
Risk Factors for Perioperative Hemodynamic Instability in Pheochromocytoma: A Systematic Review and Meta-Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
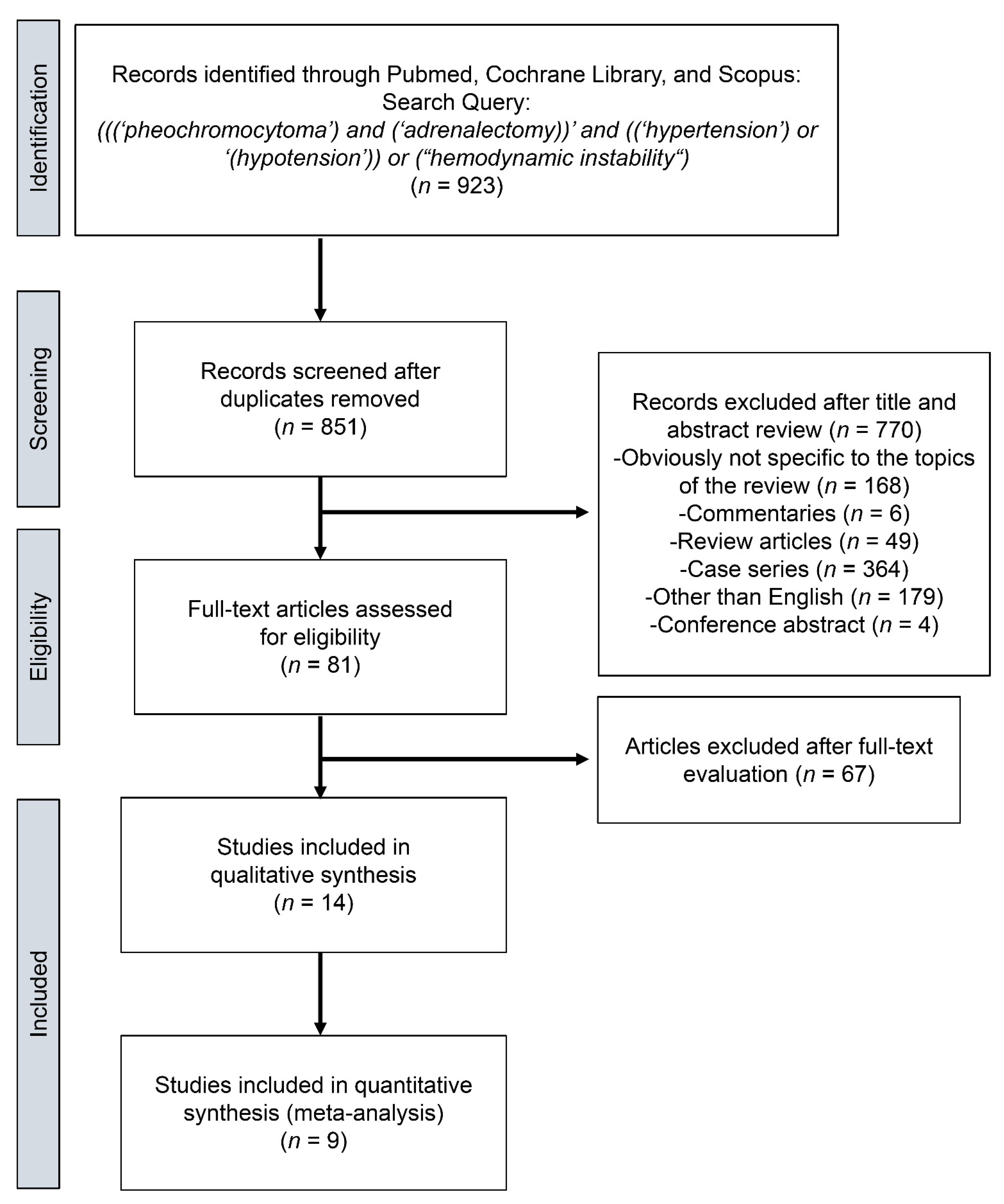
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Statistical Analysis
4. Results
4.1. Study Selection and Characteristics
4.2. Meta-Analysis
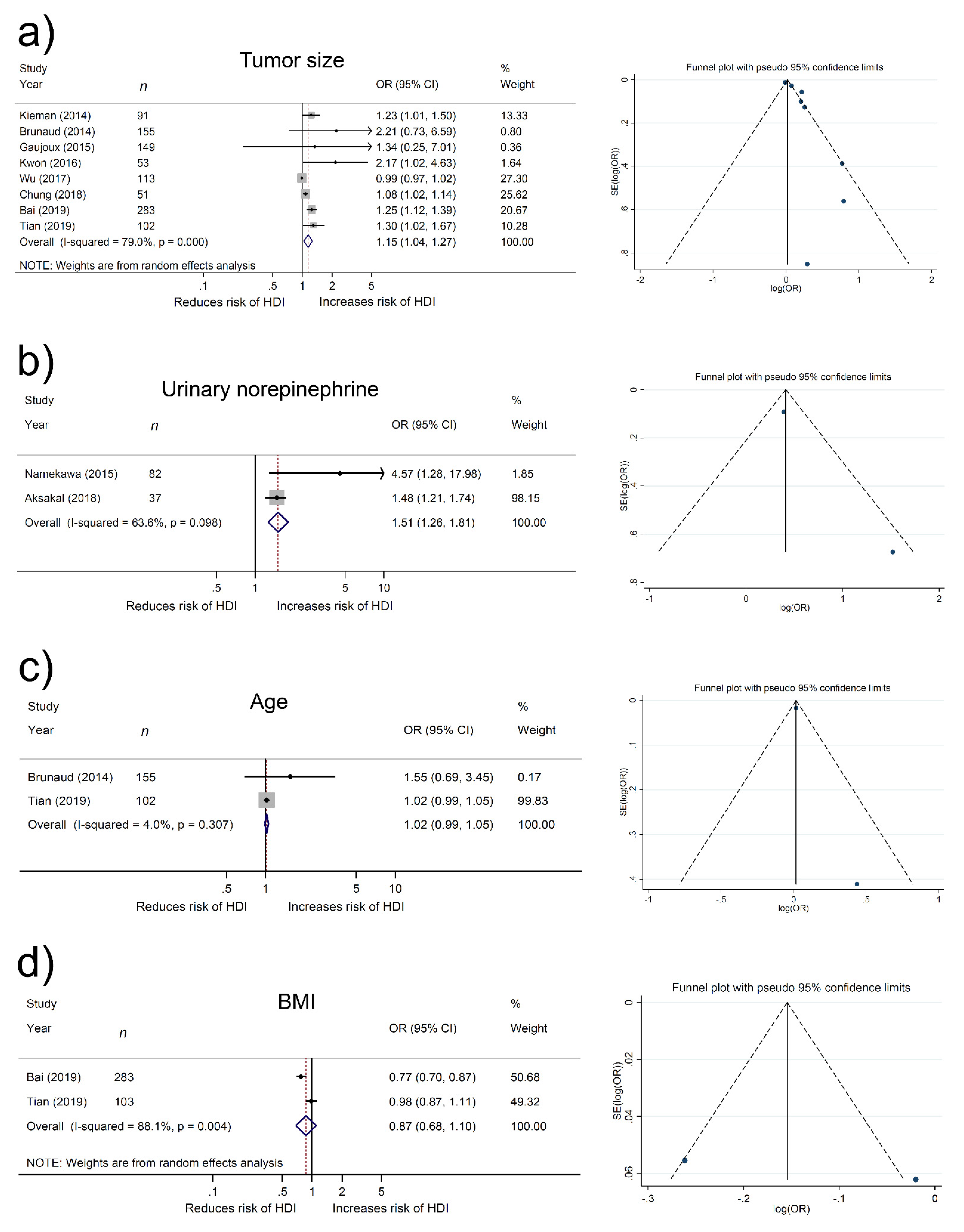
4.3. Association of Tumor Size with Hemodynamic Instability
4.4. Association of Urinary Norepinephrine with Hemodynamic Instability
4.5. Association of Age with Hemodynamic Instability
4.6. Association of BMI with Hemodynamic Instability
4.7. Other Factors Associated with Hemodynamic Instability
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, H.; Sippel, R.S.; O’Dorisio, M.S.; Vinik, A.I.; Lloyd, R.V.; Pacak, K. The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors: Pheochromocytoma, paraganglioma, and medullary thyroid cancer. Pancreas 2010, 39, 775–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenders, J.W.; Eisenhofer, G.; Mannelli, M.; Pacak, K. Phaeochromocytoma. Lancet 2005, 366, 665–675. [Google Scholar] [CrossRef]
- Bruynzeel, H.; Feelders, R.A.; Groenland, T.H.N.; Meiracker, A.H.V.D.; Van Eijck, C.H.J.; Lange, J.F.; De Herder, W.W.; Kazemier, G. Risk Factors for Hemodynamic Instability during Surgery for Pheochromocytoma. J. Clin. Endocrinol. Metab. 2010, 95, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiernan, C.M.; Du, L.; Chen, X.; Broome, J.T.; Shi, C.; Peters, M.F.; Solorzano, C.C. Predictors of Hemodynamic Instability during Surgery for Pheochromocytoma. Ann. Surg. Oncol. 2014, 21, 3865–3871. [Google Scholar] [CrossRef] [Green Version]
- Gaujoux, S.; Bonnet, S.; Lentschener, C.; Thillois, J.M.; Duboc, D.; Bertherat, J.; Samama, C.M.; Dousset, B. Preoperative risk factors of hemodynamic instability during laparoscopic adrenalectomy for pheochromocytoma. Surg. Endosc. 2016, 30, 2984–2993. [Google Scholar] [CrossRef]
- Namekawa, T.; Fukasawa, S.; Komaru, A.; Kobayashi, M.; Imamura, Y.; Ohzeki, T.; Takagi, K.; Sato, Y.; Akakura, K.; Ichikawa, T.; et al. Prospective evaluation of the safety of transrectal ultrasound-guided transperineal prostate biopsy based on adverse events. Int. J. Clin. Oncol. 2015, 20, 1185–1191. [Google Scholar] [CrossRef]
- Wu, S.; Chen, W.; Shen, L.; Xu, L.; Zhu, A.; Huang, Y. Risk factors for prolonged hypotension in patients with pheochromocytoma undergoing laparoscopic adrenalectomy: A single-center retrospective study. Sci. Rep. 2017, 7, 5897. [Google Scholar] [CrossRef] [Green Version]
