
Catheter-Directed Therapies in Patients with Pulmonary Embolism: Predictive Factors of In-Hospital Mortality and Long-Term Follow-Up

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Variables and Outcome Measures
2.3. Catheter-Directed Therapy
2.4. Patients’ Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Clinical Baseline Characteristics at PE Presentation
3.2. Characteristics of Acute PE and Treatment
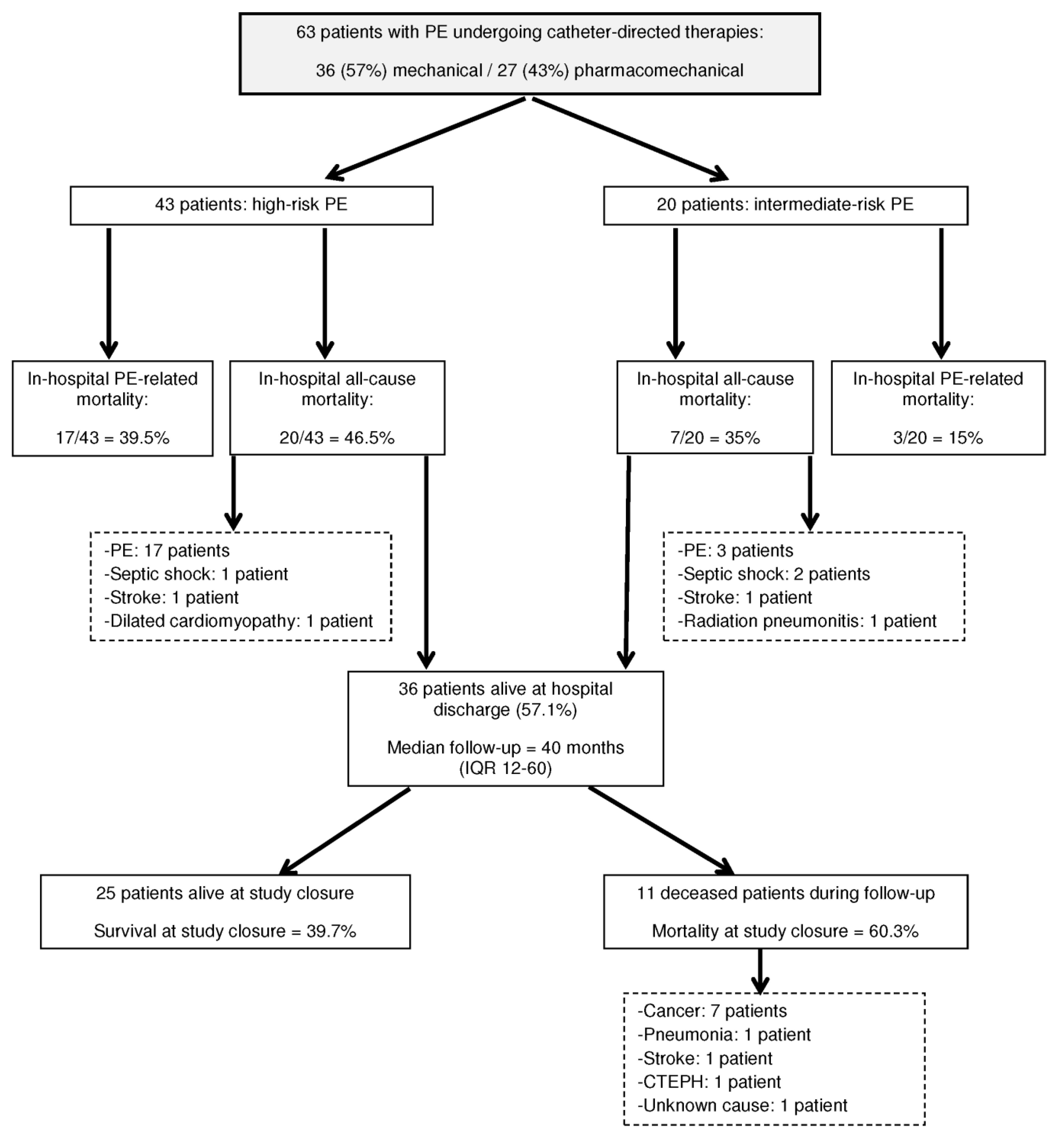
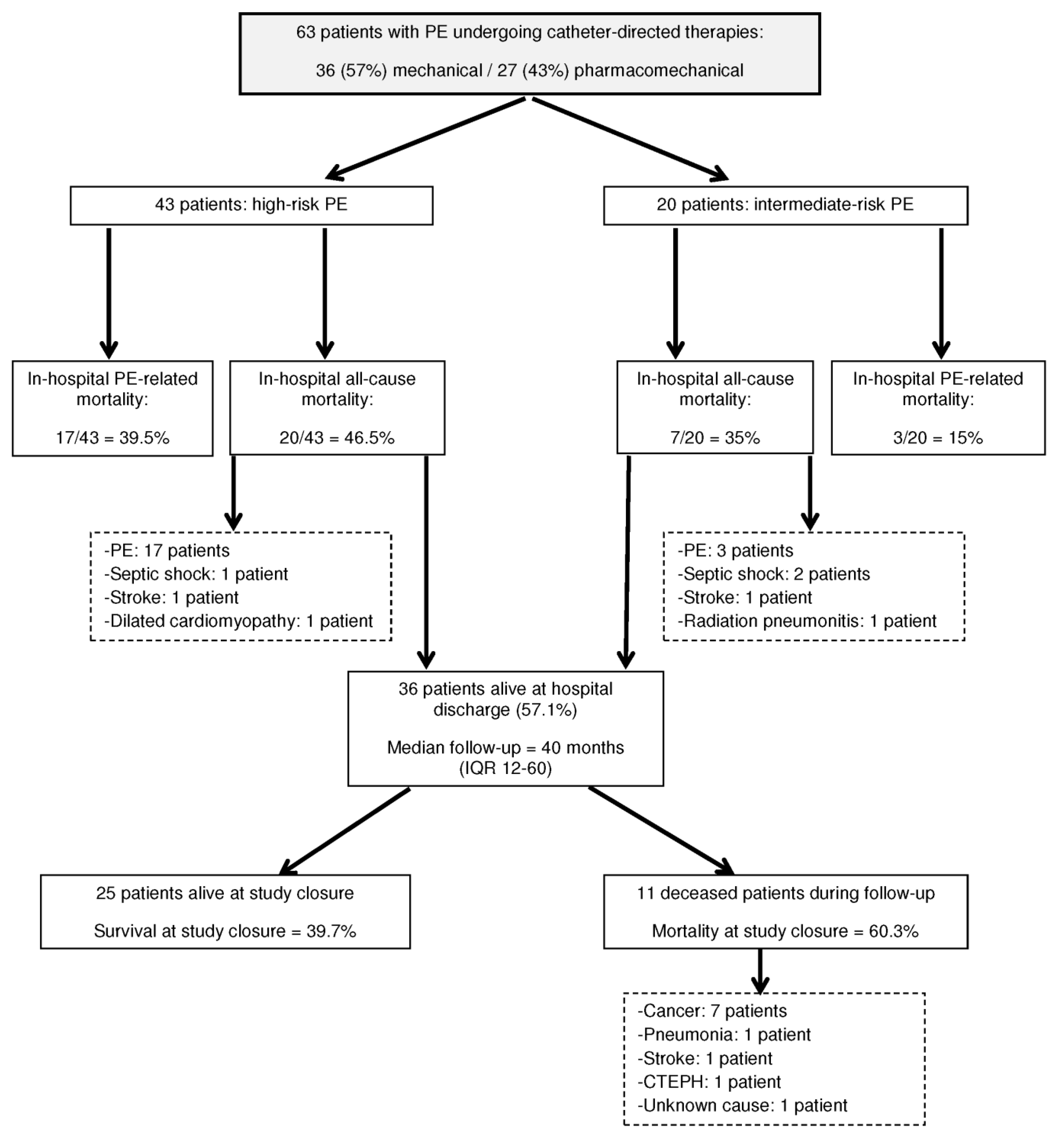
3.3. In-Hospital Outcomes
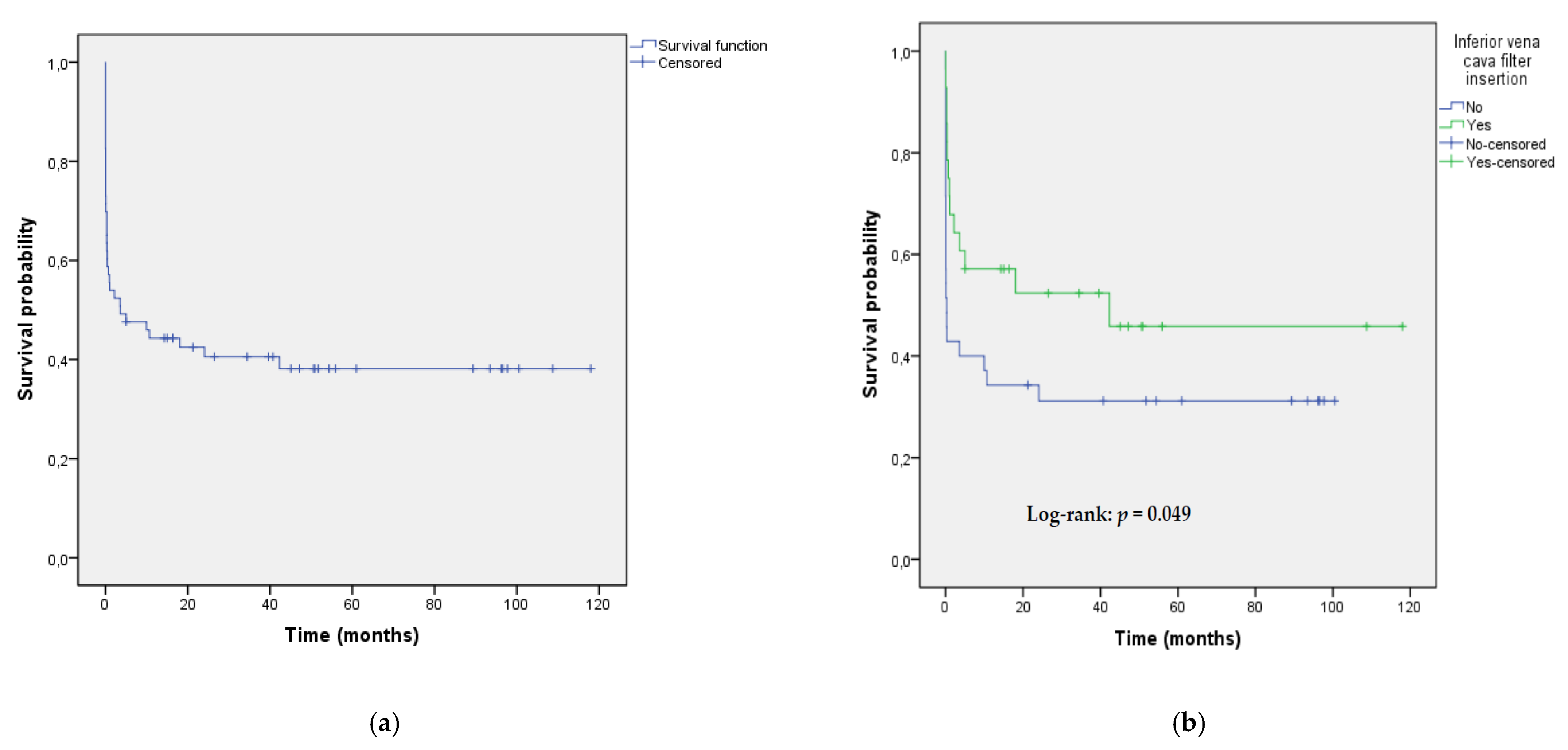
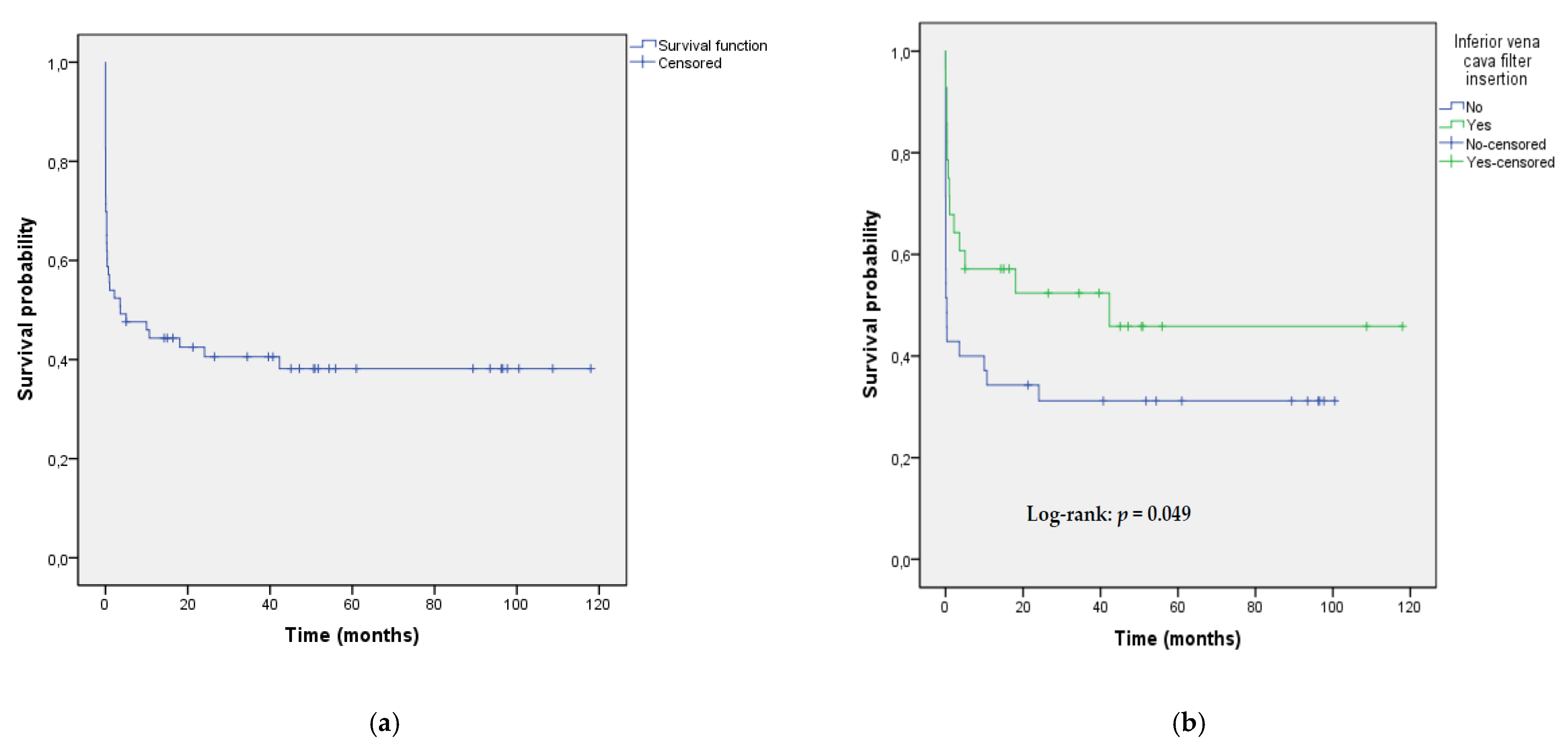
3.4. Long-Term Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Barco, S.; Mahmoudpour, S.H.; Valerio, L.; Klok, F.A.; Münzel, T.; Middeldorp, S.; Ageno, W.; Cohen, A.T.; Hunt, B.J.; Konstantinides, S.V. Trends in mortality related to pulmonary embolism in the European Region, 2000–2015: Analysis of vital registration data from the WHO Mortality Database. Lancet Respir. Med. 2020, 8, 277–287. [Google Scholar] [CrossRef]
- Goldhaber, S.Z.; Visani, L.; De Rosa, M. Acute pulmonary embolism: Clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 1999, 353, 1386–1389. [Google Scholar] [CrossRef]
- Jaff, M.R.; McMurtry, M.S.; Archer, S.L.; Cushman, M.; Goldenberg, N.; Goldhaber, S.Z.; Jenkins, J.S.; Kline, J.A.; Michaels, A.D.; Thistlethwaite, P.; et al. American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: A scientific statement from the American Heart Association. Circulation 2011, 123, 1788–1830. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Piazza, G.; Goldhaber, S.Z. Fibrinolysis for acute pulmonary embolism. Vasc. Med. 2010, 15, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Meyer, G.; Vicaut, E.; Danays, T.; Agnelli, G.; Becattini, C.; Beyer-Westendorf, J.; Bluhmki, E.; Bouvaist, H.; Brenner, B.; Couturaud, F.; et al. PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N. Engl. J. Med. 2014, 370, 1402–1411. [Google Scholar] [CrossRef] [PubMed]
- Riera-Mestre, A.; Becattini, C.; Giustozzi, M.; Agnelli, G. Thrombolysis in hemodynamically stable patients with acute pulmonary embolism: A meta-analysis. Thromb. Res. 2014, 134, 1265–1271. [Google Scholar] [CrossRef]
