
Gender Differences among Sardinians with Alcohol Use Disorder

 , , ,
, , , 
Abstract
1. Introduction
2. Methods
2.1. Authorization and Selection of Participants
2.2. Data Collection
Data Collected
2.3. Calculation
3. Results
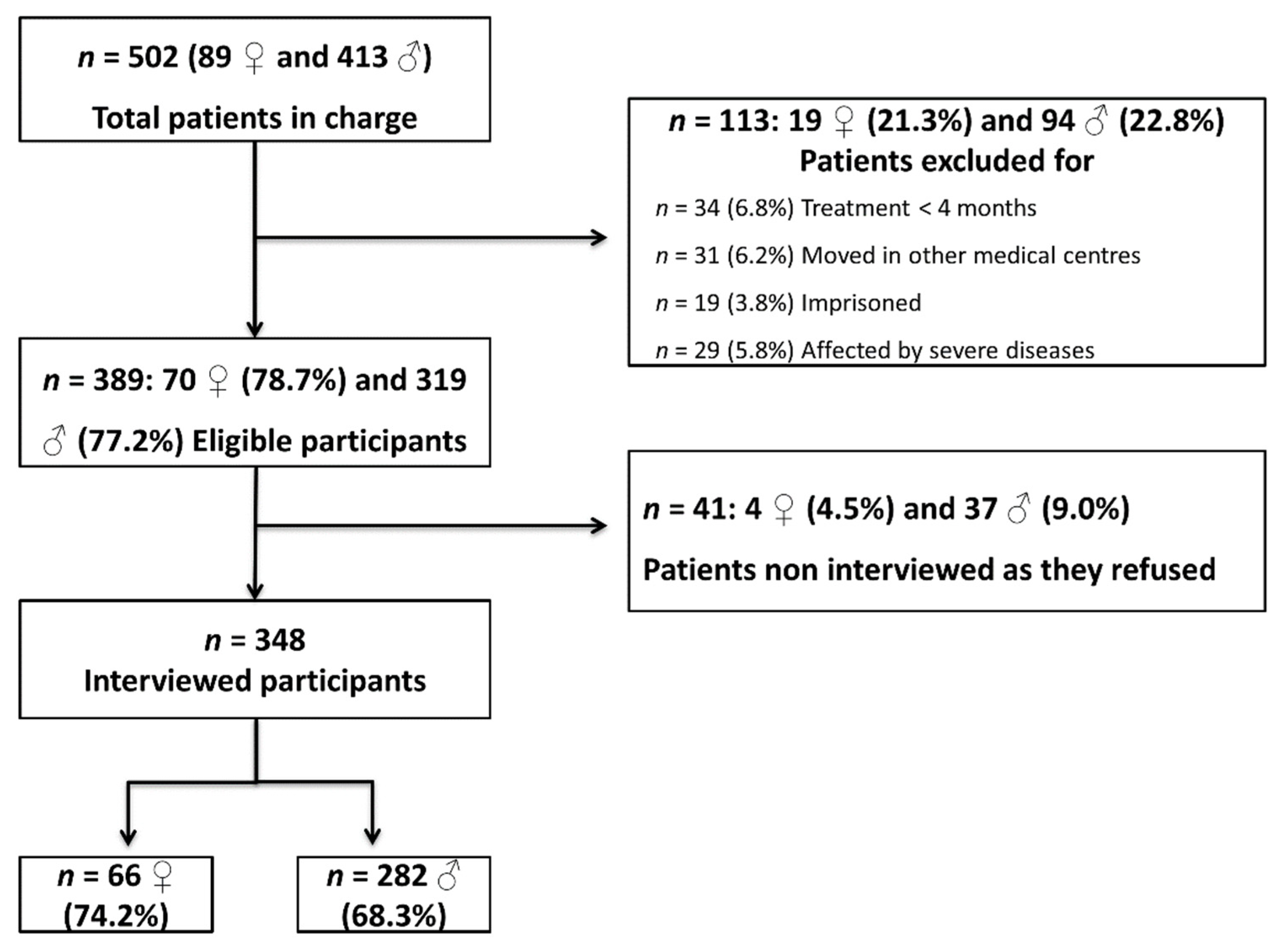
3.1. Selection of Participants
3.2. Gender Differences and Birth Cohort Effects in Drinking Characteristics of AUD Sardinian Patients
3.2.1. Main Characteristics
3.2.2. Age at First Drink
3.2.3. Age at Onset of Regular Drinking
3.2.4. Age at Onset of AUD
3.2.5. Age at First Request for Care
3.2.6. Lapse from Regular Use to AUD Onset
3.2.7. Lapse from AUD Onset to First Request for Care
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agabio, R.; Campesi, I.; Pisanu, C.; Gessa, G.L.; Franconi, F. Sex differences in substance use disorders: Focus on side effects. Addict. Biol. 2016, 21, 1030–1042. [Google Scholar] [CrossRef] [PubMed]
- Erol, A.; Karpyak, V.M. Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug Alcohol Depend. 2015, 156, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hui, P.; Nakayama, T.; Morita, A.; Sato, N.; Hishiki, M.; Saito, K.; Yoshikawa, Y.; Tamura, M.; Sato, I.; Takahashi, T.; et al. Common single nucleotide polymorphisms in Japanese patients with essential hypertension: Aldehyde dehydrogenase 2 gene as a risk factor independent of alcohol consumption. Hypertens. Res. 2007, 30, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Mulia, N.; Karriker-Jaffe, K.J.; Witbrodt, J.; Bond, J.; Williams, E.; Zemore, S.E. Racial/ethnic differences in 30-year trajectories of heavy drinking in a nationally representative U.S. sample. Drug Alcohol Depend. 2017, 170, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Martins, S.S.; Blanco, C.; Hasin, D.S. Telescoping and gender differences in alcohol dependence: New evidence from two national surveys. Am. J. Psychiatry 2010, 167, 969–976. [Google Scholar] [CrossRef]
- Khan, S.; Okuda, M.; Hasin, D.S.; Secades-Villa, R.; Keyes, K.; Lin, K.H.; Grant, B.; Blanco, C. Gender differences in lifetime alcohol dependence: Results from the national epidemiologic survey on alcohol and related conditions. Alcohol. Clin. Exp. Res. 2013, 37, 1696–1705. [Google Scholar] [CrossRef]
- Lettre, G.; Hirschhorn, J.N. Small island, big genetic discoveries. Nat. Genet. 2015, 47, 1224–1225. [Google Scholar] [CrossRef]
- Chiang, C.W.K.; Marcus, J.H.; Sidore, C.; Biddanda, A.; Al-Asadi, H.; Zoledziewska, M.; Pitzalis, M.; Busonero, F.; Maschio, A.; Pistis, G.; et al. Genomic history of the Sardinian population. Nat. Genet. 2018, 50, 1426–1434. [Google Scholar] [CrossRef]
- Pes, G.M.; Tolu, F.; Dore, M.P.; Sechi, G.P.; Errigo, A.; Canelada, A.; Poulain, M. Male longevity in Sardinia, a review of historical sources supporting a causal link with dietary factors. Eur. J. Clin. Nutr. 2015, 69, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Centro Ricerche Economiche Nord Sud (Center for Nourth South Economic Research). Economia della Sardegna. 27° Rapporto 2020. CRENoS—27° Rapporto sull’Economia della Sardegna—2020.pdf (unica.it); Arkadia Editor, Cagliari (CA). 2020. Available online: https://crenos.unica.it/crenosterritorio/sites/default/files/allegati-pubblicazioni-tes/CRENoS%20-%2027%C2%B0%20Rapporto%20sull%27Economia%20della%20Sardegna%20-%202020.pdf (accessed on 27 September 2021).