- Araujo-Castro, M.; Centeno, R.G.; López-García, M.-C.; Lamas, C.; Álvarez-Escolá, C.; Gutiérrez, M.C.; Blanco-Carrera, C.; Novoa, P.D.M.; Valdés, N.; Gimeno, P.G.; et al. Risk factors for intraoperative complications in pheochromocytomas. Endocr. Relat. Cancer 2021, 28, 695–703. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.D.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii-x, 1–173. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; Bland, J.M. How to obtain the confidence interval from a P value. BMJ 2011, 343, d2090. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ 2011, 343, d2304. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Brunaud, L.; Boutami, M.; Nguyen-Thi, P.-L.; Finnerty, B.; Germain, A.; Weryha, G.; Fahey, T.J.; Mirallie, E.; Bresler, L.; Zarnegar, R. Both preoperative alpha and calcium channel blockade impact intraoperative hemodynamic stability similarly in the management of pheochromocytoma. Surgery 2014, 156, 1410–1417. [Google Scholar] [CrossRef]
- Livingstone, M.; Duttchen, K.; Thompson, J.; Sunderani, Z.; Hawboldt, G.; Rose, M.S.; Pasieka, J. Hemodynamic Stability during Pheochromocytoma Resection: Lessons Learned Over the Last Two Decades. Ann. Surg. Oncol. 2015, 22, 4175–4180. [Google Scholar] [CrossRef]
- Kwon, S.Y.; Lee, K.S.; Lee, J.N.; Ha, Y.-S.; Choi, S.H.; Kim, H.T.; Kim, T.-H.; Yoo, E.S.; Kwon, T.G. Risk factors for hypertensive attack during pheochromocytoma resection. Investig. Clin. Urol. 2016, 57, 184–190. [Google Scholar] [CrossRef] [Green Version]
- Vorselaars, W.M.; Postma, E.L.; Mirallie, E.; Thiery, J.; Lustgarten, M.; Pasternak, J.D.; Bellantone, R.; Raffaelli, M.; Fahey, T., III; Vriens, M.R.; et al. Hemodynamic instability during surgery for pheochromocytoma: Comparing the transperitoneal and retroperitoneal approach in a multicenter analysis of 341 patients. Surgery 2018, 163, 176–182. [Google Scholar] [CrossRef]
- Chung, H.S.; Kim, M.S.; Yu, H.S.; Hwang, E.C.; Kim, S.O.; Oh, K.J.; Jung, S.I.; Kang, T.W.; Park, K.; Kwon, D.D. Laparoscopic adrenalectomy using the lateral retroperitoneal approach: Is it a safe and feasible treatment option for pheochromocytomas larger than 6 cm? Int. J. Urol. 2018, 25, 414–419. [Google Scholar] [CrossRef] [Green Version]
- Aksakal, N.; Agcaoglu, O.; Sahbaz, N.A.; Albuz, O.; Saracoglu, A.; Yavru, A.; Barbaros, U.; Erbil, Y. Predictive Factors of Operative Hemodynamic Instability for Pheochromocytoma. Am. Surg. 2018, 84, 920–923. [Google Scholar] [CrossRef]
