
Change of Renal Gallium Uptake Correlated with Change of Inflammation Activity in Renal Pathology in Lupus Nephritis Patients

 ,
,  , ,
, , 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Parameters
2.3. Renal Histology
2.4. Gallium-67 Renal Scintigraphy
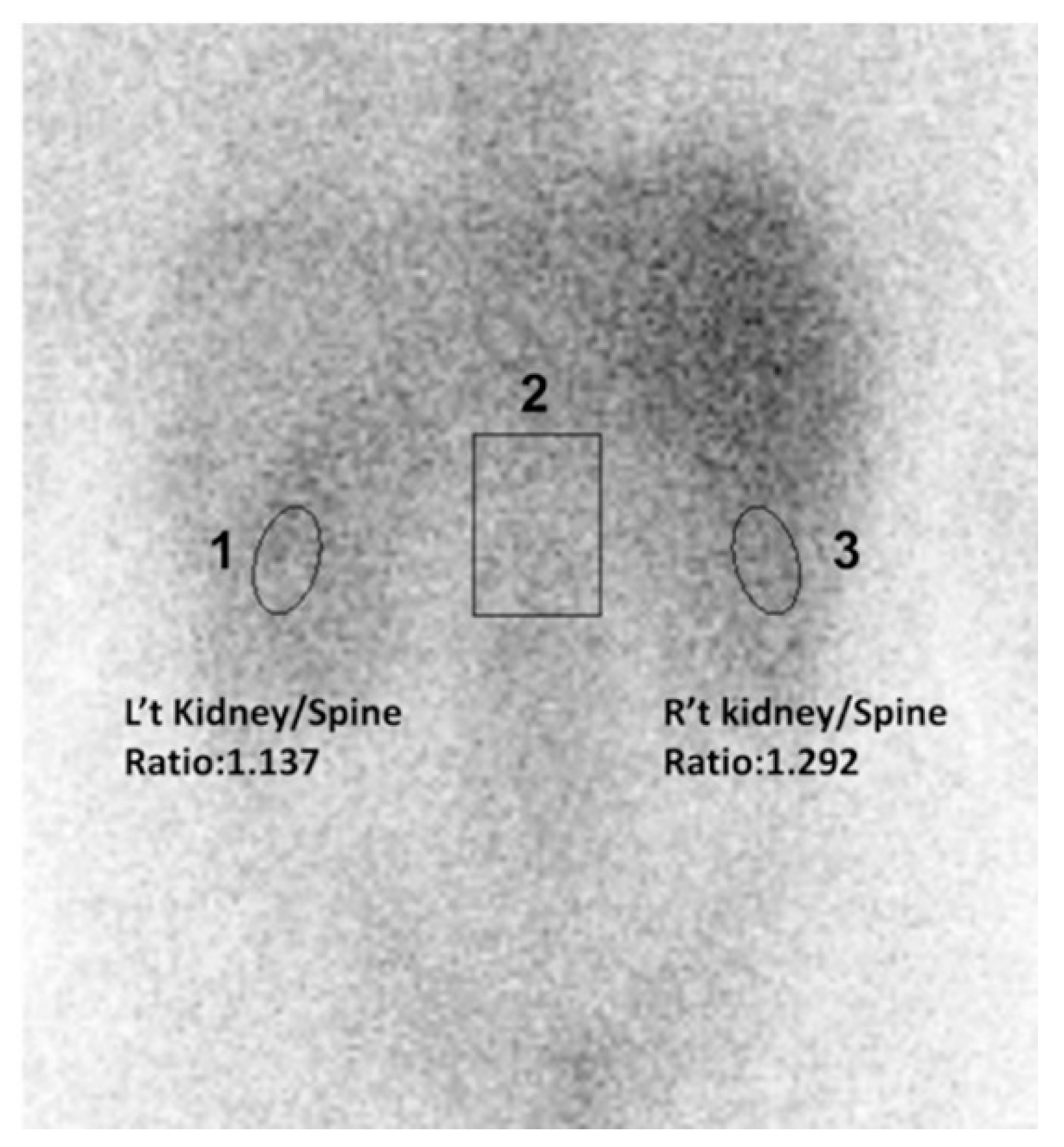
2.5. Semi-Quantitative Method of Gallium Renal Scintigraphy
2.6. Patient and Public Involvement
2.7. Statistical Analysis
3. Results
3.1. Demographic Data of Enrolled LN Patients by Pathological Classification
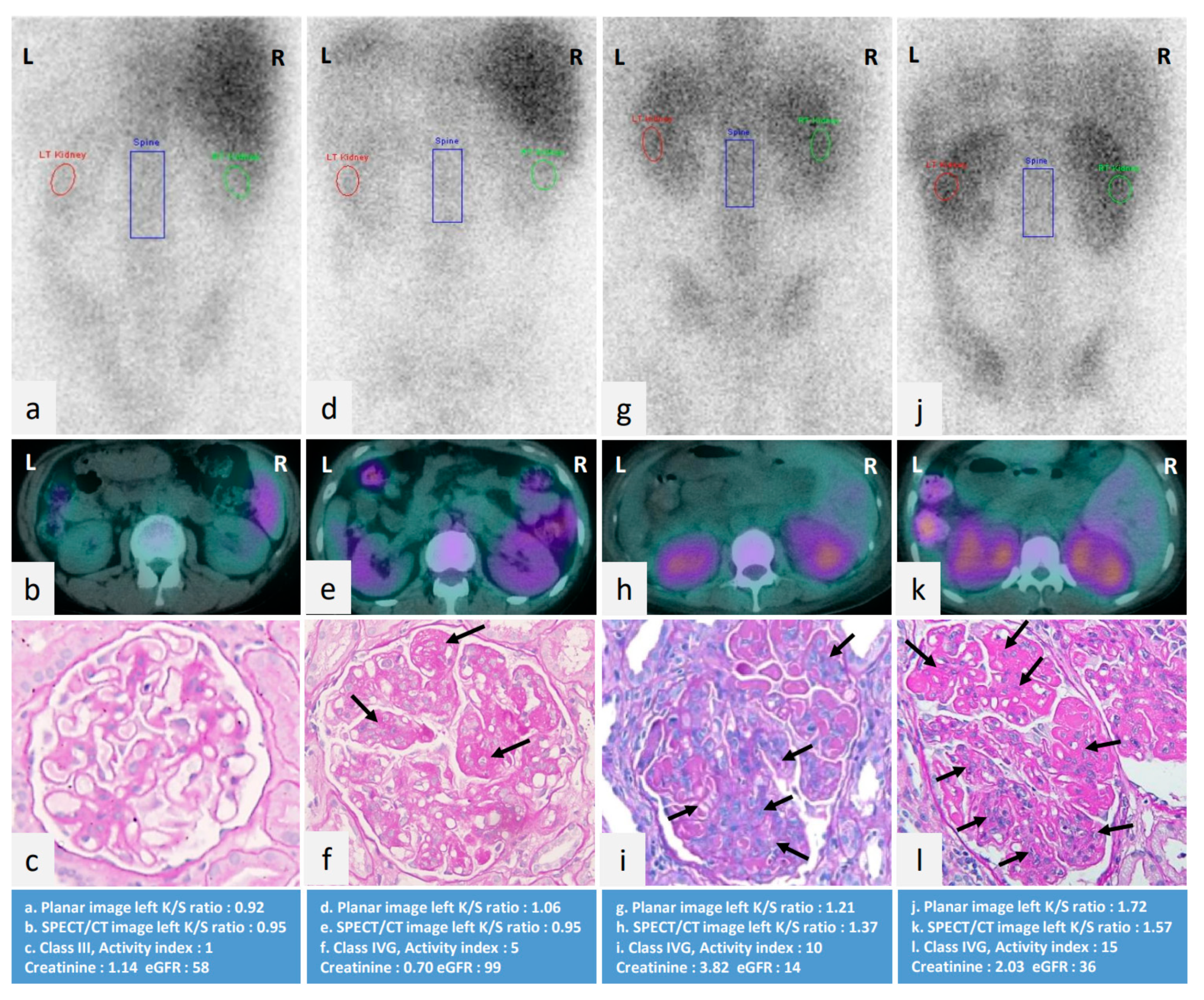
3.2. Factors Associated with Renal Gallium Uptake
3.3. Comparisons of Clinical Variables of LN Patients Receiving Repeat Renal Biopsies
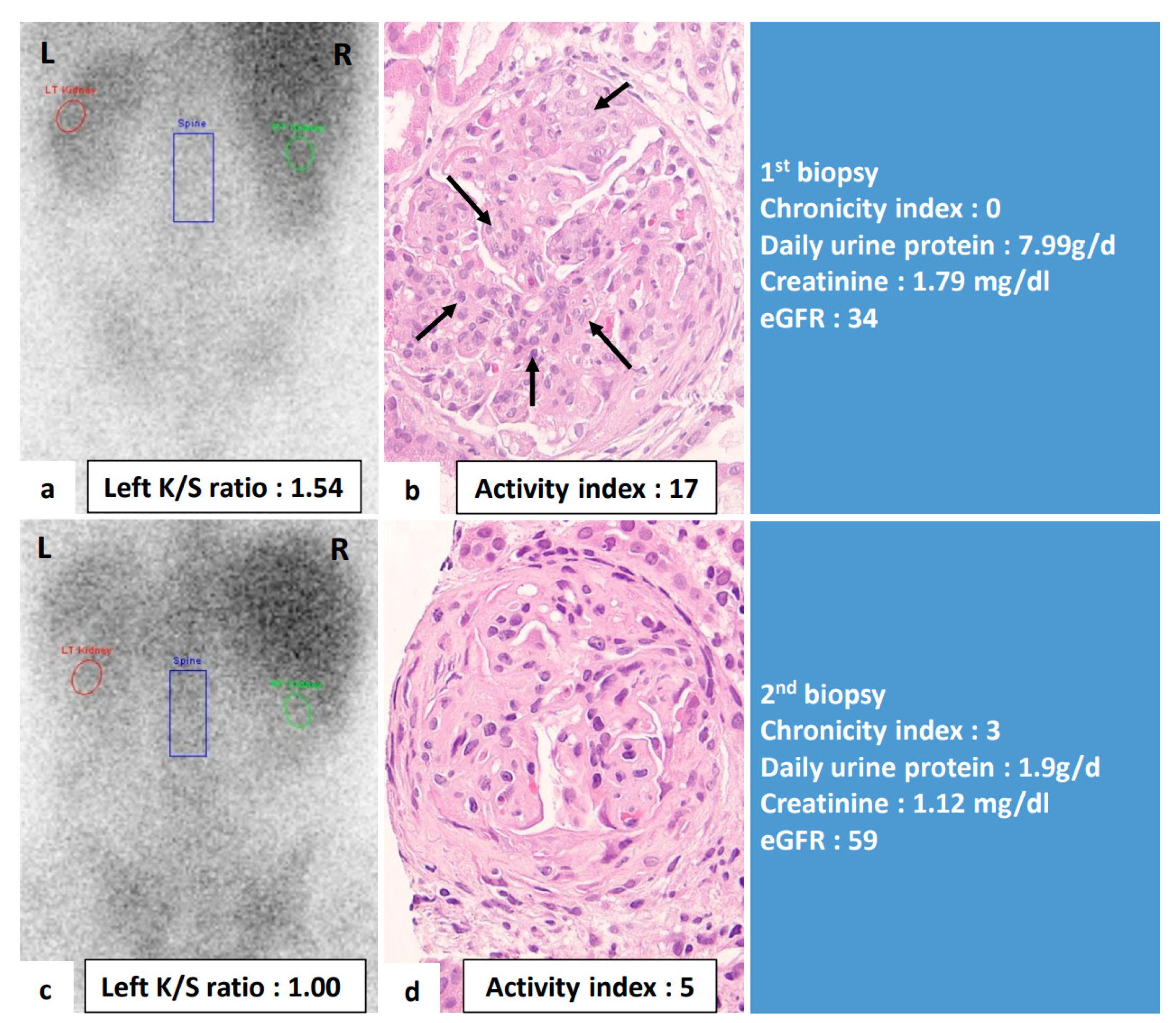
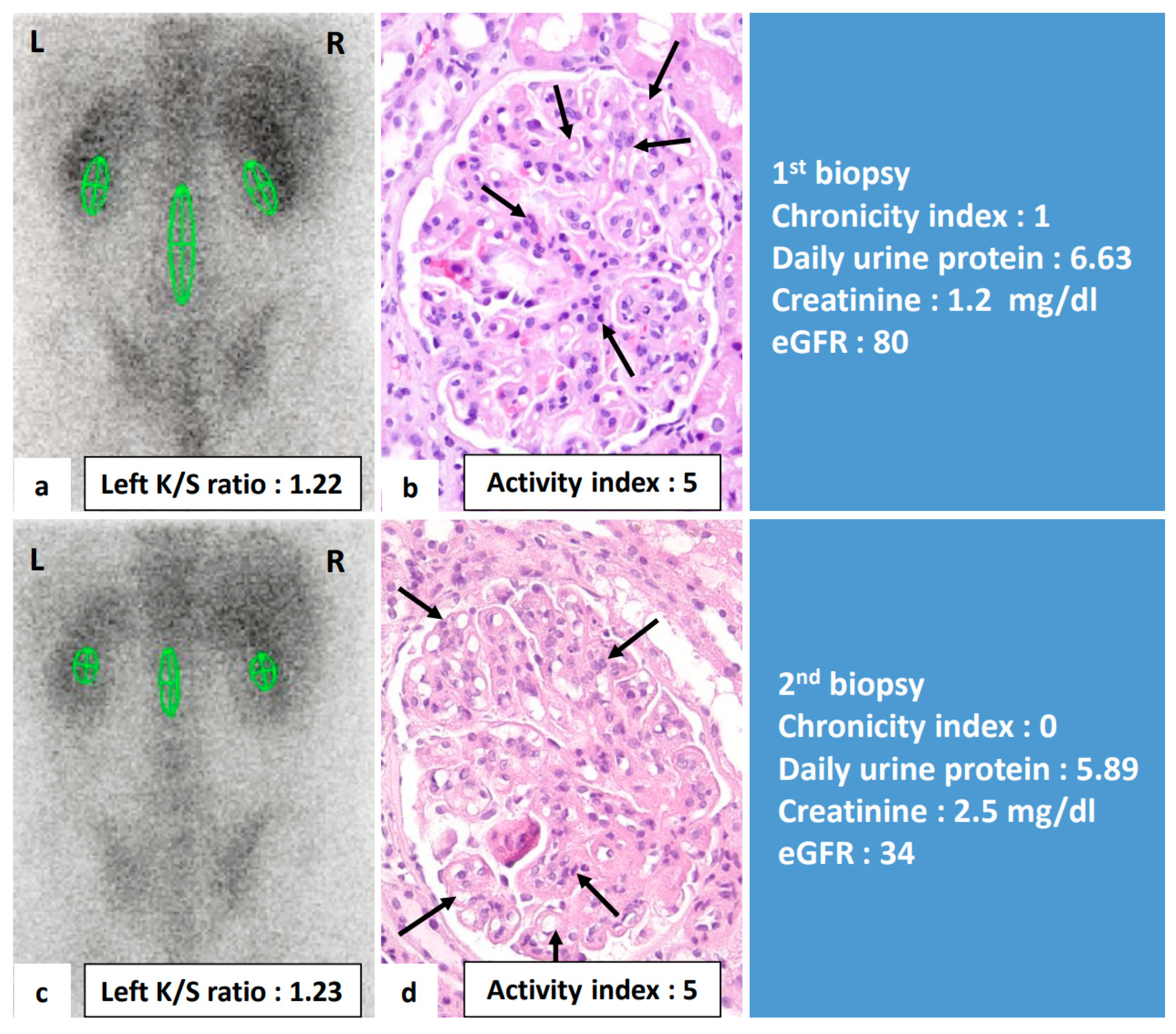
3.4. Correlation between Changes of Renal Gallium Uptake and Changes of Clinical Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almaani, S.; Meara, A.; Rovin, B.H. Update on Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 825–835. [Google Scholar] [CrossRef]
- Houssiau, F.A.; Vasconcelos, C.; D’Cruz, D.; Sebastiani, G.D.; Garrido, E.D.R.; Danieli, M.G.; Abramovicz, D.; Blockmans, D.; Mathieu, A.; Direskeneli, H.; et al. Early response to immunosuppressive therapy predicts good renal outcome in lupus nephritis: Lessons from long-term followup of patients in the Euro-Lupus Nephritis Trial. Arthritis Rheum. 2004, 50, 3934–3940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladman, D.D.; Urowitz, M.B.; Cole, E.; Ritchie, S.; Chang, C.H.; Churg, J. Kidney Biopsy in SLE. I. A Clinical-Morphologic Evaluation. QJM Int. J. Med. 1989, 73, 1125–1133. [Google Scholar]
- Nossent, J.C.; Henzen-Logmans, S.C.; Vroom, T.M.; Huysen, V.; Berden, J.H.; Swaak, A.J. Relation between serological data at the time of biopsy and renal histology in lupus nephritis. Rheumatol. Int. 1991, 11, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Hahn, B.H.; McMahon, M.A.; Wilkinson, A.; Wallace, W.D.; Daikh, D.I.; FitzGerald, J.; Karpouzas, G.A.; Merrill, J.T.; Wallace, D.J.; Yazdany, J.; et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Rheum. 2012, 64, 797–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corapi, K.M.; Chen, J.L.; Balk, E.M.; Gordon, C.E. Bleeding complications of native kidney biopsy: A systematic review and meta-analysis. Am. J. Kidney Dis. 2012, 60, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, K.; Sasaki, K.; Yamato, M.; Rakugi, H.; Isaka, Y.; Hayashi, T. Tubulointerstitial nephritis and uveitis syndrome with transient hyperthyroidism in an elderly patient. Clin. Exp. Nephrol. 