
Caval Valve Implantation (CAVI): An Emerging Therapy for Treating Severe Tricuspid Regurgitation

 ,
,
Abstract
1. Introduction
2. Context
2.1. CAVI: Concept
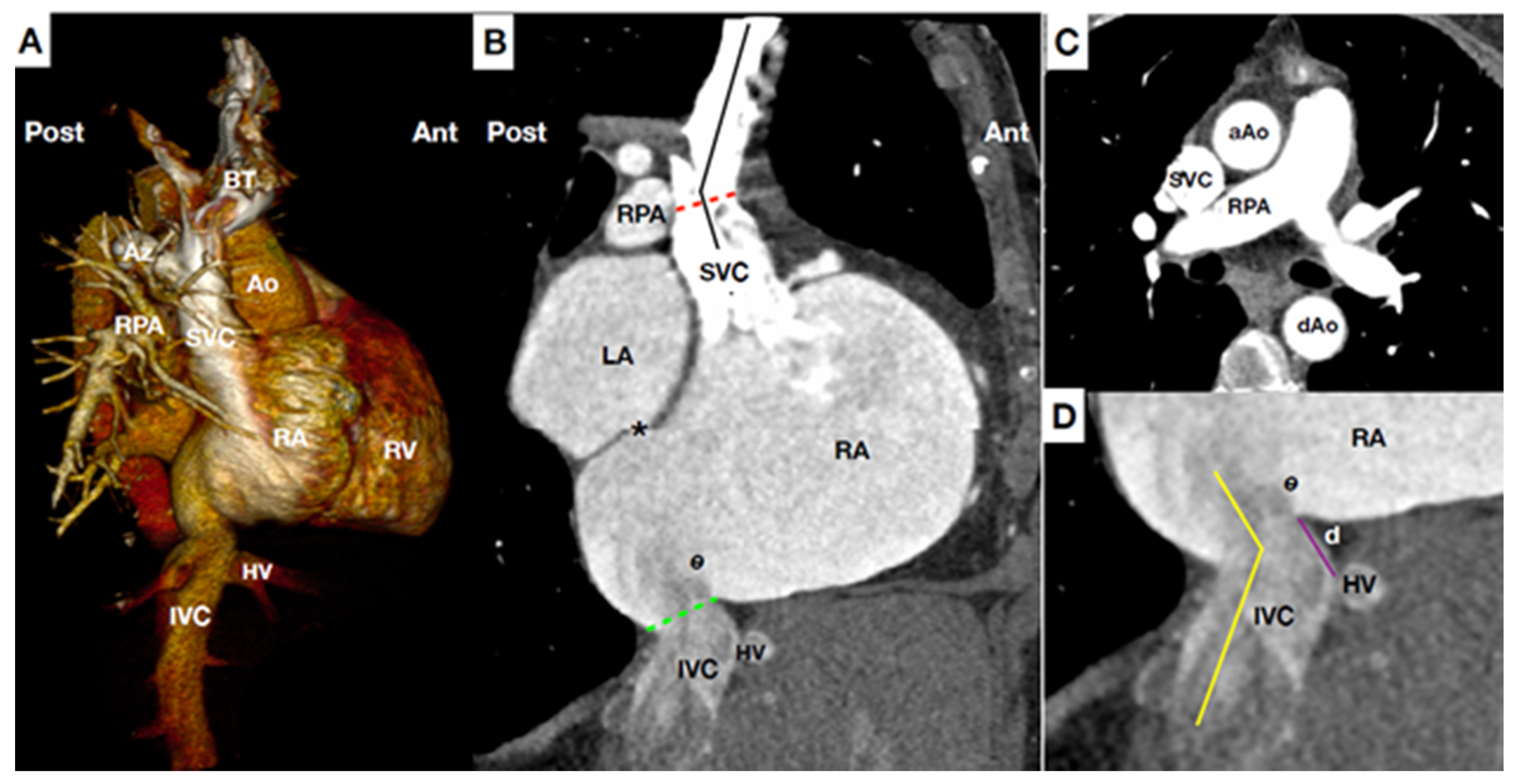
2.2. CAVI: Anatomical Considerations
2.3. CAVI: Evidence and Devices
2.4. Non-Dedicated CAVI Devices: Early CAVI Studies
3. Dedicated Devices
3.1. TricValve®: Evidence, Current Studies, and Future Trials
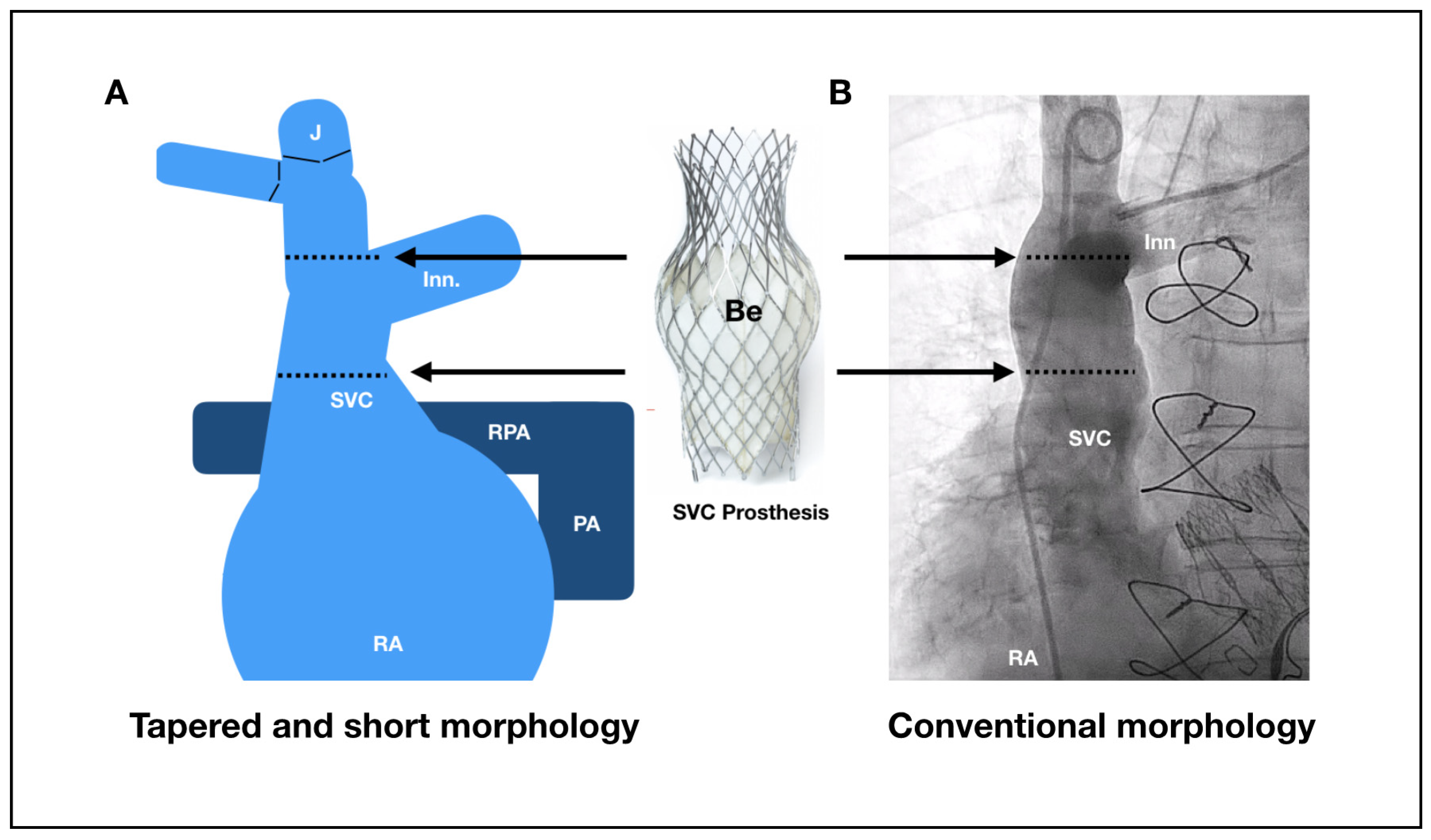
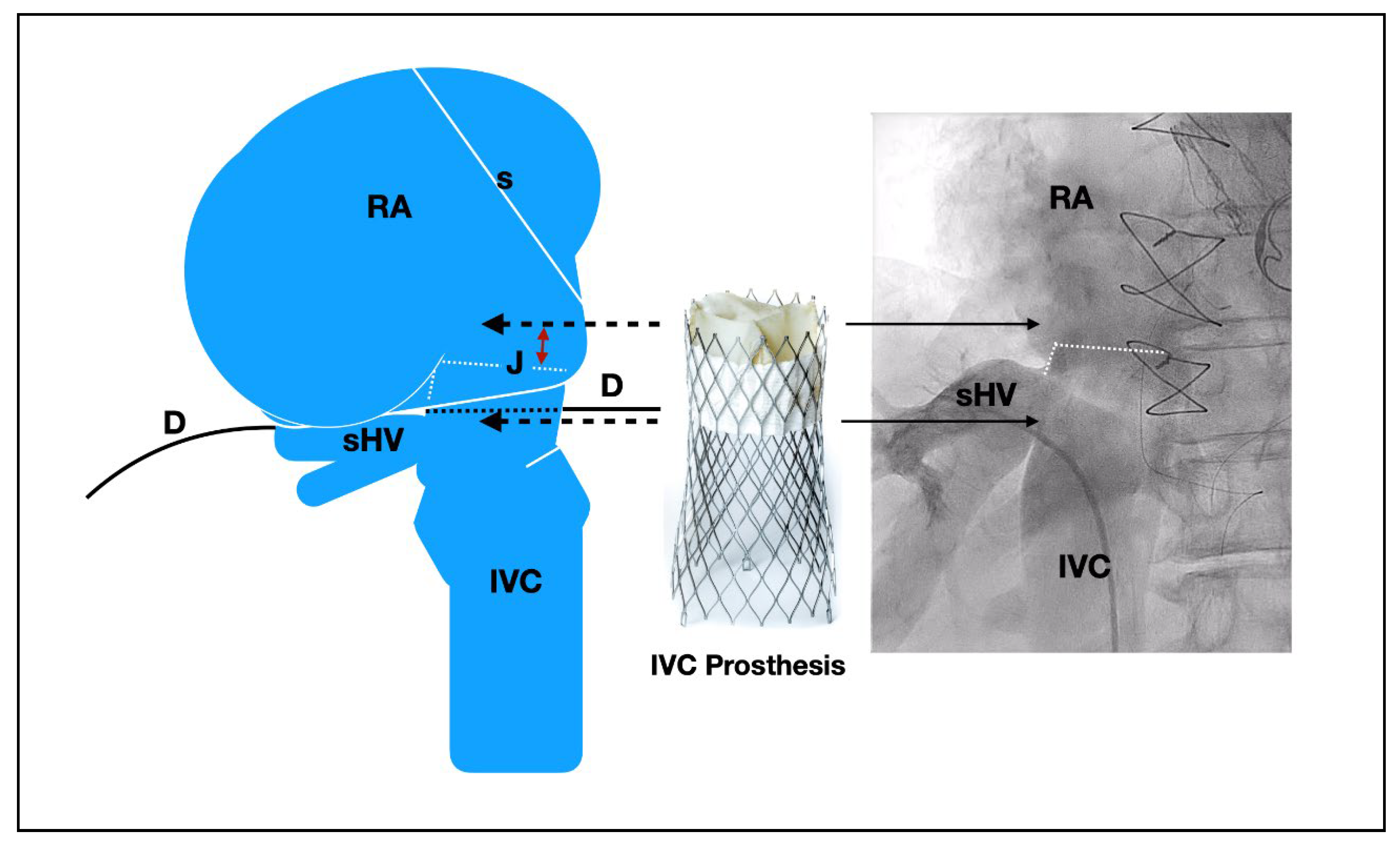
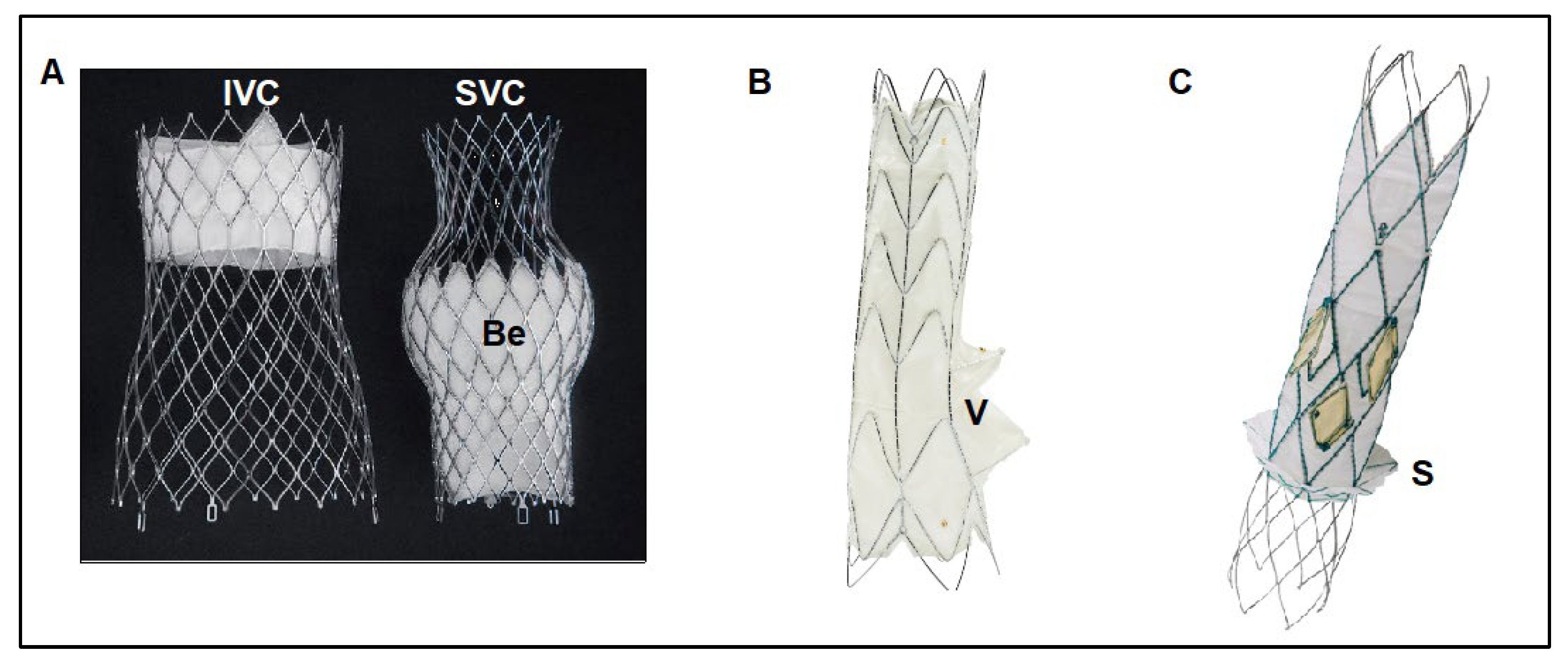
3.2. TricValve®
3.3. TricValve® Planning
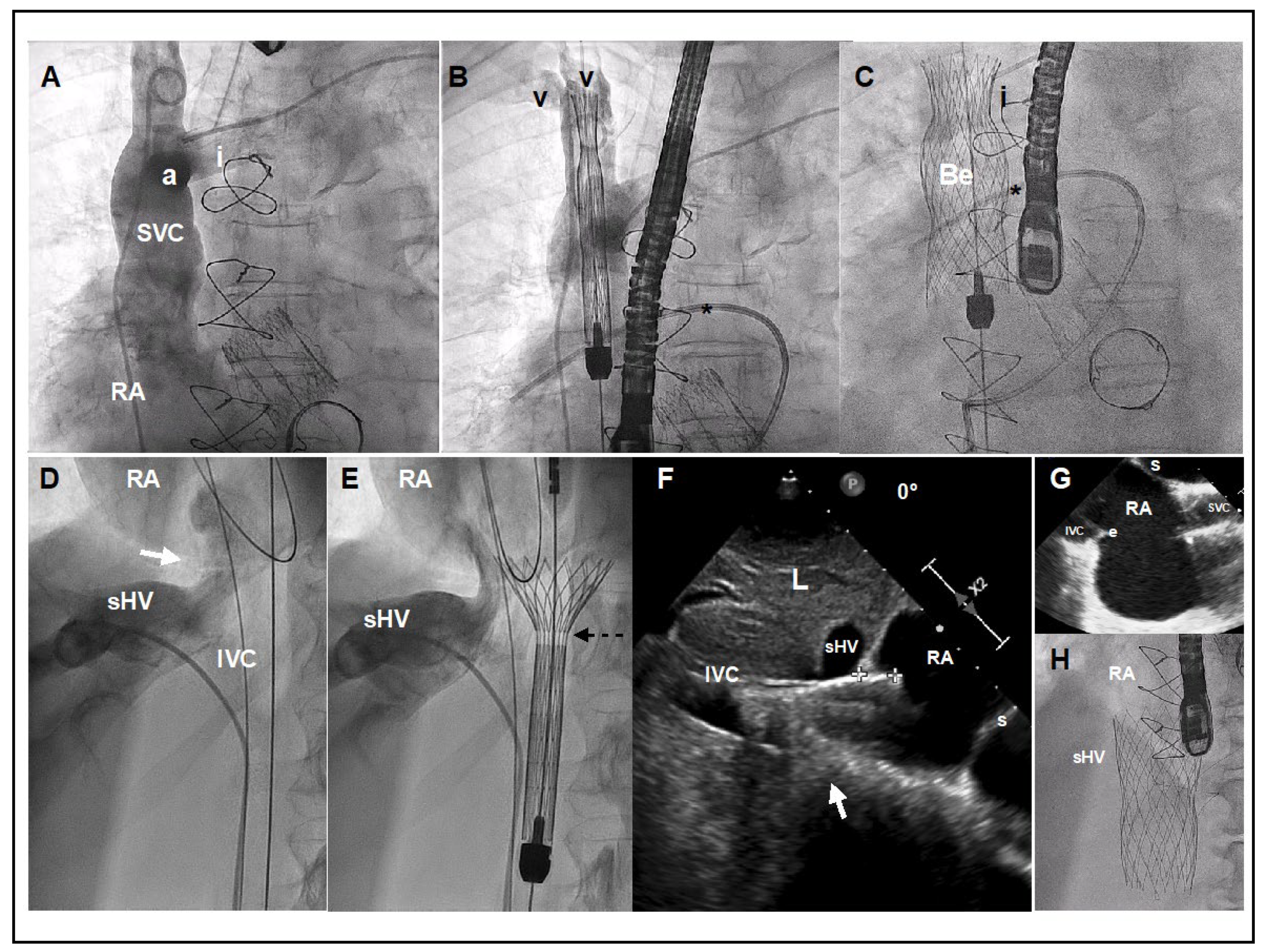
3.4. TricValve® Procedural Steps
3.5. Post-Implantation Care
3.6. Longer-Term Management
3.7. TRINCENTO®
Concept, Imaging, Anatomical Consideration and Evidence
3.8. TRILLIUM™
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’ARCY, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J.; et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Topilsky, Y.; Maltais, S.; Medina Inojosa, J.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of Tricuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc. Imaging 2019, 12, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Zack, C.J.; Fender, E.A.; Chandrashekar, P.; Reddy, Y.N.V.; Bennett, C.E.; Stulak, J.M.; Miller, V.M.; Nishimura, R.A. National Trends and Outcomes in Isolated Tricuspid Valve Surgery. J. Am. Coll. Cardiol. 2017, 70, 2953–2960. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Jung, S.-H.; Choo, S.J.; Chung, C.H.; Lee, J.W. Surgical outcomes of severe tricuspid regurgitation: Predictors of adverse clinical outcomes. Heart 2013, 99, 181–187. [Google Scholar] [CrossRef]