- Bai, S.; Wu, B.; Yao, Z.; Zhu, X.; Jiang, Y.; Wang, H. Development and validation of a clinical model to predict intraoperative hemodynamic instability in patients with pheochromocytomas surgery. Endocr. J. 2020, 67, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Tian, J.; Bao, Z.; Yuan, Y.; Fang, D.; Zhan, Y.; Wang, T.; Zhang, Z.; Liqun, Z. The Duration of Preoperative Administration of Single α-Receptor Blocker Phenoxybenzamine before Adrenalectomy for Pheochromocytoma: 18 Years of Clinical Experience from Nationwide High-Volume Center. BioMed Res. Int. 2019, 2019, 2613137. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.P.; Bennett, D.; Hodson, J.; Asia, M.; Ayuk, J.; O’Reilly, M.W.; Karavitaki, N.; Arlt, W.; Sutcliffe, R.P. Incidence, risk factors and clinical significance of postoperative haemodynamic instability after adrenalectomy for phaeochromocytoma. Gland Surg. 2019, 8, 729–739. [Google Scholar] [CrossRef]
- Buisset, C.; Guerin, C.; Cungi, P.J.; Gardette, M.; Paladino, N.C.; Taïeb, D.; Cuny, T.; Castinetti, F.; Sebag, F. Pheochromocytoma surgery without systematic preoperative pharmacological preparation: Insights from a referral tertiary center experience. Surg. Endosc. 2021, 35, 728–735. [Google Scholar] [CrossRef]
- Pacak, K. Preoperative management of the pheochromocytoma patient. J. Clin. Endocrinol. Metab. 2007, 92, 4069–4979. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.W.; Deal, L.E.; Piesman, M. Epinephrine-Secreting Pheochromocytoma Presenting with Cardiogenic Shock and Profound Hypocalcemia. Ann. Intern. Med. 2004, 140, 849–851. [Google Scholar] [CrossRef] [PubMed]
- Cryer, P.E. Physiology and pathophysiology of the human sympathoadrenal neuroendocrine system. N. Engl. J. Med. 1980, 303, 436–444. [Google Scholar] [PubMed]
- Chang, R.Y.; Lang, B.H.; Wong, K.P.; Lo, C.Y. High pre-operative urinary norepinephrine is an independent determinant of peri-operative hemodynamic instability in unilateral pheochromocytoma/paraganglioma removal. World J. Surg. 2014, 38, 2317–2323. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Ding, L.; He, Q.; Liu, M. Preoperative Management of Pheochromocytoma and Paraganglioma. Front. Endocrinol. 2020, 11, 586795. [Google Scholar] [CrossRef]
- Stefanidis, D.; Goldfarb, M.; Kercher, K.W.; Hope, W.W.; Richardson, W.; Fanelli, R.D. SAGES guidelines for minimally invasive treatment of adrenal pathology. Surg. Endosc. 2013, 27, 3960–3980. [Google Scholar] [CrossRef]