2011, 15, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Joaquim, A.I.; Mendes, G.E.; Ribeiro, P.F.; Baptista, M.A.; Burdmann, E.A. Ga-67 scintigraphy in the differential diagnosis between acute interstitial nephritis and acute tubular necrosis: An experimental study. Nephrol. Dial. Transplant. 2010, 25, 3277–3282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.Y.; Lan, J.L.; Wang, S.J. Gallium-67 scintigraphy to predict response to therapy in active lupus nephritis. J. Nucl. Med. 1998, 39, 2137–2141. [Google Scholar]
- Lin, W.Y.; Lan, J.L.; Cheng, K.Y.; Wang, S.J. Value of gallium-67 scintigraphy in monitoring the renal activity in lupus nephritis. Scand. J. Rheumatol. 1998, 27, 42–45. [Google Scholar]
- Lin, W.Y.; Hsieh, J.F.; Tsai, S.C.; Lan, J.L.; Cheng, K.Y.; Wang, S.J. Semi-quantitative evaluation of gallium-67 scintigraphy in lupus nephritis. Eur. J. Nucl. Med. 2000, 27, 1626–1631. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; Ferrario, F.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. J. Am. Soc. Nephrol. 2004, 15, 241–250. [Google Scholar] [CrossRef]
- Austin, H.A., 3rd; Boumpas, D.T.; Vaughan, E.M.; Balow, J.E. Predicting renal outcomes in severe lupus nephritis: Contributions of clinical and histologic data. Kidney Int. 1994, 45, 544–550. [Google Scholar] [CrossRef] [Green Version]
- Contreras, G.; Pardo, V.; Cely, C.; Borja, E.; Hurtado, A.; De La Cuesta, C.; Iqbal, K.; Lenz, O.; Asif, A.; Nahar, N.; et al. Factors associated with poor outcomes in patients with lupus nephritis. Lupus 2005, 14, 890–895. [Google Scholar] [CrossRef]
- Zappitelli, M.; Duffy, C.M.; Bernard, C.; Gupta, I.R. Evaluation of activity, chronicity and tubulointerstitial indices for childhood lupus nephritis. Pediatr. Nephrol. 2008, 23, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Seabold, J.E.; Palestro, C.J.; Brown, M.L.; Datz, F.L.; Forstrom, L.A.; Greenspan, B.S.; McAfee, J.G.; Schauwecker, D.S.; Royal, H.D. Procedure guideline for gallium scintigraphy in inflammation. Society of Nuclear Medicine. J. Nucl. Med. 1997, 38, 994–997. [Google Scholar] [PubMed]