- Stein, P.D.; Matta, F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: Saves lives but underused. Am. J. Med. 2012, 125, 465–470. [Google Scholar] [CrossRef]
- Adusumalli, S.; Geller, B.J.; Yang, L.; Giri, J.; Groeneveld, P.W. Trends in catheter-directed thrombolysis and systemic thrombolysis for the treatment of pulmonary embolism. Am. Heart J. 2019, 207, 83–85. [Google Scholar] [CrossRef]
- Chatterjee, S.; Chakraborty, A.; Weinberg, I.; Kadakia, M.; Wilensky, R.L.; Sardar, P.; Kumbhani, D.J.; Mukherjee, D.; Jaff, M.R.; Giri, J. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: A meta-analysis. JAMA 2014, 311, 2414–2421. [Google Scholar] [CrossRef]
- Kuo, W.T.; Sista, A.K.; Faintuch, S.; Dariushnia, S.R.; Baerlocher, M.O.; Lookstein, R.A.; Haskal, Z.J.; Nikolic, B.; Gemmete, J.J. Society of Interventional Radiology Position Statement on Catheter-Directed Therapy for Acute Pulmonary Embolism. J. Vasc. Interv. Radiol. 2018, 29, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Giri, J.; Sista, A.K.; Weinberg, I.; Kearon, C.; Kumbhani, D.J.; Desai, N.D.; Piazza, G.; Gladwin, M.T.; Chatterjee, S.; Kobayashi, T.; et al. Interventional Therapies for Acute Pulmonary Embolism: Current Status and Principles for the Development of Novel Evidence: A Scientific Statement From the American Heart Association. Circulation 2019, 140, e774–e801. [Google Scholar] [CrossRef]
- Mostafa, A.; Briasoulis, A.; Telila, T.; Belgrave, K.; Grines, C. Treatment of Massive or Submassive Acute Pulmonary Embolism With Catheter-Directed Thrombolysis. Am. J. Cardiol. 2016, 117, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Kuo, W.T.; Banerjee, A.; Kim, P.S.; DeMarco, F.J., Jr.; Levy, J.R.; Facchini, F.R.; Unver, K.; Bertini, M.J.; Sista, A.K.; Hall, M.J.; et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest 2015, 148, 667–673. [Google Scholar] [CrossRef]
