
Fecal Levels of Lactic, Succinic and Short-Chain Fatty Acids in Patients with Ulcerative Colitis and Crohn Disease: A Pilot Study

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurement of Organic Acids in Stool Samples
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Fecal Organic Acid Levels in IBD Patients and the Control Group
3.3. Fecal Organic Acid Levels and Medications
3.4. Fecal Organic Acid Levels and Dietary Factors
3.5. Fecal Organic Acid Levels and Calprotectin
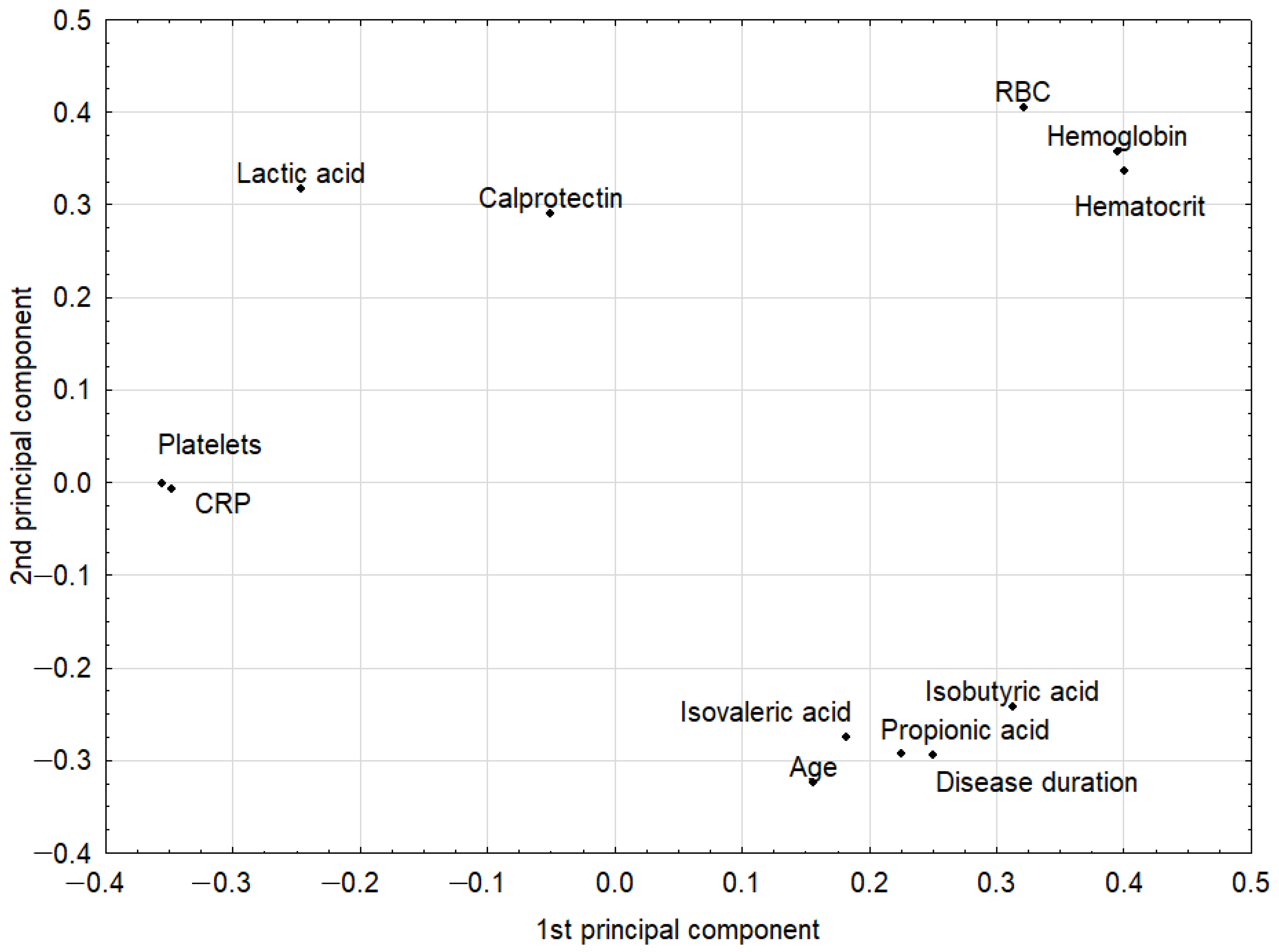
3.6. PCA Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Shouval, D.S.; Rufo, P.A. The role of environmental factors in the pathogenesis of inflammatory bowel diseases. JAMA Pediatr. 2017, 171, 999. [Google Scholar] [CrossRef] [PubMed]
- Yeshi, K.; Ruscher, R.; Hunter, L.; Daly, N.L.; Loukas, A.; Wangchuk, P. Revisiting inflammatory bowel disease: Pathology, treatments, challenges and emerging therapeutics including drug leads from natural products. J. Clin. Med. 2020, 9, 1273. [Google Scholar] [CrossRef] [PubMed]
- Abegunde, A.T.; Muhammad, B.H.; Bhatti, O.; Ali, T. Environmental risk factors for inflammatory bowel diseases: Evidence based literature review. World J. Gastroenterol. 2016, 22, 6296–6317. [Google Scholar] [CrossRef]
- Cummings, J.H.; Pomare, E.W.; Branch, W.J.; Naylor, C.P.; Macfarlane, G.T. Short chain fatty acids in human large intestine, portal, hepatic and venous blood. Gut 1987, 28, 1221–1227. [Google Scholar] [CrossRef] [Green Version]
- Lavelle, A.; Sokol, H. Gut microbiota-derived metabolites as key actors in inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 223–237. [Google Scholar] [CrossRef]
- Venegas, D.P.; De La Fuente, M.K.; Landskron, G.; González, M.J.; Quera, R.; Dijkstra, G.; Harmsen, H.J.M.; Faber, K.N.; Hermoso, M.A. Short chain fatty acids (SCFAs)mediated gut epithelial and immune regulation and its relevance for inflammatory bowel diseases. Front. Immunol. 2019, 10, 277. [Google Scholar] [CrossRef] [Green Version]
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Bäckhed, F. From dietary fiber to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Wang, J.; He, T.; Becker, S.; Zhang, G.; Li, D.; Ma, X. Butyrate: A double-edged sword for health? Adv. Nutr. 2018, 9, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Lloyd-Price, J.; Arze, C.; Ananthakrishnan, A.N.; Schirmer, M.; Avila-Pacheco, J.; Poon, T.W.; Andrews, E.; Ajami, N.J.; Bonham, K.S.; Brislawn, C.J.; et al. Multi-omics of the gut microbial ecosystem in inflammatory bowel diseases. Nature 2019, 569, 655–662. [Google Scholar] [CrossRef]