- Asmarats, L.; Puri, R.; Latib, A.; Navia, J.L.; Rodés-Cabau, J. Transcatheter Tricuspid Valve Interventions. J. Am. Coll. Cardiol. 2018, 71, 2935–2956. [Google Scholar] [CrossRef]
- Figulla, H.R.; Kiss, K.; Lauten, A. Transcatheter interventions for tricuspid regurgitation-heterotopic technology: TricValve. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2016, 12, Y116–Y118. [Google Scholar] [CrossRef]
- Toggweiler, S.; De Boeck, B.; Brinkert, M.; Buhmann, R.; Bossard, M.; Kobza, R.; Cuculi, F. First-in-man implantation of the Tricento transcatheter heart valve for the treatment of severe tricuspid regurgitation. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2018, 14, 758–761. [Google Scholar] [CrossRef]
- Prihadi, E.A.; Delgado, V.; Leon, M.B.; Enriquez-Sarano, M.; Topilsky, Y.; Bax, J.J. Morphologic Types of Tricuspid Regurgitation. JACC Cardiovasc. Imaging 2019, 12, 491–499. [Google Scholar] [CrossRef]
- Nickenig, G.; Weber, M.; Schueler, R.; Hausleiter, J.; Näbauer, M.; von Bardeleben, R.S.; Sotiriou, E.; Schäfer, U.; Deuschl, F.; Kuck, K.-H.; et al. 6-Month Outcomes of Tricuspid Valve Reconstruction for Patients With Severe Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2019, 73, 1905–1915. [Google Scholar] [CrossRef]
- Nickenig, G.; Kowalski, M.; Hausleiter, J.; Braun, D.; Schofer, J.; Yzeiraj, E.; Rudolph, V.; Friedrichs, K.; Maisano, F.; Taramasso, M.; et al. Transcatheter Treatment of Severe Tricuspid Regurgitation with the Edge-to-Edge MitraClip Technique. Circulation 2017, 135, 1802–1814. [Google Scholar] [CrossRef]
- Fam, N.P.; Braun, D.; von Bardeleben, R.S.; Nabauer, M.; Ruf, T.; Connelly, K.A.; Ho, E.; Thiele, H.; Lurz, P.; Weber, M.; et al. Compassionate Use of the PASCAL Transcatheter Valve Repair System for Severe Tricuspid Regurgitation. JACC Cardiovasc. Interv. 2019, 12, 2488–2495. [Google Scholar] [CrossRef]
