
Influence of Pharyngeal Anaesthesia on Post-Bronchoscopic Coughing: A Prospective, Single Blinded, Multicentre Trial

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Intervention/Procedure
- S1
- Flexible bronchoscopy via flexible endotracheal tube with LAP
- S2
- Flexible bronchoscopy via flexible endotracheal tube without LAP
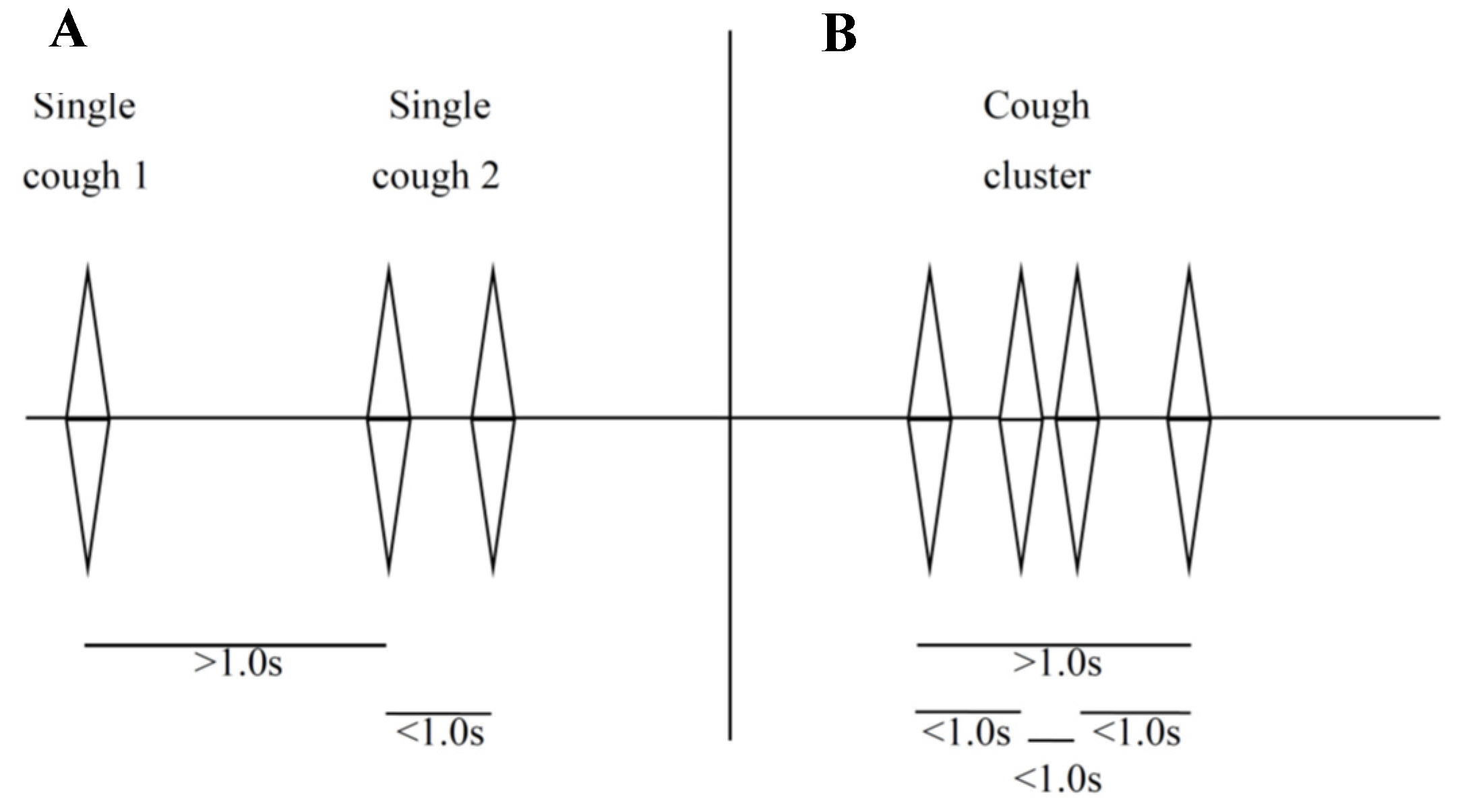
2.3. Cough Monitoring
2.4. Data Acquisition
2.5. Evaluation of Patient’s Tolerance and Comfort
2.6. Endpoints
2.7. Statistical Analysis
3. Results
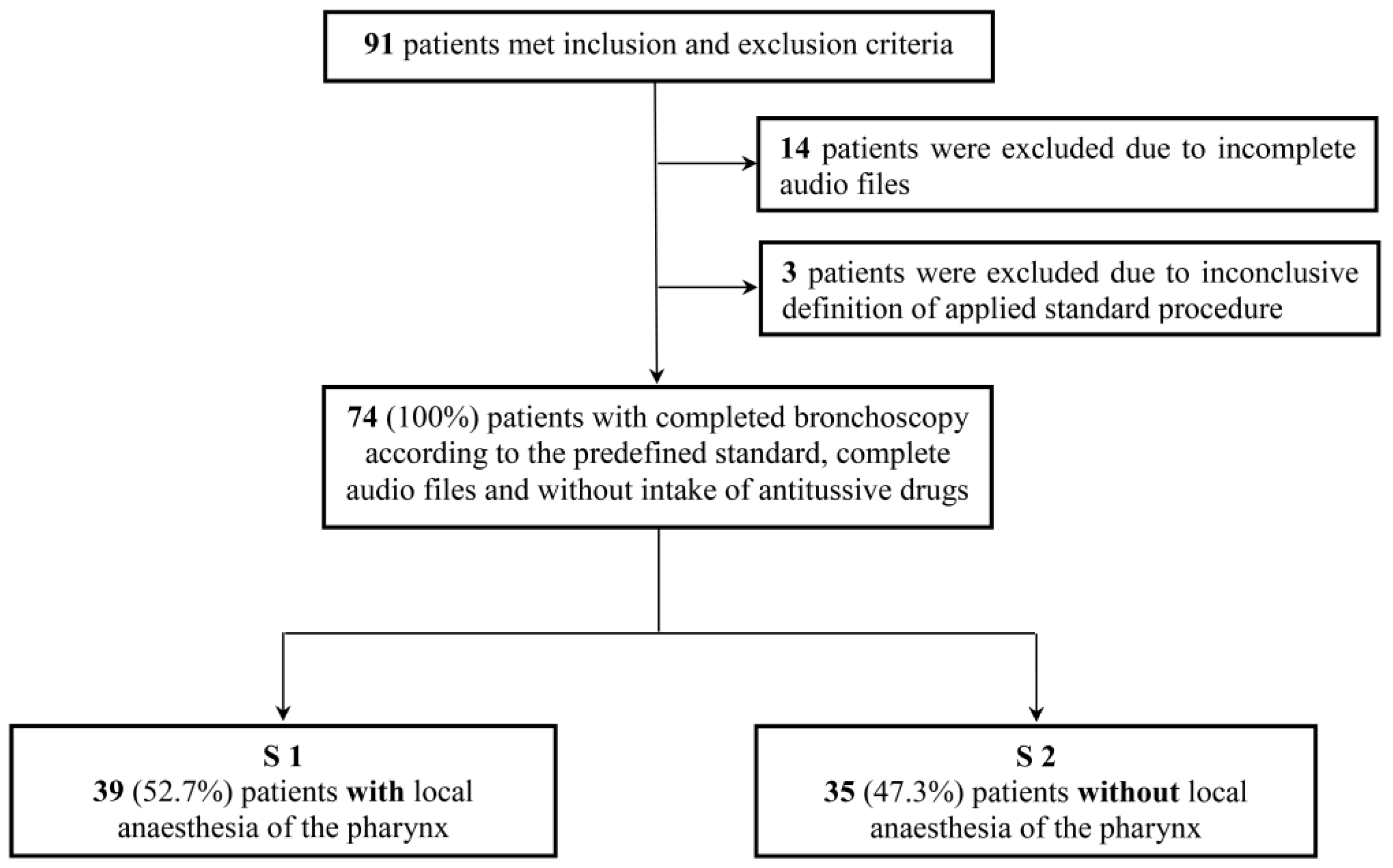
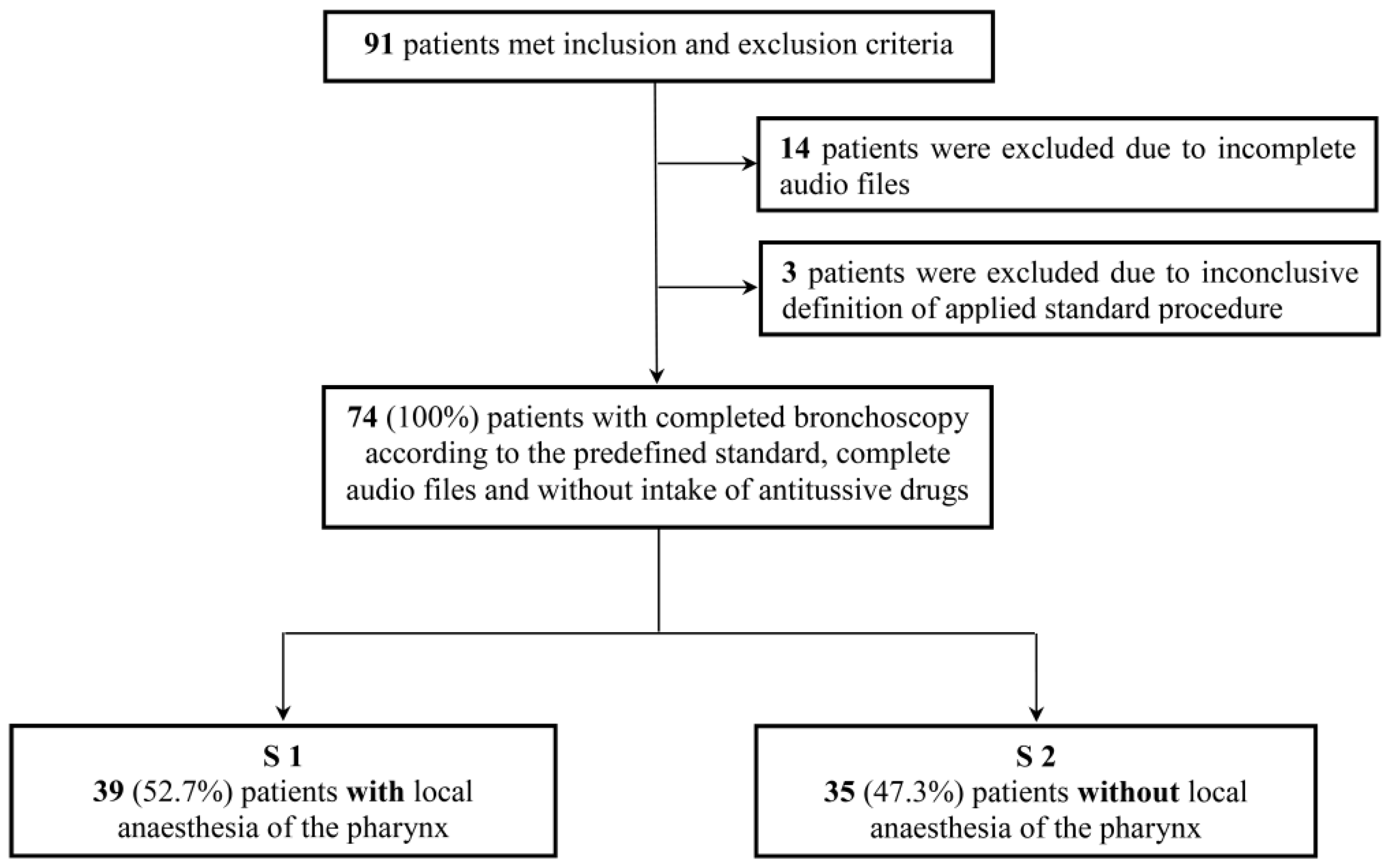
3.1. Study Population
3.2. Patient Characteristics
3.3. Bronchoscopic Procedure
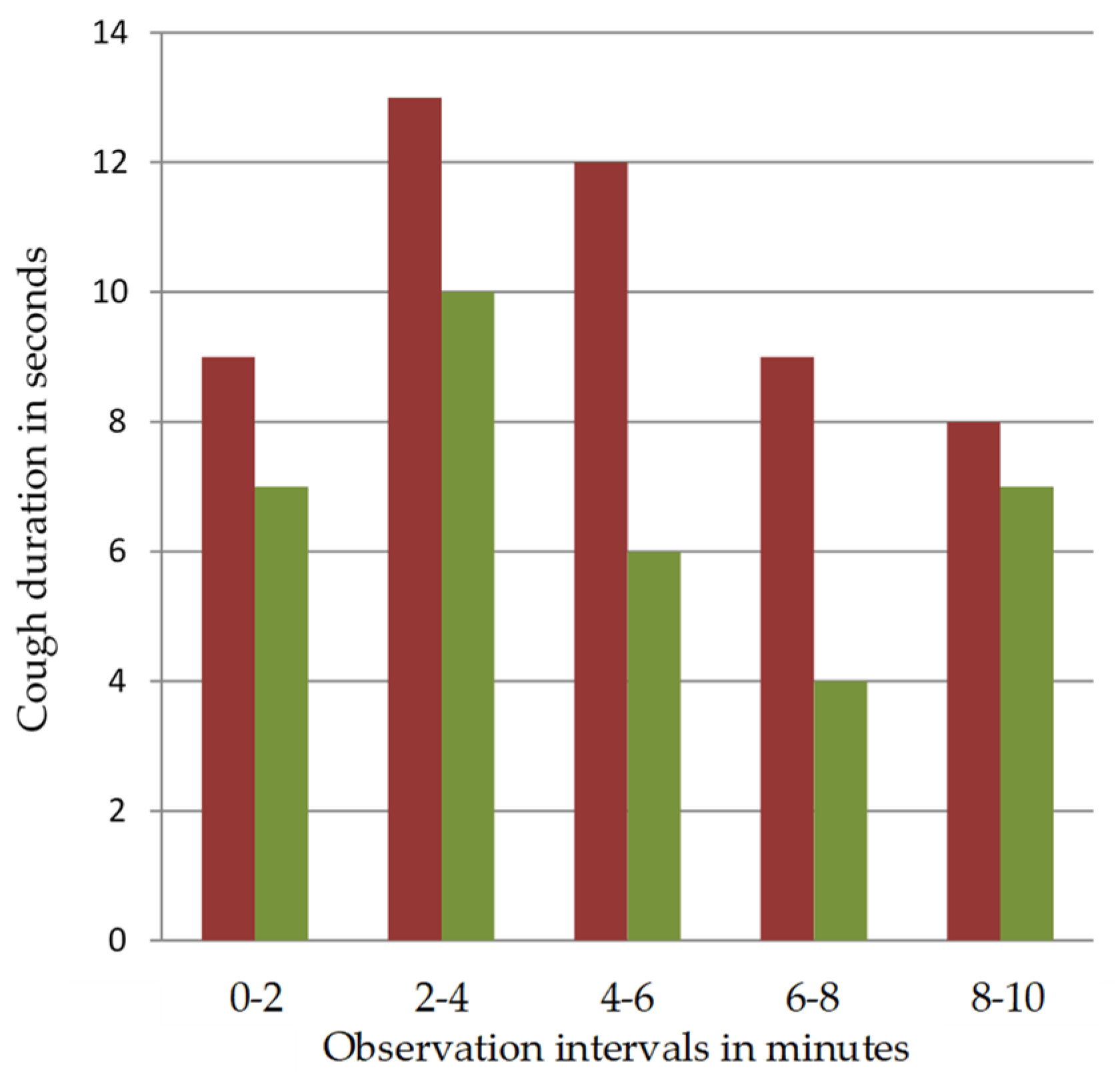
3.4. Cough Duration and Development
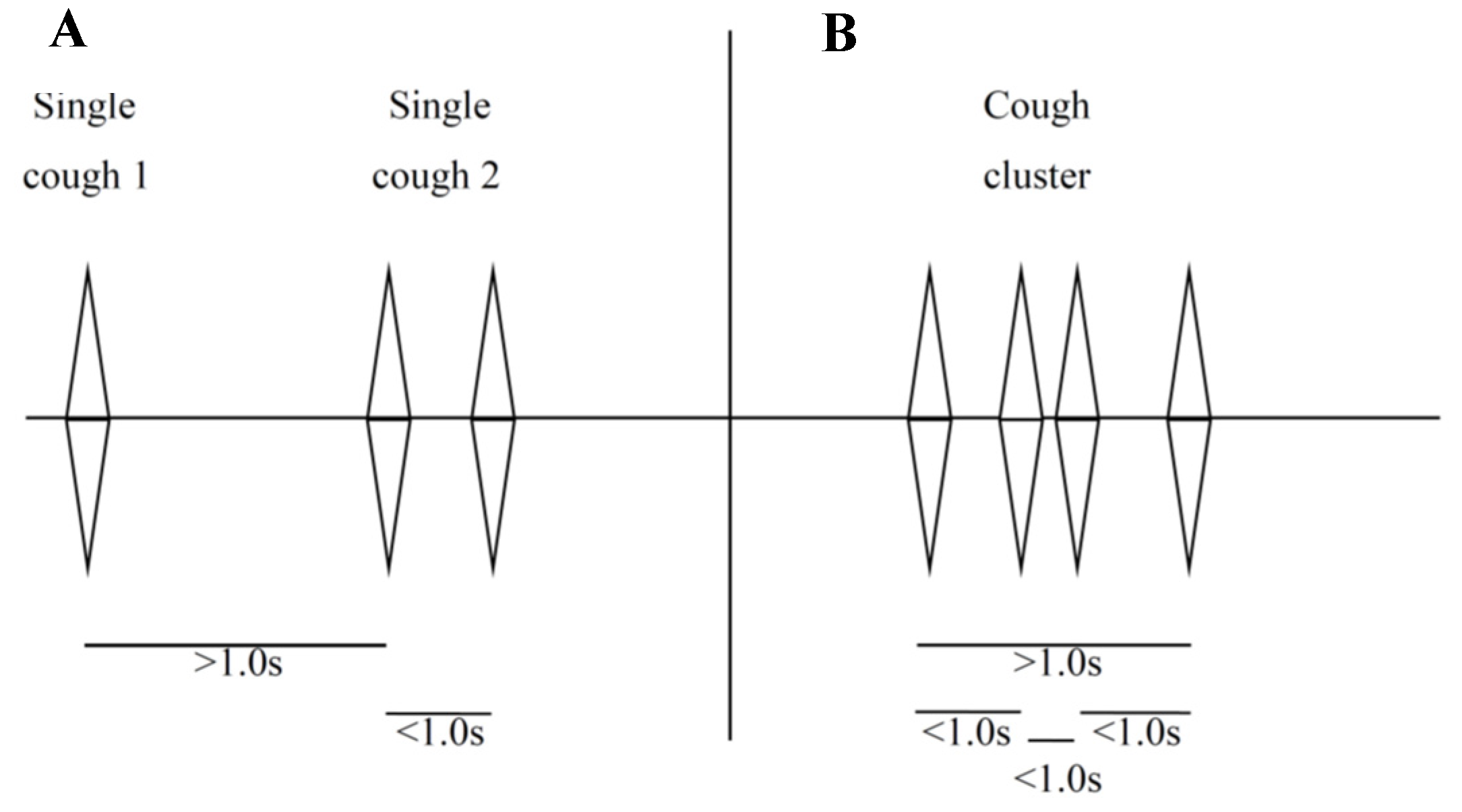
3.5. Single Coughs and Cough Clusters
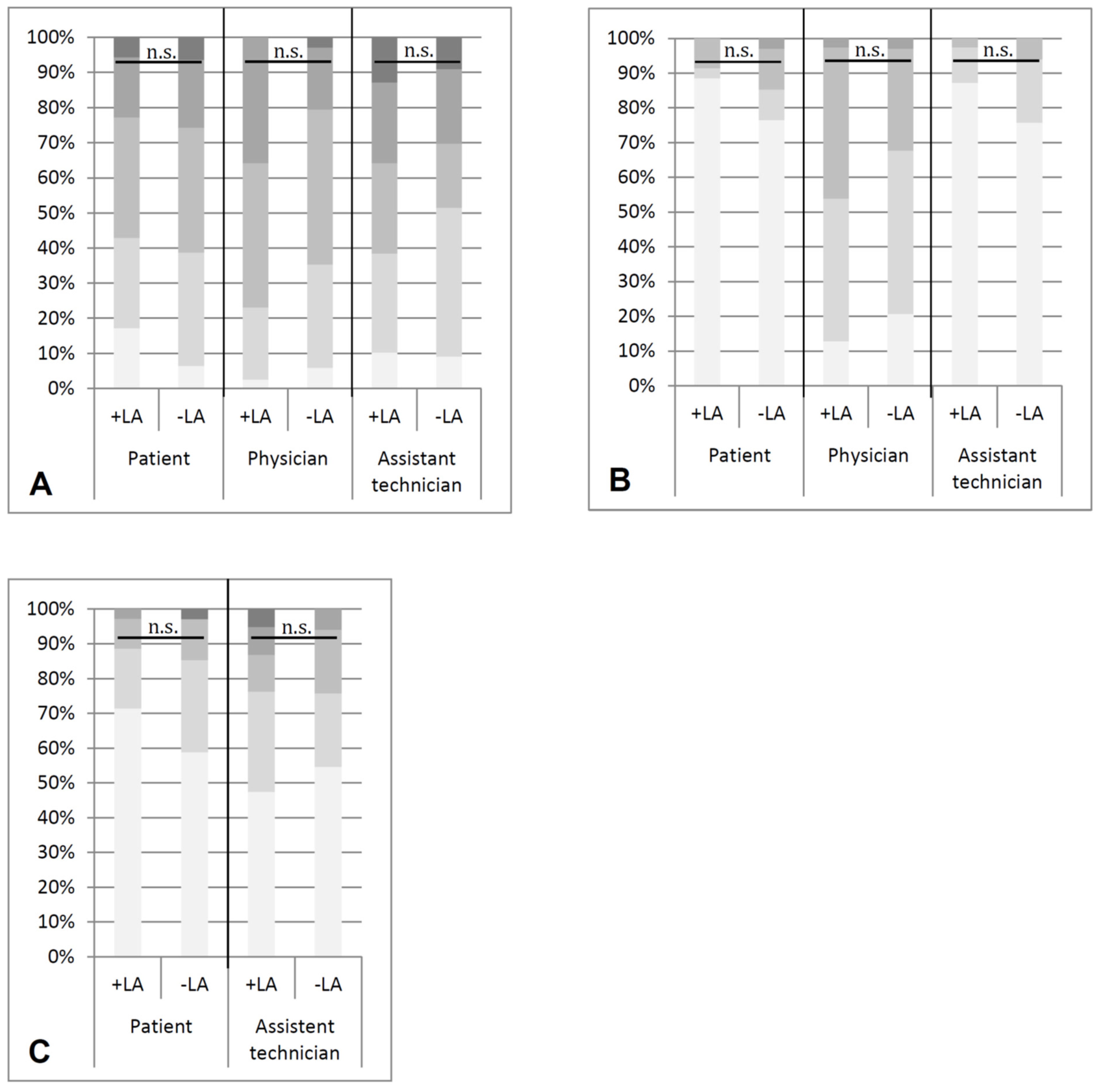
3.6. Patient’s Tolerance, Comfort and Complaints
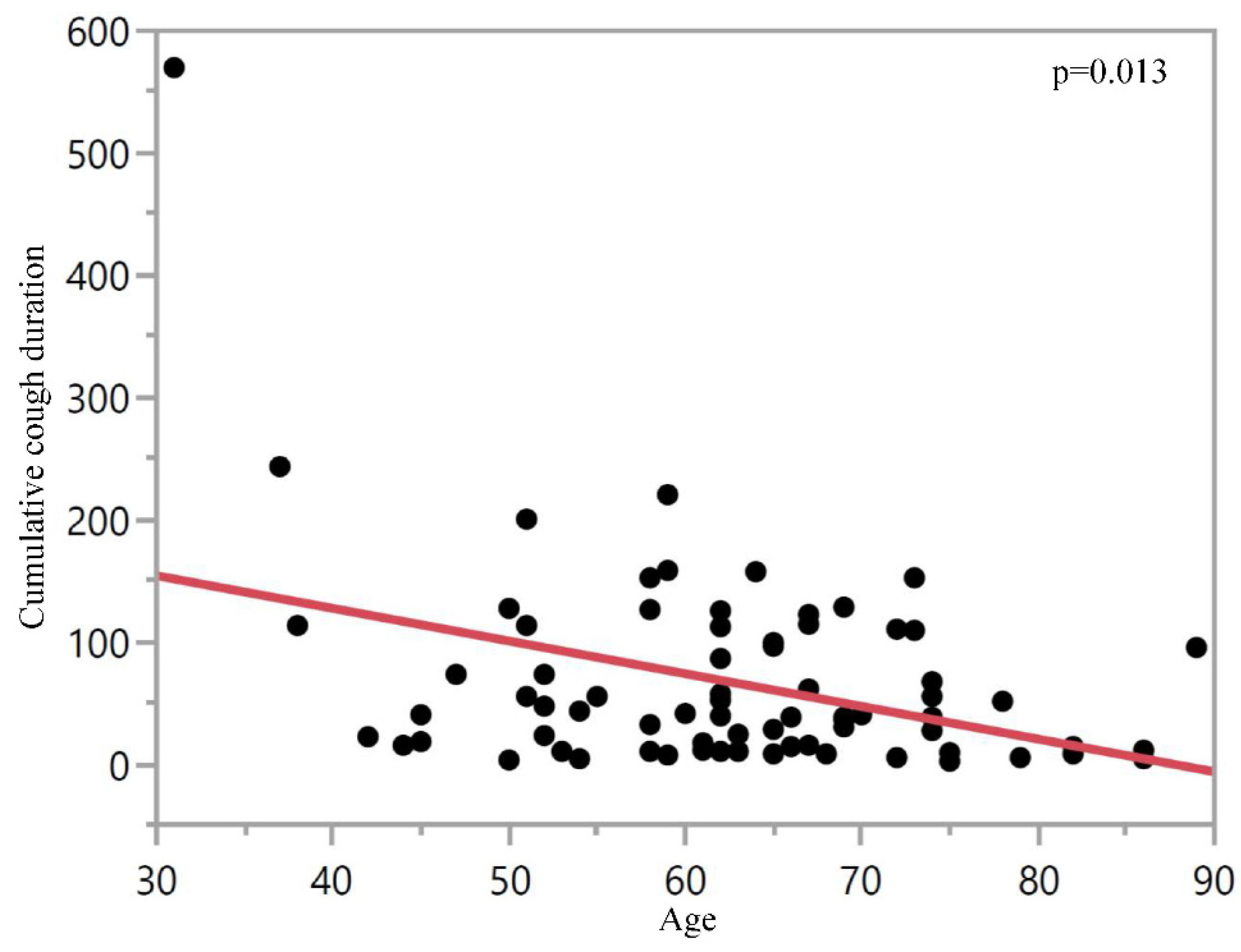
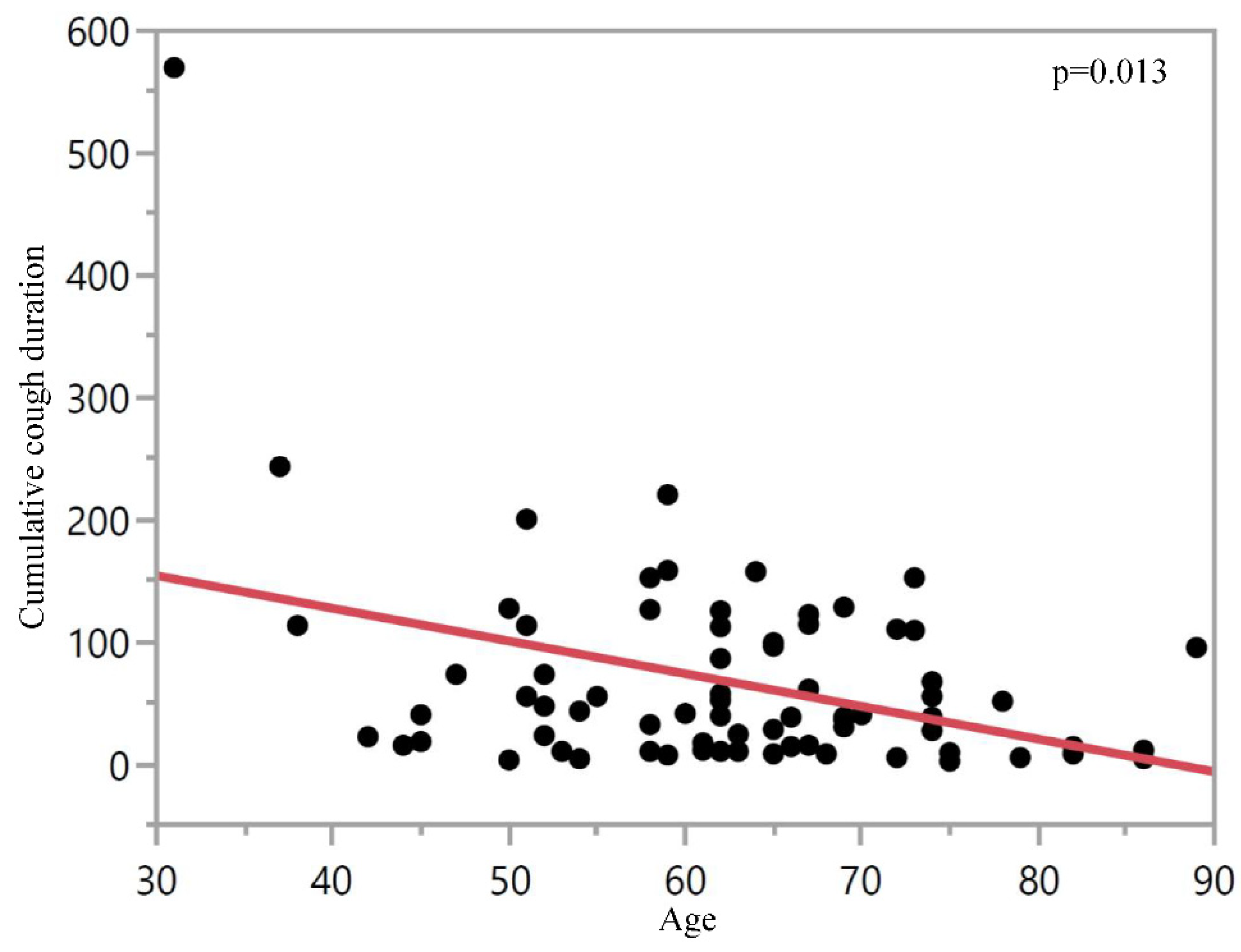
3.7. Coughing by Age
3.8. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence of Patient Assignment for Each Centre | |||
|---|---|---|---|
| Centre | Predefined Standard | Patients Received … | |
| S1 (+LAP) | S2 (−LAP) | ||
| 1 | S1 | 25 | 1 |
| S2 | 3 | 25 | |
| 2 | S2 | 0 | 8 |
| S1 | 11 | 1 | |
| 39 | 35 | ||
| Procedures, Sedation and Peri-interventional Monitoring * | ||||
|---|---|---|---|---|
| S1 (with LAP) | S2 (without LAP) | p-Value | ||
| N = 39 (100%) | N = 35 (100%) | |||