- Gill, P.A.; van Zelm, M.C.; Muir, J.G.; Gibson, P.R. Review article: Short chain fatty acids as potential therapeutic agents in human gastrointestinal and inflammatory disorders. Aliment. Pharmacol. Ther. 2018, 48, 15–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrowolska-Iwanek, J.; Zagrodzki, P.; Woźniakiewicz, M.; Woźniakiewicz, A.; Zwolińska-Wcisło, M.; Winnicka, D.; Paśko, P. Procedure optimization for extracting short-chain fatty acids from human faeces. J. Pharm. Biomed. Anal. 2016, 124, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Kumari, R.; Ahuja, V.; Paul, J. Fluctuations in butyrate-producing bacteria in ulcerative colitis patients of North India. World J. Gastroenterol. 2013, 19, 3404–3414. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; Li, T.; Li, M.; Huang, S.; Qiu, Y.; Feng, R.; Zhang, S.; Chen, M.; Xiong, L.; Zeng, Z. Systematic review and meta-analysis: Short-chain fatty acid characterization in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2019, 25, 1751–1763. [Google Scholar] [CrossRef] [PubMed]
- Machiels, K.; Joossens, M.; Sabino, J.; De Preter, V.; Arijs, I.; Eeckhaut, V.; Ballet, V.; Claes, K.; Van Immerseel, F.; Verbeke, K.; et al. A decrease of the butyrate-producing species Roseburia hominis and Faecalibacterium prausnitzii defines dysbiosis in patients with ulcerative colitis. Gut 2014, 63, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Takaishi, H.; Matsuki, T.; Nakazawa, A.; Takada, T.; Kado, S.; Asahara, T.; Kamada, N.; Sakuraba, A.; Yajima, T.; Higuchi, H.; et al. Imbalance in intestinal microflora constitution could be involved in the pathogenesis of inflammatory bowel disease. Int. J. Med. Microbiol. 2008, 298, 463–472. [Google Scholar] [CrossRef]
- Macias-Ceja, D.C.; Ortiz-Masiá, D.; Salvador, P.; Gisbert-Ferrándiz, L.; Hernández, C.; Hausmann, M.; Rogler, G.; Esplugues, J.V.; Hinojosa, J.; Alós, R.; et al. Succinate receptor mediates intestinal inflammation and fibrosis. Mucosal Immunol. 2019, 12, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Connors, J.; Dawe, N.; Van Limbergen, J. The role of succinate in the regulation of intestinal inflammation. Nutrients 2019, 11, 25. [Google Scholar] [CrossRef] [Green Version]
- Hove, H.; Mortensen, P.B. Influence of intestinal inflammation (IBD) and small and large bowel length on fecal short-chain fatty acids and lactate. Dig. Dis. Sci. 1995, 40, 1372–1380. [Google Scholar] [CrossRef]
- Huda-Faujan, N.; Abdulamir, A.S.; Fatimah, A.B.; Anas, O.M.; Shuhaimi, M.; Yazid, A.M.; Loong, Y.Y. The impact of the level of the intestinal short chain fatty acids in inflammatory bowel disease patients versus healthy subjects. Open Biochem. J. 2010, 4, 53–58. [Google Scholar] [CrossRef]