- Orban, M.; Rommel, K.-P.; Ho, E.C.; Unterhuber, M.; Pozzoli, A.; Connelly, K.A.; Deseive, S.; Besler, C.; Ong, G.; Braun, D.; et al. Transcatheter Edge-to-Edge Tricuspid Repair for Severe Tricuspid Regurgitation Reduces Hospitalizations for Heart Failure. JACC Heart Fail. 2020, 8, 265–276. [Google Scholar] [CrossRef]
- Fam, N.P.; Ong, G.; Deva, D.P.; Peterson, M.D. Transfemoral Transcatheter Tricuspid Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, e93–e94. [Google Scholar] [CrossRef]
- Nickenig, G.; Weber, M.; Lurz, P.; von Bardeleben, R.S.; Sitges, M.; Sorajja, P.; Hausleiter, J.; Denti, P.; Trochu, J.-N.; Näbauer, M.; et al. Transcatheter edge-to-edge repair for reduction of tricuspid regurgitation: 6-month outcomes of the TRILUMINATE single-arm study. Lancet 2019, 394, 2002–2011. [Google Scholar] [CrossRef]
- Rodés-Cabau, J.; Hahn, R.T.; Latib, A.; Laule, M.; Lauten, A.; Maisano, F.; Schofer, J.; Campelo-Parada, F.; Puri, R.; Vahanian, A. Transcatheter Therapies for Treating Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2016, 67, 1829–1845. [Google Scholar] [CrossRef]
- Fam, N.P.; von Bardeleben, R.S.; Hensey, M.; Kodali, S.K.; Smith, R.L.; Hausleiter, J.; Ong, G.; Boone, R.; Ruf, T.; George, I.; et al. Transfemoral Transcatheter Tricuspid Valve Replacement with the EVOQUE System. JACC Cardiovasc. Interv. 2021, 14, 501–511. [Google Scholar] [CrossRef]
- Lauten, A.; Figulla, H.R.; Willich, C.; Jung, C.; Rademacher, W.; Schubert, H.; Ferrari, M. Heterotopic Valve Replacement as an Interventional Approach to Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2010, 55, 499–500. [Google Scholar] [CrossRef]