| Procedures—no. (%) | 38 1 | 34 1 | n.s. | |
| BL or BAL without additional procedure | 12 (31.6) | 12 (35.3) | ||
| BL or BAL + additional procedure | 19 (50.0) | 15 (44.1) | ||
| EBB/TBB | 13 (34.2) | 10 (29.4) | ||
| TBNA | 1 (2.6) | 3 (8.8) | ||
| EBB/TBB + TBNA | 5 (13.2) | 2 (5.9) | ||
| Others ° | 7 (18.4) | 7 (20.6) | ||
| Sedation with propofol—no. (%) | 39 (100) | 34 (100) 1 | ||
| Absolute dose of propofol—mg | 242.7 ± 140 | 261.5 ± 108.8 1 | n.s. | |
| Propofol dose/time—mg/min | 17.0 ± 9.7 1 | 17.4 ± 10.0 7 | n.s. | |
| Intubation yes—no. (%) | 36 (100) 3 | 31 (96.9) 3 | n.s. | |
| Duration of intervention—min | 17.9 ± 10.7 1 | 19.2 ± 11.7 6 | n.s. | |
| Peri-interventional monitoring | ||||
| MAP—mmHg | pre-interventional | 98.5 ± 2.3 | 102.4 ± 2.5 | n.s. |
| lowest | 79.8 ± 14.0 4 | 85.5 ± 16.1 5 | n.s. | |
| SpO2—% | pre-interventional | 94.8 ± 4.0 1 | 95.0 ± 4.2 | n.s. |
| lowest | 89.4 ± 6.1 | 86.0 ± 11.5 4 | n.s. | |
| Oxygen supply—l/min | 5.0 ± 1.3 1 | 5.3 ± 2.2 4 | n.s. | |
| Postinterventional monitoring | ||||
| MAP—mmHg | initial | 87.2 ± 2.7 | 85.0 ± 2.9 1 | n.s. |
| lowest | 78.6 ± 13.7 3 | 83.3 ± 14.2 14 | n.s. | |
| SpO2—% | initial | 93.3 ± 6.1 1 | 93.2 ± 4.9 1 | n.s. |
| lowest | 91.1 ± 0.9 2 | 92.0 ± 1.1 8 | n.s. | |
| Adverse Events * | |||
|---|---|---|---|
| S1 (with LAP) | S2 (without LAP) | p-Value | |
| n = 39 (100%) | n = 35 (100%) | ||
| AE during intervention—n (%) | n.s. | ||
| No | 39 (100) | 33 (94.3) | |
| Yes | 0 (0) | 2 (5.7) | |
| Desaturation | 0 (0) | 2 (5.7) | |