- Pucino, V.; Bombardieri, M.; Pitzalis, C.; Mauro, C. Lactate at the crossroads of metabolism, inflammation, and autoimmunity. Eur. J. Immunol. 2017, 47, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Zasłona, Z.; O’Neill, L.A.J. Cytokine-like roles for metabolites in immunity. Mol. Cell 2020, 78, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Vich Vila, A.; Collij, V.; Sanna, S.; Sinha, T.; Imhann, F.; Bourgonje, A.R.; Mujagic, Z.; Jonkers, D.M.A.E.; Masclee, A.A.M.; Fu, J.; et al. Impact of commonly used drugs on the composition and metabolic function of the gut microbiota. Nat. Commun. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Aden, K.; Rehman, A.; Waschina, S.; Pan, W.H.; Walker, A.; Lucio, M.; Nunez, A.M.; Bharti, R.; Zimmerman, J.; Bethge, J.; et al. Metabolic functions of gut microbes associate with efficacy of tumor necrosis factor antagonists in patients with inflammatory bowel diseases. Gastroenterology 2019, 157, 1279–1292.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayesh, R.; Weststrate, J.A.; Drewitt, P.N.; Hepburn, P.A. Safety evaluation of phytosterol esters. Part 5. Faecal short-chain fatty acid and microflora content, faecal bacterial enzyme activity and serum female sex hormones in healthy normolipidaemic volunteers consuming a controlled diet either with or without. Food Chem. Toxicol. 1999, 37, 1127–1138. [Google Scholar] [CrossRef]
- El Oufir, L.; Flourié, B.; Bruley Des Varannes, S.; Barry, J.L.; Cloarec, D.; Bornet, F.; Galmiche, J.P. Relations between transit time, fermentation products, and hydrogen consuming flora in healthy humans. Gut 1996, 38, 870–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarmakiewicz-Czaja, S.; Piątek, D.; Filip, R. The influence of nutrients on inflammatory bowel diseases. J. Nutr. Metab. 2020, 2020, 2894169. [Google Scholar] [CrossRef] [Green Version]
- Sun, M.; Wu, W.; Liu, Z.; Cong, Y. Microbiota metabolite short chain fatty acids, GPCR, and inflammatory bowel diseases. J. Gastroenterol. 2017, 52, 1–8. [Google Scholar] [CrossRef]
- Hallert, C.; Björck, I.; Nyman, M.; Pousette, A.; Grännö, C.; Svensson, H. Increasing fecal butyrate in ulcerative colitis patients by diet: Controlled pilot study. Inflamm. Bowel Dis. 2003, 9, 116–121. [Google Scholar] [CrossRef]