- Bertrand, P.B.; Hung, J. Bicaval Valve Implantation for Severe Tricuspid Regurgitation. JACC Case Rep. 2019, 1, 725–726. [Google Scholar] [CrossRef]
- Lauten, A.; Hamadanchi, A.; Doenst, T.; Figulla, H.R. Caval valve implantation for treatment of tricuspid regurgitation: Post-mortem evaluation after mid-term follow-up. Eur. Heart J. 2013, 35, 1651-1651. [Google Scholar] [CrossRef][Green Version]
- Lauten, A.; Dreger, H.; Laule, M.; Stangl, K.; Figulla, H.R. Caval Valve Implantation. Interv. Cardiol. Clin. 2018, 7, 57–63. [Google Scholar] [CrossRef]
- Sonavane, S.K.; Milner, D.M.; Singh, S.P.; Abdel Aal, A.K.; Shahir, K.S.; Chaturvedi, A. Comprehensive Imaging Review of the Superior Vena Cava. Radiographics 2015, 35, 1873–1892. [Google Scholar] [CrossRef]
- Smillie, R.P.; Shetty, M.; Boyer, A.C.; Madrazo, B.; Jafri, S.Z. Imaging evaluation of the inferior vena cava. Radiographics 2015, 35, 578–592. [Google Scholar] [CrossRef]
- Lauten, A.; Doenst, T.; Hamadanchi, A.; Franz, M.; Figulla, H.R. Percutaneous Bicaval Valve Implantation for Transcatheter Treatment of Tricuspid Regurgitation. Circ. Cardiovasc. Interv. 2014, 7, 268–272. [Google Scholar] [CrossRef]
- Laule, M.; Stangl, V.; Sanad, W.; Lemcke, A.; Baumann, G.; Stangl, K. Percutaneous Transfemoral Management of Severe Secondary Tricuspid Regurgitation with Edwards Sapien XT Bioprosthesis. Fisrt-in-man Experience. J. Am. Coll. Cardiol. 2013, 18, 1929–1931. [Google Scholar] [CrossRef]
- Lauten, A.; Figulla, H.R.; Unbehaun, A.; Fam, N.; Schofer, J.; Doenst, T.; Hausleiter, J.; Franz, M.; Jung, C.; Dreger, H.; et al. Interventional Treatment of Severe Tricuspid Regurgitation. Circ. Cardiovasc. Interv. 2018, 11, e006061. [Google Scholar] [CrossRef]