| AE post-interventional—n (%) | |||
| No | 24 (70.6) | 25 (83.3) | n.s. |
| Yes | 10 (29.4) | 5 (16.7) | |
| Heart rate > 100/min | 2 (5.9) | 0 (0) | |
| Dyspnea | 4 (11.8) | 2 (6.7) | |
| Bronchospasm | 0 (0) | 1 (3.3) | |
| Desaturation | 0 (0) | 1 (3.3) | |
| Hoarseness | 1 (2.9) | 0 (0) | |
| Shivering | 2 (5.9) | 0 (0) | |
| Headache | 0 (0) | 1 (3.3) | |
| Hearing impairment | 1 (2.9) | 0 (0) | |
References
- Ikeda, S.; Yanai, N.; Ishikawa, S. Flexible bronchofiberscope. Keio J. Med. 1968, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Pickles, J.; Jeffrey, M.; Datta, A.; Jeffrey, A.A. Is preparation for bronchoscopy optimal? Eur. Respir. J. 2003, 22, 203–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hautmann, H.; Eberhardt, R.; Heine, R.; Herth, F.; Hetzel, J.; Hetzel, M.; Reichle, G.; Schmidt, B.; Stanzel, F.; Wagner, M. Recommendations for sedation during flexible bronchoscopy. Pneumologie 2011, 65, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Du Rand, I.A.; Blaikley, J.; Booton, R.; Chaudhuri, N.; Gupta, V.; Khalid, S.; Mandal, S.; Martin, J.; Mills, J.; Navani, N.; et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: Accredited by NICE. Thorax 2013, 68 (Suppl. S1), i1–i44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, R.; De-La-Rosa-Ramirez, I.; Maldonado-Hernandez, A.; Dominguez-Cherit, G. Should patients undergoing a bronchoscopy be sedated? Acta Anaesthesiol. Scand. 