- Wood, B.C.; Sharma, J.N.; Germann, D.R.; Wood, W.G.; Crouch, T.T. Gallium citrate Ga 67 imaging in noninfectious interstitial nephritis. Arch. Intern. Med. 1978, 138, 1665–1666. [Google Scholar] [CrossRef] [PubMed]
- Bakir, A.A.; Lopez-Majano, V.; Hryhorczuk, D.O.; Rhee, H.L.; Dunea, G. Appraisal of lupus nephritis by renal imaging with gallium-67. Am. J. Med. 1985, 79, 175–182. [Google Scholar] [CrossRef]
- Daleboudt, G.M.; Bajema, I.M.; Goemaere, N.N.; van Laar, J.M.; Bruijn, J.A.; Berger, S.P. The clinical relevance of a repeat biopsy in lupus nephritis flares. Nephrol. Dial. Transplant. 2009, 24, 3712–3717. [Google Scholar] [CrossRef] [Green Version]
- Esdaile, J.M.; Joseph, L.; MacKenzie, T.; Kashgarian, M.; Hayslett, J.P. The pathogenesis and prognosis of lupus nephritis: Information from repeat renal biopsy. Semin. Arthritis Rheum. 1993, 23, 135–148. [Google Scholar] [CrossRef]
- Zickert, A.; Sundelin, B.; Svenungsson, E.; Gunnarsson, I. Role of early repeated renal biopsies in lupus nephritis. Lupus Sci. Med. 2014, 1, e000018. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, S.; Albert, L.; Gladman, D.D.; Urowitz, M.B.; Hallett, D.C.; Ritchie, S. Serial renal biopsy in systemic lupus erythematosus. J. Rheumatol. 2000, 27, 2822–2826. [Google Scholar] [PubMed]
- Mok, C.C. Biomarkers for lupus nephritis: A critical appraisal. J. Biomed. Biotechnol. 2010, 2010, 638413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, G.S.; Delahousse, M.; Nochy, D.; Remy, P.; Mignon, F.; Mery, J.P.; Bariéty, J. Predictive power of the second renal biopsy in lupus nephritis: Significance of macrophages. Kidney Int. 2001, 59, 304–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunnarsson, I.; Sundelin, B.; Heimburger, M.; Forslid, J.; van Vollenhoven, R.; Lundberg, I.; Jacobson, S.H. Repeated renal biopsy in proliferative lupus nephritis–predictive role of serum C1q and albuminuria. J. Rheumatol. 2002, 29, 693–699. [Google Scholar]
- Askenazi, D.; Myones, B.; Kamdar, A.; Warren, R.; Perez, M.; De Guzman, M.; Minta, A.; Hicks, M.J.; Kale, A. Outcomes of children with proliferative lupus nephritis: The role of protocol renal biopsy. Pediatr. Nephrol. 2007, 22, 981–986. [Google Scholar] [CrossRef]
- Alvarado, A.; Malvar, A.; Lococo, B.; Alberton, V.; Toniolo, F.; Nagaraja, H.; Rovin, B. The value of repeat kidney biopsy in quiescent Argentinian lupus nephritis patients. Lupus 2014, 23, 840–847. [Google Scholar] [CrossRef]