- Gagner, M.; Breton, G.; Pharand, D.; Pomp, A. Is laparoscopic adrenalectomy indicated for pheochromocytomas? Surgery 1996, 120, 1076–1079. [Google Scholar] [CrossRef]
- Weingarten, T.N.; Cata, J.P.; O’Hara, J.F.; Prybilla, D.J.; Pike, T.L.; Thompson, G.B.; Grant, C.S.; Warner, D.O.; Bravo, E.; Sprung, J. Comparison of two preoperative medical management strategies for laparoscopic resection of pheochromocytoma. Urology 2010, 76, 508.e6-11. [Google Scholar] [CrossRef]
- Buitenwerf, E.; Boekel, M.F.; van der Velde, M.I.; Voogd, M.F.; Kerstens, M.N.; Wietasch, G.J.; Scheeren, T.W. The haemodynamic instability score: Development and internal validation of a new rating method of intra-operative haemodynamic instability. Eur. J. Anaesthesiol. 2019, 36, 290–296. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author of Study and [Ref] | Country | Recruitment Period | n | D | Factors Evaluated (Cut off Values) | Significant Factors | Definition of HDI | NOS |
|---|---|---|---|---|---|---|---|---|
| Kiernan et al. [4] | USA | 2002–2013 | 91 | R | Procedure type (Open) Blockade type (Selective) | Procedure type, Blockade type | SBP > 200 mmHg | 7 |
| Kierman et al. [4] | USA | 2002–2013 | 91 | R | Tumor size (cm), Procedure type (Open) | Tumor size, Procedure type | Postoperative vasopressor requirement | 7 |
| Brunaud et al. [17] | USA | 2002–2012 | 155 | R | Age ≥ 45 (y) Tumor size ≥ 3 (cm) Familial disease | Familial disease | SBP ≥ 160 mmHg + MAP < 60 mmHg | 7 |
| Livingsone et al. [18] | France | 2000–2017 | 134 | R | Tumor size (mm) Diuretic before surgery (%) Beta-blocker before surgery (%) | (only univariate analysis) Tumor size Diuretic before surgery Beta-blocker before surgery | >10 hypo/hypertentive episodes where anesthesilogist had to use vasoactive | 7 |
| Gaujoux et al. [5] | France | 1994–2011 | 149 | R | Clinical symptom Urinary metanephrine and/or normetanephrine > 10 N Tumor size > 7 cm | preoperative HBP with clinical symptom Urinary metanephrine and/or normetanephrine >10 N | cumulative dose of norepinephrine > 5 mg | 7 |
| Namekawa et al. [6] | Japan | 1999–2014 | 82 | R | Tumor size > 6 cm Preoperative urinary Epinephrine > 200 µg/d Preoperative urinary norepinephrine > 600 µg/d | Tumor size Preoperative urinary epinephrine Preoperative urinary norepinephrine | Required continuous catecholamine support to maintain SBP ≥ 90 mmHg after adrenalectomy | 7 |