2003, 47, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Hadzri, H.; Azarisman, S.; Fauzi, A.; Roslan, H.; Roslina, A.; Adina, A.; Fauzi, M. Can a bronchoscopist reliably assess a patient’s experience of bronchoscopy? JRSM Short Rep. 2010, 1, 35. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.; Durieux, M.E.; Marcus, M.A. Toxicity of local anaesthetics. Best Pract. Res. Clin. Anaesthesiol. 2003, 17, 111–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doumiri, M.; Moussaoui, A.; Maazouzi, W. Cardiac arrest after gargling and oral ingestion of 5% lidocaine. Can. J. Anaesth. J. Can. D’anesthesie 2008, 55, 882–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horacek, M.; Vymazal, T. Lidocaine not so innocent: Cardiotoxicity after topical anaesthesia for bronchoscopy. Indian J. Anaesth. 2012, 56, 95–96. [Google Scholar] [CrossRef]
- Peacock, A.J.; Benson-Mitchell, R.; Godfrey, R. Effect of fibreoptic bronchoscopy on pulmonary function. Thorax 1990, 45, 38–41. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.L.; Razzaghi, A.; Souney, P.F. Seizure after lidocaine for bronchoscopy: Case report and review of the use of lidocaine in airway anesthesia. Pharmacotherapy 1993, 13, 72–78. [Google Scholar] [PubMed]
- Hess, G.P.; Walson, P.D. Seizures secondary to oral viscous lidocaine. Ann. Emerg. Med. 1988, 17, 725–727. [Google Scholar] [CrossRef]
- Parish, R.C.; Moore, R.T.; Gotz, V.P. Seizures following oral lidocaine for esophageal anesthesia. Drug Intell. Clin. Pharm. 1985, 19, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Wolfram, W.; Rose, R. Toxicity--seizures in an infant caused by (or related to) oral viscous lidocaine use. J. Emerg. Med. 1992, 10, 587–590. [Google Scholar] [CrossRef]