- Grittner, U.; Wilsnack, S.; Kuntsche, S.; Greenfield, T.K.; Wilsnack, R.; Kristjanson, A.; Bloomfield, K. A Multilevel Analysis of Regional and Gender Differences in the Drinking Behavior of 23 Countries. Subst. Use Misuse 2020, 55, 772–786. [Google Scholar] [CrossRef] [PubMed]
- Kilian, C.; Manthey, J.; Kraus, L.; Makela, P.; Moskalewicz, J.; Sieroslawski, J.; Rehm, J. A new perspective on European drinking cultures: A model-based approach to determine variations in drinking practices among 19 European countries. Addiction 2021, 116, 2016–2025. [Google Scholar] [CrossRef]
- Manthey, J.; Shield, K.D.; Rylett, M.; Hasan, O.S.M.; Probst, C.; Rehm, J. Global alcohol exposure between 1990 and 2017 and forecasts until 2030: A modelling study. Lancet 2019, 393, 2493–2502. [Google Scholar] [CrossRef]
- Bloomfield, K.; Gmel, G.; Neve, R.; Mustonen, H. Investigating Gender Convergence in Alcohol Consumption in Finland, Germany, The Netherlands, and Switzerland: A Repeated Survey Analysis. Subst. Abus. 2001, 22, 39–53. [Google Scholar] [CrossRef]
- Rahav, G.; Wilsnack, R.; Bloomfield, K.; Gmel, G.; Kuntsche, S. The influence of societal level factors on men’s and women’s alcohol consumption and alcohol problems. Alcohol Alcohol. 2006, 41, i47–i55. [Google Scholar] [CrossRef]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Wilsnack, S.C. The GENACIS project: A review of findings and some implications for global needs in women-focused substance abuse prevention and intervention. Subst. Abus. Rehabil. 2012, 3, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Wilsnack, S.C.; Wilsnack, R.W. International gender and alcohol research: Recent findings and future directions. Alcohol Res. Health 2002, 26, 245–250. [Google Scholar] [PubMed]
- Ehlers, C.L.; Gizer, I.R.; Vieten, C.; Gilder, A.; Gilder, D.A.; Stouffer, G.M.; Lau, P.; Wilhelmsen, K.C. Age at regular drinking, clinical course, and heritability of alcohol dependence in the San Francisco family study: A gender analysis. Am. J. Addict. 2010, 19, 101–110. [Google Scholar] [CrossRef]
- Goldstein, R.B.; Dawson, D.A.; Chou, S.P.; Grant, B.F. Sex differences in prevalence and comorbidity of alcohol and drug use disorders: Results from wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Stud. Alcohol Drugs 2012, 73, 938–950. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, S.F.; Pettinati, H.M.; O’Malley, S.; Randall, P.K.; Randall, C.L. Gender differences in alcohol treatment: An analysis of outcome from the COMBINE study. Alcohol. Clin. Exp. Res. 2010, 34, 1803–1812. [Google Scholar] [CrossRef]
- Grucza, R.A.; Norberg, K.; Bucholz, K.K.; Bierut, L.J. Correspondence between secular changes in alcohol dependence and age of drinking onset among women in the United States. Alcohol. Clin. Exp. Res. 2008, 32, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Avila, C.A.; Rounsaville, B.J.; Kranzler, H.R. Opioid-, cannabis- and alcohol-dependent women show more rapid progression to substance abuse treatment. Drug Alcohol Depend. 2004, 74, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Holdcraft, L.C.; Iacono, W.G. Cohort effects on gender differences in alcohol dependence. Addiction 2002, 97, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.B.; Richter, L.; Kleber, H.D.; McLellan, A.T.; Carise, D. Telescoping of drinking-related behaviors: Gender, racial/ethnic, and age comparisons. Subst. Use Misuse 2005, 40, 1139–1151. [Google Scholar] [CrossRef]
- Kirpich, I.A.; McClain, C.J.; Vatsalya, V.; Schwandt, M.; Phillips, M.; Falkner, K.C.; Zhang, L.; Harwell, C.; George, D.T.; Umhau, J.C. Liver Injury and Endotoxemia in Male and Female Alcohol-Dependent Individuals Admitted to an Alcohol Treatment Program. Alcohol. Clin. Exp. Res. 2017, 41, 747–757. [Google Scholar] [CrossRef]
- Lewis, B.; Nixon, S.J. Characterizing gender differences in treatment seekers. Alcohol. Clin. Exp. Res. 2014, 38, 275–284. [Google Scholar] [CrossRef]
- Lisansky, E.S. Alcoholism in women: Social and psychological concomitants. I. Social history data. Q. J. Stud. Alcohol 1957, 18, 588–623. [Google Scholar] [CrossRef]
- Piazza, N.J.; Vrbka, J.L.; Yeager, R.D. Telescoping of alcoholism in women alcoholics. Int. J. Addict. 1989, 24, 19–28. [Google Scholar] [CrossRef]
- Randall, C.L.; Roberts, J.S.; Del Boca, F.K.; Carroll, K.M.; Connors, G.J.; Mattson, M.E. Telescoping of landmark events associated with drinking: A gender comparison. J. Stud. Alcohol 1999, 60, 252–260. [Google Scholar] [CrossRef]
- Schuckit, M.A.; Anthenelli, R.M.; Bucholz, K.K.; Hesselbrock, V.M.; Tipp, J. The time course of development of alcohol-related problems in men and women. J. Stud. Alcohol 1995, 56, 218–225. [Google Scholar] [CrossRef]
- Schuckit, M.A.; Daeppen, J.B.; Tipp, J.E.; Hesselbrock, M.; Bucholz, K.K. The clinical course of alcohol-related problems in alcohol dependent and nonalcohol dependent drinking women and men. J. Stud. Alcohol 1998, 59, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Sonne, S.C.; Back, S.E.; Diaz Zuniga, C.; Randall, C.L.; Brady, K.T. Gender differences in individuals with comorbid alcohol dependence and post-traumatic stress disorder. Am. J. Addict. 2003, 12, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Alvanzo, A.A.; Storr, C.L.; Mojtabai, R.; Green, K.M.; Pacek, L.R.; La Flair, L.N.; Cullen, B.A.; Crum, R.M. Gender and race/ethnicity differences for initiation of alcohol-related service use among persons with alcohol dependence. Drug Alcohol Depend. 2014, 140, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, A.; Dams, J.; Rosahl, A.; Hempleman, J.; Konig, H.H.; Konnopka, A.; Kraus, L.; Kriston, L.; Piontek, D.; Reimer, J.; et al. Patient-Centered Placement Matching of Alcohol-Dependent Patients Based on a Standardized Intake Assessment: Primary Outcomes of an Exploratory Randomized Controlled Trial. Eur. Addict. Res. 2020, 26, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.; Croissant, B.; Batra, A.; Mundle, G.; Nakovics, H.; Mann, K. Alcoholism in women: Is it different in onset and outcome compared to men? Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 344–351. [Google Scholar] [CrossRef]