- Dreger, H.; Mattig, I.; Hewing, B.; Knebel, F.; Lauten, A.; Lembcke, A.; Thoenes, M.; Roehle, R.; Stangl, V.; Landmesser, U.; et al. Treatment of Severe TRIcuspid Regurgitation in Patients with Advanced Heart Failure with CAval Vein Implantation of the Edwards Sapien XT VALve (TRICAVAL): A randomised controlled trial. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2020, 15, 1506–1513. [Google Scholar] [CrossRef]
- O’Neill, B.P.; Negrotto, S.; Yu, D.; Lakhter, V.; Depta, J.; McCabe, J.M.; Dube, S.; Vaikom, M.; Wang, D.D.; Patil, P.; et al. Caval Valve Implantation for Tricuspid Regurgitation: Insights From the United States Caval Valve Registry. J. Invasive Cardiol. 2020, 32, 470–475. [Google Scholar]
- Cruz-González, I.; González-Ferreiro, R.; Amat-Santos, I.J.; Carrasco-Chinchilla, F.; Alonso Briales, J.H.; Estévez-Loureiro, R. TRICENTO transcatheter heart valve for severe tricuspid regurgitation. Initial experience and mid-term follow-up. Revista Española de Cardiología 2021, 74, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Aparisi, Á.; Amat-Santos, I.J.; Serrador, A.; Rodríguez-Gabella, T.; Arnold, R.; San Román, J.A. Current clinical outcomes of tricuspid regurgitation and initial experience with the TricValve system in Spain. Revista Española de Cardiología 2020, 73, 853–854. [Google Scholar] [CrossRef]
- Lauten, A.; Figulla, H.R.; Willich, C.; Laube, A.; Rademacher, W.; Schubert, H.; Bischoff, S.; Ferrari, M. Percutaneous caval stent valve implantation: Investigation of an interventional approach for treatment of tricuspid regurgitation. Eur. Heart J. 2009, 31, 1274–1281. [Google Scholar] [CrossRef]