- Karim, A.; Ahmed, S.; Siddiqui, R.; Mattana, J. Methemoglobinemia complicating topical lidocaine used during endoscopic procedures. Am. J. Med. 2001, 111, 150–153. [Google Scholar] [CrossRef]
- Crawford, O.B. Methemoglobin in man following the use of prilocaine. Acta Anaesthesiol. Scand. Suppl. 1965, 16, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, A.D.; Santamaria, J.D.; Nana, A. Patient comfort and plasma lignocaine concentrations during fibreoptic bronchoscopy. Anaesth. Intensive Care 1985, 13, 370–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruffles, S.P.; Gayres, J.G. Fatal bronchospasm after topical lignocaine before bronchoscopy. Br. Med. J. 1987, 294, 1658–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameer, B.; Burlingame, M.B.; Harman, E.M. Rapid mucosal absorption of topical lidocaine during bronchoscopy in the presence of oral candidiasis. Chest 1989, 96, 1438–1439. [Google Scholar] [CrossRef] [PubMed]
- Labedzki, L.; Ochs, H.R.; Abernethy, D.R.; Greenblatt, D.J. Potentially toxic serum lidocaine concentrations following spray anesthesia for bronchoscopy. Klin. Wochenschr. 1983, 61, 379–380. [Google Scholar] [CrossRef] [PubMed]