- Casellas, F.; Borruel, N.; Torrejón, A.; Varela, E.; Antolin, M.; Guarner, F.; Malagelada, J.R. Oral oligofructose-enriched inulin supplementation in acute ulcerative colitis is well tolerated and associated with lowered faecal calprotectin. Aliment. Pharmacol. Ther. 2007, 25, 1061–1067. [Google Scholar] [CrossRef]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Lopetuso, L.R.; Scaldaferri, F.; Pulcini, G.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. Food components and dietary habits: Keys for a healthy gut microbiota composition. Nutrients 2019, 11, 2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svolos, V.; Hansen, R.; Nichols, B.; Quince, C.; Ijaz, U.Z.; Papadopoulou, R.T.; Edwards, C.A.; Watson, D.; Alghamdi, A.; Brejnrod, A.; et al. Treatment of active Crohn’s disease with an ordinary food-based diet that replicates exclusive enteral nutrition. Gastroenterology 2019, 156, 1354–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Cuesta-Zuluaga, J.; Mueller, N.T.; Álvarez-Quintero, R.; Velásquez-Mejía, E.P.; Sierra, J.A.; Corrales-Agudelo, V.; Carmona, J.A.; Abad, J.M.; Escobar, J.S. Higher fecal short-chain fatty acid levels are associated with gut microbiome dysbiosis, obesity, hypertension and cardiometabolic disease risk factors. Nutrients 2019, 11, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Parameter | UC | CD | Controls |
| No. of patients | 23 | 8 | 4 |
| Sex (male/female) | 13/10 (57/43) | 5/3 (63/37) | 2/2 (50/50) |
| Median age, years | 32 | 33.5 | 48 |
| CDAI score (<150/≥150 points) | NA | 4/4 (50/50) | NA |
| Mayo score (0/1/2/3) | 0/10/6/7 (0/44/26/30) | NA | NA |
| Therapy | |||
| Steroids (yes/no) | 13/9 (59/41) 1 | 2/6 (25/75) | 0/4 (0/100) |
| Azathioprine/6-mercaptopurine (yes/no) | 9/14 (39/61) | 5/3 (63/37) | 0/4 (0/100) |
| 5-Aminosalicylic acid (yes/no) | 21/2 (91/9) | 6/1 (86/14) 1 | 0/4 (0/100) |
| Biological drugs (yes/no) | 2/21 (9/91) | 3/5 (37/63) | 0/4 (0/100) |
| Trimebutine (yes/no) | 7/16 (30/70) | 1/7 (12/88) | 0/4 (0/100) |
| Organic Acid | Study Group | ||||||
|---|---|---|---|---|---|---|---|
| Controls (n = 4) | Mild UC (n = 10) | Moderate UC (n = 6) | Severe UC (n = 7) | Inactive CD (n = 4) | Active CD (n = 4) | p Value | |
| Succinic [ug/g] | 144.6 (77.0; 238.6) | 472.4 (197.3; 1368.5) | 193.3 (118.4; 279.1) | 149.4 (125.3; 551.5) | 195.3 (104.5; 456.8) | 305.8 (147.1; 516.5) | 0.495 |
| Acetic [ug/g] | 604.1 (446.7; 763.0) | 709.0 (450.7; 967.4) | 904.0 (552.4; 1082.3) | 666.9 (594.0; 906.3) | 648.0 (462.6; 742.6) | 831.8 (523.3; 1202.0) | 0.842 |
| Lactic [ug/g] | 128.3 (49.7; 843.9) | 606.6 (216.5; 2286.9) | 621.7 (119.8; 1591.0) | 871.7 (294.3; 2616.2) | 392.5 (26.5; 2077.1) | 994.5 (334.1; 1858.6) | 0.516 |
| Propionic [ug/g] | 181.5 (61.0; 331.8) | 211.3 (117.8; 576.1) | 365.5 (241.9; 548.1) | 223.9 (71.1; 440.8) | 218.1 (166.7; 457.6) | 451.7 (205.9; 598.2) | 0.593 |