- Dunne, F.J.; Galatopoulos, C.; Schipperheijn, J.M. Gender differences in psychiatric morbidity among alcohol misusers. Compr. Psychiatry 1993, 34, 95–101. [Google Scholar] [CrossRef]
- Blankfield, A. Female alcoholics. II. The expression of alcoholism in relation to gender and age. Acta Psychiatr. Scand. 1990, 81, 448–452. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Alcohol and Health; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Popova, S.; Lange, S.; Probst, C.; Gmel, G.; Rehm, J. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e290–e299. [Google Scholar] [CrossRef]
- Shield, K.D.; Soerjomataram, I.; Rehm, J. Alcohol Use and Breast Cancer: A Critical Review. Alcohol. Clin. Exp. Res. 2016, 40, 1166–1181. [Google Scholar] [CrossRef]
- Agabio, R.; Madeddu, C.; Contu, P.; Cosentino, S.; Deiana, M.; Massa, E.; Mereu, A.; Politi, C.; Sardu, C.; Sinclair, J.M.A. Alcohol Consumption Is a Modifiable Risk Factor for Breast Cancer: Are Women Aware of This Relationship? Alcohol Alcohol. 2021. [Google Scholar] [CrossRef]
- Sinclair, J.; McCann, M.; Sheldon, E.; Gordon, I.; Brierley-Jones, L.; Copson, E. The acceptability of addressing alcohol consumption as a modifiable risk factor for breast cancer: A mixed method study within breast screening services and symptomatic breast clinics. BMJ Open 2019, 9, e027371. [Google Scholar] [CrossRef] [PubMed]
- Allamani, A.; Voller, F.; Kubicka, L.; Bloomfield, K. Drinking Cultures and the Position of Women in Nine European Countries. Subst Abus. 2000, 21, 231–247. [Google Scholar] [CrossRef] [PubMed]
- Bratberg, G.H.; Wilsnack, S.C.; Wilsnack, R.; Haugland, S.H.; Krokstad, S.; Sund, E.R.; Bjørngaard, J.H. Gender differences and gender convergence in alcohol use over the past three decades (1984–2008), The HUNT Study, Norway. BMC Public Health 2016, 16, 723. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Min, A.; Min, H. Gender Convergence in Alcohol Consumption Patterns: Findings from the Korea National Health and Nutrition Examination Survey 2007–2016. Int. J. Environ. Res. Public Health 2020, 17, 9317. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Jager, J.; Mal-Sarkar, T.; Patrick, M.E.; Rutherford, C.; Hasin, D. Is There a Recent Epidemic of Women’s Drinking? A Critical Review of National Studies. Alcohol. Clin. Exp. Res. 2019, 43, 1344–1359. [Google Scholar] [CrossRef]
- Keyes, K.M.; Li, G.; Hasin, D.S. Birth cohort effects and gender differences in alcohol epidemiology: A review and synthesis. Alcohol. Clin. Exp. Res. 2011, 35, 2101–2112. [Google Scholar] [CrossRef]
- Machado, I.E.; Monteiro, M.G.; Malta, D.C.; Lana, F.C.F. Brazilian Health Survey (2013): Relation between alcohol use and sociodemographic characteristics by sex in Brazil. Rev. Bras. Epidemiol. 2017, 20, 408–422. [Google Scholar] [CrossRef]
- McPherson, M.; Casswell, S.; Pledger, M. Gender convergence in alcohol consumption and related problems: Issues and outcomes from comparisons of New Zealand survey data. Addiction 2004, 99, 738–748. [Google Scholar] [CrossRef]
- Slade, T.; Chapman, C.; Swift, W.; Keyes, K.; Tonks, Z.; Teesson, M. Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: Systematic review and metaregression. BMJ Open 2016, 6, e011827. [Google Scholar] [CrossRef]
- White, A.; Castle, I.J.; Chen, C.M.; Shirley, M.; Roach, D.; Hingson, R. Converging Patterns of Alcohol Use and Related Outcomes Among Females and Males in the United States, 2002 to 2012. Alcohol. Clin. Exp. Res. 2015, 39, 1712–1726. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Angermeyer, M.C.; Bernert, S.; Bruffaerts, R.; Brugha, T.S.; Bryson, H.; de Girolamo, G.; Graaf, R.; Demyttenaere, K.; Gasquet, I.; et al. Use of mental health services in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand. 2004, 109, 47–54. [Google Scholar] [CrossRef]
- Cohen, E.; Feinn, R.; Arias, A.; Kranzler, H.R. Alcohol treatment utilization: Findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2007, 86, 214–221. [Google Scholar] [CrossRef]
- Grant, B.F.; Goldstein, R.B.; Saha, T.D.; Chou, S.P.; Jung, J.; Zhang, H.; Pickering, R.P.; Ruan, W.J.; Smith, S.M.; Huang, B.; et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry 2015, 72, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Jones, C.M.; Einstein, E.B.; Powell, P.A.; Compton, W.M. Use of Medications for Alcohol Use Disorder in the US: Results From the 2019 National Survey on Drug Use and Health. JAMA Psychiatry 2021, 78, 922–924. [Google Scholar] [CrossRef] [PubMed]
- Mekonen, T.; Chan, G.C.K.; Connor, J.; Hall, W.; Hides, L.; Leung, J. Treatment rates for alcohol use disorders: A systematic review and meta-analysis. Addiction 2020, 116, 2617–2634. [Google Scholar] [CrossRef] [PubMed]
- Ministro della Salute. Relazione del Ministro della Salute al Parlamento Sugli Interventi Realizzati ai Sensi della Legge 30.3.2001 N. 125, Legge Quadro In Materia di Alcol e Problemi Alcolcorrelati; Report to Parliament from the Italian Ministry of Health about Interventions According to Law 30.3.2001 Number 125, General Law on Alcohol and Alcohol-Related Problems; Ministro Della Salute: Rome, Italy, 2019. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2984_allegato.pdf (accessed on 27 September 2021).