- Oni, G.; Brown, S.; Burrus, C.; Grant, L.; Watkins, J.; Kenkel, M.; Barton, F., Jr.; Kenkel, J. Effect of 4% topical lidocaine applied to the face on the serum levels of lidocaine and its metabolite, monoethylglycinexylidide. Aesthetic Surg. J. 2010, 30, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Gitman, M.; Barrington, M.J. Local Anesthetic Systemic Toxicity: A Review of Recent Case Reports and Registries. Reg. Anesth. Pain Med. 2018, 43, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Braid, D.P.; Scott, D.B. The Systemic Absorption of Local Analgesic Drugs. Br. J. Anaesth. 1965, 37, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Antoniades, N.; Worsnop, C. Topical lidocaine through the bronchoscope reduces cough rate during bronchoscopy. Respirology 2009, 14, 873–876. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.R.; Hay, J.G.; Clague, J.; Nisar, M.; Earis, J.E. Comparison of three different methods used to achieve local anesthesia for fiberoptic bronchoscopy. Chest 1992, 102, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Mendes de Leon, C.; Bezel, R.; Karrer, W.; Brandli, O. Premedication in fiber optic bronchoscopy from the patient’s and the physician’s viewpoint—A randomized study for the comparison of midazolam and hydrocodone. Schweiz. Med. Wochenschr. 1986, 116, 1267–1272. [Google Scholar] [PubMed]
- Augstkalns, I.; Bradshaw, E.G. The value of topical lignocaine for bronchoscopy under general anaesthesia. Anaesthesia 1977, 32, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Wahidi, M.M.; Jain, P.; Jantz, M.; Lee, P.; Mackensen, G.B.; Barbour, S.Y.; Lamb, C.; Silvestri, G.A. American College of Chest Physicians consensus statement on the use of topical anesthesia, analgesia, and sedation during flexible bronchoscopy in adult patients. Chest 2011, 140, 1342–1350. [Google Scholar] [CrossRef]