| Kwon et al. [19] | Korea | 2000–2012 | 53 | R | Tumor size (cm) SBP at presentation (mmHg) DBP at presentation (mmHg) Preoperative urinary epinephrine (µg/d) Preoperative urinary norepinephrine (µg/d) Preoperative urinary VMA (µg/d) Preoperative urinary metanephrine (µg/d) | Tumor size, Preoperative urinary epinephrine | SBP > 180 mmHg | 6 |
| Vorsellaars et al. [20] | Europe, USA, Canada | 2000–2016 | 341 | R | NR | retroperitoneal approach | MAP < 60 mmHg | 6 |
| Wu et al. [7] | China | 2012–2016 | 113 | R | Asymptomatic Diabetes mellitus ASA plasma norepinephrine (≥ULN) Plasma epinephrine Plasma dopamine Tumor size (cm) | Plasma epinephrine Plasma dopamine | MAP < 60 mmHg or required ≥ 30 consecutive minutes of catecholamine support intraoperatively | 7 |
| Chung et al. [21] | Korea | 2005–2016 | 51 | R | Clinical symptom Tumor laterality (right) Tumor size (cm) Perioperative urinary metanephrine (mg/day) Preoperative urinary VMA (mg/day) | Clinical symptom, Tumor size | SBP > 180 mmHg and MAP < 60 mmHg | 6 |
| Aksakal et al. [22] | Turkey | 2008–2015 | 37 | R | Age (y) Gender Side of Mass Operation duration (min) Duration of premedication (≥2 months) Urinary norepinephrine (≥2000 µg/24 h) Tumor size (≥6 cm) | Urinary norepinephrine, Tumor size | SBP > 200 mmHg or ≤ 90 mmHg | 6 |
| Bai et al. [23] | China | 2007–2016 | 283 | R | Intercept BMI (kg/m2) Coronary heart disease Use of crystal/colloid fluid Tumor size (cm) | Intercept BMI Coronary heart disease Use of crystal/colloid fluid Tumor size | SBP > 200 mmHg + MAP < 60 mmHg or Required catecholamine to maintain SBP | 6 |
| Tian et al. [24] | China | 2001–2018 | 102 | R | DFD < 14 d Age (y) Tumor size (cm) BMI (kg/m2) Surgical approach Tumor location Biochemical positive | Tumor size | SBP > 200 mmHg, SBP > 130% of basic SBP, SBP < 80 mmHg, SBP < 70% of basic SBP HR > 120 bpm | 6 |
| Thompson et al. [25] | UK | 2007–2014 | 52 | R | Tumor size (cm) Plasma norepinephrine (>3500 pmol/L) Laparoscopic approach Epidural analgesia | Plasma normetanephrine level | SBP > 200 mmHg | 6 |
| Thompson et al. [25] | UK | 2007–2014 | 45 | R | Tumor size (cm) Preoperative beta-blockade Postoperative fluid volume (<24 h, L) | Preoperative beta-blockade | SBP < 90 mmHg | 6 |
| Buisset et al. [26] | Canada | 1992–2013 | 88 | R | Preoperative penoxybenzamine dose (mg) Preoperative SBP (mmHg) Intraoperative vasopression use magnesium use | (only univariate analysis) Preoperative penoxybenzamine dose Preoperative SBP Intraoperative vasopression use magnesium use | Required pressor amines postoperatively | 6 |