- O’Neill, B.P. Caval Valve Implantation. Are 2 Valves better than 1? Circ. Cardiovasc. Interv. 2018, 11, e006334. [Google Scholar] [CrossRef] [PubMed]
- Fernández-López, I.; Peña-Otero, D.; Ángeles Atín-Arratibel, M.d.l.; Eguillor-Mutiloa, M. Influence of the phrenic nerve in shoulder pain: A systematic review. Int. J. Osteopath. Med. 2020, 36, 36–48. [Google Scholar] [CrossRef]
- Mitrosz, M.; Chlabicz, M.; Hapaniuk, K.; Kaminski, K.A.; Sobkowicz, B.; Piszcz, J.; Dobrzycki, S.; Musial, W.J.; Hirnle, T.; Tycinska, A.M. Thrombocytopenia associated with TAVI—The summary of possible causes. Adv. Med. Sci. 2017, 62, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Montorfano, M.; Beneduce, A.; Ancona, M.B.; Ancona, F.; Sgura, F.; Romano, V.; Ferri, L.A.; Bellini, B.; Khawaja, S.A.; Moroni, F.; et al. Tricento Transcatheter Heart Valve for Severe Tricuspid Regurgitation. JACC Cardiovasc. Interv. 2019, 12, e189–e191. [Google Scholar] [CrossRef]
- Werner, P.; Russo, M.; Scherzer, S.; Aref, T.; Coti, I.; Mascherbauer, J.; Kocher, A.; Laufer, G.; Andreas, M. Transcatheter Caval Valve Implantation of the Tricento Valve for Tricuspid Regurgitation Using Advanced Intraprocedural Imaging. JACC Case Rep. 2019, 1, 720–724. [Google Scholar] [CrossRef]
- Wilbring, M.; Tomala, J.; Ulbrich, S.; Murugaboopathy, V.; Matschke, K.; Kappert, U. Recurrence of Right Heart Failure After Heterotopic Tricuspid Intervention. JACC Cardiovasc. Interv. 2020, 13, e95–e96. [Google Scholar] [CrossRef]
- Boeder, N.F.; Bayer, M.; Dörr, O.; Nef, H.M. Fusion imaging guided implantation of a Tricento transcatheter heart valve for severe tricuspid regurgitation. Catheter. Cardiovasc. Interv. 2021. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Favorable Conditions/Aspects | Unfavorable Conditions/Aspects |