- Rehm, J.; Allamani, A.; Elekes, Z.; Jakubczyk, A.; Manthey, J.; Probst, C.; Struzzo, P.; Della Vedova, R.; Gual, A.; Wojnar, M. Alcohol dependence and treatment utilization in Europe—A representative cross-sectional study in primary care. BMC Fam. Pract. 2015, 16, 90. [Google Scholar] [CrossRef]
- Grosso, J.A.; Epstein, E.E.; McCrady, B.S.; Gaba, A.; Cook, S.; Backer-Fulghum, L.M.; Graff, F.S. Women’s motivators for seeking treatment for alcohol use disorders. Addict. Behav. 2013, 38, 2236–2245. [Google Scholar] [CrossRef] [PubMed]
- McCrady, B.S.; Epstein, E.E.; Fokas, K.F. Treatment Interventions for Women with Alcohol Use Disorder. Alcohol Res. 2020, 40, 8. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Allamani, A.; Aubin, H.J.; Della Vedova, R.; Elekes, Z.; Frick, U.; Jakubczyk, A.; Kostogianni, N.; Landsmane, I.; Manthey, J.; et al. People with alcohol use disorders in specialized care in eight different European countries. Alcohol Alcohol. 2015, 50, 310–318. [Google Scholar] [CrossRef]
- Terplan, M.; McNamara, E.J.; Chisolm, M.S. Pregnant and non-pregnant women with substance use disorders: The gap between treatment need and receipt. J. Addict. Dis. 2012, 31, 342–349. [Google Scholar] [CrossRef]
- Ministro della Salute. Relazione del Ministro della Salute al Parlamento Sugli Interventi Realizzati ai Sensi della Legge 30.3.2001 N. 125, Legge Quadro In Materia di Alcol e Problemi Alcolcorrelati; Report to Parliament from the Italian Ministry of Health about Interventions According to Law 30.3.2001 Number 125, General Law on Alcohol and Alcohol-Related Problems; Ministro della Salute: Rome, Italy, 2012. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_1899_allegato.pdf (accessed on 27 September 2021).
- Trogu, E.; Vacca, R.; Agabio, R.; Carta, I.; Pani, P.P.; Siza, R. Rapporto Regionale Sullo Stato delle Dipendenze in Sardegna 2008. 2008. Available online: https://www.yumpu.com/it/document/read/23165637/rapporto-regionale-sullo-stato-delle-dipendenze-sardegna-salute (accessed on 27 September 2021).
- Ashley, M.J.; Olin, J.S.; le Riche, W.H.; Kornaczewski, A.; Schmidt, W.; Rankin, J.G. Morbidity in alcoholics. Evidence for accelerated development of physical disease in women. Arch. Intern. Med. 1977, 137, 883–887. [Google Scholar] [CrossRef]
- Hesselbrock, M.N.; Meyer, R.E.; Keener, J.J. Psychopathology in hospitalized alcoholics. Arch. Gen. Psychiatry 1985, 42, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, L. Female alcoholics. III. Development and pattern of problem drinking. Acta Psychiatr. Scand. 1978, 57, 325–335. [Google Scholar] [CrossRef]
- Picci, R.L.; Vigna-Taglianti, F.; Oliva, F.; Mathis, F.; Salmaso, S.; Ostacoli, L.; Sodano, A.J.; Furlan, P.M. Personality disorders among patients accessing alcohol detoxification treatment: Prevalence and gender differences. Compr. Psychiatry 2012, 53, 355–363. [Google Scholar] [CrossRef]
- Verhulst, B.; Neale, M.C.; Kendler, K.S. The heritability of alcohol use disorders: A meta-analysis of twin and adoption studies. Psychol. Med. 2015, 45, 1061–1072. [Google Scholar] [CrossRef]
- Hart, A.B.; Kranzler, H.R. Alcohol Dependence Genetics: Lessons Learned from Genome-Wide Association Studies (GWAS) and Post-GWAS Analyses. Alcohol. Clin. Exp. Res. 2015, 39, 1312–1327. [Google Scholar] [CrossRef]
- Schuckit, M.A. A brief history of research on the genetics of alcohol and other drug use disorders. J. Stud. Alcohol Drugs 2014, 75, 59–67. [Google Scholar] [CrossRef][Green Version]
- Agabio, R.; Pisanu, C.; Gessa, G.L.; Franconi, F. Sex Differences in Alcohol Use Disorder. Curr. Med. Chem. 2017, 24, 2661–2670. [Google Scholar] [CrossRef]
- Calo, C.M.; Vona, G.; Robledo, R.; Francalacci, P. From old markers to next generation: Reconstructing the history of the peopling of Sardinia. Ann. Hum. Biol. 2021, 48, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Nunes, E.V.; Kunz, K.; Galanter, M.; O’Connor, P.G. Addiction Psychiatry and Addiction Medicine: The Evolution of Addiction Physician Specialists. Am. J. Addict. 2020, 29, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, I.; Gentili, C.; Guazzelli, M. Alcohol consumption and heavy drinking: A survey in three Italian villages. Alcohol Alcohol. 2006, 41, 336–340. [Google Scholar] [CrossRef]
