | GRPR Imaging | RM2 Gallium-68 | 2 | PCa patients scheduled for HDR Brachytherapy n = 100 | Definition of [68Ga]Ga-RM2 PET/MRI detection rate versus mpMRI Definition of [68Ga]Ga-RM2 PET/MRI ability to assess changes response to treatment Determination of progression-free survival |
| NCT03949517 | GRPR Imaging | RM2 Gallium-68 | 1/2 | PCa patients scheduled for HDR or HIFU n = 10 | Evaluation of PCa response to HIFU or HDR Therapy |
| NCT03809078 | GRPR Imaging | RM2 Gallium-68 | 2 | Suspected PCa n = 20 | Evaluation of [68Ga]Ga-RM2 PET/MRI for biopsy guidance in patients with suspected PCa |
| NCT03698370 | GRPR Imaging | NeoBOMB1 Gallium-68 | 2 | Recurrent PCa n = 50 | To evaluate gallium [68Ga]Ga-NeoBOMB1 PET/MRI for detection of recurrent PCa after initial definitive therapy |
| NCT03606837 | GRPR Imaging | RM2 Gallium-68 | 2 | PCa patients scheduled for prostatectomy n = 15 | Determination of uptake intensity assessed with median SUV |
| NCT03113617 | GRPR Imaging | RM2 Gallium-68 | 2 | PCa patients scheduled for prostatectomy n = 90 | Determination of [68Ga]Ga-RM2 PET/CT detection rate in intermediate and high-risk PCa patients prior to prostatectomy. |
| NCT02624518 | GRPR Imaging | RM2 Gallium-68 | 2/3 | Recurrent PCa n = 125 | Determination of [68Ga]Ga-RM2 PET/MRI detection rate in recurrent PCa after initial definitive therapy |
| NCT00588185 | Androgen receptor Imaging | FHDT Fluorine-18 | Ns | Progressive PCa n = 300 | Determination of the accumulation and biodistribution of FDHT in patients with progressive PCa |
| NCT04457232 | FAP Imaging | FAPi-46 Gallium-68 | 1 | Metastatic recurrent PCa n = 30 | Definition of the biodistribution of [68Ga]Ga-FAPi-46 in normal and cancer tissues of PCa patients |
| NCT04000776 | SSTR Imaging | Octreotate Gallium-68 | Ns | mCRPC patients n = 100 | Determination of the prevalence of mCPRC intrapatient intermetastasis polyclonality and neuroendocrine using PET/CT triple tracer PSMA/FDG/OCTREOTATE imaging and their eligibility for radioligand therapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gauthé, M.; Sargos, P.; Barret, E.; Fromont-Hankard, G.; Beauval, J.-B.; Brureau, L.; Créhange, G.; Renard-Penna, R.; Dariane, C.; Fiard, G.; et al. Potential Targets Other Than PSMA for Prostate Cancer Theranostics: A Systematic Review. J. Clin. Med. 2021, 10, 4909. https://doi.org/10.3390/jcm10214909
Gauthé M, Sargos P, Barret E, Fromont-Hankard G, Beauval J-B, Brureau L, Créhange G, Renard-Penna R, Dariane C, Fiard G, et al. Potential Targets Other Than PSMA for Prostate Cancer Theranostics: A Systematic Review. Journal of Clinical Medicine. 2021; 10(21):4909. https://doi.org/10.3390/jcm10214909
Chicago/Turabian StyleGauthé, Mathieu, Paul Sargos, Eric Barret, Gaëlle Fromont-Hankard, Jean-Baptiste Beauval, Laurent Brureau, Gilles Créhange, Raphaële Renard-Penna, Charles Dariane, Gaëlle Fiard, and et al. 2021. "Potential Targets Other Than PSMA for Prostate Cancer Theranostics: A Systematic Review" Journal of Clinical Medicine 10, no. 21: 4909. https://doi.org/10.3390/jcm10214909
APA StyleGauthé, M., Sargos, P., Barret, E., Fromont-Hankard, G., Beauval, J.-B., Brureau, L., Créhange, G., Renard-Penna, R., Dariane, C., Fiard, G., Mathieu, R., Roubaud, G., Ruffion, A., Rouprêt, M., Ploussard, G., & on behalf of the CC-AFU. (2021). Potential Targets Other Than PSMA for Prostate Cancer Theranostics: A Systematic Review. Journal of Clinical Medicine, 10(21), 4909. https://doi.org/10.3390/jcm10214909