- Kirkpatrick, M.B. Lidocaine topical anesthesia for flexible bronchoscopy. Chest 1989, 96, 965–967. [Google Scholar] [CrossRef] [PubMed]
- Aviv, J.E.; Martin, J.H.; Jones, M.E.; Wee, T.A.; Diamond, B.; Keen, M.S.; Blitzer, A. Age-related changes in pharyngeal and supraglottic sensation. Ann. Otol. Rhinol. Laryngol. 1994, 103, 749–752. [Google Scholar] [PubMed]
- Aviv, J.E. Effects of aging on sensitivity of the pharyngeal and supraglottic areas. Am. J. Med. 1997, 103, 74s–76s. [Google Scholar] [CrossRef]
- Lowery, E.M.; Brubaker, A.L.; Kuhlmann, E.; Kovacs, E.J. The aging lung. Clin. Interv. Aging 2013, 8, 1489–1496. [Google Scholar] [PubMed] [Green Version]

| Baseline Characteristics * | |||
|---|---|---|---|
| S1 (with LAP) | S2 (without LAP) | p-Value | |
| Variable | N = 39 (100%) | N = 35 (100%) | |
| Age—years | 61.6 ± 11.4 | 63.7 ± 12.2 | n.s. |
| Sex—no. (%) ^ | |||
| Male | 13 (46.4) | 20 (76.9) | 0.02 |
| Female | 15 (53.6) | 6 (23.1) | |
| Body weight—kg | 71.5 ± 17.9 | 74.1 ± 12.7 | n.s. |
| Body height—cm | 169.5 ± 8.6 | 171.7 ± 9.5 | n.s. |
| Body mass index—kg/m2 | 24.8 ± 5.5 | 25.2 ± 4.1 | n.s. |
| Smoking status—no. (%) | |||
| Never smoker | 12 (30.8) | 7 (20.0) | 0.36 |
| Ever smoker | 27 (69.2) | 28 (80.0) | |
| Former smoker | 13 (33.3) | 17 (40.0) | |
| Current Smoker | 14 (35.9) | 11 (40.0) | |
| Preexisting lung disease—no. (%) | |||