- Digrande, L.; Perrier, M.P.; Lauro, M.G.; Contu, P. Alcohol use and correlates of binge drinking among university students on the Island of Sardinia, Italy. Subst. Use Misuse 2000, 35, 1471–1483. [Google Scholar] [CrossRef]
- Mereu, A.; Liori, A.; Dessi, C.; Girau, M.; Mc Gilliard, D.C.; Sotgiu, A.; Agabio, R.; Contu, P.; Sardu, C. Alcohol-Related Behaviour in Freshmen University Students in Sardinia, Italy. Int. J. Environ. Res. Public Health 2021, 18, 7203. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Shield, K.D.; Gmel, G.; Rehm, M.X.; Frick, U. Modeling the impact of alcohol dependence on mortality burden and the effect of available treatment interventions in the European Union. Eur. Neuropsychopharmacol. 2013, 23, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Agabio, R.; Pani, P.P.; Preti, A.; Gessa, G.L.; Franconi, F. Efficacy of Medications Approved for the Treatment of Alcohol Dependence and Alcohol Withdrawal Syndrome in Female Patients: A Descriptive Review. Eur. Addict. Res. 2016, 22, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Baraona, E.; Abittan, C.S.; Dohmen, K.; Moretti, M.; Pozzato, G.; Chayes, Z.W.; Schaefer, C.; Lieber, C.S. Gender differences in pharmacokinetics of alcohol. Alcohol. Clin. Exp. Res. 2001, 25, 502–507. [Google Scholar] [CrossRef]
- Roerecke, M.; Gual, A.; Rehm, J. Reduction of alcohol consumption and subsequent mortality in alcohol use disorders: Systematic review and meta-analyses. J. Clin. Psychiatry 2013, 74, e1181–e1189. [Google Scholar] [CrossRef]
- Witkiewitz, K.; Litten, R.Z.; Leggio, L. Advances in the science and treatment of alcohol use disorder. Sci. Adv. 2019, 5, eaax4043. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Phelan, J.C.; Link, B.G. Stigma as a fundamental cause of population health inequalities. Am. J. Public Health 2013, 103, 813–821. [Google Scholar] [CrossRef]
- Probst, C.; Manthey, J.; Martinez, A.; Rehm, J. Alcohol use disorder severity and reported reasons not to seek treatment: A cross-sectional study in European primary care practices. Subst. Abus. Treat. Prev. Policy 2015, 10, 32. [Google Scholar] [CrossRef]
- Stangl, A.L.; Earnshaw, V.A.; Logie, C.H.; van Brakel, W.; Simbayi, L.C.; Barré, I.; Dovidio, J.F. The Health Stigma and Discrimination Framework: A global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. 2019, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Hilderbrand, E.R.; Lasek, A.W. Studying Sex Differences in Animal Models of Addiction: An Emphasis on Alcohol-Related Behaviors. ACS Chem. Neurosci. 2018, 9, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Berthold, H.K.; Campesi, I.; Carrero, J.J.; Dakal, S.; Franconi, F.; Gouni-Berthold, I.; Heiman, M.L.; Kautzky-Willer, A.; Klein, S.L.; et al. Sex- and Gender-Based Pharmacological Response to Drugs. Pharmacol. Rev. 2021, 73, 730–762. [Google Scholar] [CrossRef] [PubMed]
- McKay, J.R. Studies of factors in relapse to alcohol, drug and nicotine use: A critical review of methodologies and findings. J. Stud. Alcohol 1999, 60, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Felton, J.W.; Collado, A.; Shadur, J.M.; Lejuez, C.W.; MacPherson, L. Sex differences in self-report and behavioral measures of disinhibition predicting marijuana use across adolescence. Exp. Clin. Psychopharmacol. 2015, 23, 265–274. [Google Scholar] [CrossRef]


{kind=link}
| Women | Men | p | |
|---|---|---|---|
| n (%) | 66 (19.0) | 282 (81.0) | - |
| Mean age in years (SD) | 50.5 (9.0) | 47.6 (9.5) | 0.02 |
| Civil status | |||
| Single n (%) | 15 (22.7) | 134 (47.5) | <0.01 |
| Married n (%) | 24 (36.4) | 88 (31.2) | 0.46 |
| Separated or widowed n (%) | 27 (40.9) | 60 (21.3) | <0.01 |
| Education | |||
| ≤8 years n (%) | 35 (53.0) | 178 (63.1) | 0.13 |
| >8 years n (%) | 31 (47.0) | 104 (36.9) | 0.13 |
| Employment status | |||
| Employed n (%) | 38 (57.6) | 159 (56.4) | 0.89 |
| Unemployed n (%) | 15 (22.7) | 68 (24.1) | 0.87 |
| Retired n (%) | 13 (19.7) | 55 (19.5) | 1.00 |
| Family history | |||
| Father with AUD n (%) | 21 (36.4) | 65 (23.0) | 0.15 |
| Mother with AUD n (%) | 11 (16.7) | 6 (2.1) | <0.01 |
| Spouse with AUD n (%) | 8 (12.1) | 6 (2.1) | <0.01 |
| Comorbidity | |||