- Avgerinos, E.D.; Abou Ali, A.N.; Liang, N.L.; Rivera-Lebron, B.; Toma, C.; Maholic, R.; Makaroun, M.S.; Chaer, R.A. Catheter-directed interventions compared with systemic thrombolysis achieve improved ventricular function recovery at a potentially lower complication rate for acute pulmonary embolism. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Tu, T.; Toma, C.; Tapson, V.F.; Adams, C.; Jaber, W.A.; Silver, M.; Khandhar, S.; Amin, R.; Weinberg, M.; Engelhardt, T.; et al. A Prospective, Single-Arm, Multicenter Trial of Catheter-Directed Mechanical Thrombectomy for Intermediate-Risk Acute Pulmonary Embolism: The FLARE Study. JACC. Cardiovasc. Interv. 2019, 12, 859–869. [Google Scholar] [CrossRef]
- Ciampi-Dopazo, J.J.; Romeu-Prieto, J.M.; Sánchez-Casado, M.; Romerosa, B.; Canabal, A.; Rodríguez-Blanco, M.L.; Lanciego, C. Aspiration Thrombectomy for Treatment of Acute Massive and Submassive Pulmonary Embolism: Initial Single-Center Prospective Experience. J. Vasc. Interv. Radiol. 2018, 29, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Kucher, N.; Boekstegers, P.; Müller, O.J.; Kupatt, C.; Beyer-Westendorf, J.; Heitzer, T.; Tebbe, U.; Horstkotte, J.; Müller, R.; Blessing, E.; et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation 2014, 129, 479–486. [Google Scholar] [CrossRef] [Green Version]
- Engelberger, R.P.; Moschovitis, A.; Fahrni, J.; Willenberg, T.; Baumann, F.; Diehm, N.; Do, D.D.; Baumgartner, I.; Kucher, N. Fixed low-dose ultrasound-assisted catheter-directed thrombolysis for intermediate and high-risk pulmonary embolism. Eur. Heart J. 2015, 36, 597–604. [Google Scholar] [CrossRef] [Green Version]
- Piazza, G.; Hohlfelder, B.; Jaff, M.R.; Ouriel, K.; Engelhardt, T.C.; Sterling, K.M.; Jones, N.J.; Gurley, J.C.; Bhatheja, R.; Kennedy, R.J.; et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc. Interv. 2015, 8, 1382–1392. [Google Scholar] [CrossRef] [Green Version]
- Tapson, V.F.; Sterling, K.; Jones, N.; Elder, M.; Tripathy, U.; Brower, J.; Maholic, R.L.; Ross, C.B.; Natarajan, K.; Fong, P.; et al. A Randomized Trial of the Optimum Duration of Acoustic Pulse Thrombolysis Procedure in Acute Intermediate-Risk Pulmonary Embolism: The OPTALYSE PE Trial. JACC. Cardiovasc. Interv. 2018, 11, 1401–1410. [Google Scholar] [CrossRef] [PubMed]