- Singh, A.; Ghosh, R.; Kaur, P.; Golay, V.; Pandey, R.; Roychowdhury, A. Protocol renal biopsy in patients with lupus nephritis: A single center experience. Saudi J. Kidney Dis. Transpl. 2014, 25, 801–807. [Google Scholar] [CrossRef]
- Malvar, A.; Pirruccio, P.; Alberton, V.; Lococo, B.; Recalde, C.; Fazini, B.; Nagaraja, H.; Indrakanti, D.; Rovin, B.H. Histologic versus clinical remission in proliferative lupus nephritis. Nephrol. Dial. Transplant. 2017, 32, 1338–1344. [Google Scholar] [CrossRef]
- Alsuwaida, A.; Husain, S.; Alghonaim, M.; AlOudah, N.; Alwakeel, J.; Ullah, A.; Kfoury, H. Strategy for second kidney biopsy in patients with lupus nephritis. Nephrol. Dial. Transplant. 2011, 27, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Stoenoiu, M.S.; Aydin, S.; Tektonidou, M.; Ravelingien, I.; le Guern, V.; Fiehn, C.; Remy, P.; Delahousse, M.; Petera, P.; Quémeneur, T.; et al. Repeat kidney biopsies fail to detect differences between azathioprine and mycophenolate mofetil maintenance therapy for lupus nephritis: Data from the MAINTAIN Nephritis Trial. Nephrol. Dial. Transplant. 2012, 27, 1924–1930. [Google Scholar] [CrossRef] [Green Version]
- Grootscholten, C.; Bajema, I.M.; Florquin, S.; Steenbergen, E.J.; Peutz-Kootstra, C.J.; Goldschmeding, R.; Bijl, M.; Hagen, E.C.; van Houwelingen, H.C.; Derksen, R.H.W.M.; et al. Treatment with cyclophosphamide delays the progression of chronic lesions more effectively than does treatment with azathioprine plus methylprednisolone in patients with proliferative lupus nephritis. Arthritis Rheum. 2007, 56, 924–937. [Google Scholar] [CrossRef]
- Moroni, G.; Pasquali, S.; Quaglini, S.; Banfi, G.; Casanova, S.; Maccario, M.; Zucchelli, P.; Ponticelli, C. Clinical and prognostic value of serial renal biopsies in lupus nephritis. Am. J. Kidney Dis. 1999, 34, 530–539. [Google Scholar] [CrossRef]
- Wang, G.B.; Xu, Z.J.; Liu, H.F.; Zhou, Q.G.; Zhou, Z.M.; Jia, N. Changes in pathological pattern and treatment regimens based on repeat renal biopsy in lupus nephritis. Chin. Med. J. 2012, 125, 2890–2894. [Google Scholar] [PubMed]
- Greloni, G.; Scolnik, M.; Marin, J.; Lancioni, E.; Quiroz, C.; Zacariaz, J.; Niveyro, P.D.L.I.; Christiansen, S.; Pierangelo, A.M.; Varela, C.F.; et al. Value of repeat biopsy in lupus nephritis flares. Lupus Sci. Med. 2014, 1, e000004. [Google Scholar] [CrossRef] [PubMed]