| Anxiety disorders n (%) | 59 (89.4) | 199 (70.6) | <0.01 |
| Depression n (%) | 56 (84.8) | 174 (61.7) | <0.01 |
| Substance Use Disorders n (%) | 13 (19.7) | 114 (40.4) | <0.01 |
| Smokers n (%) | 41 (62.1) | 209 (74.1) | 0.07 |
| Drinking characteristics | |||
| Severity of AUD | |||
| DSM-IV + criteria for alcohol dependence | 5.8 (1.5) | 5.7 (1.7) | 0.90 |
| Age at first drink in years | 16.8 (8.2) | 13.7 (4.8) | <0.01 |
| Age at onset of regular drinking in years | 26.0 (10.2) | 19.7 (6.4) | <0.01 |
| Age at onset of AUD in years | 35.8 (11.1) | 31.8 (10.8) | <0.01 |
| Age at first request for care in years | 44.1 (10.0) | 41.1 (10.2) | 0.07 |
| Lapse from regular use to AUD onset | 9.9 (10.7) | 12.2 (10.3) | 0.03 |
| Lapse from AUD onset to first request for care | 8.3 (7.8) | 9.3 (9.3) | 0.50 |
| Alcohol consumption the year before treatment | |||
| Number of drinks per drinking day | 13.0 (9.5) | 19.5 (18.1) | <0.01 |
| Number of drunk days per year | 187.5 (162.4) | 186.2 (164.8) | 0.76 |
| Severe medical consequences the year before treatment | |||
| Patients with at least 1 ER admission n (%) | 20 (30.3) | 88 (31.2) | 0.89 |
| Patients with at least 1 suicide attempt n (%) | 13 (19.7) | 23 (8.2) | <0.01 |
| Cohort | Number | Age at First Drink (Years) | Age at Onset of Regular Drinking (Years) | Age at Onset of AUD (Years) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ♀ | ♂ | ♀ | ♂ | Δ | p | ♀ | ♂ | Δ | p | ♀ | ♂ | Δ | p | |
| A (1937–1953) | 13 | 33 | 14.8 (6.6–22.9) | 14.5 (12.5–16.5) | 0.3 | 0.372 | 28.2 (20.7–35.7) | 20.6 (18.1–23.1) | 7.6 | 0.080 | 48.6 (42.9–54.4) | 38.2 (32.9–43.5) | 10.5 | 0.023 |
| B (1954–1963) | 24 | 107 | 18.8 (15.5–22.0) | 13.4 (12.5–14.4) | 5.3 | 0.002 | 27.4 (23.0–31.8) | 20.6 (19.2–22.0) | 6.8 | 0.001 | 36.6 (33.0–40.3) | 35.5 (33.5–37.5) | 1.1 | 0.612 |
| C (1964–1973) | 25 | 94 | 16.4 (14.3–18.4) | 14.2 (13.2–15.2) | 2.2 | 0.017 | 24.4 (20.7–28.1) | 19.6 (18.3–20.9) | 4.8 | 0.008 | 30.5 (27.1–33.8) | 29.7 (28.1–31.4) | 0.7 | 0.717 |
| D (1974–1991) | 4 | 48 | 14.0 (5.4–22.6) | 13.0 (12.0–14.0) | 1.0 | 0.277 | 19.8 (9.2–30.3) | 17.0 (16.0–18.0) | 2.8 | 0.489 | 23.0 (11.9–34.1) | 23.3 (21.6–25.0) | −0.3 | 0.916 |
| A (1937–1953) | 13 | 33 | 58.4 (54.5–62.3) | 53.4 (49.8–56.9) | 5.0 | 0.089 | 20.4 (11.9–28.9) | 17.5 (12.3–22.8) | 2.9 | 0.547 | 9.8 (4.2–15.4) | 15.4 (10.6–20.2) | −5.6 | 0.387 |
| B (1954–1963) | 24 | 107 | 44.6 (42.7–47.0) | 46.5 (45.3–47.7) | −1.9 | 0.128 | 9.3 (5.1–13.4) | 14.9 (12.8–17.0) | −5.6 | 0.010 | 8.0 (4.7–11.2) | 11.0 (9.1–12.8) | −3.0 | 0.113 |
| C (1964–1973) | 25 | 94 | 38.7 (36.3–41.1) | 37.0 (35.8–38.3) | 1.7 | 0.265 | 6.1 (3.6–8.6) | 10.2 (8.6–11.7) | −4.1 | 0.013 | 8.2 (4.9–11.5) | 7.3 (5.8–8.8) | 0.9 | 0.734 |
| D (1974–1991) | 4 | 48 | 28.8 (20.2–37.3) | 28.9 (27.4–30.3) | −0.1 | 0.891 | 3.3 (1.3–5.3) | 6.4 (5.1–7.7) | −3.1 | 0.126 | 5.8 (1.0–10.5) | 5.4 (3.9–6.8) | 0.4 | 0.492 |
| Reference | N | Age in Years Mean (SD) | Civil Status (%) | Familial History (%) | Comorbidity (%) | Age at First Drink in Years Mean (SD) | Age at Onset of Regular Use in Years Mean (SD) | Age at Onset of AUD in Years Mean (SD) | Age at First Request for Care in Years Mean (SD) | Lapse from Regular Use to AUD Onset in Years Mean (SD) | Lapse from AUD Onset to First Request of Care in Years Mean (SD) | g/day Mean (SD) | DSM-IV Criteria for AD Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agabio et al., Outpatient Sardinia, Italy | 66 ♀: 282 ♂ | ♀: 50.5 (9.0) ♂: 47.6 (9.5) p = 0.02 | Single ♀: 22.7 ♂: 47.5 p < 0.01 | Mother with AUD ♀: 16.7; ♂: 2.1 Spouse with AUD ♀: 12.1; ♂: 2.1 p < 0.01 | Anxiety ♀: 89.4 ♂: 70.6 SUDs ♀: 19.7 ♂: 40.4 p < 0.01 | ♀: 16.8 (8.2) ♂: 13.7 (4.8) p < 0.01 | ♀: 26.0 (10.2) ♂: 19.7 (6.4) p < 0.01 | ♀: 35.8 (11.1) ♂: 31.8 (10.8) p < 0.01 | ♀: 44.1 (10.0) ♂: 41.1 (10.2) p = 0.07 | ♀: 9.9 (10.7) ♂: 12.2 (10.3) p = 0.03 | ♀: 8.3 (7.8) ♂: 9.3 (9.3) p = 0.50 | ♀: 156 (114) ♂: 234 (217.2) p < 0.01 | ♀: 5.8 (1.5) ♂: 5.7 (1.7) p = 0.90 |
| Alvanzo et al., 2014 Alcohol-related services US [34] | 3311 ♂ and ♀ age < 45 years | NR | NR | NR | NR | NR | NR | NR | ♀: 23.1 (22.0–24.3) ♂: 24.9 (24.2–25.6) p < 0.05 | NR | ♀: 7.6 (6.6–8.6) ♂: 9.3 (8.6–10.0) p < 0.05 | NR | NR |