- Tajima, H.; Ueda, T.; Mine, T.; Onozawa, S.; Murata, S. Late clinical outcomes of manual aspiration thrombectomy for a massive acute pulmonary thromboembolism. Jpn. J. Radiol. 2021, 39, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Gong, M.; Chen, G.; Zhao, B.; Kong, J.; Gu, J.; He, X. Rescue catheter-based therapies for the treatment of acute massive pulmonary embolism after unsuccessful systemic thrombolysis. J. Thromb. Thrombolysis 2021, 51, 805–813. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Qanadli, S.D.; El Hajjam, M.; Vieillard-Baron, A.; Joseph, T.; Mesurolle, B.; Oliva, V.L.; Barré, O.; Bruckert, F.; Dubourg, O.; Lacombe, P. New CT index to quantify arterial obstruction in pulmonary embolism: Comparison with angiographic index and echocardiography. Am. J. Roentgenol. 2001, 176, 1415–1420. [Google Scholar] [CrossRef]
- Jiménez, D.; Aujesky, D.; Moores, L.; Gómez, V.; Lobo, J.L.; Uresandi, F.; Otero, R.; Monreal, M.; Muriel, A.; Yusen, R.D.; et al. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch. Intern. Med. 2010, 170, 1383–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jara-Palomares, L.; Jiménez, D.; Bikdeli, B.; Muriel, A.; Rali, P.; Yamashita, Y.; Morimoto, T.; Kimura, T.; Le Mao, R.; Riera-Mestre, A.; et al. Derivation and validation of a clinical prediction rule for thrombolysis-associated major bleeding in patients with acute pulmonary embolism: The BACS score. Eur. Respir. J. 2020, 56, 2002336. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C.; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S.; Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Agnelli, G.; Lankeit, M.; Masotti, L.; Pruszczyk, P.; Casazza, F.; Vanni, S.; Nitti, C.; Kamphuisen, P.; Vedovati, M.C.; et al. Acute pulmonary embolism: Mortality prediction by the 2014 European Society of Cardiology risk stratification model. Eur. Respir. J. 2016, 48, 780–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becattini, C.; Giustozzi, M.; Cerdà, P.; Cimini, L.A.; Riera-Mestre, A.; Agnelli, G. Risk of recurrent venous thromboembolism after acute pulmonary embolism: Role of residual pulmonary obstruction and persistent right ventricular dysfunction. A meta-analysis. J. Thromb. Haemost. 2019, 17, 1217–1228. [Google Scholar] [CrossRef]