- Moroni, G.; Depetri, F.; Ponticelli, C. Lupus nephritis: When and how often to biopsy and what does it mean? J. Autoimmun. 2016, 74, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Akashi, Y.; Oshima, S.; Takeuchi, A.; Kubota, T.; Shimizu, J.; Shimizu, E.; Ishida, A.; Nakabayashi, I.; Nishiyama, J.; Tazawa, K.; et al. Identification and analysis of immune cells infiltrating into the glomerulus and interstitium in lupus nephritis. Nihon Rinsho Meneki Gakkai Kaishi. 1995, 18, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsan, M.F. Mechanism of gallium-67 accumulation in inflammatory lesions. J. Nucl. Med. 1985, 26, 88–92. [Google Scholar] [PubMed]
- Soliman, S.; Mohan, C. Lupus nephritis biomarkers. Clin. Immunol. 2017, 185, 10–20. [Google Scholar] [CrossRef]
- Chen, Y.-M.; Hung, W.T.; Liao, Y.W.; Hsu, C.Y.; Hsieh, T.-Y.; Chen, H.H.; Hsieh, C.W.; Lin, C.T.; Lai, K.L.; Tang, K.T.; et al. Combination immunosuppressant therapy and lupus nephritis outcome: A hospital-based study. Lupus 2019, 28, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Yen, T.C.; Tzen, K.Y.; Chen, W.P.; Lin, C.Y. The value of Ga-67 renal SPECT in diagnosing and monitoring complete and incomplete treatment in children with acute pyelonephritis. Clin. Nucl. Med. 1999, 24, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, M.; Higashi, K.; Ohguchi, M.; Okimura, T.; Yamamoto, I. Gallium-67-citrate scintigraphy of primary renal lymphoma. Ann. Nucl. Med. 1998, 12, 51–53. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class I & II (n = 7) | III (n = 36) | IV (n = 134) | V (n = 60) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 42.0 (33.0–43.0) | 31.5 (25.3–40.0) | 32.0 (25.0–41.0) | 31.5 (26.0–39.5) | 0.586 |
| Female gender | 7 (100.0%) | 30 (83.3%) | 108 (80.6%) | 50 (83.3%) | 0.606 |
| Laboratory data | |||||
| Daily urine protein (gram) | 0.7 (0.1–1.8) | 1.9 (0.9–2.4) | 3.7 (2.1–5.8) | 2.3 (1.1–7.0) | <0.001 **‡§|| |
| Creatinine (mg/dL) | 0.7 (0.5–0.8) | 0.9 (0.6–1.2) | 1.4 (0.9–2.9) | 0.8 (0.7–1.1) | <0.001 **‡||†† |
| eGFR (mg/mL) | 97.5 (91.0–139.2) | 85.1 (63.5–118.4) | 51.7 (22.1–79.9) | 84.3 (60.7–117.1) | <0.001 **‡||†† |
| Anti-dsDNA (WHO units/mL) | 248.7 (166.5–477.0) | 174.3 (71.2–353.0) | 265.4 (125.5–464.1) | 130.4 (35.6–277.6) | <0.001 **†† |
| C3 (mg/dL) | 78.2 (71.3–90.5) | 77.4 (64.5–94.0) | 54.6 (39.4–66.7) | 63.8 (46.5–89.9) | <0.001 **||†† |
| C4 (mg/dL) | 15.1 (4.1–20.9) | 14.2 (10.6–22.1) | 10.2 (6.3–17.6) | 11.7 (6.5–23.5) | 0.045 *|| |