|---|---|---|
| Edge-to-edge technique |
|
|
| Annuloplasty |
|
|
| Orthotopic Valve Replacement |
|
|
| Heterotopic Valve Replacement |
|
|
| Author | N | Device Used | Proc. Success | Embolisation | Leak | Open-Surgery | In-Hospital Death | 30-Day Death |
|---|---|---|---|---|---|---|---|---|
| Lauten [23] | 1 | Customized | 1 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Laule [24] | 3 | Sapient XT | 3 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Lauten [25] | 25 | Sapien XT TricValve DirectFlow | 23 (92) | 2 (8) | NA | 1 (4.0) | 6 (24) | 9 (36) |
| Toggweiler [7] | 1 | Tricento | 1 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Dreger [26] | 14 | Sapien XT | 14 (100) | 0 (0) | 2 (14.3) | 4 (28.6) | 3 (21.4) | 3 (21.4) |
| O’Neill [27] | 24 | Sapien XT | 24 (100) | 0 (0) | 2 (10) | 0 (0) | 5 (20.8) | 6 (25) |
| Cruz-Gonzalez [28] | 6 | Tricento | 6 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Aparisi [29] | 2 | TricValve | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| TricValve SP * | 47 | TricValve | 46 (98) | 1 (2) | NA | 1 (2) | 0 (0) | 2 (8) |
| Inclusion Criteria |
|---|
Clinical
|
| Exclusion Criteria |
Clinical
|
| SVC Prosthesis Sizing | 25 mm | 29 mm | 33 mm | |
|---|---|---|---|---|
| Confluence Innominate | Larger than 14 mm | |||
| SVC to PA | 19–31 mm | 22–34 mm | 25–40 mm | |
| SVC to middle PA | 22–31 mm | 27–34 mm | 25–40 mm | |
| Length of middle PA | Larger than 35 mm | |||
| Length of SVC to Confluence | Larger than 50 mm | |||
| IVC prosthesis sizing | 31 mm | 35 mm | 41 mm | 45 mm |
| IVC-RA junction | 24 to 31 mm | 28 to 35 mm | 33 to 41 mm | 38 to 45 mm |
| IVC-on top of sHV confluence | 24 to 31 mm | 28 to 35 mm | 33 to 41 mm | 38 to 45 mm |