- Kuo, W.T.; Gould, M.K.; Louie, J.D.; Rosenberg, J.K.; Sze, D.Y.; Hofmann, L.V. Catheter-directed therapy for the treatment of massive pulmonary embolism: Systematic review and meta-analysis of modern techniques. J. Vasc. Interv. Radiol. 2009, 20, 1431–1440. [Google Scholar] [CrossRef] [PubMed]
- Laporte, S.; Mismetti, P.; Décousus, H.; Uresandi, F.; Otero, R.; Lobo, J.L.; Monreal, M.; RIETE Investigators. Clinical predictors for fatal pulmonary embolism in 15,520 patients with venous thromboembolism: Findings from the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) Registry. Circulation 2008, 117, 1711–1716. [Google Scholar] [CrossRef]
- Meneveau, N.; Séronde, M.F.; Blonde, M.C.; Legalery, P.; Didier-Petit, K.; Briand, F.; Caulfield, F.; Schiele, F.; Bernard, Y.; Bassand, J.P. Management of unsuccessful thrombolysis in acute massive pulmonary embolism. Chest 2006, 129, 1043–1050. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, J.A.; Barnes, G.D.; Chaer, R.A.; Cuschieri, J.; Eberhardt, R.T.; Johnson, M.S.; Kuo, W.T.; Murin, S.; Patel, S.; Rajasekhar, A.; et al. Society of Interventional Radiology Clinical Practice Guideline for Inferior Vena Cava Filters in the Treatment of Patients with Venous Thromboembolic Disease: Developed in collaboration with the American College of Cardiology, American College of Chest Physicians, American College of Surgeons Committee on Trauma, American Heart Association, Society for Vascular Surgery, and Society for Vascular Medicine. J. Vasc. Interv. Radiol. 2020, 31, 1529–1544. [Google Scholar] [CrossRef]
- De Gregorio, M.A.; Guirola, J.A.; Kuo, W.T.; Serrano, C.; Urbano, J.; Figueredo, A.L.; Sierre, S.; Quezada, C.A.; Barbero, E.; Jiménez, D. Catheter-directed aspiration thrombectomy and low-dose thrombolysis for patients with acute unstable pulmonary embolism: Prospective outcomes from a PE registry. Int. J. Cardiol. 2019, 287, 106–110. [Google Scholar] [CrossRef]
- Kucher, N.; Rossi, E.; De Rosa, M.; Goldhaber, S.Z. Massive pulmonary embolism. Circulation 2006, 113, 577–582. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Characteristics | Overall (n = 63) | High-Risk PE (n = 43) | Intermediate-Risk PE (n = 20) |
|---|---|---|---|
| Demographics | |||
| Age, mean (SD) | 60.2 (13.9) | 61.6 (14.5) | 57.3 (12.4) |