| Renal pathology | |||||
| Activity index | 0 (0–1) | 3 (1.0–3.8) | 8 (5.0–10.3) | 0 (0–2) | <0.001 **‡||†† |
| Cellular crescents | 0 (0–0) | 0 (0–0) | 2 (0–2) | 0 (0–0) | <0.001 **‡||†† |
| Fibrinoid necrosis/ Karyorrhexis | 0 (0–0) | 0 (0–2) | 2 (0–2) | 0 (0–0) | <0.001 **‡†† |
| Endocapillary hypercellularity | 0 (0–0) | 1 (0–1) | 2 (2–3) | 0 (0–1) | <0.001 **‡||†† |
| Subendothelial hyaline deposits | 0 (0–0) | 0 (0–0) | 1 (0–2) | 0 (0–0) | <0.001 **‡||†† |
| Leukocyte infiltration | 0 (0–0) | 0 (0–0) | 1 (0–1) | 0 (0–0) | <0.001 **||†† |
| Interstitial inflammation | 0 (0–1) | 0 (0–1) | 1 (0–2) | 0 (0–1) | <0.001 **||†† |
| Chronicity Index | 0 (0–1) | 3 (0–3) | 1 (0–4) | 1 (0–2.8) | 0.159 |
| Glomerular sclerosis | 0 (0–0) | 1 (0–1) | 1 (0–1) | 0 (0–1) | 0.011 * |
| Tubular atrophy | 0 (0–0) | 1 (0–1) | 0 (0–1) | 0 (0–1) | 0.157 |
| Interstitial fibrosis | 0 (0–1) | 1 (0–1) | 0 (0–1) | 0 (0–1) | 0.656 |
| Fibrous crescent | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.155 |
| Left K/S ratio | 0.910 (0.8–1.2) | 0.950 (0.9–1.1) | 1.16 (1.0–1.3) | 1.040 (1.0–1.2) | <0.001 **||¶ |
| Right K/S ratio | 0.990 (0.9–1.4) | 0.995 (0.9–1.2) | 1.220 (1.1–1.4) | 1.080 (1.0–1.2) | <0.001 **||†† |
| Univariate | Multivariate 1 | Multivariate 2 | Multivariate 3 | |||||
|---|---|---|---|---|---|---|---|---|
| B (95%CI) | p Value | B (95%CI) | p Value | B (95%CI) | p Value | B (95%CI) | p Value | |
| Age (years) | −0.003 (−0.005, 0.000) | 0.061 | ||||||
| Gender | ||||||||
| Female | Reference | |||||||
| Male | 0.004 (−0.082, 0.088) | 0.941 | ||||||
| Laboratory data | ||||||||
| Daily urine protein (gram) | 0.022 (0.015, 0.030) | <0.001 ** | 0.019 (0.011, 0.026) | <0.001 ** | 0.018 (0.010, 0.026) | <0.001 ** | 0.018 (0.010, 0.025) | <0.001 ** |
| Creatinine (mg/dL) | 0.018 (−0.001, 0.037) | 0.067 | ||||||
| eGFR (mg/mL) | −0.001 (−0.002, 0.000) | 0.016 * | 0.000 (−0.001, 0.001) | 0.752 | 0.000 (−0.001, 0.001) | 0.994 | ||
| Anti-dsDNA (WHO units/mL) | 0.000 (0.000, 0.000) | 0.350 | ||||||
| C3 (mg/dL) | −0.001 (−0.002, 0.000) | 0.072 | ||||||
| C4 (mg/dL) | −0.001 (−0.003, 0.002) | 0.565 | ||||||
| Renal pathology | ||||||||
| Activity index | 0.021 (0.015, 0.028) | <0.001 ** | 0.018 (0.010, 0.025) | <0.001 ** | ||||
| Cellular crescents | 0.051 (0.026, 0.070) | <0.001 ** | 0.008 (−0.023, 0.030) | 0.618 | ||||