| Pt No. | Sex (M; F) | Age (y) | BMI (kg/m2) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author of Study and [Ref] | Total | HI | Non-HI | Total | HI | Non-HI | Total | HI | Non-HI | Total | HI | Non-HI |
| Kiernan et al. [4] | 91 | NR | NR | 43; 48 | NR | NR | 52 | NR | NR | 27.5 | NR | NR |
| Brunaud et al. [17] | 155 | NR | NR | 68; 87 | NR | NR | 52 | NR | NR | 25.8 | NR | NR |
| Livingsone et al. [18] | 88 | NR | NR | 42; 46 | NR | NR | 50 | NR | NR | NR | NR | NR |
| Gaujoux et al. [5] | 149 | 13 | 136 | 48; 101 | 7; 6 | 41; 95 | NR | 58 | 53 | NR | 24.2 | 23.2 |
| Namekawa et al. [6] | 73 | 34 | 39 | 30; 43 | 15; 19 | 15; 24 | 48 | 46 | 53 | 21 | 21 | 22 |
| Kwon et al. [19] | 53 | 33 | 20 | 28; 25 | 15; 18 | 13; 7 | 47.5 | 47.5 | 47.5 | 23.3 | 23.1 | 23.5 |
| Vorsellaars et al. [20] | 341 | 169 | 172 | 149; 192 | NR | NR | 49 | NR | NR | 24.9 | NR | NR |
| Wu et al. [7] | 123 | 54 | 69 | 48; 75 | 21; 33 | 27; 42 | 46 | 47 | 45 | 24 | 23 | 24 |
| Chung et al. [21] | 51 | 25 | 26 | 25; 26 | NR | NR | 52 | NR | NR | 23.3 | NR | NR |
| Aksakal et al. [22] | 37 | 13 | 24 | 14; 23 | 5; 8 | 9; 15 | 39.3 | 40.6 | 38.6 | NR | NR | NR |
| Bai et al. [23] | 283 | 74 | 209 | 141; 142 | 31; 43 | 110; 99 | 52.4 | 54 | 51.9 | 23.5 | 21.9 | 24.1 |
| Tian et al. [24] | 102 | NR | NR | 47; 55 | NR | NR | 43.1 | NR | NR | 47 | NR | NR |
| Thompson et al. [25] | 42 | 25 | 17 | 11; 31 | 6; 19 | 5; 12 | 51 | 52 | 49 | 26 | 26 | 27 |
| Thompson et al. [25] | 45 | 21 | 24 | 12; 33 | 7; 14 | 5; 19 | 51 | 50 | 51 | 27 | 25 | 29 |
| Buisset et al. [26] | 134 | NR | NR | 62; 72 | NR | NR | 51 | NR | NR | 24 | NR | NR |
| Tumor Size (cm) | Tumor Laterality (Right) | Surgical Approach (Laparoscopic Surgery) | Clinical Symptom | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author of Study and [Ref] | Total | HI | Non-HI | Total | HI | Non-HI | Total | HI | Non-HI | Total | HI | Non-HI |
| Kiernan et al. [4] | 4 | NR | NR | NR | NR | NR | 71 (78%) | NR | NR | NR | NR | NR |
| Brunaud et al. [17] | 4.5 | NR | NR | 84 (54.2%) | NR | NR | 100% | 100% | 100% | Palpitation: 60 (39%) Sweating: 60 (39%) Headaches: 55 (35%) | NR | NR |
| Livingsone et al. [18] | 4.2 | NR | NR | NR | NR | NR | 43 (48.9%) | NR | NR | NR | NR | NR |
| Gaujoux et al. [5] | NR | 6.5 | 5 | 55 (36.9%) | 7 (53.8%) | 58 (42.6%) | 149 (100%) | 13 (100%) | 136 (100%) | 45 (30.2%) | 9 (69.2%) | 36 (26.5%) |
| Namekawa et al. [6] | 4.6 | 5 | 4.2 | NR | NR | NR | 100% | 100% | 100% | 35 (47.9%) | 20 (58.8%) | 15 (38.5%) |