| Age > 70 years, n (%) | 14 (22.2%) | 12 (27.9%) | 2 (10%) |
| Male gender, n (%) | 32 (50.8%) | 22 (51.2%) | 10 (50%) |
| Underlying conditions | |||
| Arterial hypertension, n (%) | 22 (34.9%) | 15 (34.9%) | 7 (35%) |
| Diabetes, n (%) | 7 (11.1%) | 6 (14%) | 1 (5%) |
| Chronic heart disease, n (%) | 3 (4.8%) | 2 (4.7%) | 1 (5%) |
| Chronic lung disease, n (%) | 11 (17.5%) | 7 (16.3%) | 4 (20%) |
| Chronic renal failure, n (%) | 9 (14.3%) | 7 (16.3%) | 2 (10%) |
| Recent bleeding (<30 days), n (%) | 8 (12.7%) | 7 (16.3%) | 1 (5%) |
| Risk factors for VTE | |||
| Previous VTE, n (%) | 12 (19%) | 6 (14%) | 6 (30%) |
| Active cancer, n (%) | 16 (25.4%) | 10 (23.3%) | 6 (30%) |
| Recent surgery (<2 months), n (%) | 17 (27%) | 9 (20.9%) | 8 (40%) |
| Reasons for hospital admission, n (%) | |||
| PE | 45 (71.4%) | 31 (72%) | 14 (70%) |
| Stroke | 3 (4.8) | 3 (7%) | 0 (0%) |
| Medical conditions other than VTE | 6 (9.5%) | 3 (7%) | 3 (15%) |
| Surgical procedures | 6 (9.5%) | 3 (7%) | 3 (15%) |
| Polytrauma | 3 (4.8%) | 3 (7%) | 0 (0%) |
| Length of hospital stay (days), Median (IQR) | 13 (3–22) | 12 (1–21) | 13 (8–22) |
| Clinical presentation of PE, n (%) | |||
| Dyspnea ± chest pain | 30 (47.6%) | 20 (46.5%) | 10 (50%) |
| Syncope | 19 (30.2%) | 9 (20.9%) | 10 (50%) |
| Cardiac arrest | 14 (22.2%) | 14 (32.6%) | 0 (0%) |
| Characteristics | Overall (n = 63) | High-Risk PE (n = 43) | Intermediate-Risk PE (n = 20) |
|---|---|---|---|
| Simplified PESI Index ≥ 1, n (%) | 61 (96.8%) | 43 (100%) | 18 (90%) |
| Hemodynamic status | |||
| Systolic BP (mmHg), median (IQR) | 90 (80–120) | 82 (77–90) | 120 (108–125) |
| Heart rate (beats/min), median (IQR) | 114 (100–120) | 117 (97–126) | 112 (100–120) |
| Shock Index †, median (IQR) | 1.15 (0.93–1.41) | 1.33 (1.07–1.5) | 0.94 (0.82–1.1) |
| SpO2/FiO2 ratio, median (IQR) | 371 (231–429) | 371 (214–429) | 367 (253–438) |
| Residual DVT §, n (%) | 34 (72.3%) | 19 (63.3%) | 15 (88.2%) |
| D-dimer µg/L, median (IQR) | 5962 (3314–17,563) | 7106 (3259–38,563) | 5583 (3646–6160) |
| Positive troponin levels ‡, n (%) | 40 (76.9%) | 33 (91.7%) | 7 (43.8%) |
| CT features | |||
| Bilateral PE, n (%) | 61 (96.8%) | 42 (97.7%) | 19 (95%) |