| Fibrinoid necrosis/Karyorrhexis | 0.036 (0.016, 0.057) | <0.001 ** | 0.017 (−0.008, 0.041) | 0.185 | ||||
| Endocapillary hypercellularity | 0.072 (0.045, 0.098) | <0.001 ** | 0.025 (−0.017, 0.066) | 0.241 | 0.041 (0.011, 0.070) | 0.008 ** | ||
| Subendothelial hyaline deposits | 0.082 (0.046, 0.118) | <0.001 ** | 0.018 (−0.029, 0.065) | 0.456 | ||||
| Leukocyte infiltration | 0.090 (0.040, 0.141) | <0.001 ** | −0.014 (−0.071, 0.044) | 0.643 | ||||
| Interstitial inflammation | 0.094 (0.059, 0.130) | <0.001 ** | 0.054 (0.013, 0.095) | 0.010 * | 0.061 (0.023, 0.100) | 0.002 ** | ||
| Chronicity Index | −0.002 (−0.015, 0.010) | 0.694 | ||||||
| Glomerular sclerosis | −0.020 (−0.054, 0.014) | 0.244 | ||||||
| Tubular atrophy | −0.009 (−0.046, 0.029) | 0.648 | ||||||
| Interstitial fibrosis | −0.001 (−0.039, 0.036) | 0.848 | ||||||
| Fibrous crescent | 0.049 (−0.077, 0.175) | 0.442 | ||||||
| First Biopsy | Second Biopsy | p Value | |
|---|---|---|---|
| Age (years) | 26.0 (21.0–36.0) | 30.0 (24.0–37.0) | <0.001 ** |
| Daily urine protein (gram) | 3.8 (1.8–6.7) | 3.9 (1.0–5.6) | 0.600 |
| Creatinine (mg/dL) | 1.0 (0.8–1.7) | 1.1 (0.8–2.7) | 0.013 * |
| eGFR (mg/mL) | 74.1 (38.3–95.3) | 58.1 (22.5–96.4) | 0.072 |
| Anti-dsDNA (WHO units/mL) | 148.75 (95.8–409.1) | 141.4 (37.0–364.7) | 0.135 |
| C3 (mg/dL) | 56.9 (41.9–83.8) | 70.4 (48.9–87.3) | 0.109 |
| C4 (mg/dL) | 10.5 (5.7–13.5) | 16.8 (6.2–22.3) | 0.020 * |
| Lupus nephritis category | 0.931 | ||
| I & II | 2 (5.7%) | 2 (5.7%) | |
| III | 3 (8.6%) | 3 (8.6%) | |
| IV | 22 (62.9%) | 23 (65.7%) | |
| V | 8 (22.9%) | 7 (20.0%) | |
| Activity index | 6.0 (1.0–9.0) | 2.0 (0.3–6.8) | 0.028 * |
| Cellular crescents | 0 (0–2) | 0 (0–0) | 0.218 |
| Fibrinoid necrosis/ Karyorrhexis | 2.0 (0.0–2.0) | 0 (0–0) | 0.028 * |
| Endocapillary hypercellularity | 2 (0–3) | 1 (0–3) | 0.045 * |
| Subendothelial hyaline deposits | 0 (0–2) | 0 (0–1) | 0.301 |
| Leukocyte infiltration | 0 (0–1) | 0 (0–1) | 0.120 |
| Interstitial inflammation | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.655 |
| Chronicity Index | 1 (0–2) | 3.0 (1.0–7.0) | <0.001 ** |
| Glomerular sclerosis | 0 (0–1) | 1 (0–3) | <0.001 ** |
| Tubular atrophy | 0 (0–0) | 1 (0–2) | 0.001 ** |
| Interstitial fibrosis | 0 (0–1) | 1 (0–2) | 0.001 ** |
| Fibrous crescent | 0 (0–0) | 0 (0–0) | 0.317 |
| Left K/S ratio | 1.140 (1.0–1.4) | 1.060 (1.0–1.3) | 0.241 |