| Ashley et al., 1977 Inpatient Canada [66] | 85 ♀ 630 ♂ | ♀: 44.8 (10.2) ♂: 45.8 (10.2) p > 0.05 | NR | NR | NR | ♀: 18.7 (4.3) ♂: 17.2 (3.7) p < 0.01 | NR | ♀: 30.5 (10.5) ♂: 25.4 (8.5) p < 0.01 | ♀: 40.5 (9.5) ♂: 39.9 (9.1) p > 0.05 | NR | ♀: 14.1 (8.5) ♂: 20.2 (9.3) p < 0.01 | ♀: 227.6 (103.5) ♂: 316 (119.7) p < 0.01 | NR |
| Blankfield, 1990. In and outpatient Australia [38] | 52 ♀ 104 ♂ | ♀: 45 (NR) ♂: 44.0 (NR) p = NR | Single ♀: 18 ♂: 27 p = NR | Positive parental history ♀: 37.9; ♂: 40.2 p > 0.05 | NR | ♀: 19.3 (NR) ♂: 15.0 (NR) p = NR | ♀: 27.5 (NR) ♂: 19.3 (NR) p < 0.001 | ♀: 35.0 (NR) ♂: 31.5 (NR) p = NR | NR | ♀:16.1 (NR) ♂: 24.0 (NR) p = NR | ♀: 8.5 (NR) ♂: 11.6 (NR) p < 0.001 | ♀: 210 (NR) ♂: 279 (NR) p < 0.001 | NR |
| Dahlgren, 1978 Inpatients Sweden [68] | 100 ♀ 100 ♂ | ♀: 40.5 (11.9) ♂: 41.0 (11.3) p > 0.05 | Single ♀: 22 ♂: 25 p = NR | Mother with AUD ♀: 4; ♂: 5 p > 0.05 Spouse with AUD ♀: 51; ♂: 13 p < 0.001 | NR | ♀: 21.2 (5.8) ♂: 17.0 (2.3) p < 0.001 | ♀: 27.2 (8.5) ♂: 23.1 (6.6) p < 0.001 | ♀: 34.9 (11.2) ♂: 30.8 (8.8) p < 0.01 | NR | ♀: 6.0 (5.6) ♂: 8.0 (5.7) p < 0.01 | ♀: 5.9 (4.7) ♂: 8.2 (5.7) p < 0.05 | NR | NR |
| Diehl et al., 2007 Inpatient Germany [36] | 106 ♀ 106 ♂ | ♀: 41.6 (8.4) ♂: 41.9 (8.6) p > 0.05 | NR | NR | NR | ♀: 15.8 (4.4) ♂: 14.5 (4.0) p = 0.02 | ♀: 25.3 (7.8) ♂: 20.1 (4.7) p < 0.001 | ♀: 35.4 (8.6) ♂: 31.7 (8.5) p = 0.01 | Inpatient treatment ♀: 39.9 (8.6) ♂: 39.6 (9.3) p > 0.05 | ♀: 10.0 (4.1) ♂: 11.6 (4.2) p = 0.047 | Inpatient treatment ♀: 4.5 (4.8) ♂: 7.9 (6.7) p < 0.001 | ♀: 153.0 (78.6) ♂:182.8 (103.7) p = 0.02 | NR |
| Dunne et al., 1993 Unclear UK [37] | 121 ♀ 121 ♂ | ♀: 42.2 (10.1) ♂: 42.5 (9.3) p > 0.05 | Single ♀: 13 ♂: 16 p NR | Positive parental history ♀: 35; ♂: 13 p < 0.05 | Anxiety ♀: 46 ♂: 22 p < 0.001 Depression ♀: 37 ♂: 14 p < 0.01 | NR | Median (CI) ♀: 25 (12–61) ♂: 19 (12–55) p NR | NR | NR | ♀: 9.2 (NR) ♂: 9.6 (NR) p > 0.05 | NR | ♀: 201.1 (NR) ♂: 301.7 (NR) p NR | NR |
| Hernandez-Avila et al., 2004 In and outpatient US [23] | 41 ♀ 42 ♂ | NR | NR | NR | NR | NR | ♀: 20.3 (7.1) ♂: 18.0 (6.4) p > 0.05 | ♀: 20.6 (6.9) ♂: 19.0 (9.6) p > 0.05 | NR | NR | ♀: NR (NR) ♂: NR (NR) p < 0.01 | NR p > 0.05 | NR p > 0.05 |
| Hesselbrock et al., 1985 Inpatient US [67] | 90 ♀ 231 ♂ | ♀: 37.3 (11.0) ♂: 39.5 (12.0) p > 0.05 | Single ♀: 22 ♂: 30 p = NR | NR | Depression ♀: 52 ♂: 32 SUDs ♀: 38 ♂: 45 p NR | ♀: 15.4 (NR) ♂: 14.1 (NR) p < 0.05 | NR | ♀: 30.0 (NR) ♂: 31.5 (NR) p > 0.05 | ♀: 33.1 (NR) ♂: 35.6 (NR) p = 0.07 | NR | ♀: 7.4 (11.0) ♂: 15.0 (12.0) p < 0.05 | NR | NR |
| Holdcraft and Iacono, 2002a Earlier-born cohort Data NR US [24] | 37 ♀ 261 ♂ | ♀: 44.1 (3.3) ♂: 46.5 (4.5) p < 0.001 | NR | NR | NR | NR | NR | ♀: 20.5 (4.5) ♂: 18.6 (3.6) p < 0.05 | NR | NR | NR | NR | ♀: 4.4 (1.6) ♂: 4.8 (1.7) p > 0.05 |
| Holdcraft and Iacono, 2002b Later-born cohort community-based sample US [24] | 95 ♀ 207♂ | ♀: 36.2 (3.5) ♂: 37.6 (3.6) p < 0.01 | NR | NR | NR | NR | NR | ♀:17.0 (3.1) ♂: 17.5 (2.6) p > 0.05 | NR | NR | NR | NR | ♀: 4.5 (1.6) ♂: 4.8 (1.7) p > 0.05 |
| Khan et al., 2013 National survey US [6] | 1807 ♀ 2974 ♂ | NR | Single ♀: 27.6 ♂: 29.5 p > 0.05 | Positive parental history ♀: 60.2 ♂: 50.5 p < 0.05 Spouse with AUD ♀: 38.8 ♂: 13.3 p < 0.05 | Depression ♀: 33.1 ♂: 16.8 Anxiety ♀: 44.3 ♂: 26.2 SUDs ♀: 62.6 ♂: 64.3 p < 0.05 | ♀: 17.4 (17.1–17.7) ♂: 16.6 (16.4–16.7) p < 0.0001 | NR | ♀: 24.4 (23.8–24.9) ♂: 23.9 (23. 5–24.3) p = 0.1402 | NR | NR | NR | NR | NR |
| Keyes et al., 2010a US Data of 2 national surveys Total sample [5] | 30.125 ♀ 23.113 ♂ | NR | NR | NR | NR | NR | Age at initiation of use ♀: 19.0 (0.04 SE) ♂: 17.8 (0.03 SE) p < 0.001 | NR | NR | From use to AUD ♀: 5.6 (0.15 SE) ♂: 5.8 (0.12 SE) p > 0.05 | ♀: 6.1 (0.4 SE) ♂: 7 (0.3 SE) p < 0.05 | NR | NR |
| Keyes et al., 2010b US Born 1974–1983 [5] | 3292 ♀ 2553 ♂ | NR | NR | NR | NR | NR | Age at initiation of use ♀: 17.5 (0.09 SE) ♂: 17.1 (0.08 SE) p < 0.001 | NR | NR | From use to AUD ♀: 3.1 (0.17 SE) ♂: 2.8 (0.12 SE) p > 0.05 | ♀: 5.1 (0.4 SE) ♂: 5.4 (0.4 SE) p > 0.05 | NR | NR |
| Keyes et al., 2010c US Born 1964–1973 [5] | 7.759 ♀ 5.796 ♂ | NR | NR | NR | NR | NR | Age at initiation of use ♀: 18.5 (0.06 SE) ♂: 17.5 (0.05 SE) p < 0.001 | NR | NR | From use to AUD ♀: 3.7 (0.16 SE) ♂: 4.2 (0.16 SE) p < 0.05 | ♀: 8.1 (0.6 SE) ♂: 8.1 (0.4 SE) p > 0.05 | NR | NR |