| PE at main PA level, n (%) | 56 (88.9%) | 39 (95.1%) | 17 (85%) |
| RV/LV ratio on CT > 1, n (%) | 43 (68.3%) | 32 (82.1%) | 11 (55%) |
| Qanadli Index (%), mean (SD) | 37.7 (±14) | 38 (±13) | 37 (±16.9) |
| Echocardiographic features # | |||
| RV dilation, n (%) | 48 (98%) | 34 (100%) | 14 (93.3%) |
| TAPSE (mm), mean (SD) | 14.3 (5.2) | 14.6 (5.1) | 13.9 (5.6) |
| Systolic PAP (mmHg), mean (SD) | 60 (12) | 59 (12) | 60 (13) |
| Bleeding risk (BACS score), n (%) | |||
| Low | 25 (39.7%) | 20 (46.5%) | 5 (25%) |
| Intermediate | 30 (47.6%) | 16 (37.2%) | 14 (70%) |
| High | 8 (12.7%) | 7 (16.3%) | 1 (5%) |
| Previous systemic thrombolysis, n (%) | 12 (19%) | 11 (25.6%) | 1 (5%) |
| Mean PAP (mmHg) ¶ before CDT, mean (SD) | 36 (±10) | 36 (±10) | 36 (±11) |
| CDL, n (%) | 27 (42.9%) | 18 (41.9%) | 9 (45%) |
| IVC filter insertion, n (%) | 28 (44.5%) | 16 (37.2%) | 12 (60%) |
| Major bleeding, n (%) | 8 (12.7%) | 6 (14%) | 2 (10%) |
| In-hospital PE-related mortality, n (%) | 20 (31.7%) | 17 (39.5%) | 3 (15%) |
| In-hospital all-cause mortality, n (%) | 27 (42.9%) | 20 (46.5%) | 7 (35%) |
| Bleeding Risk, n (%) | Major Bleeding | ||
|---|---|---|---|
| Yes | No | ||
| Low | 1 (4%) | 24 (96%) | p-value = 0.077 * |
| Intermediate | 5 (16.7%) | 25 (83.3%) | |
| High | 2 (25%) | 6 (75%) | |
| Risk Factor | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age > 70 years | 6.22 (1.72–22.43) | 0.005 | 8.93 (1.58–50.34) | 0.013 |
| Sex (male) | 1.73 (0.59–5.06) | 0.321 | ||
| Active cancer | 0.41 (0.10–1.63) | 0.205 | ||
| Diabetes | 6.83 (1.20–39.06) | 0.031 | ||
| Chronic renal failure | 5.71 (1.26–25.96) | 0.024 | ||
| Clinical presentation of PE * | 0.06 | |||
| Dyspnea ± chest pain | ||||
| Syncope | 1.85 (0.49–6.89) | 0.362 | ||
| Cardiac arrest | 5.33 (1.33–21.33) | 0.018 | ||
| High-risk PE | 3.71 (0.94–14.60) | 0.061 | ||
| Simplified PESI Index, per point | 1.59 (0.95–2.65) | 0.076 | ||
| Previous systemic thrombolysis | 6.50 (1.66–25.41) | 0.007 | 13.12 (1.84–93.75) | 0.010 |
| IVC filter insertion | 0.073 (0.015–0.354) | 0.001 | 0.06 (0.01–0.37) | 0.002 |
| CDL | 0.619 (0.207-1.855) | 0.392 | ||