| Yes | 31 (79.5) | 22 (62.9) | 0.11 |
| No | 8 (20.5) | 13 (37.1) | |
| Preexisting cardiac disease—no. (%) ^ | |||
| Yes | 8 (21.1) | 10 (29.4) | 0.41 |
| No | 30 (78.9) | 24 (70.6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Häntschel, M.; Zahn-Paulsen, M.; Ehab, A.; Böckeler, M.; Spengler, W.; Lewis, R.A.; Hautmann, H.; Hetzel, J. Influence of Pharyngeal Anaesthesia on Post-Bronchoscopic Coughing: A Prospective, Single Blinded, Multicentre Trial. J. Clin. Med. 2021, 10, 4773. https://doi.org/10.3390/jcm10204773
Häntschel M, Zahn-Paulsen M, Ehab A, Böckeler M, Spengler W, Lewis RA, Hautmann H, Hetzel J. Influence of Pharyngeal Anaesthesia on Post-Bronchoscopic Coughing: A Prospective, Single Blinded, Multicentre Trial. Journal of Clinical Medicine. 2021; 10(20):4773. https://doi.org/10.3390/jcm10204773
Chicago/Turabian StyleHäntschel, Maik, Mariella Zahn-Paulsen, Ahmed Ehab, Michael Böckeler, Werner Spengler, Richard A. Lewis, Hubert Hautmann, and Jürgen Hetzel. 2021. "Influence of Pharyngeal Anaesthesia on Post-Bronchoscopic Coughing: A Prospective, Single Blinded, Multicentre Trial" Journal of Clinical Medicine 10, no. 20: 4773. https://doi.org/10.3390/jcm10204773
APA StyleHäntschel, M., Zahn-Paulsen, M., Ehab, A., Böckeler, M., Spengler, W., Lewis, R. A., Hautmann, H., & Hetzel, J. (2021). Influence of Pharyngeal Anaesthesia on Post-Bronchoscopic Coughing: A Prospective, Single Blinded, Multicentre Trial. Journal of Clinical Medicine, 10(20), 4773. https://doi.org/10.3390/jcm10204773