| Keyes et al., 2010d US Born 1954–1963 [5] | 9.291 ♀ 7.038 ♂ | NR | NR | NR | NR | NR | Age at initiation of use ♀: 20.5 (0.09 SE) ♂: 18.4 (0.06 SE) p < 0.001 | NR | NR | From use to AUD ♀: 5.5 (0.31 SE) ♂: 6.4 (0.21 SE) p > 0.05 | ♀: 14.1 (0.5 SE) ♂: 14.8 (0.7 SE) p > 0.05 | NR | NR |
| Keyes et al., 2010e US Born 1944–1953 [5] | 7.209 ♀ 5.697 ♂ | NR | NR | NR | NR | NR | Age at initiation of use ♀: 22.1 (0.22 SE) ♂: 19.1 (0.12 SE) p < 0.001 | NR | NR | From use to AUD ♀: 8.6 (0.44 SE) ♂: 7.9 (0.28 SE) p > 0.05 | ♀: 18.5 (1.1 SE) ♂: 20.0 (0.6 SE) p > 0.05 | NR | NR |
| Keyes et al., 2010f US Born 1934–1943 [5] | 2.574 ♀ 2.029 ♂ | NR | NR | NR | NR | NR | NR | NR | NR | From use to AUD ♀: 11.8 (0.87 SE) ♂: 10.4 (0.63 SE) p > 0.05 | ♀: 19.4 (1.4 SE) ♂: 23.5 (0.9 SE) p < 0.001 | NR | NR |
| Lewis and Nixon, 2014 Inpatient US [27] | 257 ♀ 274 ♂ | ♀: 33.1 (9.9) ♂: 38.5 (11.1) p < 0.001 | NR | Positive parental history ♀: 73.1 ♂: 60.6 P < 0.05 Spouse with AUD ♀: 65.2 ♂: 25.0 p < 0.05 | NR | ♀: 12.6 (4.6) ♂: 11.5 (3.9) p = 0.007 | ♀: 18.8 (6.0) ♂: 17.6 (4.1) p > 0.05 | ♀: 21.1 (7.6) ♂: 21.5 (8.4) p > 0.05 | ♀: 31.6 (9.2) ♂: 35.1 (10.1) p = 0.007 | ♀: 3.1 (4.9) ♂: 4.5 (6.2) p > 0.05 | ♀: 10.3 (9.0) ♂: 14.5 (9.8) p < 0.05 | NR | NR |
| Piazza et al., 1989 Outpatient and self-help groups US [29] | 33 ♀ 105 ♂ | ♀: 59.3 (8.9) ♂: 63.4 (8.8) NR | NR | NR | NR | ♀: 17.5 (2.2) ♂: 15.7 (4.1) p = 0.002 | NR | ♀: 34.3 (11.3) ♂: 32.1 (14.7) p > 0.05 | ♀: 43.7 (12.7) ♂: 45.8 (15.3) p > 0.05 | NR | ♀: 10.4 (7.9) ♂: 14.7 (12.6) p = 0.017 | NR | NR |
| Picci et al., 2012 Inpatient Turin, Italy [69] | 56 ♀ 150 ♂ | ♀: 45.4 (12.1) ♂: 46.3 (10.1) p < 0.05 | Single ♀: 23.2 ♂: 37.3 p < 0.05 | Positive parental history ♀: 62.5 ♂: 45.6 p < 0.05 | SUDs ♀: 23.2 ♂: 37.3 p < 0.05 | NR | ♀: 25.9 (11.3) ♂: 21.6 (8.3) p < 0.05 | ♀: 34.7 (11.4) ♂: 36.3 (11.0) p < 0.05 | NR | ♀: 9 (NR) ♂: 15 (NR) p < 0.05 | NR | NR | NR |
| Randall et al., 1999 Outpatient US [30] | 231 ♀ 634 ♂ | ♀: 38.3 (10.7) ♂: 38.5 (10.5) p > 0.05 | NR | NR | NR | NR | NR for outpatients | NR for outpatients | NR for outpatients | NR for outpatients | NR for outpatients | NR for outpatients | DSM III (max 9) ♀: 5.9 (1.8) ♂: 5.9 (1.9) p > 0.05 |
| Randall et al., 1999 Outpatient US entire sample [30] | 1589 ♀ 1210 ♂ | NR for the entire sample | NR | NR | NR | NR | ♀: 26.6 (10.3) ♂: 22.7 (9.0) p < 0.001 | Worst problems ♀: 35.2 (10.9) ♂: 35.0 (10.9) p > 0.05 | NR for the entire sample | NR for the entire sample | NR for the entire sample | NR for the entire sample | NR for the entire sample |
| Schuckit et al., 1995 Probants for COGA study US [31] | 161 ♀ 317 ♂ | 37.8 (12.6) NR ♀ and ♂ | NR | NR | NR | NR | ♀: 18.5 (5.3) ♂: 17.5 (4.8) p = 0.04 | NR | ♀: 30.1 (8.9) ♂: 32.5 (11.7) p = 0.08 | NR | NR | NR | NR |
| Schuckit et al., 1998 Probants for COGA study US 1 drink = 14 g [32] | 1.085♀ 2.120 ♂ | ♀: 36.9 (10.8) ♂: 39.3 (12.7) p < 0.001 | Single ♀: 26.9 ♂: 33.3 p < 0.001 | NR | ♀ > ♂ Mood and anxiety ♀ < ♂ SUDs | NR | ♀: 18.5 (6.5) ♂: 17.0 (4.2) p < 0.001 | ♀: 25.2 (9.3) ♂: 24.2 (8.5) p < 0.001 | ♀: 31.0 (9.5) ♂: 31.7 (10.7) p < 0.001 | NR | ♀: 3.8 (6.0) ♂: 6.4 (8.1) p = 0.01 | Maximum amount per day ♀: 280 (221.2) ♂: 446.6 (315) p < 0.01 | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agabio, R.; Pisanu, C.; Minerba, L.; Gessa, G.L.; Franconi, F. Gender Differences among Sardinians with Alcohol Use Disorder. J. Clin. Med. 2021, 10, 4688. https://doi.org/10.3390/jcm10204688
Agabio R, Pisanu C, Minerba L, Gessa GL, Franconi F. Gender Differences among Sardinians with Alcohol Use Disorder. Journal of Clinical Medicine. 2021; 10(20):4688. https://doi.org/10.3390/jcm10204688
Chicago/Turabian StyleAgabio, Roberta, Claudia Pisanu, Luigi Minerba, Gian Luigi Gessa, and Flavia Franconi. 2021. "Gender Differences among Sardinians with Alcohol Use Disorder" Journal of Clinical Medicine 10, no. 20: 4688. https://doi.org/10.3390/jcm10204688
APA StyleAgabio, R., Pisanu, C., Minerba, L., Gessa, G. L., & Franconi, F. (2021). Gender Differences among Sardinians with Alcohol Use Disorder. Journal of Clinical Medicine, 10(20), 4688. https://doi.org/10.3390/jcm10204688