| Length IVC/RA Junction-sHV | Larger than 10 mm | |||
| IVC just below sHV confluence | 21 to 35 mm | 27 to 43 mm | 30 to 48 mm | 35 to 50 mm |
| IVC at 5 cm below RA junction | 21 to 35 mm | 27 to 43 mm | 30 to 48 mm | 35 to 50 mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul-Jawad Altisent, O.; Benetis, R.; Rumbinaite, E.; Mizarien, V.; Codina, P.; Gual-Capllonch, F.; Spitaleri, G.; Fernandez-Nofrerias, E.; Bayes-Genis, A.; Puri, R. Caval Valve Implantation (CAVI): An Emerging Therapy for Treating Severe Tricuspid Regurgitation. J. Clin. Med. 2021, 10, 4601. https://doi.org/10.3390/jcm10194601
Abdul-Jawad Altisent O, Benetis R, Rumbinaite E, Mizarien V, Codina P, Gual-Capllonch F, Spitaleri G, Fernandez-Nofrerias E, Bayes-Genis A, Puri R. Caval Valve Implantation (CAVI): An Emerging Therapy for Treating Severe Tricuspid Regurgitation. Journal of Clinical Medicine. 2021; 10(19):4601. https://doi.org/10.3390/jcm10194601
Chicago/Turabian StyleAbdul-Jawad Altisent, Omar, Rimantas Benetis, Egle Rumbinaite, Vaida Mizarien, Pau Codina, Francisco Gual-Capllonch, Giosafat Spitaleri, Eduard Fernandez-Nofrerias, Antoni Bayes-Genis, and Rishi Puri. 2021. "Caval Valve Implantation (CAVI): An Emerging Therapy for Treating Severe Tricuspid Regurgitation" Journal of Clinical Medicine 10, no. 19: 4601. https://doi.org/10.3390/jcm10194601
APA StyleAbdul-Jawad Altisent, O., Benetis, R., Rumbinaite, E., Mizarien, V., Codina, P., Gual-Capllonch, F., Spitaleri, G., Fernandez-Nofrerias, E., Bayes-Genis, A., & Puri, R. (2021). Caval Valve Implantation (CAVI): An Emerging Therapy for Treating Severe Tricuspid Regurgitation. Journal of Clinical Medicine, 10(19), 4601. https://doi.org/10.3390/jcm10194601