| Right K/S ratio | 1.210 (1.1–1.4) | 1.120 (1.0–1.3) | 0.225 |
| Changes in Variables | Change in Left K/S Ratio | |
|---|---|---|
| rs | p Value | |
| ∆Daily urine protein (gram) | 0.768 | <0.001 ** |
| ∆Creatinine (mg/dL) | 0.045 | 0.796 |
| ∆eGFR (mg/mL) | −0.192 | 0.270 |
| ∆Anti-dsDNA (WHO units/mL) | 0.768 | 0.348 |
| ∆C3 (mg/dL) | 0.027 | 0.888 |
| ∆C4 (mg/dL) | 0.022 | 0.902 |
| ∆Activity Index | 0.357 | 0.035 * |
| ∆Cellular crescent | 0.258 | 0.161 |
| ∆Fibrinoid necrosis/ Karyorrhexis | 0.324 | 0.075 |
| ∆Endocapillary hypercellularity | 0.385 | 0.032 * |
| ∆Subendothelial hyaline deposits | 0.253 | 0.017 |
| ∆Leukocyte infiltration | 0.390 | 0.030 * |
| ∆Interstitial inflammation | 0.300 | 0.101 |
| ∆Chronicity Index | −0.106 | 0.543 |
| ∆Glomerular sclerosis | −0.009 | 0.961 |
| ∆Tubular atrophy | −0.113 | 0.545 |
| ∆Interstitial fibrosis | −0.070 | 0.707 |
| ∆Fibrous crescent | 0.243 | 0.187 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, T.-Y.; Lin, Y.-C.; Hung, W.-T.; Chen, Y.-M.; Wen, M.-C.; Chen, H.-H.; Lin, W.-Y.; Hsieh, C.-W.; Lin, C.-T.; Lai, K.-L.; et al. Change of Renal Gallium Uptake Correlated with Change of Inflammation Activity in Renal Pathology in Lupus Nephritis Patients. J. Clin. Med. 2021, 10, 4654. https://doi.org/10.3390/jcm10204654
Hsieh T-Y, Lin Y-C, Hung W-T, Chen Y-M, Wen M-C, Chen H-H, Lin W-Y, Hsieh C-W, Lin C-T, Lai K-L, et al. Change of Renal Gallium Uptake Correlated with Change of Inflammation Activity in Renal Pathology in Lupus Nephritis Patients. Journal of Clinical Medicine. 2021; 10(20):4654. https://doi.org/10.3390/jcm10204654
Chicago/Turabian StyleHsieh, Tsu-Yi, Yi-Ching Lin, Wei-Ting Hung, Yi-Ming Chen, Mei-Chin Wen, Hsin-Hua Chen, Wan-Yu Lin, Chia-Wei Hsieh, Ching-Tsai Lin, Kuo-Lung Lai, and et al. 2021. "Change of Renal Gallium Uptake Correlated with Change of Inflammation Activity in Renal Pathology in Lupus Nephritis Patients" Journal of Clinical Medicine 10, no. 20: 4654. https://doi.org/10.3390/jcm10204654
APA StyleHsieh, T.-Y., Lin, Y.-C., Hung, W.-T., Chen, Y.-M., Wen, M.-C., Chen, H.-H., Lin, W.-Y., Hsieh, C.-W., Lin, C.-T., Lai, K.-L., Tang, K.-T., Tseng, C.-W., Huang, W.-N., Chen, Y.-H., Tsai, S.-C., & Wu, Y.-D. (2021). Change of Renal Gallium Uptake Correlated with Change of Inflammation Activity in Renal Pathology in Lupus Nephritis Patients. Journal of Clinical Medicine, 10(20), 4654. https://doi.org/10.3390/jcm10204654