| Kwon et al. [19] | 5.59 | 6.48 | 4.11 | 24 (45.3%) | 13 (36.4%) | 11 (55.0%) | 44 (83.0%) | 26 (78.8%) | 18 (90%) | 25 (47.2%) | 18 (54.5%) | 7 (35.0%) |
| Vorsellaars et al. [20] | 4.17 | NR | NR | 175 (51%) | NR | NR | NR | NR | NR | NR | NR | NR |
| Wu et al. [7] | 4.6 | 4.9 | 4.4 | NR | NR | NR | 123 (100%) | 100% | 100% | 21 (17.1%) | 5 (9%) | 16 (23%) |
| Chung et al. [21] | 5.6 | NR | NR | 22 (43.1%) | NR | NR | 51 (100%) | 100% | 100% | 26 (51%) | NR | NR |
| Aksakal et al. [22] | <6 cm: 24 (64.7%) | <6 cm: 11 (84.6%) | <6 cm: 13 (54.1%) | 21 (56.8%) | 8 (61.5%) | 13 (54.2%) | NR | NR | NR | NR | NR | NR |
| Bai et al. [23] | 5.5 | 6.5 | 5.2 | 141 (49.8%) | 35 (47.3%) | 106 (50.7%) | 132 (46.6%) | 32 (43.2%) | 100 (47.8%) | NR | NR | NR |
| Tian et al. [24] | 5 | NR | NR | 57 (55.9%) | NR | NR | 63 (61.8%) | NR | NR | NR | NR | NR |
| Thompson et al. [25] | 4.4 | 4.8 | 3.8 | NR | NR | NR | 15 (35.7%) | 13 (52%) | 2 (13%) | NR | NR | NR |
| Thompson et al. [25] | 4.4 | 5 | 3.8 | NR | NR | NR | 18 (40%) | 6 (30%) | 12 (50%) | NR | NR | NR |
| Buisset et al. [26] | 3.96 | NR | NR | 71 (53.0%) | NR | NR | 134 (100%) | NR | NR | NR | NR | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urabe, F.; Kimura, S.; Iwatani, K.; Takahashi, K.; Ito, K.; Tashiro, K.; Tsuzuki, S.; Miki, J.; Kimura, T.; Furuta, N.; et al. Risk Factors for Perioperative Hemodynamic Instability in Pheochromocytoma: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 4531. https://doi.org/10.3390/jcm10194531
Urabe F, Kimura S, Iwatani K, Takahashi K, Ito K, Tashiro K, Tsuzuki S, Miki J, Kimura T, Furuta N, et al. Risk Factors for Perioperative Hemodynamic Instability in Pheochromocytoma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(19):4531. https://doi.org/10.3390/jcm10194531
Chicago/Turabian StyleUrabe, Fumihiko, Shoji Kimura, Kosuke Iwatani, Kazuhiro Takahashi, Kagenori Ito, Kojiro Tashiro, Shunsuke Tsuzuki, Jun Miki, Takahiro Kimura, Nozomu Furuta, and et al. 2021. "Risk Factors for Perioperative Hemodynamic Instability in Pheochromocytoma: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 19: 4531. https://doi.org/10.3390/jcm10194531
APA StyleUrabe, F., Kimura, S., Iwatani, K., Takahashi, K., Ito, K., Tashiro, K., Tsuzuki, S., Miki, J., Kimura, T., Furuta, N., & Egawa, S. (2021). Risk Factors for Perioperative Hemodynamic Instability in Pheochromocytoma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(19), 4531. https://doi.org/10.3390/jcm10194531