| Butyric [ug/g] | 109.0 (67.5; 176.3) | 226.2 (72.5; 375.4) | 378.0 (144.4; 642.2) | 157.5 (54.7; 375.4) | 217.0 (109.4; 228.7) | 147.2 (<LOD; 305.9) | 0.768 |
| Isobutyric [ug/g] | 19.0 (<LOD; 50.1) | 26.8 (<LOD; 61.8) | <LOD (<LOD; 49.9) | <LOD (<LOD; 42.4) | 40.1 (21.4; 61.8) | 21.9 (<LOD; 39.1) | 0.902 |
| Valeric [ug/g] | 13.4 (<LOD; 31.1) | <LOD (<LOD; <LOD) | <LOD (<LOD; <LOD) | <LOD (<LOD; 29.7) | <LOD (<LOD; 20.3) | <LOD (<LOD; 24.9) | 0.916 |
| Isovaleric [ug/g] | 41.4 (<LOD; 122.8) | 29.7 (<LOD; 280.2) | 24.5 (<LOD; 51.3) | <LOD (<LOD; 49.9) | 42.1 (18.8; 67.0) | <LOD (<LOD; 20.3) | 0.742 |
| Pairs of Correlated Parameters | Correlation Weights | |
|---|---|---|
| Hemoglobin | Hematocrit | 0.158 |
| RBC | Hemoglobin | 0.142 |
| RBC | Hematocrit | 0.133 |
| RBC | Lactic acid | 0.128 |
| Platelets | CRP | 0.124 |
| Hemoglobin | Lactic acid | 0.111 |
| Hematocrit | Lactic acid | 0.104 |
| Hemoglobin | CRP | −0.100 |
| Hemoglobin | Platelets | −0.104 |
| Hematocrit | CRP | −0.105 |
| Hematocrit | Platelets | −0.109 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaczmarczyk, O.; Dąbek-Drobny, A.; Woźniakiewicz, M.; Paśko, P.; Dobrowolska-Iwanek, J.; Woźniakiewicz, A.; Piątek-Guziewicz, A.; Zagrodzki, P.; Mach, T.; Zwolińska-Wcisło, M. Fecal Levels of Lactic, Succinic and Short-Chain Fatty Acids in Patients with Ulcerative Colitis and Crohn Disease: A Pilot Study. J. Clin. Med. 2021, 10, 4701. https://doi.org/10.3390/jcm10204701
Kaczmarczyk O, Dąbek-Drobny A, Woźniakiewicz M, Paśko P, Dobrowolska-Iwanek J, Woźniakiewicz A, Piątek-Guziewicz A, Zagrodzki P, Mach T, Zwolińska-Wcisło M. Fecal Levels of Lactic, Succinic and Short-Chain Fatty Acids in Patients with Ulcerative Colitis and Crohn Disease: A Pilot Study. Journal of Clinical Medicine. 2021; 10(20):4701. https://doi.org/10.3390/jcm10204701
Chicago/Turabian StyleKaczmarczyk, Olga, Agnieszka Dąbek-Drobny, Michał Woźniakiewicz, Paweł Paśko, Justyna Dobrowolska-Iwanek, Aneta Woźniakiewicz, Agnieszka Piątek-Guziewicz, Paweł Zagrodzki, Tomasz Mach, and Małgorzata Zwolińska-Wcisło. 2021. "Fecal Levels of Lactic, Succinic and Short-Chain Fatty Acids in Patients with Ulcerative Colitis and Crohn Disease: A Pilot Study" Journal of Clinical Medicine 10, no. 20: 4701. https://doi.org/10.3390/jcm10204701
APA StyleKaczmarczyk, O., Dąbek-Drobny, A., Woźniakiewicz, M., Paśko, P., Dobrowolska-Iwanek, J., Woźniakiewicz, A., Piątek-Guziewicz, A., Zagrodzki, P., Mach, T., & Zwolińska-Wcisło, M. (2021). Fecal Levels of Lactic, Succinic and Short-Chain Fatty Acids in Patients with Ulcerative Colitis and Crohn Disease: A Pilot Study. Journal of Clinical Medicine, 10(20), 4701. https://doi.org/10.3390/jcm10204701