| Risk Factor | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age > 70 years | 4.71 (1.28–17.27) | 0.020 | 4.83 (1.15–20.26) | 0.031 |
| Sex (male) | 1.40 (0.51–3.81) | 0.513 | ||
| Active cancer | 0.52 (0.16–1.72) | 0.282 | ||
| Diabetes | 10.0 (1.13–88.91) | 0.039 | ||
| Chronic renal failure | 5.95 (1.13–31.47) | 0.036 | ||
| High-risk PE | 1.62 (0.54–4.84) | 0.392 | ||
| Simplified PESI Index, per point | 1.13 (0.72–1.79) | 0.594 | ||
| Previous systemic thrombolysis | 5.50 (1.32–22.92) | 0.019 | 6.37 (1.31–30.82) | 0.021 |
| IVC filter insertion | 0.250 (0.084–0.741) | 0.012 | 0.28 (0.08–0.91) | 0.034 |
| CDL | 0.500 (0.178-1.405) | 0.188 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribas, J.; Valcárcel, J.; Alba, E.; Ruíz, Y.; Cuartero, D.; Iriarte, A.; Mora-Luján, J.M.; Huguet, M.; Cerdà, P.; Martínez-Yélamos, S.; et al. Catheter-Directed Therapies in Patients with Pulmonary Embolism: Predictive Factors of In-Hospital Mortality and Long-Term Follow-Up. J. Clin. Med. 2021, 10, 4716. https://doi.org/10.3390/jcm10204716
Ribas J, Valcárcel J, Alba E, Ruíz Y, Cuartero D, Iriarte A, Mora-Luján JM, Huguet M, Cerdà P, Martínez-Yélamos S, et al. Catheter-Directed Therapies in Patients with Pulmonary Embolism: Predictive Factors of In-Hospital Mortality and Long-Term Follow-Up. Journal of Clinical Medicine. 2021; 10(20):4716. https://doi.org/10.3390/jcm10204716
Chicago/Turabian StyleRibas, Jesús, Joana Valcárcel, Esther Alba, Yolanda Ruíz, Daniel Cuartero, Adriana Iriarte, José María Mora-Luján, Marta Huguet, Pau Cerdà, Sergio Martínez-Yélamos, and et al. 2021. "Catheter-Directed Therapies in Patients with Pulmonary Embolism: Predictive Factors of In-Hospital Mortality and Long-Term Follow-Up" Journal of Clinical Medicine 10, no. 20: 4716. https://doi.org/10.3390/jcm10204716
APA StyleRibas, J., Valcárcel, J., Alba, E., Ruíz, Y., Cuartero, D., Iriarte, A., Mora-Luján, J. M., Huguet, M., Cerdà, P., Martínez-Yélamos, S., Corbella, X., Santos, S., & Riera-Mestre, A. (2021). Catheter-Directed Therapies in Patients with Pulmonary Embolism: Predictive Factors of In-Hospital Mortality and Long-Term Follow-Up. Journal of Clinical Medicine, 10(20), 4716. https://doi.org/10.3390/jcm10204716